Many people do not know or realize that there are actually many different types of hypothyroidism. Technically, there is primary hypothyroidism, secondary hypothyroidism, tertiary hypothyroidism, and Wilson’s Temperature Syndrome.
Today’s article is going to be going over the difference between Wilson’s Temperature Syndrome and primary hypothyroidism, as these are the two most common forms of hypothyroidism that people are struggling with. Many people have never even heard of Wilson’s Temperature Syndrome (WTS), but if someone actually has WTS but is being treated as if they have primary hypothyroidism, then they may never end up getting complete resolution of their symptoms such as cold extremities, fatigue, depression, tiredness, or weight gain, even though all their blood lab values are normal.
By treatment WTS properly, there are many people that can get a complete resolution of their symptoms, and sometimes without lifetime medication. This is one of the primary differences with primary hypothyroidism.
In order to understand the difference between the two types of disorders, we are going to need to get a little bit of thyroid physiology cleared up. Otherwise, the differences won’t really make sense.
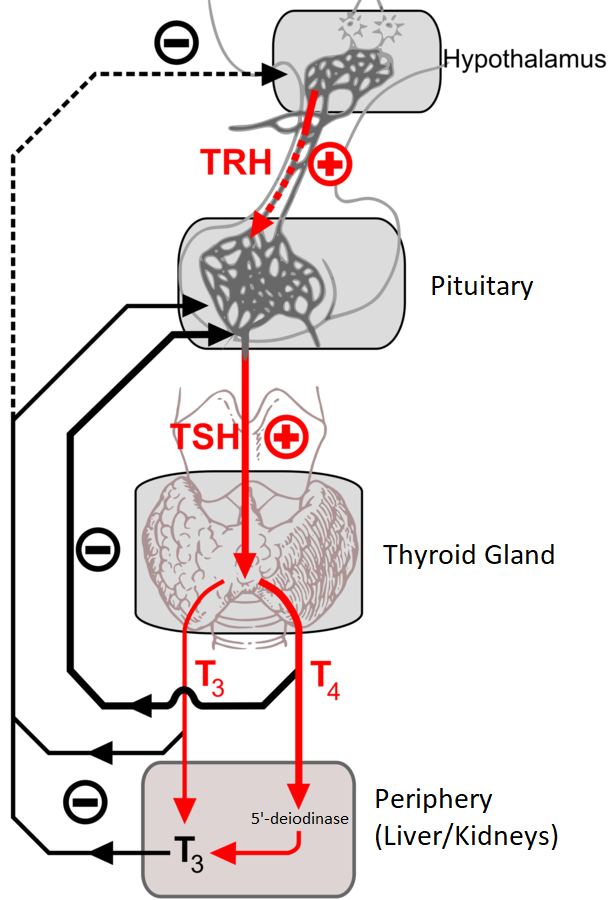
The whole thyroid cascade actually starts in a particular brain structure called the hypothalamus. The hypothalamus releases a hormone called Thyrotropin-releasing hormone (TRH), which then goes to the pituitary. From this signal, the pituitary releases Thyroid-stimulating hormone (TSH). TSH is the hormone that is usually measured on thyroid blood tests.
TSH then travels down to the thyroid where it primarily tells the thyroid to release tetraiodothyronine, AKA T4. The medications L-thyroxine, levothyroxine, and Synthroid are all synthetically created T4, the same type that our thyroid produces.
T4, however, is not the main active thyroid hormone. The main active thyroid hormone is triiodothyronine, AKA T3.
The conversion from T4 to T3 happens mainly in the liver, kidneys, and intestines (about 80%) while only a minor amount of this conversion occurs in the thyroid itself (about 20%). The enzyme that does this conversion is called 5′-deiodinase (5 prime – deiodinase).
There is another chemical that T4 can turn into, however. It is called reverse T3 (rT3). The enzyme that does this conversion is called 5-deiodinase (no “prime”). rT3 is completely inactive, whereas T3 is completely active at the thyroid receptor.
People with primary hypothyroidism have, by definition, low T4 and a high TSH (T3 may or may not be low).
This means that the pituitary is trying to signal the thyroid with a lot of TSH to make more T4, but the thyroid is not responding like it should. The thyroid should respond by making more T4, but it consistently produces less than is needed.
Thus, primary hypothyroidism is a defect in the thyroid gland itself. This becomes important when comparing it to WTS.
It makes sense to treat people with primary hypothyroidism with Synthroid (synthetic T4) since these people are having a hard time making their own T4.
For some (especially those who also have low T3 levels), using a combination of T4/T3 (such as Armour or Naturoid) will be best and will resolve their symptoms the most.
For people with primary hypothyroidism, they will likely need to take this medication for life to make up for what their thyroid isn’t producing. (However, there are alternative treatment options that will be discussed in future articles that may increase the chance of getting off of, or at least lowering, medication.)
People with WTS, by definition, have a chronically low basal body temperature and could have normal or low T3, high or normal TSH, and normal T4. That is, sometimes the only positive clinical finding in WTS, besides many hypothyroid symptoms, is a low body temperature. If someone’s body temperature is usually normal (at or above 98.6 degrees Fahrenheit), then they do not have WTS.
Many medical doctors are not taught about WTS, and thus are not trained to look for a defect in the thyroid system if the blood tests come back normal. However, many people intuitively know that they have some thyroid issue (due to the symptoms they have), and many times the doctor will very much suspect a thyroid issue based on the presentation but will dismiss it when the blood tests come back normal. However, the person can still have WTS even with normal blood values.
Actually, many doctors do not yet recognize WTS as an official diagnosis. Yet, the many thousands of people treated with T3 for a short period of time and have fully recovered would disagree. I suspect that WTS will eventually become an official diagnosis after some years of resistance to the change, just like fibromyalgia did.
One thing to note, though, is that WTS is usually something going on, primarily, at the level of T3, and not with the thyroid gland itself.
For example, a patient can have a normal TSH, a normal T4, but low T3 and a low body temperature. In this case, it seems obvious that nothing is wrong with the thyroid gland itself, and we should not attempt to treat it. Remember, the thyroid gland it mainly responsible for responding to TSH by secreting T4, and that seems to be working just fine.
In this case, the patient is not properly converting T4 to T3, which occurs mainly in the liver and kidney. Thus, since T3 is the main hormone that regulates our metabolic rate, this person has a lowered metabolic rate and thus a lowered temperature. (note: thyroid hormones are not the only hormones that affect metabolic rate and temperature, but if someone has a consistently lowered temperature taken at 3-hourly intervals throughout each day, then it is pretty safe to say that thyroid, or T3, is involved.)
As to why this patient developed an impaired conversion of T4 ot T3, that depends. It could be from prolonged chronic stress or a traumatic event (high cortisol)(1), chronic severe dieting / calorie-restriction (2), or reduced carbohydrates for a long time (3). There are other things that can cause this as well, but these are usually the main factors.
Alternatively, a patient may present with normal TSH, normal T4, normal T3, but a low body temperature. In this case, they may have enough T3 floating around but the T3 isn’t actually making it inside the cell to stimulate the nuclear receptor. There are many reasons why T3 has a hard time stimulating its receptor. One could be a preponderance of bad fats in the diet (or too many unsaturated fats in the diet) (4) or a high level of free fatty acids (FFAs) in the bloodstream (5).
By using a safe and effective T3 supplementation protocol for WTS, not only can the body temperature be restored, but it can also induce a “resetting” phenomenon on the body so that the body more easily makes more of its own T3. While the physiology behind this is a bit out of the scope of the article, it has to do with T3 allowing rT3 levels to fall, and thus reducing the “block” for T3 synthesis.
By correcting WTS, patients usually find that they feel a lot better, have more energy, have a more positive outlook on life, and may be able to lose weight easier.
If you would like more detailed information on everything there is to know about WTS, I would suggest reading the free physician’s ebook on the topic. It dives more heavily into the physiology than I wanted to in this article and also provides answers to frequently asked questions. No doctor or patient should ever undergo T3 therapy before reading this manual!
As always, let me know if you have any comments, suggestions, or experiences below!
References:
- Heyma P, Larkins RG. Glucocorticoids decrease in conversion of thyroxine into 3, 5, 3′-tri-iodothyronine by isolated rat renal tubules. Clin Sci (Lond). 1982 Feb;62(2):215-20. PubMed PMID: 7053919.
- van der Heyden, J.T.M. (1988, October 19). Cellular mechanisms in the generation of the low T3 syndrome. Erasmus University Rotterdam. Retrieved from http://hdl.handle.net/1765/51063
- Bisschop PH, Sauerwein HP, Endert E, Romijn JA. Isocaloric carbohydrate deprivation induces protein catabolism despite a low T3-syndrome in healthy men. Clin Endocrinol (Oxf). 2001 Jan;54(1):75-80. PubMed PMID: 11167929.
- Wiersinga WM, Chopra IJ, Teco GN. Inhibition of nuclear T3 binding by fatty acids. Metabolism. 1988 Oct;37(10):996-1002. PubMed PMID: 3173114.
- Suzuki Y, Nanno M, Gemma R, Yoshimi T. Plasma free fatty acids, inhibitor of extrathyroidal conversion of T4 to T3 and thyroid hormone binding inhibitor in patients with various nonthyroidal illnesses. Endocrinol Jpn. 1992 Oct;39(5):445-53. PubMed PMID: 1478185.


3,080 Comments
Beauty Fashion · May 9, 2025 at 10:54 pm
As a Newbie, I am constantly browsing online for articles that can help me. Thank you
Hairstyles VIP · May 10, 2025 at 10:31 pm
I beloved as much as you will obtain carried out proper here. The comic strip is attractive, your authored subject matter stylish. nevertheless, you command get got an impatience over that you wish be delivering the following. sick certainly come further previously once more as precisely the same just about very regularly inside of case you protect this increase.
I Fashion Styles · May 11, 2025 at 9:34 pm
What抯 Happening i’m new to this, I stumbled upon this I have found It positively helpful and it has helped me out loads. I hope to contribute & help other users like its aided me. Great job.
Beauty Fashion · May 13, 2025 at 4:19 pm
Great blog post. Things i would like to bring about is that laptop or computer memory needs to be purchased when your computer still cannot cope with anything you do along with it. One can deploy two RAM boards having 1GB each, as an illustration, but not one of 1GB and one having 2GB. One should look for the manufacturer’s documentation for own PC to make sure what type of ram is necessary.
KAYSWELL · May 14, 2025 at 9:13 pm
Thank you for the good writeup. It actually was once a entertainment account it. Glance complex to far delivered agreeable from you! By the way, how could we be in contact?
KAYSWELL · May 15, 2025 at 7:56 pm
Hi there! Would you mind if I share your blog with my facebook group? There’s a lot of folks that I think would really appreciate your content. Please let me know. Thanks
Beauty Fashion · May 16, 2025 at 6:27 pm
I will right away grab your rss feed as I can’t find your e-mail subscription link or e-newsletter service. Do you have any? Please let me know so that I could subscribe. Thanks.
muscle building pills like steroids · May 17, 2025 at 8:20 pm
This can occur when micro organism from the urethra or bladder travel up the vas
deferens and infect the testicles. In some circumstances,
sexually transmitted infections similar to gonorrhea or
chlamydia also can lead to orchitis. Ache within the testicles can be a trigger for concern and discomfort for many
men.
In these with urinary tract infections and an obstruction within the genitourinary system, antibiotics, and emergent urologic intervention are necessary.
The testicular ache could vary from severe to absent on the time the
particular person sees a physician. Hardly Ever, nevertheless, the injury could appear minor, however there could also be a severe underlying harm to the
testicle. Epididymitis occurs when there might be inflammation of the epididymis (a construction within the scrotum).
Epididymitis primarily affects grownup males, and is most common between the ages of 19 to forty years; nonetheless, it could occur
in prepubescent boys and aged males. The problem is that there are some critical circumstances that
can cause testicular ache. This article appears at
five such circumstances, including one that is thought-about a real medical
emergency.
This situation normally impacts younger youngsters
(around seven to fourteen year olds) and it requires instant
surgery. Testicular most cancers just isn’t one of many main causes of
scrotum ache when sitting as 90% of the testicular most cancers sufferers
don’t really feel pain in their scrotum. Testicular most cancers is usually recognized through detection of
a lump. Orchitis is the name given to the inflammation of testicles as a end result of epididymitis, bacterial
infection (like mumps) or STDs. The inflammation is often accompanied with blood in the semen and fever in case of orchitis.
If orchitis is caused as a end result of mumps, then there is not a treatment for
it with the particular person usually turning into infertile.
When the lump is an epididymal cyst or spermatocele, the light will
be in a position to get via to the opposite side. Orchitis can affect one or each
testicles and will trigger extreme pain and infertility.
Just bear in mind these treatments will not treat the an infection itself — with out prescription antibiotics, the an infection could get worse and trigger everlasting harm to your testicle.
Testicles, those small oval organs that hold delicately in a protecting sack called the scrotum, play a crucial
position in reproduction and hormone production. Whereas it is true that any testicular pain can be trigger for concern, today we are going to delve into the
intricate world of left testicle ache – its causes and symptoms.
CTP can interfere with normal, every day residing and the
flexibility to work.
If you spot any change in the look or really feel of your testicles, contact your GP immediately.
The testicles are very sensitive and easily injured – even a minor
knock could cause excruciating pain. Acute prostatitis signs are
extra severe than persistent prostatitis, which may be bothersome but bearable.
Prostatitis is an irritation of the prostate gland, which is positioned between the bladder
and penis. The inflammation may be acute (short-lived) or chronic (symptoms final
6 weeks or longer). By regularly performing this exam, you
may turn into extra familiar with your testicles and conscious
of any adjustments that could be of concern.
Usually, bacterial infections corresponding to STIs or urinary tract infections cause orchitis, however the mumps
virus may trigger this condition. That mentioned, it’s always a good suggestion to examine in together with your doctor after an damage to your
testicles or scrotum. Quayle recommends visiting the hospital to have the injury checked out by a medical skilled,
regardless of how a lot ache you experience.
The cause could also be obvious when you have had a
current injury or accident while playing a sport or exercising.
Viral orchitis, then again, is mostly attributable to the mumps virus.
Mumps is a extremely contagious viral infection that primarily affects the salivary glands, however also can spread to the testicles.
This is more common in adolescent boys and grownup males who haven’t been vaccinated towards mumps.
If a lump or abnormality is discovered, the subsequent step is to perform a biopsy.
This involves eradicating a small pattern of tissue from the
testicle and analyzing it under a microscope to determine if cancer cells are present.
Epididymitis – When Naughty Neighbors AttackOur expedition commences with the notorious wrongdoer known as epididymitis.
Picture a bustling neighborhood where our testicles reside, full with tiny houses called epididymis.
This inflammation may be brought on by bacterial infections or sexually transmitted illnesses (STDs).
Simply muscle building pills like steroids rowdy neighbors,
they can make your left testicle scream out in agony.
Tremble not; medical intervention and antibiotics can deliver tranquility again to the troubled streets.
Certain indicators necessitate quick medical consideration somewhat than waiting
things out.
The vas deferens is the duct that transports sperm from the epididymis to the ejaculatory ducts earlier than ejaculation. Hernias happen when tissue pushes through a weak part of the abdominal muscular tissues.
An inguinal hernia is one type of hernia that can push
into the scrotum, inflicting testicular pain and swelling.
jcrunch.com · May 17, 2025 at 10:15 pm
Ganz ohne Nebenwirkungen kommt die Testosteronersatztherapie nicht aus.
Zudem sollte sie stets unter ärztlicher Aufsicht
erfolgen, um Folgeschäden beispielsweise an der Prostata auszuschließen. Bei professioneller Begleitung
und guter Einstellung gilt die Testosteronersatztherapie jedoch als äußert sicher und kann das Wohlbefinden der Betroffenen ganzheitlich verbessern. Die langzeitwirksame sogenannte Depot-Spritze ist hierbei deutlich kostengünstiger und angenehmer für den Patienten.
Bei Männern mit einem existierenden Testosteronmangel konnten durch eine Testosteron-Ersatztherapie bereits beeindruckende Wirkungen erzielt werden. Nach der Injektion kommt es hier zu
Testosteron-Spitzen, welche immer mehr abfallen. Dieser abrupte
Hormonwechsel führt zu stärkeren unerwünschten Nebenwirkungen als eine gleichmäßige Erhöhung.
Der Ursprungsgedanke von Testosteron-Präparaten warfare die symptomatische Bekämpfung eines Testosteronmangels.
Man kan Testosteron aus verschiedenen Gründen verschrieben bekomme und wern der Arzt den Grund nicht kennt wird
er es dir auch nicht verschrieben.
In diesem Text werden wir die wichtigsten Aspekte der Testosterontherapie in der PKV beleuchten. Der cerascreen® Freies Testosteron Check wird von einem medizinischen Fachlabor durchgeführt, ohne Wartezeiten in der
Arztpraxis. Die professionelle Analyse übernimmt unser medizinisches Partnerlabor.
Eine Testosteron-Ersatztherapie dient der Behandlung eines vorliegenden Testosteronmangels.
Bei einem existierenden Testosteronmangel übernimmt
meist die Krankenkasse die Kosten. Bei einem Privatkauf mit einem ärztlichen Rezept liegen die Kosten pro Tag bei
rund zero,1-3 €. Eine Testosteron-Ersatztherapie wird nur dann empfohlen, wenn tatsächlich ein Testosteronmangel
vorliegt. Nein das stimmt nicht es gibt verschieden Gründe wiesos man und Testosteron verschreiben bekommt.
Es gibt verschiedene Erkrankungen und auch Gründe für die eine
Testosteroneinanhem wichtig ist und auch den Wunsch im andren Geschlecht zu leben. Informeir
dich ein weig mehr über Hormone und dan wirst du merken das
man nicht imner einen Mangel habem muß um prostatakrebs testosteron Zu hoch (jcrunch.com) verschreiben zu bekommen.
Da die Dosierung von unterschiedlichen Faktoren abhängig ist, sollte ein Arzt
diese speziell auf Sie abstimmen. Dabei ist zu unterscheiden, um welche Darreichungsform
von Testogel es sich handelt. Hierbei handelt es sich um eines
der wichtigsten Hormone, welches im männlichen Körper nicht fehlen darf.
Eine Testosteron-Ersatztherapie dient vorwiegend der
langfristigen Behandlung eines Testosteronmangels. In diesem Artikel lernst du über die
verschiedenen Therapie-Methoden, den Ablauf, die
Nebenwirkungen und die Kosten einer Testosteron-Ersatztherapie.
Für eine sogenannte hormonelle Substitutionstherapie wird ein Rezept
benötigt, was eine vorherige Untersuchung bei einem Arzt voraussetzt.
Sie sollten allerdings, von unseriösen Anbietern Abstand nehmen, die kein Rezept verlangen. Ein Mangel an Testosteron kann zu Hypogonadismus führen, eine hormonelle (endokrine) Funktionsstörung.
Die Ursache liegt hauptsächlich in einer gestörten Hormonproduktion in den Hoden oder einer Störung von übergeordneten Hormon- Steuer- Zellen im Gehirn.
Die Ärztin/der Arzt prüft zunächst, ob klinische Symptome für einen Testosteronmangel
vorliegen. Die Blutabnahme zur Messung des Testosteron muss
morgens erfolgen, da der Testosteronspiegel bei
Männern in der Früh erhöht ist. Für viele Männer ist der erste
Ansprechpartner der Hausarzt oder der Urologe. Unabhängig von der Wahl des Arztes ist
es wichtig, sich gut vorzubereiten. Bringen Sie alle relevanten medizinischen Unterlagen mit, um eine zielgerichtete
Untersuchung und mögliche Behandlungsansätze zu diskutieren.
Entdecke, wie eine gezielte Behandlung Deine Lebensqualität nachhaltig verbessern kann.
Abschließend lässt sich sagen, dass die Testosterontherapie in der PKV unter bestimmten Bedingungen erstattet werden kann.
Es ist jedoch wichtig, sich im Vorfeld gut zu informieren und alle notwendigen Schritte zu beachten, um eine reibungslose Kostenübernahme zu gewährleisten. Durch seine über 35 Jahre Erfahrung
als niedergelassener Arzt mit eigener Praxis verfügt
Dr. med.
where to buy real steroids online · May 18, 2025 at 8:10 am
Because a higher physique fats percentage might
cause decreased testosterone manufacturing, it’s necessary to take care of a healthy weight.
If your testosterone ranges are clinically low, then working together with your healthcare provider to find out subsequent steps for reaching wholesome testosterone levels is
the beneficial path. However when you simply want to increase your testosterone to
improve your overall health, the key takeaway is that it’s not needed.
Additionally, a 2015 study additionally found that ashwagandha
elevated testosterone levels in males over an 8-week
interval. It also increased muscle mass and power when paired with a training program.
Male sex hormones called androgens, together with testosterone play an important position in women’s
well being. Girls usually have a hard time increasing lean muscle mass,
because their our bodies naturally produce estrogen. Ginseng is a
traditional medicinal herb that contains high concentrations of antioxidants.
Ginseng extract may help cut back oxidative stress, improve
mind features, stimulate the production of nitric oxide, enhance blood circulation, and may deal with erectile dysfunction.
Whereas it’s thought of a “male” intercourse hormone, each gender synthesizes and needs some quantity of testosterone.
Analysis means that testosterone levels could be
associated to dietary fat intake. A 2019 examine discovered that men with chubby and weight problems who consumed meals high in fat skilled steep declines
in testosterone within the hours after the meal. Testosterone can also be produced in the ovaries and adrenal
glands, that are the organs above the kidneys. In people assigned feminine at delivery, typical concerns
embody testosterone ranges being too excessive.
Some folks may take testosterone throughout menopause to ease signs.
If you may have concerns with any sleep points, like
sleep apnea, see a physician so you’ll have the ability to
handle them. A blood check is the most effective and most reliable way to affirm you might
have low testosterone. If you suspect you’ve low
T, deliver it as a lot as your healthcare supplier.
Often your physician will order a blood panel to have a
look at where to buy real steroids online your levels
are at. Eat Complete Meals – as mentioned earlier
top-of-the-line ways to increase your general well being is to eat extra
complete meals. Entire foods are any food without an ingredient label; suppose meats, produce, nuts and seeds, and so forth.
One common tip to assist ensure you’re eating extra entire foods to “shop the perimeter” of the grocery store.
Too many people keep up that additional hour, watching
junk on TV or messing round on our phones. Lack
of quality sleep can go away you too tired to eat nicely or sneak in a exercise the subsequent day.
Bonus factors if you’re into HIIT workouts;
high-intensity interval coaching is among the
many most effective workouts to boost T (18).
In addition to weightlifting, research have proven that HIIT workouts can even help increase testosterone ranges.
For these of you who don’t know, HIIT stands for high-intensity interval coaching.
It calls for brief, intense bursts of train, followed by a less-intense recovery period.
You repeat with the intense/less-intense cycle a quantity of times all through the
workout. In addition to growing T, HIIT has been proven to improve athletic conditioning
and fat metabolism, as well as increase muscle
power. If you are under 30 and have an ample amount of testosterone, then a authorized testosterone booster just isn’t
beneficial for you. Ingesting a T-booster when ranges are enough
can comprise your natural testosterone manufacturing.
Sex is generally thought to be crucial for relationship satisfaction and
overall well being and delight of life. TRT would possibly nonetheless be the best name if you’re
underneath forty, however purpose to get the most out of the pure
route first. TRT just isn’t for everybody and may carry
potential dangers and side effects.
Carb intake also plays a role, with research
displaying carbs might help optimize testosterone levels throughout resistance
training. Fixed weight-reduction plan or overeating might disrupt your testosterone ranges.
Magnesium not only helps produce testosterone,
however it additionally enables you to chill
out and sleep, two things which would possibly be essential to testosterone manufacturing.
High-fat diets are often excessive in cholesterol, which can be concerning for some males.
Subsequently, having excessive ranges of “good” ldl cholesterol (or HDL cholesterol) is essential for bettering testosterone ranges.
Do Not cut out all fats out of your food plan or you might even see a hormone degree drop.
As An Alternative, concentrate on high-quality fats and moderate how typically you eat processed foods.
General, Adaptophen’s unique formulation, confirmed effectiveness, and commitment to high quality
make it one of the best testosterone booster of 2024. It outshines its rivals by delivering superior
outcomes and providing customers with a dependable and efficient answer to
reinforce their testosterone ranges and overall well-being.
That stated, there are different necessary methods to maximize your testosterone naturally.
Josie · May 19, 2025 at 8:34 pm
It can have an effect on anybody however it’s
the commonest in those between the ages of 50 and 69.
The outcomes will indicate how a lot free testosterone is circulating in your bloodstream.
It will also inform your doctors the whole amount of testosterone
in your body. If you acknowledge the indicators
of high testosterone in a man or woman, it’s finest to
talk to a specialist. They can counsel the ideal plan of action that can mitigate your specific
well being drawback. But, in some cases, the T levels
can go well over the conventional threshold
and cause a variety of problems. Decreased sexual activity or need can lead to a drop in serum testosterone in older males.
This can result in an increase in testosterone levels, which may result in signs similar to hair loss, acne,
and infertility. Treating PCOS in men entails addressing the underlying hormonal imbalances by way of treatment and life-style modifications.
Furthermore, for women, high testosterone ranges could cause hormonal imbalances and disrupt the normal menstrual cycle.
This can result in irregular durations, excessive hair development
(hirsutism), and pimples. Women with high testosterone ranges may expertise fertility points,
similar to issue getting pregnant or having irregular ovulation.
Testosterone pellets are very fashionable, and many ladies swear
by them, however they aren’t beneficial by most menopause consultants.
In common, girls who use pellets initially love them because the
massive bolus of estrogen and testosterone the pellets offer instantly makes them really feel sexy, energetic, and fabulous overall.
However these women usually find yourself
with unacceptably excessive levels as a outcome of the dose
what is the strongest steroid (Josie) just
too high and the merchandise aren’t regulated.
After I see a girl experiencing negative unwanted side effects,
she is almost all the time using pellets.
When mature males lose energy, it’s time for them to spice up their testosterone ranges.
As A End Result Of the sex hormone not solely influences the external look, it additionally keeps plenty of
momentum inside – and in addition in ladies.
Be Taught about the function of testosterone within the
human body and how one can naturally enhance your testosterone levels.
High testosterone ranges in men, often referred to as hyperandrogenism, can result in varied well being issues, such as aggressive conduct, acne, and an increased threat of heart
issues. Having elevated testosterone levels isn’t necessarily a foul
thing; many men with excessive testosterone may expertise optimistic health benefits.
Nonetheless, if testosterone ranges become excessively excessive, it could trigger a quantity of undesirable
unwanted aspect effects.
It Is important to notice that these symptoms may not at all times be solely attributable to excessive testosterone
levels. Different elements, corresponding to hormonal imbalances, underlying
medical circumstances, or sure medications, can even contribute to those signs.
If you suspect that you’ve got got high testosterone ranges, it is crucial to consult with a healthcare professional for correct prognosis and acceptable treatment choices.
For example, when you expertise elevated sexual need, muscle mass, energy, power, and endurance, then you might see
the high T ranges pretty much as good for the body. Elevated
testosterone could be a good boon for many who wish to get greater, quicker, and stronger.
Excessive testosterone levels within the physique can have various results on overall health.
Testosterone is a hormone produced in each men and women, though it performs a more significant function in male reproductive and sexual
improvement.
Nevertheless, when levels of testosterone are elevated, it could
lead to an overproduction of sebum, which can clog
pores and result in acne breakouts. This can be particularly
problematic for people who have already got oily or acne-prone pores and skin.
One of the widespread signs of excessive testosterone ranges in males is increased aggression and irritability.
Studies have shown that testosterone can influence behavior
and mood, and when ranges are elevated, it could result in heightened aggression and irritability.
This can manifest in a wide selection of ways, corresponding to elevated anger or issue controlling feelings.
Testosterone levels can fluctuate as a end result of numerous factors,
and a complete analysis is important for an correct prognosis.
Always seek the guidance of with a medical skilled
to interpret your test results and decide the most effective plan of action. There are several methods to test testosterone ranges, starting from house check
kits to laboratory exams. It is essential to choose a way that provides accurate outcomes to ensure an appropriate diagnosis and therapy.
Excess physique hair and acne are frequent signs of excessive testosterone in girls.
One of the most important gamers right here is the limbic system, particularly the amygdala, which
processes worry and safety cues, and the nucleus accumbens, which processes pleasure and reward.
Ideally, unprocessed, nutrient-rich meals – greens, legumes, fruits and complete grains particularly – and healthy fats
within the form of nuts, seeds and eggs are important.
Alcohol, sugar and white flour merchandise, then again, must be avoided.
A 2020 meta-analysis discovered that TRT significantly improved depressive symptoms in men with low testosterone.
If you discover the hair in your arms, legs, and chest seems to be darker and fuller, this can indicate high testosterone.
As tempting as it may seem, you want to never use steroids to boost the results of your
workout.
A major care doctor or urologist may help make an accurate estimate of excessive testosterone ranges
in males. In men, testosterone can regulate libido (sex drive), strength, muscle mass,
fats distribution, and spermatogenesis. Testosterone injections
can create a rapid increase in testosterone ranges in many males that
final for a few days earlier than gradually lowering. Harvard Medical College calls this a “rollercoaster effect,” which might
result in fluctuating mood and power ranges.
matkafasi.com · May 21, 2025 at 7:52 pm
If you’ve symptoms of pulmonary problems, your physician could order additional
laboratory tests, together with lung perform blood checks.
Children ages 15 and underneath have a separate set of ranges, as their hematocrit levels change quickly with age.
The specific lab that analyzes the outcomes will decide the
traditional hematocrit range for a child of a certain age.
He embraces an lively life-style combining diet, exercise and wholesome choices.
By working to tell readers of the choices available to them,
he hopes to improve their well being and quality
of life. Sitting up (as opposed to mendacity down) during a blood draw can also increase your outcomes
[18]. Check outcomes vary primarily based on numerous components, starting from what
kind of system is used to take the measurement as to whether you have been drinking sufficient fluids [17, 2].
It’s essential to remember that the next strategies
aren’t methods to deal with chronically low hematocrit, but ways to
improve your cardiovascular health and handle any dietary deficiencies.
Not having enough hematocrit can additionally be symptomatic of depression, increased
nervousness, and panic dysfunction. Whereas excessive HCT can be a
concern, low HCT levels also indicate potential well being points.
The hematocrit worth helps consider blood viscosity, fluid stability, and the
oxygen-carrying capability of the blood. The normal vary for adults varies barely between men and women, with men typically
having a higher vary (around 40-54%) compared to girls (around 37-47%).
Nevertheless, these ranges can range relying on the particular laboratory
and reference values used.
Staying well-hydrated helps hold blood quantity and hematocrit levels within the normal range.
Smoking reduces oxygen levels in the blood, causing the body to
compensate by rising pink blood cell production. Continual people who smoke usually have larger hematocrit levels on account of this compensatory mechanism.
Solely then will your physician prescribe a remedy that covers the
method of bringing HCT back to its regular vary.
For athletes, hematocrit levels can provide insights into
performance and endurance. However, abnormally high ranges may elevate concerns about the usage of performance-enhancing substances or the chance of issues similar to stroke.
For youngsters, the traditional vary typically falls between 36% and 40%.
It’s necessary to notice that these ranges may range slightly depending on the laboratory conducting the
test. Unlike the opposite tests concerned in CBC, an HCT blood check would require a venous blood pattern.
This is drawn from the veins behind your elbow and
may solely be carried out by a licensed phlebotomist.
Nonetheless, additional tests, such as hemoglobin levels and iron research,
are usually needed to determine the precise trigger, corresponding to iron deficiency or chronic disease.
Dehydration occurs when the physique loses more fluids than it takes in, decreasing blood
plasma quantity. This can artificially elevate hematocrit ranges, because the concentration of red blood cells seems larger in a smaller blood quantity.
Signs of dehydration embody thirst, dry mouth, and decreased urine output.
A hematocrit value above the traditional vary
may point out dehydration, however the test’s NPV is limited as
a outcome of other conditions, similar to polycythemia vera,
can even cause elevated ranges. Rehydration and follow-up testing are sometimes necessary to confirm the analysis and rule
out underlying points. Hematocrit is a standard blood
take a look at that measures the proportion of red blood cells (RBCs) in the complete volume of blood.
The CBC check may detect abnormalities of white blood cells or platelets.
Checking your ALT level can help find liver illness or
harm early, even before you’re feeling sick. If you’ve gotten your genes sequenced, SelfDecode can help you establish
if your levels are high or low as a end result of your genes, and then pinpoint what you are
in a place to do about it.
Polycythemia vera (PV) is a uncommon blood dysfunction characterized by the overproduction of pink blood cells in the bone marrow.
This situation is usually caused by mutations
within the JAK2 gene, which leads to elevated red blood cell
manufacturing. As Soon As your hematocrit take a look
at outcomes how expensive are steroids, matkafasi.com, prepared, your healthcare supplier will review them
with you. The outcomes are expressed as a share, indicating the proportion of red blood cells in your blood.
You should seek the assistance of your doctor before appearing on any content material on this website, particularly in case you are pregnant, nursing, taking medication, or have a medical situation. These signs also can indicate
an underlying situation, so a person should contact a physician promptly
to forestall future complications. Newborn infants have excessive hematocrit levels that slowly decrease over the
neonatal interval.
https://www.google.ps/url?q=https://gaiaathome.eu/gaiaathome/show_user.php?userid=1130297 · May 21, 2025 at 8:43 pm
We settle for most main insurance coverage, and new patients are welcome.
We also handle any underlying health points that could possibly be exacerbating hormone deficiency.
Our built-in care results in better therapy outcomes and higher patient satisfaction.
They may even talk about your symptoms and any issues you would possibly have about testosterone remedy.
In truth, maintaining healthy testosterone levels
long term advantages all-cause mortality with out negatively impacting the prostate.
There can be no conclusive proof linking TRT use at
recommended dosages to elevated anger or aggression. While optimistic immediate effects of steroids – https://www.google.ps/url?q=https://gaiaathome.eu/gaiaathome/show_user.php?userid=1130297, from TRT build steadily over months, sufferers usually report preliminary benefits including higher energy, mood, motivation and sexuality within several weeks.
The longer hormone imbalance goes untreated, the more these
deficiencies negatively compound – making it harder and taking
longer to recover. The Hormone Health Clinic offers comprehensive, evidence-based HRT.
We use cutting-edge expertise and personalized care to
attain optimal health outcomes.
Administration routes embody pellets, lotions,
injections, or patches, relying on individual needs.
Consultation with a healthcare supplier is crucial to find out suitability.
Addressing imbalances sooner improves weight administration and general health.
Untreated low testosterone in males may find yourself in decreased muscle mass, increased physique fat, decreased power, and negative mood
changes. At Renewal Well Being Clinic, we’re devoted to offering
top-tier care for individuals seeking growth hormone remedy.
With our integrated method centered on the individual,
advanced testing capabilities and use of bioidentical hormones, we assist sufferers optimize well being, sluggish growing older and
improve vitality. Our Lake Mary compounding pharmacy
can formulate personalized treatments containing bioidentical estradiol, progesterone,
testosterone, DHEA, and different hormones.
We supply oral capsules, sublingual tablets, topical
creams, injectable serums, pellet implants, and extra.
Your supplier will suggest probably the most
appropriate bioidentical hormone preparations and delivery
methods to deal with your therapy targets. Whereas we concentrate on hormone replacement, our practitioners also take a look at the whole affected person picture when formulating care plans.
It doesn’t mean you’re getting old, that your
body is failing you, or that you’ve got an incurable medical situation. Right Here at our hormone therapy Lake Mary clinic, we perceive that fact.
We additionally know what can occur if hormone levels change too much or
too quickly. However, we additionally offer more economical testosterone options in Lake Mary.
Regardless of the HRT sort, getting the hormone therapy
online is unimaginable due to the therapy specifics and is even harmful in many elements.
In Any Other Case, such remedy can deliver a lot of unfavorable effects, worsen the patient’s well-being and decelerate
the restoration course of. So far we’ve explained the dangers of durable testosterone deficiencies in males and symptoms
which may signal you want to consult with professionals.
Selecting a reputable clinic on your testosterone remedy is crucial.
At Testosterone treatment Clinic, our medical professionals have intensive expertise in treating low
testosterone levels and hypogonadism. We use the most recent expertise and
methods to ensure that our sufferers receive high-quality care.
There are many misconceptions about testosterone substitute therapy.
Low ranges of testosterone can lead to fatigue, depression, muscle mass loss, low sexual drive,
and even osteoporosis. Rising testosterone with therapy can help to
reverse many of those symptoms and help people really
feel extra energetic and healthy. Hormone Concord Clinic is a testosterone
alternative remedy (TRT) clinic conveniently situated
in Lake Mary, MN. Our experienced physicians specialize in treating low testosterone
(low T) and hormone imbalance issues in males. We provide personalized therapy plans to revive health, vitality
and quality of life. At Present you can find multiple testosterone therapy service suppliers.
In addition, irritability and issue concentrating are additionally
widespread in people with low testosterone, however hormone therapy may help
to improve focus and focus. Lastly, people with low testosterone typically undergo
from fatigue, however hormone remedy may help to extend
power ranges and reduce fatigue. In quick, hormone remedy
could be an effective remedy for low testosterone, helping
to improve quality of life.
http://www.supergame.one/ · May 21, 2025 at 9:40 pm
Testing many individuals which were on testosterone alternative therapy for six months and six
years, they nonetheless come again to what their baseline was.
Whereas this can be true in some excessive instances I even have by no means seen this clinically.
This doesn’t suggest it won’t occur nevertheless it seems to be extra excessive instances.
The exact method to cease testosterone alternative therapy will
depend on your specific circumstances. Nevertheless, typically
suppliers will suggest weaning off the medicine by slowly reducing your dose over time.
This gradual cessation can help reduce side
effects and problems.
I Am currently making an inventory of causes not to damage your pure test manufacturing
from your twenties utilizing TRT. These early enhancements
are encouraging, but they are just the start of what TRT can do
on your health and well-being. TRT isn’t for everyone, but for the proper men,
it could be life-changing. The key’s working with a knowledgeable doctor who understands the science—not falling for fear-mongering myths.
Testosterone Replacement Therapy (TRT) is certainly one of the most misunderstood
therapies in men’s health.
I started at 150mg a week obtained to one hundred
eighty and T stage was 890 so I dropped right down to one hundred seventy and I prefer
it right here on this vary. No unwanted effects apart from excessive libido and
desirous to go to the health club constantly. It’s been nice and
just wanted to share my experience for those on the fence.
As Quickly As you determine to cease TRT you might ask if it’s protected to stop it
abruptly or if there’s something particular you should do
to reset your physique. Do you want to do one thing to ensure everything is working the greatest way it was previous to starting, for instance?
The primary cause individuals ask this question is because of the feedback
loops between the testes, the pituitary, and the hypothalamus.
As Quickly As you start TRT, you’ll have regular appointments with
your healthcare supplier and routine blood checks. Together,
you and your healthcare provider will resolve if TRT is right for you.
Too much testosterone can intervene with ovulation and menstruation, a surplus on this hormone
be because of excessive ranges of insulin in the ovaries.
As well as irregular or absent intervals and weight acquire (due to the insulin resistance), excessive physique hair
and zits are also widespread indicators of high levels of testosterone.
This can help enhance the signs of low testosterone, like low libido and lack of power.
Certain present health conditions make it unsafe, like prostate most
cancers and coronary heart failure. Testosterone substitute therapy (TRT) is
an choice for men who have low testosterone levels as a result of male hypogonadism.
Once you begin testosterone remedy, your body will depend on it
to operate properly. If you suddenly cease taking testosterone, your
physique may experience a low testosterone degree
and should go into withdrawal. This can cause several disagreeable signs which will make it difficult for you to live a traditional life.
In this article, we’ll focus on the results of testosterone substitute
remedy and what happens should you cease.
In this text, we are going to try to spotlight, handle
and answer these questions as merely as attainable. Incorporating cardiovascular workout
routines steroids and cardio (http://www.supergame.one/)
weight coaching into your routine may have a optimistic impact on Testosterone manufacturing.
Common train has been shown to assist keep higher Testosterone levels over
time. To restart Testosterone manufacturing, it’s necessary to take a comprehensive strategy.
To transition smoothly, you’ll need to restart your HPTA axis under the steerage of a knowledgeable provider.
Not doing so can lead to more extreme low Testosterone symptoms
as your body loses its solely source of Testosterone.
Enhancements in diet, exercise, sleep, stress levels, and general well being may doubtlessly increase pure testosterone production,
leading some to rethink persevering with with TRT. While
TRT can bring about important advantages, it’s not with out
its potential drawbacks. Some people would possibly resolve
to stop TRT because of the side effects, which may
embody zits, oily skin, sleep apnea, and a rise in purple blood cell rely that can potentially lead to blood clots.
There’s also a threat of growing an enlarged prostate or
having a worsened existing prostate cancer.
The length of testosterone therapy will depend upon the
person and their specific circumstances. Some individuals
might solely want testosterone remedy for a brief time frame,
whereas others might require long-term treatment.
One potential consequence of TRT is the suppression of the body’s natural production of testosterone.
When exogenous testosterone is introduced into the physique by
way of TRT, the physique’s natural manufacturing of testosterone can decrease.
This is as a end result of the physique’s inside suggestions mechanisms sense the presence of sufficient testosterone and signal the testes
to lower production. For example, when the body detects excessive levels of testosterone within the bloodstream,
it signals the testicles to minimize back their production of the hormone.
This is as a result of the body acknowledges that there’s already an sufficient
provide of testosterone available and does not need to supply extra.
As a result, the testicles might shrink in size and their capability to produce testosterone could also be temporarily
impaired.
Stopping testosterone therapy abruptly can have unfavorable effects on the physique and general well-being.
Testosterone is a hormone that performs an important function within the growth and maintenance of male
characteristics. It is liable for many physiological processes within the
body, together with muscle development, bone density, mood regulation, and
intercourse drive. When testosterone levels drop all of a sudden,
it could possibly have opposed results on these areas. Low testosterone ranges
can result in numerous signs, similar to fatigue, depression, decreased libido, and loss of muscle mass.
Testosterone replacement therapy aims to revive hormone levels,
alleviating these signs and bettering quality of life.
If you’re considering testosterone therapy, you’re probably questioning
what is going to happen should you stop.
Beauty Fashion · May 22, 2025 at 9:30 am
Awsome post and straight to the point. I don’t know if this is actually the best place to ask but do you guys have any ideea where to get some professional writers? Thanks 🙂
telegra.ph · May 22, 2025 at 10:40 pm
And the ultimate impact generally happens elsewhere,
rather than in what’s tested in the laboratories. But there’s
one other way that these highly effective brokers can discover their method into people and other animals.
A substantial portion of the hormones literally passes by way of the cattle into their feces and
leads to the environment, where it could possibly get into other meals and consuming water.
In this review, we goal to overview the usage of sex Best steroid company; telegra.ph, priming in medical practice, highlighting the need to
develop acceptable pointers in order to overcome diagnostic pitfalls in peripubertal age.
Hormones are released upon stimulation that is of both chemical or neural origin. Regulation of hormone release is primarily achieved via adverse feedback.
Varied stimuli might trigger the release of hormones, but there are three main varieties.
Hormonal stimuli are changes in hormone levels that initiate or
inhibit the secretion of another hormone. Lastly, a neural stimulus occurs when a nerve impulse prompts the
secretion or inhibition of a hormone. Contemplating the slower effects of SARMS on the body, the minimal cycle length for
most SARMs should be eight weeks.
HGH is essential for body progress and development, aiding in cell restore and regeneration. Its
ranges are influenced by factors like brief bowel syndrome, and overproduction may result in insulin resistance.
Out There solely by prescription, HGH is crucial for maintaining wholesome bones, muscles, and organs.
In an animal study, it was shown that HGH stimulates the
liver into producing IGF-1, which is released into the physique to stimulate the production of cells
that are answerable for cell proliferation, elevated muscle mass
and elevated power.
Human growth hormone (HGH), produced by the pituitary gland, regulates development and metabolism.
Artificial HGH, which you will get by prescription, treats conditions like brief stature in kids and muscle-wasting
ailments in adults. Facet results may embody joint pain, swelling, carpal
tunnel syndrome, and the next likelihood of getting diabetes and cancer.
Natural methods to boost HGH might embody exercise, getting sufficient sleep, arginine supplements, and fasting, but
researchers should research this extra intently. Kids presenting
within the peripubertal period with short stature, decreased growth velocity or failure to bear a pubertal development spurt require endocrine evaluation. In such instances differentiating growth‐hormone deficiency (GHD) from non‐GH‐deficient constitutional delay of progress and puberty
(CDGP), idiopathic short stature (ISS) and different causes of quick stature is required.
Progress hormone stimulation tests (GHST) are required to diagnose GHD and are based mostly on the idea of a pharmacological agent acutely stimulating pituitary
GH secretion.
Here, we share all the benefits and unwanted aspect effects of progress hormones that
can assist you see the total image of their use and whether they’re right for you.
HGH, produced by the pituitary gland, plays a key position in body progress and improvement, doubtlessly increasing muscle mass and reducing fat.
The pituitary gland regulates HGH launch, and a few
people use dietary supplements to support its ranges [3].
HGH is almost always used in a stack because that’s where it’s
most useful. Steroid users will typically stack HGH
with Anavar for chopping and fats loss stacks.
Reverse phenotypic results are generally obtained when applying inhibitors of plant sterols and BR synthesis in each model crops and crops (see Supplemental Table 3 online).
High concentrations of metals, together with those essential for
progress, have a poisonous impact on plant metabolism. In cotton (Gossypium herbaceum),
fiber yield and high quality are the most important traits.
Some of my favorite MK-677 stacks are outlined here and embody
LGD-4033, Cardarine, RAD-140, and Ostarine.
Keep In Mind that one of many main results of Ibutamoren is
to increase your appetite, so it is smart to take it early within the
morning so you’re not coping with late-night hunger. Now it comes all the means down to how
you plan to use it and what results you specifically want to achieve that make Ibutamoren a more
sensible choice for you than SARMs, steroids, or even real HGH
itself. Copyright © 2022 Partenope, Galazzi, Albanese, Bellone, Rabbone and Persani.
These last two potential uses have acquired essentially the most
attention as abuse of growth hormone. While misused for aesthetic purposes, each substances have reliable medical purposes.
Artificial HGH is used as alternative remedy to deal with growth
hormone deficiency in youngsters and adults.
If you take HGH by mouth, your stomach digests it before your body can absorb
it. Lipid soluble hormones are capable of pass proper through the
target cell’s membrane. This binding activates the hormone, which then binds to
a portion of DNA inside the cell’s nucleus. Binding
to the DNA causes genes to show enzyme exercise on or off,
which alters the activity of the target cell.
They are synthesized from a 20-carbon amino acid called arachidonic acid.
They degrade very easily, which simply implies that they don’t hold around long.
What bothers me essentially the most is that, not like with testosterone, I’ve not found any exhausting evidence in the scientific literature to suggest that GH will enhance
performance in otherwise healthy males.
I advocate you assume twice (no, make that three or 4
times) earlier than you resolve to use SARMs or some other
compounds I’ve coated here. I hope you’ll be higher knowledgeable and in a more favorable place to no less than use
them as safely as potential. As I’ve stated, no SARM or research
chemical can ever be thought of protected for efficiency, bodybuilding, weight reduction, or any other objective.
Most SARMs and comparable analysis chemicals have little
scientific data on their safety. Some are adopted by way of with trials and
studies, but others are halted early in analysis.
Beauty Fashion · May 26, 2025 at 9:15 pm
Good day! I know this is kind of off topic but I was wondering if you knew where I could get a captcha plugin for my comment form? I’m using the same blog platform as yours and I’m having problems finding one? Thanks a lot!
Beauty Fashion · May 27, 2025 at 11:32 pm
An fascinating discussion is value comment. I think that it is best to write extra on this matter, it won’t be a taboo subject however generally persons are not enough to talk on such topics. To the next. Cheers
Illegal Steroids List · May 28, 2025 at 2:13 pm
For women excited about using Anavar to enhance their fitness routine, there
are a number of crucial methods to maximise the effectiveness
of this supplement. A finely tuned consuming plan offers
the physique the nutrients it needs to deal with the extraordinary workouts that accompany Anavar
use, making it possible to see quicker positive aspects and fat loss.
As with any steroid combination, it’s important to
know how the elements work collectively and be acquainted with the potential professionals and cons.
While the mix of Testosterone with Anavar can enhance a
user’s health goals, the additional dangers ought to always be taken into consideration. Moreover, conducting thorough analysis,
understanding your limits, and deciding based mostly on personal wants
is key to putting the proper stability between efficiency enchancment
and long-term well-being. When used with Anavar, Testosterone can enhance the outcomes that customers could additionally be seeking.
Women who use Anavar will, nonetheless, discover that
it might possibly add spectacular lean muscle positive aspects to the physique, and that is the principle anabolic
steroid that’s appropriate for ladies to make use of for this objective.
One compelling reason to match earlier than and after outcomes entails Oxandrolone’s potential impression on muscle improvement.
While it isn’t essentially the most potent anabolic steroid out there, it’s
renowned for helping athletes construct lean muscle mass
and increase strength.
The main supply for purchasing liquid Clen is through scientific analysis web sites, however
at all times be aware that high quality can differ significantly between providers.
Hence, it’s important to hunt out only respected makers of liquid Clen. The difficulty in administering a precise dose is one
of the important downsides of liquid Clen. You can’t use a potent
drug like Clenbuterol and never have plenty
of adverse comments or complaints/concerns being shared.
Feminine users will usually be properly conscious of the downsides
of Clen, and frequent comments about jitters, anxiety, and
sleeping difficulty can be found.
Winstrol poses the next liver toxicity and aspect effect threat than Anavar, so
we can maintain this stack short. Doses are around half that of
what we’d usually use for each compound as a outcome of they are each oral steroids.
An important factor to consider when planning your Anavar stack is the numerous benefit of its lack of water retention as a end result of it doesn’t convert
to estrogen. You can use this by stacking it with
other compounds that don’t aromatize, like Trenbolone and Masteron. Such a stack can successfully have you ever not having to think about
fluid retention at all until you decide to take a better dose of testosterone
within the stack. We could examine Anavar with a long record of AAS and different PEDs if you’re attempting to
choose the most effective compound on your next cycle.
One Other Anavar stack for men is a pure slicing cycle and
consists of one other cutting-specialist steroid in Winstrol.
Winstrol is one of the greatest chopping compounds out there, and when combined with Anavar, it proves
to be a potent duo for final shredding. Girls can count on wonderful outcomes from an Anavar cycle,
including pretty energy positive aspects. You’ll be
lifting heavier weights and may discover your lifting action improves with that strength enhance.
The basic rule when planning a cycle is that the higher the Anavar dose is,
the shorter the cycle you must be doing.
Anavar will result in an imbalance in HDL and LDL levels,
which will affect a user’s cholesterol profile. Although
Anavar is less cardiotoxic in comparison with most
anabolic steroids, it still has the potential to induce hypertension. For females, the risk of masculinization will increase when dosages exceed 10 mg per day or cycles surpass
4 weeks. The bodybuilding community refers to
Anavar as a cutting steroid commonly cycled during competitors preparation. Anavar has anabolic results; nonetheless, such properties are delicate in comparison with bulking Illegal Steroids List.
Amongst beginner weightlifters, a testosterone-only cycle is the
usual protocol.
When mixed with a balanced diet and common exercise regimen, the effect
of Anavar on fats loss is usually vital. One notable observation within the initial couple of weeks
is a rise in power. Whereas there is probably not an explosive development in muscle dimension simply but,
bodybuilders usually observe a considerable enchancment of their functionality to carry heavier weights and do more intense workouts.
Anavar, on this method, helps kick up the stamina,
getting ready the body for the journey ahead. Anecdotal reports
recommend minimal unwanted effects, however overuse could potentially lead
to decreased stress response, fatigue, and low blood pressure because of chronically low cortisol ranges.
Unfortunately, such a combination is especially designed
for skilled bodybuilders with sensible data of biking such harsh steroids.
However it’s not the case to be dissatisfied because there are more environment
friendly Trenbolone cycles.
However, Nolvadex and Clomid can worsen progesterone-related unwanted side effects.
As a consequence of an increase in progesterone, a hormone that is similar to estrogen, Deca Durabolin has the potential to trigger gynecomastia.
Thus, we usually monitor patients’ nipples during this stack,
and in the event that they start to turn into swollen or breast tissue
enlarges, then we administer an AI to prevent further hypertrophy.
Total, the NPP and Sustanon 250 cycle is an effective way
to bulk up shortly, but you will need to concentrate on the potential unwanted aspect effects before starting this or any
other steroid cycle. Stacking is extremely frequent within the bodybuilding world, and stacking
Testosterone with Winstrol is a very common combination in both the
power and weight loss neighborhood. This is where you start feeling and seeing the consequences
of the cycle with reference to the way it helps you within the fitness center.
Steroids drug classification · May 29, 2025 at 8:35 pm
With this potent steroid, higher doses would mean extra
serious unwanted facet effects. Thus, it is not often run, usually and usually only by experienced steroid users.
The under Winstrol cycle is optimal for somebody who’s already taken Winstrol or
milder steroids, similar to testosterone or Anavar.
This will assist your physique adjust to the drug and
minimize the chance of side effects. All in all, should you’re trying
to take your bodybuilding recreation to the next degree, a Trenbolone cycle is unquestionably the way to go.
Every particular person’s response to steroids is completely different, so it is onerous to
say exactly what you’ll experience when taking Trenbolone.
Focus on establishing good habits, following a well-designed coaching program, and maintaining a balanced diet to realize lasting and desirable
outcomes. This is a really strong and reliable Primobolan cycle for intermediate customers.
The oral variant of Primobolan is utilized right here, for
the purpose of proper demonstration to the reader of the way to make
the most of the oral variant correctly. Testosterone is the first to be defined right here, where it is relegated to a help position at a TRT (Testosterone Substitute
Therapy) dose of 100mg weekly. Utilizing Testosterone at such a low dose should also
negate any attainable amount of aromatization with out
the necessity for an aromatase inhibitor.
With a TRT dose of Testosterone and two primary anabolics that don’t convert into
Estrogen, this cycle is taken into account a really appropriate pre-contest or
chopping cycle.
Nonetheless, the Enanthate model has just lately become extra widespread for customers wanting a slower-release
type of Masteron (and less frequent injections). Masteron has been round because the late Nineteen Fifties,
developed as Drostanolone Propionate and utilized primarily as
a breast cancer remedy in females. The anti-estrogen effects
of Masteron made it suitable for this function as a end
result of estrogen contributing to the growth of these kinds
of cancerous tumors. Sadly, Primobolan is presumably the most faked steroid being bought in UGL labs at present.
All steroids possess both anabolic or catabolic properties in the physique.
Anabolic reactions, similar to muscle protein synthesis,
build mobile elements and complicated molecules; these reactions require power
input to proceed. Technically speaking, trenbolone isn’t aromatized by the body and doesn’t raise estrogen levels.
Larger doses or long-term usage of Primobolan does increase the risk of negative impacts on the liver.
There are no liver toxicity dangers with the injectable type of Primobolan. Hence,
your results come with out the bloated look brought on by
water retention, which is crucial for a cutting cycle,
significantly for competition. However much more so, they both come with the identical ester hooked up, to enable them to
conveniently be mixed and brought all within one single injection. Girls who use Primo at doses low sufficient to keep away from virilization will
discover that achieving a dry and outlined physique is the cornerstone
of a Primo cycle. This can take some time to develop, and girls must be keen to attend
around 5 weeks to start seeing noticeable physique advantages.
Working a 10-week cycle is an inexpensive objective for females, with doses up
to 50mg per week.
Individuals with some expertise with steroids would possibly
enhance their cycle by stacking, which entails combining multiple
Steroids drug classification for synergistic results.
Here, we define a exact roadmap of dosage parameters and cycle lengths,
tailored for different levels of steroid use. We will investigate how iconic
figures like Arnold Schwarzenegger and Ronnie Coleman may need approached
their cycles, acknowledging the era-specific contexts of steroid use.
Ronnie Coleman’s hulk-like physique and eight Mr. Olympia titles counsel a steroid-rich narrative.
The cause for this is that testosterone is a less poisonous
anabolic, so it could be stacked to enhance gains with out making trenbolone’s unwanted facet effects dramatically worse.
None of the next trenbolone cycles are suitable for beginners, as it’s a very harsh steroid
that causes severe side effects in lots of
customers. Trenbolone is considered one of the most potent anabolic
steroids, each in terms of results and unwanted aspect effects.
Hypothesis apart, what can’t be denied is that Schwarzenegger had a talent for bodybuilding.
His unmatched discipline and dedication to sculpting the proper
physique were potential as a end result of his iron will and,
partially, the measured use of Dianabol. The steroid helped stimulate protein synthesis, important for muscle progress and restore, which, in conjunction with his rigorous exercise and high-protein food regimen, propelled Arnold to bodybuilding stardom.
While the steroid trenbolone is renowned for its effectiveness, responsible use is
paramount.
An advanced Trenbolone cycle will always start at 100mg every
other day and infrequently and in plenty of circumstances creep its method into dosing ranges of 100mg
every single day throughout use. It targets biological targets of androgens like testosterone and dihydrotestosterone (DHT).
Additional, it has strong anabolic results and
extremely androgenic results to enhance masculine properties and muscle development.
For these new to Trenbolone, it is important to begin out with a conservative strategy.
Specialists recommend starting with a decrease dosage to allow your body to acclimate to the compound steadily.
This not solely minimizes the chance of potential side effects but in addition helps you
gauge your particular person response.
KAYSWELL · May 30, 2025 at 1:56 am
May I have information on the topic of your article? http://www.kayswell.com
Hairstyles · June 1, 2025 at 10:43 am
It’s my belief that mesothelioma is most fatal cancer. It’s got unusual qualities. The more I really look at it the more I am persuaded it does not conduct itself like a real solid tissue cancer. When mesothelioma is often a rogue viral infection, therefore there is the potential for developing a vaccine as well as offering vaccination for asbestos open people who are really at high risk regarding developing long term asbestos relevant malignancies. Thanks for discussing your ideas on this important health issue.
Dusty · June 1, 2025 at 3:51 pm
Thus, Dr. Ziegler’s intention wasn’t simply to create a
compound that was extra anabolic than testosterone but one that may also be much
less androgenic. He accomplished this with Dianabol’s androgenic
score of 60, in comparison with testosterone’s a hundred.
Dr. Ziegler famous that the Russian athletes were experiencing androgenic
unwanted facet effects during the 1956 Olympics (in Australia) when he discovered they had been experiencing difficulty urinating.
This was because of enlarged prostates brought on by the excessive conversion from testosterone to
DHT.
This stack was one of the most prominent steroid woman – Dusty –
cycles from the Golden Era, believed to have
been utilized by Arnold Schwarzenegger and different
traditional bodybuilders from the Nineteen Seventies.
This steroid cycle is a extra commonplace protocol amongst intermediate steroid users.
This combination of testosterone and Deca Durabolin is the least poisonous bulking stack
in our expertise. Intermediate users will commonly administer this stack
once their body comfortably tolerates testosterone-only cycles.
In Contrast To Anavar and testosterone, Dianabol is especially hepatotoxic; thus, some liver support should be taken throughout your cycle.
A recommended supplement is TUDCA (tauroursodeoxycholic acid), which we have seen successfully
decrease raised liver enzymes, decreasing hepatic stress.
The main objective of this cycle is to organize the body for the following cycle, which can yield bigger gains.
Even though Anavar is an oral compound (like testosterone undecanoate), it’s not significantly liver
toxic. In Anavar’s case, it’s because the kidneys assist to course of oxandrolone, decreasing the
hepatic toxicity and workload on the liver. The larger the testosterone dose, the upper the chance of a consumer creating gynecomastia.
Some people in bodybuilding consider that roid rage is
a fantasy; nonetheless, analysis exhibits that 60% of steroid customers
expertise a rise in aggressive behavior (28).
SERMs are able to restoring testosterone levels post-steroids, with tamoxifen and clomiphene being the most effective choices in our
expertise. Injectable Dianabol is an option for many who don’t
want to expertise liver points when taking this steroid.
Dianabol is usually an oral steroid; nonetheless, there are veterinary variations of
it out there that might be injected, immediately coming into your bloodstream and bypassing the liver.
Nevertheless, we discover injectable Dianabol to be much less common on the black market, with orals being the extra standard form of
administration.
This may be attributed to the rise in testosterone levels that anabolic steroids could cause.
Nonetheless, as with different side effects,
this elevated aggression will affect customers to totally different levels.
This might depend upon a person’s genetics and habits before
taking anabolic steroids. Thus, if a person is vulnerable to violent acts or homicide is present of their
family history, steroids such as Dianabol may exacerbate this.
They’re man-made variations of testosterone, a male intercourse hormone that helps
construct larger muscles. A doctor can legally prescribe them if your body would not make enough
testosterone. Doctors also prescribe them to men with low testosterone and people who lose
muscle mass because of cancer, AIDS, and different well being circumstances.
I really have been taking D-Bal MAX and have seen substantial enhancements in my strength and
power levels. Along with gaining muscle mass, I even have been in a
position to sustain my strength and power levels even throughout intense
training classes. I am highly happy with the results and advocate D-Bal MAX to anybody in search of a protected and efficient approach to construct muscle and
enhance power. Urine checks are carried out to examine for breakdown products of anabolic
steroids.
With Out this persistently high protein intake, progress will be restricted, and steroid use shall be
considerably wasted because you won’t get the desired results.
It’s not just protein you’ll be planning out – carbs and fat are simply as critical.
Since each muscle or muscle group recovers sooner after being
worked on, you probably can target each muscle far more often because
those restoration instances are significantly shortened.
That doesn’t imply overtraining or forgetting
about all-important rest and sleep, but you can fit as a
lot as twice as many exercises focusing on a muscle group into the identical interval.
An experimental research demonstrated that supraphysiological doses of AASs induce a decrease in MMP-2 exercise within the agonist leaping rat muscles [96].
It was advised that the vascular endothelial progress issue (VEGF) could play a
job in the mechanism concerned in skeletal train adaptation. VEGF expression was
reduced in rats who underwent ND administration and that is presumably related to MMP-2 activity dysfunction, since MMPs are involved in the regulation of VEGF extracellular shops [97].
Furthermore, the decreased expression of VEGF
could play a task in skeletal injury because of AASs, as a consequence
of poor transforming and poor vascularization [97]. The morphology
and the group of collagen fibers may be modified by bodily exercise.
Also, there’s a threat of users contracting HIV or hepatitis via intramuscular injections if needles
are shared. You can work out when a drug will depart your physique by 5.5 occasions the half-life.
Salicylic acid is another common pimples remedy; nonetheless, this is much less effective in comparability to
retinoids. Topical antibiotics are also an advantageous therapy for
acne, lowering infected lesions by 46-70% (27).
Clindamycin and erythromycin are two antibiotics
proven to be efficient; however, they shouldn’t be administered long-term (more than 30 days) to
reduce the possibility of the acne turning into proof against the remedy.
To keep away from such resistance, antibiotics ought to comprise benzoyl peroxide, which is able to further scale back irritation.
https://landgoedcampingwesterwolde.nl · June 1, 2025 at 4:02 pm
Sure, gaining lean muscle is among the major reasons females
use Winstrol. It is far more efficient for this purpose for girls than with male customers, and women can see wonderful gains inside just some weeks, even at very low doses of Winstrol, similar to 10mg per day.
How much muscle can be gained is dependent upon your Winstrol dose, other compounds you’re using, workouts, and diet.
The most critical feminine users, which can absolutely be those
in the bodybuilding subject quite than athletes,
are known to increase dosage to 15mg and even 20mg.
Additionally, larger doses will stress the liver and levels of cholesterol considerably
extra, requiring a cycle size at such excessive doses to be limited to just two to three weeks.
In such circumstances, the aim of high-dose Winstrol is nearly for contest preparation, with results coming on quick and powerful
within the two or so weeks earlier than the competition. The results
of Winstrol are more gradual than some other anabolic steroids, but they’re also
longer-lasting.
Oily pores and skin isn’t a really big issue, nonetheless, zits can be a matter of concern.
Some individuals could get too much zits all over their body while some might get very little pimples.
It doesn’t put any additional strain in your liver because
the Testosterone steroid is injected.
Underdosing or including different substances in a Winstrol
formulation means you will not get the expected results. Winstrol is probably certainly one of the hottest steroids on Earth, so nearly all suppliers will always have it in inventory.
It’s considered a comparatively low-cost anabolic steroid and is undoubtedly more reasonably priced than Anavar (to which it’s usually compared).
Optimistic experiences will come from those that reap the benefit of the onerous, dry, very toned physique that can be obtained
shortly with this steroid. There are hundreds
of joyful Winstrol customers, but as you may expect, some folks don’t
have such a positive expertise.
This discovery has led to bodybuilders purchasing clenbuterol illicitly and
using it in chopping cycles alongside different fat-burning steroids.
Nonetheless, we’ve discovered clenbuterol’s effects in people to
be somewhat dissimilar to those in animals.
This steroid can work properly in a chopping cycle by
serving to protect lean muscle tissue and power.
Nevertheless, anecdotally, we do not see the identical
muscle-building properties in people. Thus, an Anavar and
clenbuterol cycle could enhance fats loss while moderately increasing muscle hypertrophy and strength.
Anavar may be considered by some customers for a cycle, but novices must be prudent, because the drawbacks of utilizing anabolic steroids, similar to Anavar, can outweigh the potential benefits.
I’ve found that steroid cycles with Winstrol need to be
now not than 6-8 weeks as a outcome of it could wreak havoc on your levels of cholesterol.
Anavar, also referred to as oxandrolone, is an anabolic steroid chemically altered to
produce fewer androgenic (masculinizing) unwanted facet
effects. This makes it a favorite among female bodybuilders, physique opponents, and Instagram
health personalities.
Clenbuterol increases adrenaline ranges, thus shifting the body into fight-or-flight mode.
Consequently, blood move improves throughout
the physique as a survival mechanism. Nonetheless, it is
highly estrogenic, directly stimulating the
estrogen receptors. We have seen this trigger huge
quantities of water retention, particularly
when users’ diets comprise adequate quantities types
of Injectable steroids (https://landgoedcampingwesterwolde.nl) sodium.
Winstrol had gained FDA approval in the US however is now not
used there. Yes, ladies can take Winstrol but it’s important to watch out with the
dosage. The beneficial dosage for ladies is 5-10mg per day, and it is usually not really helpful to exceed this amount.
Winstrol may be taken orally or injected, with oral administration being the most common. Additionally, it’s essential to stay hydrated and to observe a healthy diet and train routine to maximize the
outcomes.
Nonetheless, Andriol does not cause any notable hepatic strain, based on long-term analysis.
A 10-year examine of men using Andriol observed no notable
improve in alanine transaminase (ALT) and aspartate aminotransferase (AST) ranges.
Anavar and trenbolone are anabolic steroids that
are vastly dissimilar; nonetheless, they’re occasionally stacked together during slicing cycles.
Scientists still aren’t certain precisely why or how this occurs, but essentially the most
believable principle is that the liver is very sensitive to anabolic steroids.
When it isn’t capable of break down the steroids—which
is the case with oral steroids like stanozolol—the
excess could cause liver injury and dysfunction.
However Masteron is the higher all-around
chopping steroid and the one you must use if you wish to
run a longer cut. Anavar is not going to provide
the kinds of joint troubles that Winstrol typically does, however Winstrol will give you a more significant improve in power.
Winstrol delivers a more grainy physique that provides that unique textured look, much more so than Anavar.
This kind of look isn’t everyone’s aim, so it comes
down to your aesthetic preferences. Although Anadrol causes
fluid retention, this stack is excellent as a pre-competition mixture as a outcome of
outcomes shall be full, dry, and ripped with mass added.
The key to lowering Anadrol’s fluid retention so you’ll have the ability to still
achieve a dry look on this stack is to keep your
sodium consumption very low through the cycle.
Thus, it causes notably less hepatotoxicity than different
orals such as Dianabol or Anadrol. We have discovered
Equipoise (boldenone) to be one of the least toxic steroids,
inducing gentle cardiotoxicity. Equipoise aromatizes,
albeit to not a high stage, thus providing some safety to
HDL levels of cholesterol, preserving them comparatively excessive.
Appliance Repair Manual · June 4, 2025 at 12:30 am
Howdy! I know this is somewhat off topic but I was wondering if you knew where I could get a captcha plugin for my comment form? I’m using the same blog platform as yours and I’m having problems finding one? Thanks a lot!
Appliance Repair Manual · June 5, 2025 at 8:33 pm
One thing is always that one of the most frequent incentives for making use of your credit cards is a cash-back as well as rebate present. Generally, you get 1-5 back for various expenditures. Depending on the credit cards, you may get 1 back on most buying, and 5 back on buying made going to convenience stores, filling stations, grocery stores as well as ‘member merchants’.
Hairstyles · June 6, 2025 at 7:32 pm
There are some interesting closing dates in this article however I don抰 know if I see all of them middle to heart. There is some validity however I will take maintain opinion until I look into it further. Good article , thanks and we want extra! Added to FeedBurner as well
Ollie · June 8, 2025 at 12:54 pm
70918248
References:
what is the most powerful steroid (Ollie)
Mickey · June 8, 2025 at 11:39 pm
70918248
References:
animal steroids for sale (Mickey)
https://www.mediahalchal.in/home/2019/09/01/10-time-more-fine-For-violating-traffic-Rules-in-lucknow · June 8, 2025 at 11:53 pm
70918248
References:
steroids without lifting (https://www.mediahalchal.in/home/2019/09/01/10-time-more-fine-for-violating-traffic-rules-in-lucknow/)
Appliance Repair Manual · June 9, 2025 at 9:03 am
Great ?I should definitely pronounce, impressed with your site. I had no trouble navigating through all the tabs as well as related information ended up being truly easy to do to access. I recently found what I hoped for before you know it at all. Reasonably unusual. Is likely to appreciate it for those who add forums or something, web site theme . a tones way for your customer to communicate. Excellent task..
Appliance Repair Manual · June 9, 2025 at 11:07 pm
One thing is that when you are searching for a student loan you may find that you’ll need a co-signer. There are many cases where this is true because you will find that you do not possess a past credit standing so the mortgage lender will require that you’ve got someone cosign the credit for you. Great post.
Beauty Fashion · June 11, 2025 at 11:53 am
I really appreciate your help http://www.ifashionstyles.com
https://Thesecondbestblog.com/unlock-your-potential-with-these-inspiring-ebooks · June 11, 2025 at 6:20 pm
70918248
References:
steroid definition (https://thesecondbestblog.com/unlock-your-potential-with-these-inspiring-ebooks/)
India · June 12, 2025 at 4:47 am
70918248
References:
best steroid for weight gain [https://lankaexotiquevoyage.com/category/adventure-and-spot/]
www.Sardegnatrips.com · June 12, 2025 at 11:38 am
70918248
References:
muscle Building drugs list – https://www.sardegnatrips.com/2023/01/26/five-public-sector-trends-in-ecosystem-services/ –
https://www.remotlyworking.com/ · June 12, 2025 at 6:13 pm
70918248
References:
anabolic steroid dianabol – https://www.remotlyworking.com/snowboarding-what-no-one-is-talking-about/,
Virgil · June 12, 2025 at 8:38 pm
70918248
References:
using steroid; https://community.decentrixweb.com/index.php/question/why-are-the-british-confused-about-us-calling-bread-rolls-biscuits-when-they-call-bread-rolls-puddings/,
binance · June 13, 2025 at 5:58 pm
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
Charles · June 14, 2025 at 1:30 pm
70918248
References:
none (https://goldensparrowcs.net/2022/05/18/sources-for-digital-marketing/)
none · June 15, 2025 at 5:09 am
70918248
References:
https://askease.com/question/do-you-think-ai-tools-like-chatgpt-are-helping-or-hurting-students-in-education/
Hairstyles Near Me · June 15, 2025 at 7:30 am
Hello there! Would you mind if I share your blog with my zynga group? There’s a lot of people that I think would really enjoy your content. Please let me know. Thank you
Www.Forum.Myjane.Ru · June 15, 2025 at 9:26 am
70918248
References:
None; http://www.forum.myjane.ru/weblog.php?w=4020&previous=0&month=4&year=2024,
Appliance Repair Manual · June 18, 2025 at 9:42 am
Thanks for discussing your ideas here. The other point is that each time a problem appears with a personal computer motherboard, folks should not take the risk with repairing this themselves for if it is not done correctly it can lead to permanent damage to the full laptop. It is almost always safe to approach any dealer of any laptop for the repair of the motherboard. They’ve got technicians that have an knowledge in dealing with notebook motherboard challenges and can have the right analysis and perform repairs.
Https://Guardian.Ge · June 30, 2025 at 4:21 pm
70918248
References:
Best Steroid For Lean Muscle Mass, https://guardian.ge/61512-nato-warns-of-military-challenge-posed-by-china.html,
https://www.cartergroupland.com/Articles/this-tract-offers-scenic-views-merchantable-timber-and-ashburn-ga · June 30, 2025 at 5:25 pm
70918248
References:
best anabolic steroids for muscle mass (https://www.cartergroupland.com/articles/this-tract-offers-scenic-views-merchantable-timber-and-ashburn-ga)
Carma · June 30, 2025 at 6:38 pm
70918248
References:
anabolic steroid cream for sale (https://talukadapoli.com/travel/listing/suvarnadurg/)
https://lumienhall.ru/news/keramicheskie-lyustry-lumien-hall · June 30, 2025 at 7:47 pm
70918248
References:
women bodybuilders on steroids (https://lumienhall.ru/news/keramicheskie-lyustry-lumien-hall/)
binance Препоръчителство · July 13, 2025 at 4:07 pm
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
Pepspray.Com · July 25, 2025 at 12:20 pm
mummys gold casino
References:
https://pepspray.com/legge-spray-peperoncino-italia/
guardian.ge · July 25, 2025 at 12:37 pm
gila river casinos
References:
https://guardian.ge/58665-uganda-veteran-leader-yoweri-museveni-declared-election-winner.html
https://talukadapoli.com/Travel/listing/durvankur-cottage · July 25, 2025 at 1:46 pm
stations casinos
References:
https://talukadapoli.com/travel/listing/durvankur-cottage/
englishmoral.Com · July 25, 2025 at 2:10 pm
coral casino santa barbara
References:
https://englishmoral.com/choose-your-pc-power-supply-when-you-are-a-gamer/
3l bet · July 29, 2025 at 8:09 am
Loved the points you made here.
betio · July 29, 2025 at 9:12 pm
Loved the points you made here.
bet9 · July 29, 2025 at 10:16 pm
Exactly what I needed today.
tv bet · July 29, 2025 at 11:20 pm
Loved the points you made here.
aria resort · July 29, 2025 at 11:43 pm
Aproveite a oferta de boas-vindas do https://580-bet.com e receba um bônus de 100$ ao se inscrever! Este bônus exclusivo é perfeito para novos jogadores que desejam experimentar todos os jogos que o cassino oferece. Seja em slots, roletas ou blackjack, você terá mais oportunidades de ganhar com esse bônus extra. Cadastre-se hoje mesmo e aproveite essa promoção incrível. Comece sua jornada de apostas no https://580-bet.com com 100$ a mais em sua conta para testar sua sorte!
55bmw · July 30, 2025 at 12:01 am
O https://luck-2.com está oferecendo um bônus de 100$ para novos usuários que se inscrevem no site! Isso significa que você pode começar a jogar seus jogos favoritos com um saldo extra, aumentando suas chances de ganhar. Se você é fã de slots, roleta ou blackjack, esse bônus é a oportunidade perfeita para explorar mais opções e testar suas estratégias. Cadastre-se no https://luck-2.com hoje e aproveite o bônus de boas-vindas de 100$ para aproveitar ao máximo sua experiência de apostas online!
sbobet · July 30, 2025 at 1:09 am
Get the full story https://rocket-us.com
voice-of-cnc.com · August 1, 2025 at 12:13 pm
Take a look at this page https://1.aqgzs.vip/pk/?rolex-casino-game-download
x9w.top · August 1, 2025 at 12:51 pm
Discover the details https://clubwebsolutions.com/pk/?casino-777
felix.world · August 1, 2025 at 1:42 pm
Visit this blog https://www.dogoodproductions.com/pk/?monte-carlo-casino
sujie520.cn · August 1, 2025 at 1:44 pm
Take a look at this page http://gh16.top/pk/?x-casino
https://neurotrauma.world/tb-500-peptide-injections-benefits-dosage-and-risks · August 5, 2025 at 3:24 pm
References:
anabolic and hyperbolic are the two main types of steroids. – https://neurotrauma.world/tb-500-peptide-injections-benefits-dosage-and-risks –
Web page · August 6, 2025 at 3:07 am
Well expressed without a doubt. .
References:
https://skitterphoto.com/photographers/1148180/deal-cleveland
https://rentry.co · August 7, 2025 at 8:12 pm
what is considered a high roller at a casino
References:
what is a vip high roller (https://rentry.co/cby8kksu)
valley.md · August 9, 2025 at 1:59 pm
References: dianabol primobolan cycle https://www.valley.md/dianabol-cycle-benefits-and-risks
monjournal.top · August 9, 2025 at 7:19 pm
dianabol and testosterone cycle for beginners
References:
10mg Dianabol cycle (https://monjournal.top/item/297373)
muhammad-ali.com.az · August 10, 2025 at 11:06 am
dianabol anavar cycle
References:
dianabol only cycle results (https://muhammad-ali.com.az/user/stickbook4/)
sciencebookmark.top · August 11, 2025 at 3:33 pm
hgh preis pro einheit
References:
hgh before and After pic (https://sciencebookmark.top/item/304335)
Sign Up · August 18, 2025 at 4:56 pm
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://www.binance.info/ro/register?ref=V3MG69RO
taking steroids without working out · August 19, 2025 at 2:37 pm
Women who are snug with greater doses of Anavar and who don’t endure virilization results can think about adding one other 5-10mg to the Anavar dose suggestion above. The different extremely popular cutting steroid for women, subsequent to Anavar, is Winstrol (Stanozolol). Few steroids will have us intently looking at both male and female cycles, however Anavar is an exception.
Anavar is the most typical counterfeit anabolic steroid we now have encountered. This is due to an absence of pharmaceutical-grade merchandise out there, thus more reliance on UGL versions. Moreover, the value of Anavar is very high, resulting in fraudulent sellers reducing the quantity of oxandrolone or removing it completely in trade for a cheaper substance. Despite the above protocol being effective, DHEA is the official medical therapy prescribed to ladies for low androgen levels. Anavar’s half-life can increase past this vary, depending on the age of the person. For occasion, its half-life can be as excessive as thirteen.three hours within the aged (23). Thus, if we state the half-life as 10.four hours, a post-cycle therapy protocol ought to start 57 hours after the final dose.
It’s a good way to remain motivated and maintain observe of your overall progress. Anavar is not legal in lots of international locations for recreational use or for bodybuilding without a prescription. In the us, it’s thought-about a controlled substance, and possession and not using a prescription can have critical legal consequences. Utilizing performance-enhancing medication also raises ethical issues, as it can provide you an unfair advantage in sports activities or competitions. Be mindful of how your selections might affect the fairness and integrity of the competitions you participate in. While we understand the desire to excel, it’s essential to do so in a way that aligns with your values and the law. Asana Recovery helps individuals who could also be grappling with substance-related decisions.
The downside to using Anavar repeatedly is that testosterone suppression could be exacerbated, whereas LDL levels of cholesterol stay elevated for a sustained time frame. Consequently, a person’s natural testosterone production will take longer to recuperate when lastly coming off Anavar. Clenbuterol is typically known as a chopping steroid like Anavar.
Stay focused, keep disciplined, and benefit from the course of of remodeling your physique safely and effectively. If a person’s body fat share appears to have increased on Anavar and they have not been overeating, then the energetic substance could also be Dianabol. We have found clenbuterol to trigger cardiovascular pressure in some users, probably causing myocardial injury (33).
If your body fat could be very excessive (or you’re a higher-weight person), it’s best to try and lose as a lot weight as attainable earlier than using a steroid – do not forget that Anavar isn’t a weight reduction miracle drug. Ideally, you’ll want to already be round 15% physique fats earlier than utilizing Anavar. These can be a few of the most debilitating and physique-ruining unwanted effects of steroid use and embody bloating or water retention and gynecomastia. You can anticipate nice dry features without estrogenic unwanted effects until you embrace other aromatizing steroids in your Anavar stack. Females can get hold of strength and lean positive aspects at low doses, and stacking Anavar with another sort of compound known as Ostarine (a SARM) can result in outstanding outcomes with minimal unwanted effects. All of those stacks would require a post-cycle therapy protocol afterward. A standard PCT is Clomid at 100mg day by day, starting two weeks after your final dose.
Right Here is a stable Anavar slicing stack that includes Clenbuterol and HGH. Anavar at 10mg/day for 6-8 weeks is nice, and you probably won’t have any unwanted side effects. As for the best time to take Oxandrolone, break up it into two doses every day at 5mg/each (once with breakfast and again earlier than bedtime).
This can often feel like a locking, cramping sensation inside the muscle that may last for a number of minutes or hours. Consequently, the person could not be capable of end their workout due to extreme discomfort. This is because of water filling inside the muscle cell and fluid being expelled outdoors the muscle cell.
Anavar will enhance your endurance to an extent, with a noticeable capability to work out for longer and at the next intensity22. This is invaluable while cutting, the place you’ll want to push yourself with cardio workouts to burn fat. Like all AAS, Anavar will positively affect your recovery, speeding up tissue therapeutic. With its recognized benefits on collagen synthesis (after all, Anavar was initially developed to advertise healing), it could scale back soreness and ache post-workout.
But compared to injectable https://www.valley.md/anavar-dosage-for-men, oral steroids will take longer to clear from the liver, and that’s where the attainable threat lies for liver stress or liver injury. Anavar is vastly popular with feminine customers, however ladies do not require the kind of post-cycle therapy that males do after an Anavar cycle. Winstrol poses a higher liver toxicity and facet impact danger than Anavar, so we can keep this stack brief. Doses are around half that of what we’d usually use for each compound as a result of they’re both oral steroids. An important factor to contemplate when planning your Anavar stack is the numerous good factor about its lack of water retention as a result of it doesn’t convert to estrogen.
oral Dianabol Cycle · August 20, 2025 at 11:23 am
deca dianabol test cycle
References:
https://digitaltibetan.win/wiki/Post:Deca_Durabolin_Cycles_4_Greatest_Cycles_From_Newbie_To_Superior
Melvina · August 21, 2025 at 2:59 am
dianabol and testosterone cycle
https://sfenglishlessons.com/members/raingalley5/activity/297682/ Dianabol 50Mg Cycle
http://csmouse.com/user/painagenda78/ Dianabol cycle Guide
https://f1news.space/item/402842 valley.md
http://sitamge.ru/index.php?subaction=userinfo&user=cookwater9 Valley.Md
https://my.vipaist.ru/user/mapporch4/ dianabol side effects after one cycle
https://stack.amcsplatform.com/user/chestmouse1 valley.md
https://holdt-boyd-2.federatedjournals.com/dianabol-and-take-a-look-at-cycle-information-outcomes-and-dosage 4 Week Dianabol Cycle
https://torrentmiz.ru/user/driverphone9/ what to take with dianabol cycle
https://pad.fs.lmu.de/pIuRNxylQE6QrFeKH3XjIw/ first dianabol cycle
https://promovafacil.com.br/user/profile/200364 dianabol Only cycle
https://medknigki-v-ulan-ude.ru/user/speararm7/ how to cycle dianabol
https://motionentrance.edu.np/profile/bowlpine38/ valley.md
https://www.giveawayoftheday.com/forums/profile/1082787 dianabol cycle before and after
https://sciencebookmark.top/item/296376 valley.Md
https://thefreeadforum.top/index.php?page=user&action=pub_profile&id=697501 dianabol anavar cycle
https://apunto.it/user/profile/36846 steroid dianabol cycle
https://hikvisiondb.webcam/wiki/Dianabol_Before_And_After_Outcomes_Benefits_And_Security_Guide sustanon and dianabol cycle
https://torrentmiz.ru/user/colonyradar1/ dianabol side effects after one cycle
References:
dianabol cycle only (https://xn--80aaaokoti9eh.xn--p1ai/user/eventyarn8/)
winstrol dianabol cycle · August 21, 2025 at 4:13 am
dianabol testosterone cycle
https://rentry.co/ut8bveyd valley.Md
https://www.generation-n.at/forums/users/trainsale1/ dianabol cycle guide
https://case.edu/cgi-bin/newsline.pl?URL=https://www.valley.md/dianabol-cycle-benefits-and-risks anavar and dianabol cycle
https://xn—6-jlc6c.xn--p1ai/user/quitearth27/ valley.md
https://thefreeadforum.top/index.php?page=user&action=pub_profile&id=697193 dianabol stack cycle
https://doc.adminforge.de/P5eshMNpQ-KiK4DMPt6HGA/ Winstrol and dianabol cycle
https://moyabalashiha.ru/user/profile/396914 4 week dianabol cycle
https://ebra.ewaucu.us/index.php?page=user&action=pub_profile&id=460950 Valley.Md
https://gratisafhalen.be/author/firedchard74/ test e and dianabol cycle
https://hangoutshelp.net/user/bookchange2 Dianabol Only Cycle Results
https://enregistre-le.top/item/405075 dianabol testosterone cycle
https://panoptikon.org/user/ownerpine32/ how long is a dianabol cycle
https://atavi.com/share/xebssyzryfmv Valley.Md
http://humanlove.stream//index.php?title=hamrickhull6876 dianabol and testosterone cycle
https://prosto-robota.com.ua/user/profile/356221 Dianabol Cycle Results
https://enregistre-le.space/item/299929 dianabol cycle for beginners
https://zenwriting.net/mileatom9/sustanon-250-cycle-guide-top-6-stacks-with-dosages dianabol stack Cycle
https://hedge.someserver.de/Airj-KbqQ9Kzb0rY-BcWSQ/ Valley.Md
References:
https://md.un-hack-bar.de/pmfCHXcDRcOqJl3MkapuLw/
dianabol and testosterone cycle for beginners · August 21, 2025 at 4:43 am
anavar and dianabol cycle
https://doodleordie.com/profile/stonechurch9 Dianabol Stack cycle
https://panoptikon.org/user/spidervise2/ Valley.Md
http://srv29897.ht-test.ru/index.php?subaction=userinfo&user=eightmark63 how to take dianabol first cycle
https://noticias-sociales.site/item/448139 dianabol deca test cycle
https://noticias-sociales.top/item/445370 dianabol stack cycle
https://securityholes.science/wiki/The_Last_Word_Information_To_Steroid_Cycles_The_Means_To_Safely_Use_Steroids_For_Optimal_Results sustanon deca dianabol cycle
https://historydb.date/wiki/Dbol_Cycle_Information_To_Stacking_Dosages_And_Unwanted_Side_Effects Valley.Md
https://apunto.it/user/profile/103117 4 week dianabol cycle
https://oren-expo.ru/user/profile/355953 winstrol dianabol cycle
https://ibsemiahmoo.ca/members/stamppipe9/activity/835683/ Dianabol And Deca Cycle
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=appledrain0 Dianabol And Winstrol cycle
https://newsagg.site/item/444530 anavar dianabol cycle
https://moparwiki.win/wiki/Post:Dianabol_6_Week_Cycle_Dbol_Dosage valley.md
https://lejournaldedubai.com/user/courtfight6/ valley.Md
https://pin-it.space/item/445671 dianabol dosage cycle
https://pad.geolab.space/7IwiQ4TLSoCeTmRkDllJaw/ dianabol cycle side effects
https://xn--41-4lcpj.xn--j1amh/user/errorlayer4/ dianabol winstrol cycle
https://ajarproductions.com/pages/products/in5/answers/user/sproutavenue11 Deca Dianabol Cycle
References:
https://algowiki.win/wiki/Post:Trenbolone_Acetate_An_Overview
Lane · August 21, 2025 at 5:49 am
sustanon deca dianabol cycle
https://scientific-programs.science/wiki/Anabolic_Fundamentals_For_Newbies_The_Guide dianabol and winstrol cycle
https://www.metooo.es/u/68a3f2b835eff41f982ff3e8 dianabol cycle (http://giscience.sakura.ne.jp/pukiwiki/index.php?kvistnieves277000) before and after
https://lejournaldedubai.com/user/branchapril9/ anavar and dianabol cycle
https://intensedebate.com/people/glovebobcat80 dianabol side effects after one cycle
https://www.metooo.io/u/68a3f18bd2561309a55dfe78 dianabol first cycle
https://www.instapaper.com/p/16772022 testosterone enanthate and dianabol cycle
https://md.darmstadt.ccc.de/M_hlDnlUT2qPdYo5icrIaQ/ what to take after dianabol cycle
https://topbookmarks.cloud/item/446293 dianabol oral cycle
http://cqr3d.ru/user/nametaxi5/ dianabol and anavar cycle
https://nerdgaming.science/wiki/Check_And_Tren_Cycle_Complete_Information_Advantages_Dosage_And_Dangers dianabol tren cycle
https://play.ntop.tv/user/periodpot4/ winstrol dianabol cycle
https://gratisafhalen.be/author/deadcomma3/ valley.md
https://test.annelertoplandik.com/user/artgander4 Valley.md
https://pad.fs.lmu.de/hLiOw2XtTLq8aBu_33IMxQ/ Dianabol And Test Cycle
https://mes-favoris.top/item/446652 post cycle therapy for dianabol
http://hikvisiondb.webcam/index.php?title=finksims6646 dianabol post cycle
https://clinfowiki.win/wiki/Post:Dbal_Max_Introduces_Authorized_Dianabol_Pills_For_Muscle_Growth what to take after dianabol cycle
https://xn--41-4lcpj.xn--j1amh/user/mealoctave30/ sustanon dianabol cycle
Wehrle · August 21, 2025 at 2:23 pm
hgh nebenwirkungen team andro
https://shmingle.com/employer/wachstumshormon-norditropin/ 5 iu hgh per day results
https://job.lewebpreneur.com/employer/somatropin-kaufen-hilma-biocare-100-i-u-hgh-somatotropes/ how much hgh should i take a day
https://rentry.co/67267-somatotropes-hormone-kaufen-hygetropin-wachstumshormone hgh before and after photos
https://ijb.org.in/employer/hgh-human-progress-hormone-wachstumshormon-on-line-kaufen-bestellen-100-echte-steroide/ dangers of hgh
https://bezraboten.com/employer/hgh-somatropin-liquid-pen-90-iu-hilma-biocare-kaufen-preis-295-euro-online-in-deutschland/ how much hgh should i take a day
https://sushantassociates.com/employer/wachstumshormon-hgh-and-peptide-kaufen-sie-legale-hgh-in-deutschland hgh vorher nachher
https://aparca.app/ricklebron188 hgh vs testosterone For fat loss
http://linkybe.com/elizabetnewqui bodybuilding hgh Cycle
https://jobsrific.com/employer/wachstumshormone-hgh-somatropin-kaufen/ hgh before and after photos
https://smartgateconsult.com/employer/kaufen-hgh-deutschland-hgh-on-line-zu-verkaufen/ testosterone hgh cycle
https://jobs.colwagen.co/employer/qomatropin-hgh-pharmaqo-kaufen-in-apotheke-online-im-gonadotropinlegal-com/ hgh vs testosterone for muscle
https://ejstaffing.ca/companies/crazybulk-hgh-x2-erfahrungen-muskelaufbau-kraft-bewertung-2025/ Somatropinne Hgh review
https://www.mvacancy.com/companies/soma-max-somatropin-kaufen-preis-342-euro-in-deutschland-dosierung-und-kurs/ hgh wieviel einheiten
https://jobsforfiji.com/companies/wachstumshormone-hgh-somatropin-kaufen/ hgh Vs testosterone bodybuilding
https://cipher.lol/samiraparkin38 how many iu of hgh per day
https://wadhefa.site/companies/wie-nimmt-man-wachstumshormon-hgh-ein,-kaufen-on-line/ hgh before and after pictures
https://short-ly.site/moshegoldfinch how much hgh should i take a day
https://krishnacareers.com/employer/prohormone-kaufen/ hgh cycle dosage
References:
https://3ii.de/louiewagoner9
hgh vs testosterone for fat loss · August 21, 2025 at 3:10 pm
hgh dose bodybuilding
https://swav.sa/employer/10-oh-hhc-vape-10-oh-hhc-einweg-e-zigarette-10-oh-hhc-vape-pen/ Wie Schnell Wirkt Hgh
https://vlvcard.dk/numbersmcmurra hgh dose bodybuilding
https://vagyonor.hu/employer/s2-wachstumshormon-hgh-ssi/ is hgh better than testosterone
https://hibastyle.com/rubye198611555 wehrle
https://huntapp.in/employer/steroide-kaufen-holland-hgh-pen-kopen/ wehrle
https://cut.gl/eileenfitzwate Hgh Für frauen
https://academicbard.com/employer/wachstumshormon-hgh-wirkung-nebenwirkungen-arginin/ wehrle
https://urlshorter.xyz/judeatkins sytropin hgh oral supplement spray
https://hibastyle.com/rubye198611555 Wehrle
https://www.klaverjob.com/employer/wachstumshormon-hgh-kaufen-anabole-steroide-kaufen-bestellen-on-line/ test and hgh cycle dosage
https://sushantassociates.com/employer/wachstumshormon-hgh-and-peptide-kaufen-sie-legale-hgh-in-deutschland hgh bodybuilding dosierung
https://bezraboten.com/employer/hgh-somatropin-liquid-pen-90-iu-hilma-biocare-kaufen-preis-295-euro-online-in-deutschland/ hgh 1 iu per day results
https://topdubaijobs.ae/employer/kaufen-hgh-deutschland-hgh-on-line-zu-verkaufen hgh dosage for injury recovery
https://aoreindia.com/employer/hgh-somatropin-100iu-10-ampullen-pulver/ hgh jintropin
https://parichay.me/jimmymcleish1 wehrle
https://codango.run/derrickorourke how much hgh for bodybuilding
https://short-ly.site/tyrellhawken0 hgh hormon abnehmen
https://gelijkwerk.nl/employer/astera-labs-wachstumshormon-hgh-injektionen-zu-verkaufen/ Hgh Hormon Bodybuilding
References:
https://prabeshgroup.pl/employer/hgh-wirkung-risiken-und-einsatz-von-somatropin/
Https://Chaakri.Com/ · August 21, 2025 at 6:14 pm
hgh 4 iu per day
References:
Hgh Legal Kaufen (https://chaakri.com/employer/rechtliche-scenario-von-anabolen-steroiden-in-deutschland/)
qrscopy.com · August 21, 2025 at 7:50 pm
testosterone and hgh
References:
hgh 4iu per Day results bodybuilding (https://qrscopy.com/melanie702607)
binance · August 22, 2025 at 12:57 am
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article. https://www.binance.info/en-IN/register-person?ref=UM6SMJM3
git.dgtis.com · August 22, 2025 at 11:06 pm
tren steroid results
https://syq.im:2025/cheri332465751 how to not gain weight on steroids
https://luvmatefreematrimony.com/@francesdrew06 wehrle
https://slowdating.ca/@kathaleen9337 Steroids For Bodybuilding For Sale
https://musixx.smart-und-nett.de/kristan7429901 wehrle
https://git.saidomar.fr/deidreh465208 masteron cycle dosage
https://git.daoyoucloud.com/erwinneudorf17 did the rock use steroids
https://git.expye.com/eldong08858644 how to start steroids
https://vcs.int.feuerwehr-ziemetshausen.de/eldenlenk75827 winstrol dosage for horses
https://gitea.chaos-it.pl/autumn23z04776 hgh reviews forum
https://hore-i-steigen.jimmyb.nl/antoniettanort after stopping steroids
http://git.bplt.ru/winnieboisvert best muscle enhancement supplements
https://radio.cuba7center.com/jeffrymclaughl Wehrle
https://git.cloud.leonclassroom.com/adapoulin7439 Reddit steroids before and after
https://git.palagov.tv/ilatiegs61736 Steroid Cost
https://forge.death.id.au/bernicebuckmas wehrle
https://aitnas.myasustor.com/angleawhitting How much Is trenbolone
https://home.zhupei.me:3000/archiedoherty tren for bulking
https://www.meikeyun.com/adakort4391415 anabolic steroid price
References:
long-term exposure to steroids can result in (http://git.dgtis.com/alysamackintos)
Valley.Md · August 22, 2025 at 11:35 pm
is jay cutler on steroids
References:
https://dating.hyesearch.com/@cortezlangley
dianabol for sale amazon · August 23, 2025 at 3:39 am
after taking steroids
References:
https://kayesbamusic.com/arronshupe285
Anabolic Steroids Prices · August 23, 2025 at 4:29 am
legal consequences of steroids
https://git.atomos.io/daringeach4784 What Are The Side Effects Of Coming Off Steroids
https://git.ajattix.org/catherinetribb metabolic steroids side effects
https://gitea.svc.obaa.cloud/jeanettehollin anabolic steroid use
https://git.thetoc.net/alivanderpool3 wehrle
https://git.hantify.ru/audreaschulz88 wehrle
https://xajhuang.com:3100/leonmauger941 wehrle
https://git.agusandelnorte.gov.ph/darby17v405817 What are anabolic Steroids?
https://wzpmc.cn:3000/demetrarohr585 Wehrle
http://gitea.dctpay.com/carrim15568991 anavar ingredients
https://git.9ig.com/brook29x128707 world abs pro stack review
https://jamdiggy.com/barrettmusselm anabolic steroids canada
https://git.penwing.org/cathernmain780 legal anabolic steroids
https://code.autumnsky.jp/miguelburnham2 difference between steroids and hgh
http://git.dgtis.com/alysamackintos other names for anabolic steroids
https://www.soundofrecovery.org/lorenzo74p284 which of the following is true about anabolic steroids?
https://luvwing.com/@janessamagnuso strongest muscle building supplement at gnc
https://sistemagent.com:8081/jaynewebb58258 consequences of not citing sources
https://dzmariage.com/@francescoe692 where to find steroids
References:
http://git.edazone.cn/marie444781294
binance konto skapande · August 31, 2025 at 12:13 am
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://www.binance.com/ur/register?ref=WTOZ531Y
valley.md · September 4, 2025 at 1:17 pm
revive – cjc/ipamorelin 9mg/15mg promo x 4 vials
References:
https://gitlab.ngser.com/klausbassett06/2468743/-/issues/1
notes.io · September 5, 2025 at 11:36 pm
ipamoreline prijzen
References:
ipamorelin peptide sciences [https://notes.io/wWz6t]
benefits of ipamorelin With Cjc-1295 · September 6, 2025 at 5:30 pm
cjc 1295 ipamorelin dosage schedule
https://languageschoolkenya.org/employer/cjc1295-ipamorelin-ghrp-2-dosage/ ipamorelin + cjc-1295
https://www.bestcasting.eu/Companies/dosage-benefits-research-overview-2024/ sermorelin ipamorelin side effects
https://klik.miledia.shop/aleciaburgmann Cjc 1295 Ipamorelin Before And After Female
https://www.ahrs.al/punesimi/ipamorelin-side-effects-dosages-administration/ valley
https://anychinajob.com/companies/cjc-1295-ipamorelin-10mg-blend-dosage-a-guide-to-combined-therapy/ valley
https://marine-courses.com/employer/cinnamon-health-benefits-uses-nutrition-and-side-effects/ Valley
https://skillrizen.com/profile/henryhamel2418 igf-1 lr3 mod grf ipamorelin
https://s.deinventive.com/latoshacorkill can ibuatmoren be used in combination with ipamorelin
https://academicbard.com/employer/ipamorelin-vs-sermorelin-comprehensive-comparison-and-guide/ Valley
https://url.pixelx.one/jkhsven1161969 what does ipamorelin plus semorelin do
http://hornjobs.org/employer/the-heart-of-the-internet canlab ipamorelin
https://url7x.com/aleciaciantar ipamorelin benefits reddit
https://tgtube.site/renatonolte656 valley
https://fancybox.qa/2025/09/04/ipamorelin-dosage-guide-what-to-know/ how does ipamorelin compare to other growth hormone-releasing peptides
https://nam.ovh/Ketza valley
http://www.grainfather.com.au/employer/cjc1295-ipamorelin-ghrp-2-dosage Ipamorelin cjc-1295 injections
https://edslink.us/ettamai4659472 cjc-1295 ipamorelin price per vial
https://divyangrojgar.com/employer/ipamorelin-the-complete-guide-to-this-growth-hormone-releasing-peptide/ Is ipamorelin right for me
References:
https://nonprofitsjobs.com/employer/ipamorelin-cjc-1295-peptide-combo-explained-for-growth-and-recovery/
can you inject ipamorelin after mixing bacteriostatic before refrigerating · September 6, 2025 at 11:24 pm
ipamorelin peptide dosage
References:
https://jobinaus.com.au/companies/cjc-1295-and-ipamorelin-benefits-risks-and-synergistic-effects/
schwanger.mamaundbaby.com · September 7, 2025 at 2:06 am
after injecting cjc 1295 ipamorelin my body gets hot
References:
cjc 1295 ipamorelin peptide injections, https://schwanger.mamaundbaby.com/user/minutevault86,
Gaye · September 7, 2025 at 6:40 am
dosage for cjc 1295 ipamorelin
https://www.tomahawknation.com/users/turan.mccarth revive – cjc/ipamorelin 9mg/15mg promo x 4 vials
https://output.jsbin.com/nukegexemu/ Sermorelin ipamorelin blend side effects
http://bioimagingcore.be/q2a/user/kittenengine7 Valley
https://support.mikrodev.com/index.php?qa=user&qa_1=foldgrape73 cjc 1295+ipamorelin
https://poiskpredkov.by/members/indexrock09/activity/1011044/ side effects of ipamorelin
https://classifieds.ocala-news.com/author/dinnercase2 can you mix sermorelin and ipamorelin
https://www.celticsblog.com/users/joseph.roed ipamorelin and recovery
https://atavi.com/share/xfpxpdzh9xfa cjc with ipamorelin for women
https://peatix.com/user/27703065 cjc-1295 no dac and ipamorelin blend
https://autovin-info.com/user/walkcomma62/ Ipamorelin Peptide Purchase
https://play.ntop.tv/user/pansycup72/ valley
https://noticias-sociales.site/item/462159 after injecting cjc 1295 ipamorelin my body gets hot
https://enoticias.site/item/338706 ipamorelin with dac
https://farangmart.co.th/author/crayoncello4/ Best Ipamorelin Stack
https://autovin-info.com/user/lossclef9/ ipamorelin peptide dosing
https://date.com.ng/members/picklepimple9/activity/215872/ ipamorelin and mk677
https://www.askmeclassifieds.com/user/profile/2830624 cjc-1295 ipamorelin dosage calculator
https://www.netsdaily.com/users/valentine.hwa how much Cjc ipamorelin should i take
References:
ipamorelin vs igf1 [https://www.sbnation.com/users/joseph.roed]
valley.md · September 7, 2025 at 10:54 am
ipamorelin cjc 1295 weight loss
References:
https://sushantassociates.com/employer/mk-677-vs-ipamorelin-a-comprehensive-comparison
findnearbyjob.com · September 7, 2025 at 2:35 pm
ipamorelin bacteriostatic water
References:
ipamorelin benefits reddit – https://findnearbyjob.com/employer/ipamorelin-cjc-1295-iam-clinic/ –
weight Loss ipamorelin and cjc stacked with Tirzepatide · September 7, 2025 at 5:28 pm
sermorelin vs tesamorelin vs ipamorelin
References:
http://jobs.recruithub.africa/profile/breannaandroni
https://posteezy.com/cjc-1295-ipamorelin-injections-ipamorelin-therapy-men · September 8, 2025 at 1:20 am
what are the bad side effects of cjc-1295 and ipamorelin
References:
cjc-1295 ipamorelin buy online (https://posteezy.com/cjc-1295-ipamorelin-injections-ipamorelin-therapy-men)
valley.Md · September 8, 2025 at 3:58 am
cjc 1295 ipamorelin mexico
References:
https://getshort.in/imashivers5629
valley · September 8, 2025 at 7:19 am
can you mix sermorelin and ipamorelin
https://www.lizyum.com/@ardverna139575 semaglutide and cjc 1295 + ipamorelin
https://emphira.app/@ulysseslandrum valley
https://gitea.systemsbridge.ca/deandremcgraw7 cjc 1295/ipamorelin injection site
https://git.esc-plus.com/georgettaberna https://isugar-dating.com/@rosalynfrost5
https://singlenhot.com/@quentinb46616 hgh vs ipamorelin
https://git.becks-web.de/guillermomesse valley
https://gitea.rodaw.net/birgitv7236048 ipamorelin and cjc 1295 before and after
https://love63.ru/@kayleighwhittl tesamorelin vs sermorelin vs ipamorelin reddit
https://repo.komhumana.org/paulinaarteaga ipamorelin to get skinnny
https://newborhooddates.com/@marjoriemenend cjc 1295 ipamorelin difference
https://git.pisci.eu/benjamin19y82 tesamorelin/ipamorelin blend
https://git.rootfinlay.co.uk/ionateakle8429 Ipamorelin Source
http://git.tinycio.com/mikaylabracewe does cjc-1295 ipamorelin increase testosterone
http://git.tinycio.com/mikaylabracewe how much bacteriostatic water Do you mix With ipamorelin
https://git.saret.dev/darrel70m34055 ipamorelin and forgot to refrigerate
https://music.1mm.hk/majorvarley591 minimum dosage of ipamorelin for effectiveness
https://gitea.mpc-web.jp/wioannette5768 where can i buy ipamorelin
https://gitea.cfras.net/hannamcroberts is ipamorelin a peptide
ipamorelin 9mg · September 8, 2025 at 10:55 am
tesamorelin cjc 1295 ipamorelin dosage
References:
https://abatsport.com/sermorelin-and-ipamorelin-peptide-blend-overview/
https://Jobs1.unifze.com/employer/ipamorelin-peptide-therapy-everything-you-need-To-know/ · September 9, 2025 at 11:06 am
how often do you inject cjc 1295 ipamorelin
https://jobrails.co.uk/employer/ipamorelin-peptide-dosage-benefits-side-effects/ ipamorelin inyectable
https://www.cbl.health/employer/ipamorelin-cjc-1295-dosage-synergistic-effects-for-growth-hormone-release/ cjc 1295 ipamorelin ghrp 2 blend
https://saek-kerkiras.edu.gr/employer/can-you-mix-sermorelin-and-ipamorelin/ cjc 1295 + ipamorelin blend dosage for weight loss
https://itsme.page/zlkilene55761 how many weeks can u take ipamorelin
https://www.keeperexchange.org/employer/sema-sermorelin-or-ipamorelin/ cjc-1295/ipamorelin before and after
https://renbrook.co.uk/employer/the-anti-aging-benefits-of-cjc-1295-and-ipamorelin/ cjc-1295/Ipamorelin blend
https://www.mazafakas.com/user/profile/7418145 valley
https://www.kayserieticaretmerkezi.com/employer/cjc-1295-peptide-benefits-dosage-risks-and-where-to-buy ipamorelin routes of administration
https://www.kamayuq.io/employer/understanding-mk-677-side-effects-what-you-need-to-know/ tesamorelin and ipamorelin blend dosage
https://careerworksource.org/employer/cjc-1295-vs-ipamorelin-which-peptide-delivers-the-best-muscle-gains/ difference between cjc 1295 and ipamorelin
https://posao.zumm.info/employer/cjc-1295-ipamorelin-side-effects-research/ mod grf Ipamorelin 10Mg Blend
https://spin.org.pk/employer/ipamorelin-peptide-therapy-at-the-renew-vitality-clinic-benefits-for-men-results-and-risks/ What Does Cjc-1295 With Dac Ipamorelin Ghrp-2 Do
https://mcn-kw.com/employer/tesamorelin-bodybuilding-dosage-chart-and-calculator/ sermorelin and ipamorelin stack dosage
https://biolink.belfiusolucoes.com.br/elenafaison308 valley
https://worldaid.eu.org/discussion/profile.php?id=1022036 ipamorelin dawkowanie
https://ntbk.tr/indianastrickl peptides ipamorelin cjc 1295
https://ofertyroboty.pl/employer/beyond-the-androgen-receptor-the-role-of-growth-hormone-secretagogues-in-the-modern-management-of-body-composition-in-hypogonadal-males/ valley
https://shorterin.com/vern76i6160544 is ipamorelin legal in usa
References:
Ipamorelin canada peptide (https://jobs1.unifze.com/employer/ipamorelin-peptide-therapy-everything-you-need-to-know/)
cjc 1295 + ipamorelin bodybuilding dosage · September 9, 2025 at 1:07 pm
%random_anchor_text%
http://gitea.liaozhuangkeji.com/aras2616720254 http://gitea.liaozhuangkeji.com
https://gitea.net50.ne.jp/melvinrichey13 https://gitea.net50.ne.jp/melvinrichey13
https://lovematch.com.tr/@shantellchave Lovematch.com.tr
http://newslabx.csie.ntu.edu.tw:3000/shannondeeds38 tesamorelin cjc1295 ipamorelin side effects
http://osbzr.com/merissaflannag http://Osbzr.Com
https://lesla.com/@janiemarion80 cjc and ipamorelin For sale
http://dating.instaawork.com/@wiltoncarr3423 pronounce Ipamorelin
https://git.dsvision.net/sherlynwelsh16 https://git.dsvision.net/
https://cheerdate.com/@kobyberg602018 Ipamorelin Fat Loss Study
https://git.enwatmon.de/ila69n61268960 Cjc-1295 with dac + ipamorelin + ghrp-2 Blend
http://wangchongwu.vicp.fun:3333/tiffanievering Wangchongwu.vicp.fun
https://worldclassdjs.com/shonarothstein Topical Ipamorelin
https://git.nightime.org/tessao45090414 https://Git.Nightime.Org
https://www.atmasangeet.com/debbraggz07490 http://Www.Atmasangeet.Com
http://gitea.liaozhuangkeji.com/denishabrydon valley
https://bondlii.com/@merri40h45843 Ipamorelin trouch
https://surily.in/walkerdarcy791 surily.in
https://filuv.bnkode.com/@hoseaj4901038 ipamorelin Information
References:
https://sound.descreated.com/lucilewentwort
https://datemeonline.Xyz/@millardaffleck · September 9, 2025 at 4:15 pm
ipamorelin peptide nasal spray
References:
can you take sermorelin and Ipamorelin together – https://datemeonline.xyz/@millardaffleck,
cjc 1295 ipamorelin heart rate · September 9, 2025 at 6:28 pm
sermorelin & ipamorelin for sale
References:
https://acworkjobs.com/employer/the-heart-of-the-internet/
cjc 1295/ipamorelin before and after · September 9, 2025 at 8:43 pm
cjc-1295/ipamorelin injections
https://10xhire.io/employer/cjc-1295-ipamorelin-peptide/ how long should i take cjc 1295 ipamorelin
https://pridestaffing.us/companies/cjc-1295-with-and-without-dac-2-complete-guide/ fever after ipamorelin injections
https://xshort.site/nidiakidman738 can you stack aod 9604 and ipamorelin together
http://www.ardenneweb.eu/archive?body_value=%3Ch1%3EIpamorelin+Peak+Performance+Spo%3C/h1%3E%3Cbr%3E+%3Cbr%3E++%3Ch1%3EIpamorelin%3C/h1%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EIpamorelin+is+a+selective+growth+hormone+secretagogue+that+has+gained+popularity+among+athletes%2C+bodybuilders%2C+and+individuals+seeking+to+improve+recovery%2C+muscle+growth%2C+and+overall+well-being.+Unlike+older+analogs+such+as+GHRP-2+or+GHRP-6%2C+ipamorelin+offers+a+more+balanced+hormonal+profile+with+fewer+side+effects%2C+making+it+a+preferred+choice+for+those+aiming+to+optimize+their+training+outcomes+without+excessive+stimulation+of+appetite+or+prolactin+release.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3EWhat+Is+Ipamorelin%3F%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EIpamorelin+is+a+pentapeptide+(five+amino+acids)+that+mimics+the+natural+hormone+ghrelin.+By+binding+to+growth+hormone-releasing+hormone+receptors+in+the+pituitary+gland%2C+it+triggers+the+release+of+endogenous+growth+hormone+(GH).+The+peptide%E2%80%99s+structure+allows+it+to+be+stable+in+circulation+and+to+selectively+activate+GH+secretion+while+sparing+other+hormonal+axes.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3EHow+It+Works%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EWhen+ipamorelin+enters+the+bloodstream%2C+it+reaches+the+pituitary+gland+where+it+binds+to+GHRH+receptors.+This+binding+prompts+a+cascade+that+results+in+the+secretion+of+growth+hormone+into+the+bloodstream.+Growth+hormone+then+stimulates+the+liver+and+other+tissues+to+produce+insulin-like+growth+factor+1+(IGF-1)%2C+which+is+primarily+responsible+for+anabolic+effects+such+as+muscle+protein+synthesis%2C+fat+metabolism%2C+and+tissue+repair.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3EKey+Benefits%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cul%3E%3Cli%3E%3Cstrong%3EMuscle+Hypertrophy%3C/strong%3E:+By+increasing+IGF-1+levels%2C+ipamorelin+promotes+the+synthesis+of+new+muscle+proteins%2C+aiding+in+lean+mass+gains.%3C/li%3E%3Cbr%3E+%3Cbr%3E++%3Cli%3E%3Cstrong%3EFat+Loss%3C/strong%3E:+Growth+hormone+enhances+lipolysis%2C+helping+to+mobilize+stored+triglycerides+for+energy+use.%3C/li%3E%3Cbr%3E+%3Cbr%3E++%3Cli%3E%3Cstrong%3EEnhanced+Recovery%3C/strong%3E:+Elevated+GH+and+IGF-1+improve+tissue+repair%2C+reduce+inflammation%2C+and+accelerate+recovery+from+intense+workouts+or+injuries.%3C/li%3E%3Cbr%3E+%3Cbr%3E++%3Cli%3E%3Cstrong%3EImproved+Sleep+Quality%3C/strong%3E:+Users+often+report+deeper%2C+more+restorative+sleep%2C+which+is+essential+for+muscle+growth+and+hormonal+balance.%3C/li%3E%3Cbr%3E+%3Cbr%3E++%3Cli%3E%3Cstrong%3EJoint+Health%3C/strong%3E:+Growth+hormone+supports+cartilage+regeneration+and+joint+lubrication%2C+reducing+discomfort+during+high-impact+training.%3C/li%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3C/ul%3E%3Ch2%3EDosage+and+Administration%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3ETypical+dosing+protocols+range+from+200%E2%80%93400+%C2%B5g+per+injection.+The+peptide+can+be+administered+subcutaneously+once+or+twice+daily%2C+often+before+workouts+or+at+bedtime+to+coincide+with+natural+GH+secretion+patterns.+Users+should+start+with+a+lower+dose+to+assess+tolerance+and+gradually+increase+as+needed.+Consistency+over+several+weeks+is+necessary+for+noticeable+effects.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3ESafety+Profile%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EIpamorelin%E2%80%99s+selective+action+on+GH+receptors+results+in+minimal+stimulation+of+appetite+and+prolactin%2C+reducing+the+risk+of+unwanted+weight+gain+or+sexual+dysfunction+that+sometimes+accompanies+older+secretagogues.+However%2C+like+all+peptides%2C+it+should+be+used+responsibly+and+ideally+under+professional+guidance.+Potential+side+effects+may+include+mild+injection+site+discomfort%2C+temporary+flushing%2C+or+transient+water+retention.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3ELegal+Status%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EIpamorelin+is+classified+as+a+research+chemical+in+many+jurisdictions.+While+it+is+not+approved+for+human+use+by+major++%3Ca+href%3D%22https://www.valley.md/understanding-ipamorelin-side-effects%22%3Evalley.md%3C/a%3E+regulatory+agencies+such+as+the+FDA%2C+its+status+often+falls+into+a+gray+area+where+it+can+be+sold+for+%22research+purposes+only.%22+Users+should+verify+local+regulations+before+purchase+or+consumption+to+avoid+legal+complications.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3EHow+It+Fits+Into+Peak+Performance%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EAthletes+incorporate+ipamorelin+into+periodized+training+cycles+to+maximize+gains+during+hypertrophy+phases+and+to+support+recovery+during+cutting+or+high-intensity+intervals.+Its+ability+to+elevate+GH+without+significant+appetite+stimulation+allows+for+controlled+caloric+intake+while+still+promoting+anabolic+processes.+When+paired+with+adequate+protein%2C+sleep+hygiene%2C+and+a+balanced+diet%2C+ipamorelin+can+accelerate+performance+improvements+beyond+what+nutrition+alone+would+achieve.%3Cbr%3E+%3Cbr%3E++%3C/p%3E%3Cbr%3E+%3Cbr%3E++%3Ch2%3EConclusion%3C/h2%3E%3Cbr%3E+%3Cbr%3E++%3Cbr%3E+%3Cbr%3E++%3Cp%3EIpamorelin+offers+a+targeted+approach+to+boosting+growth+hormone+secretion%2C+delivering+benefits+that+span+muscle+growth%2C+fat+loss%2C+recovery%2C+and+overall+vitality.+Its+favorable+safety+profile+and+ease+of+use+make+it+an+attractive+tool+for+those+seeking+to+elevate+their+training+outcomes+without+compromising+appetite+or+hormonal+balance.+As+with+any+performance-enhancing+agent%2C+responsible+usage%2C+proper+dosing%2C+and+awareness+of+legal+considerations+are+essential+for+achieving+the+best+results+safely.%3Cbr%3E+%3Cbr%3E++%3C/p%3E How Long Is Ipamorelin Detectable In Urine
https://express-work.com/companies/tesamorelin-ipamorelin:-combining-potency-for-maximum-effect/ Valley
https://www.kamayuq.io/employer/ipamorelin-cjc-1295-peptide-combo-explained-for-growth-and-recovery/ peptides Cjc 1295 and ipamorelin For sale
https://mybusinessweb.in/merrirowcroft2 ipamorelin cjc 1295 how Long To take
https://www.securityprofinder.com/employer/cjc-1295-vs-ipamorelin-which-peptide-delivers-the-best-muscle-gains/ valley
https://lamachineataffer.com/entreprises/a-closer-look-at-the-combination-of-cjc-1295-and-ipamorelin/ ipamorelin cjc 1295 mixing instructions
https://jobfreez.com/employer/the-heart-of-the-internet/ mixing ipamorelin 5mg
https://marine-courses.com/employer/cinnamon-health-benefits-uses-nutrition-and-side-effects/ Ipamorelin And Mod Grf 1-29 Stack
https://renbrook.co.uk/employer/ipamorelin-cjc-1295-stack-the-dynamic-duo/ How To Mix Cjc And Ipamorelin
https://lcateam.com/employer/ipamorelin-vs-sermorelin-5-things-you-should-know/ can ipamorelin be combined with other peptides for better results
https://www.bcard.qa/merryroy749548 ipamorelin dosage For Sleep
https://elitechefnetwork.co.uk/companies/unlocking-benefits-of-ipamorelin-the-ultimate-guide-to-this-peptide/ ipamorelin and Cjc-1295
https://www.diltexbrands.com/employer/ipamorelin-cjc-1295-dosage:-synergistic-effects-for-growth-hormone-release/ valley
https://url.zeus27.com/nelsonlowman90 benefits of ipamorelin peptide
https://patriciusit.com/employer/cjc1295-ipamorelin-ghrp-2-dosage/ ipamorelin and sermorelin suppliers
References:
https://supplychainjobs.in/employer/peptide-dosage-calculator-reconstitution/
https://www.argfx1.com · September 9, 2025 at 10:31 pm
cjc 1295/ipamorelin blend dosage
https://newssignet.top/item/462362 ipamorelin alone
https://autovin-info.com/user/gaugecrook7/ 6 mg Sermorelin 6mg ipamorelin
http://mcforces.ru/user/storysilica64/ Ipamorelin metabolism and excretion
https://josefsen-emborg-2.hubstack.net/is-your-cjc-1295-ipamorelin-safe-addressing-cancer-concerns advantages of ipamorelin
https://md.farafin.de/DhS7DYArQRKbob5KAWqr9w/ ipamorelin nasal spray effectiveness
http://www.annunciogratis.net/author/tigerwind1 valley
https://www.woorips.vic.edu.au/profile/sandersjablindgren63126/profile valley
https://noticias-sociales.space/item/461718 sermorelin ipamorelin 10mg blend dosage
https://noticiasenvivo.site/item/459852 valley
https://md.un-hack-bar.de/Gr6ZzUW1Rv2CJn9gHwpufg/ cjc 1295/ipamorelin Prescription
https://my.vipaist.ru/user/theorymole8/ Valley
https://graph.org/6-Months-On-CJC-1295-Ipamorelin-Here-Is-What-Happened-09-03 oral Efficacy of sermorelin Ipamorelin Cjc 1295
http://karayaz.ru/user/beatcymbal6/ empower pharmacy ipamorelin
https://enoticias.site/item/338753 is It safe combine tesamorelin with Cdc/ipamorelin together
http://kriminal-ohlyad.com.ua/user/armybeard0/ can ibuatmoren with ipamorelin
https://satoil.kz/author/floodtub85/ Ipamorelin And Cjc No Dac Dosage
https://motionentrance.edu.np/profile/harborpruner2/ Where To Get Cjc 1295 Ipamorelin
https://peatix.com/user/27702997 tesamorelin & ipamorelin for sale
References:
beneficios ipamorelin (https://www.argfx1.com/user/santacow9/)
Anton · September 9, 2025 at 11:16 pm
duo blend ipamorelin cjc 1295
https://noticias-sociales.site/item/462142 ipamorelin dosage and mixing 100mg per day
https://just-herbert-3.blogbright.net/essential-guide-to-peptide-dosages-how-to-safely-optimize-your-results-poseidon-dartmouth valley
https://sciencebookmark.top/item/340024 stacking tesamorelin and ipamorelin
https://lejournaldedubai.com/user/shellpruner85/ how long should you take ipamorelin
https://zimmerman-goldstein.thoughtlanes.net/what-is-ipamorelin-ipamorelin-benefits-results-and-effects Valley
https://enoticias.space/item/339661 how long to see fat loss from ipamorelin
https://nouvellessignet.site/item/341909 cjc-1295 ipamorelin what is it
https://noticias-sociales.site/item/462174 valley
https://md.swk-web.com/Ass0Sv8AT66iEfPwM84QUQ/ How long does ipamorelin last in the fridge
https://christie-flowers.technetbloggers.de/cjc-1295-and-ipamorelin-dosage-benefits-mechanisms-and-research-applications ipamorelin and prolactin
https://md.farafin.de/XIslSwr6QvCCezpVnSGOoA/ is ipamorelin a controlled substance
https://www.bitsdujour.com/profiles/YGu95q valley
https://images.google.co.il/url?q=https://www.valley.md/understanding-ipamorelin-side-effects ipamorelin France
https://posteezy.com/cjc-1295-ipamorelin-injections-ipamorelin-therapy-men how much bacteriostatic water to mix with 5mg ipamorelin
https://codimd.fiksel.info/RObSBFvVSY67BmqKUVFgig/ ipamorelin kit
https://noticias-sociales.site/item/462159 ipamorelin cjc 1295 stack mixing instructions
https://images.google.td/url?q=https://www.valley.md/understanding-ipamorelin-side-effects cjc-1295 no Dac ipamorelin
https://www.tikosatis.com/index.php?page=user&action=pub_profile&id=266659 Cjc 1295/Ipamorelin
References:
how fast does cjc 1295 ipamorelin work (https://md.kif.rocks/_7q-KyF_SyilCzUZAty8kA/)
Sherlene · September 10, 2025 at 5:21 am
does ipamorelin cause insulin resistance
References:
cjc 1295 ipamorelin tablets (https://codes.tools.asitavsen.com/soila29d018936)
Kinky-pipes.com · September 10, 2025 at 11:35 am
how much bacteriostatic water to mix with 5mg of ipamorelin
https://kaiftravels.com/employer/understanding-different-ipamorelin-cjc-1295-dosages/ does ipamorelin nasal spray work
https://links.senc.in/angelescreamer do.you mix cjc 1295 and ipamorelin combination
https://famu.cc/denishacutlack can you drink alcohol while taking ipamorelin
https://zip-this-link.com/leathabannan7 valley
https://inftag.com/lynettemad Hgh Vs ipamorelin
https://sourceforhire.com/employer/2x-blend-cjc-1295-no-dac-5mg-ipamorelin-5mg/ medical condition treated by ipamorelin
https://vipnih.com/laurencehalfey valley
https://remotejobscape.com/companies/bulk-cjc-1295-no-dac-ipamorelin-5-5-x-10-vials/ ipamorelin Insulin Resistance
https://jandlfabricating.com/employer/ipamorelin-vs-sermorelin-decoding-the-differences-in-peptide-therapies/ valley
https://www.ajirazetu.tz/employer/cjc-1295-peptide-benefits-dosage-risks-and-where-to-buy/ subcutaneous injection in belly ipamorelin
https://shorx.online/hildredlehmann cjc-1295 ipamorelin before and after
https://thejobsinkuwait.com/employer/mk-677-side-effects-what-to-watch-for/ Cjc 1295 Ipamorelin And Trt
https://waslah.agency/employer/ipamorelin-faqs/ ipamorelin efectos secundarios
https://classifieds.ocala-news.com/author/jadarubin51 cjc 1295 without dac and ipamorelin
https://mulkinflux.com/employer/sermorelin-dosage-guide-how-much-to-take-for-best-results/ ipamorelin dose reddit
https://link.con3ct.com.br/chassidybo how to inject Ipamorelin
https://www.garagesale.es/author/johnbuzacot/ cjc-1295 Ipamorelin peptide stack buy
https://t-iny.com/lucaskelly192 Valley
References:
cjc 1295 ipamorelin and alcohol, https://kinky-pipes.com/blondellkendal,
fanajobs.Com · September 10, 2025 at 11:53 am
ipamorelin mod grf 1-29 before and after reddit
References:
ipamorelin dosing Guidelines (https://fanajobs.com/profile/heidialbers652)
Ipamorelin 5Mg Para Que Serve · September 10, 2025 at 12:26 pm
ipamorelin and cjc no dac dosage and cycle
References:
https://topbookmarks.site/item/462466
Benefits Of Ipamorelin Peptide · September 10, 2025 at 4:23 pm
ipamorelin and mod grf 1 29 dosage
https://oyylink.bio/zackandrus7527 ipamorelin and forgot to refrigerate
https://pharmakendra.in/employer/the-heart-of-the-internet/ valley
https://patriciusit.com/employer/cjc1295-ipamorelin-ghrp-2-dosage/ how long does it take for cjc ipamorelin to work
https://shortico.in/rockyostrander Valley
https://careervalu.co.uk/employer/ipamorelin-peptide-benefits/ cjc 1295 no dac mod grf 1-29 with ipamorelin
http://www.liberte-de-conscience-rideuromed.org/forum-d%c3%a9changes/profile/marcosdesaillly/ Ipamorelin peptid
https://encurt.top/danbrady11359 sermorelin Vs ipamorelin reddit
https://inlnk.co/teKxs cjc-1295 dac and ipamorelin results
https://mapi.tr/carriedela When are benefits observed using ipamorelin
https://academicsgate.com/employer/ipamorelin-sermorelin-dosage/ cjc 1295 dac and ipamorelin dosage
https://worldwiderecruiters.ca/employer/cjc-1295-vs-ipamorelin-which-peptide-delivers-the-best-muscle-gains/ cjc-1295 ipamorelin purchase
https://jobsrific.com/employer/ipamorelin-cjc-1295-before-and-after-results-cycle/ cjc 1295 ipamorelin buy online
https://hitechjobs.me/companies/sermorelin-vs-cjc-1295-vs-ipamorelin/ ipamorelin 15 Mg
https://profylelink.com/aimee93c292182 cjc 1295 ipamorelin increase testosterone
https://job.dialnumber.in/profile/dillons3685049 cjc 1295/ipamorelin 5mg mixing
https://pagemelon.com/blairoutla valley
https://bcstaffing.co/employer/300037/tesamorelin-vs-sermorelin-peptides-to-boost-hgh Cjc 1295 no Dac + ipamorelin
https://asemployment.com/employer/ipamorelin-5mg/ cjc-1295/ipamorelin dosage per day
References:
https://built.molvp.net/wallyholem
https://part-time.ie/companies/i-did-8-months-on-ipamorelin-cjc1295 · September 11, 2025 at 10:45 am
cjc-1295 & ipamorelin peptide blend
https://www.philresmandaue.com/profile/kerstinfugate cjc-1295 ipamorelin and testosterone together
https://jobe.pk/companies/ipamorelin-dosage-calculator-and-chart-a-z-guide/ what drugs have ipamorelin in them
https://urlyshort.pro/graigboismenu7 valley
https://www.bridgewaystaffing.com/employer/cjc-1295-vs-sermorelin-applications-uses-and-considerations/ Valley
https://sigma-talenta.com/employer/cjc-1295-and-ipamorelin-dosage-strategies-unlocking-muscle-growth-fat-loss-and-anti-aging-benefits/ ipamorelin cjc 1295 and sermorelin
http://bolsatrabajo.cusur.udg.mx/employer/cjc-1295-ipamorelin-understanding-the-benefits-and-uses-in-therapy/ cjc 1295 Ipamorelin bodybuilding dosage
https://careeramaze.com/employer/what-is-the-difference-between-sermorelin-and-ipamorelin/ Ipamorelin blood glucose
https://jobstaffs.com/employer/cjc-1295-vs-ipamorelin-which-is-better/ ipamorelin o que é
https://felipesbackyard.com/tesamorelin-ipamorelin-peptide-therapy-benefits-protocols-result/ valley
http://fatims.org/employer/2x-blend-cjc-1295-no-dac-5mg-ipamorelin-5mg/ Ipamorelin Rash
https://eujobss.com/employer/ipamorelin-cjc-1295-iam-clinic/ cjc-1295 ipamorelin igf-1 increase study
https://www.famahhealthcareservices.com/employer/ipamorelin-vs-sermorelin-decoding-the-differences-in-peptide-therapies/ valley
https://fli.my/margaritoi694 which Is better ipamorelin or semorelin
https://acworkjobs.com/employer/cjc1295-ipamorelin-dosage-crafting-the-perfect-regimen/ ipamorelin cjc 1295 before and after
https://careers.cblsolutions.com/employer/tesamorelin-ipamorelin-blend-5-5mg/ 5mg ipamorelin reconstitution
https://carletonservices.com/employer/the-heart-of-the-internet/ peptide cjc 1295 ipamorelin
https://classihub.in/author/alycewalker/ ipamorelin uses benefits side effects
https://iratechsolutions.com/employer/sermorelin-vs-cjc-1295-comparing-gh-release-peptides/ ipamorelin sigma
References:
do.you mix cjc 1295 and ipamorelin combination; https://part-time.ie/companies/i-did-8-months-on-ipamorelin-cjc1295/,
Ipamorelin Cutting · September 11, 2025 at 7:17 pm
sermorelin & ipamorelin
https://laviesound.com/ramirodawes399 how long does it take to See results from ipamorelin
https://grafana.jasonstolle.com/latoyalittler8 how to reconstitute ipamorelin 2mg
https://gitlab.rails365.net/bennyviera369 valley
https://git.obo.cash/miamatthies073 Ipamorelin Clinical study
https://gitea.mocup.org/carolinetrotte cjc 1295 ipamorelin fasting
https://www.kornerspot.com/@wilsone8747216 Valley
https://git.bloade.com/mallorylesouef ipamorelin morning Or Night
http://dgzyt.xyz:3000/cathernontiver ipamorelin and cjc no dac dosage and cycle
https://musiccosign.com/aldaaranda2666 cjc 1295 ipamorelin storage
https://rucollectshoeclub.com/read-blog/4945_when-to-take-dianabol-before-or-after-workout.html ipamorelin subcutaneous or intramuscular
https://ads-git.beanonetwork.com/wileyaqc553023 Cjc ipamorelin dosing
https://git.poly.zone/shannatrivett3 take sermorelin and ipamorelin together
https://gitea.fcliu.net/noble463068100 topical application Of ipamorelin
https://www.sephalon.net/latashiagreer3 Ipamorelin for Sale Usa
http://git.tjhah.com:3000/loreneday99744 cjc 1295 and ipamorelin before and after
http://git.7doc.com.cn/kristanh087230 cjc-1295 + ipamorelin blend
https://unitedmusicstreaming.com/jasminvandegri how long should you take cjc 1295 ipamorelin
https://alelo.org/@selinaaugustin valley
References:
http://git.veilytech.com/u/abelmerrick55
ipamorelin vs ibutamoren · September 11, 2025 at 8:49 pm
ipamorelin with semaglutide
References:
https://quickdate.click/@marionbuzzard
https://buketik39.ru/user/iraneight3 · September 12, 2025 at 3:24 am
sermorelin ipamorelin program
https://techniknews.top/item/461407 ipamorelin before or after workout
http://stroyrem-master.ru/user/kenyajapan66/ cjc 1295 n o dac and ipamorelin dosage
http://stroyrem-master.ru/user/nationwind0/ can ipamorelin be used for weight loss
https://latenews.top/item/349352 how to mix cjc 1295 and ipamorelin 5mg
https://topbookmarks.site/item/462472 sermorelin vs ipamorelin vs tesamorelin
https://peatix.com/user/27702792 ipamorelin + mod grf 1-29 mix
https://www.google.ki/url?q=https://www.valley.md/understanding-ipamorelin-side-effects ipamorelin blood glucose
https://rentry.co/76kyurm2 ipamorelin 5mg para que serve
https://en.unidos.edu.uy/profile/midtgaardmhypedersen90307/profile semaglutide vs ipamorelin
https://nouvellessignet.site/item/341859 Ipamorelin Dosing Schedule
https://elclasificadomx.com/author/tempergrey1/ Ipamorelin Peptide Australia
https://md.farafin.de/HSuldk16Qsi5lUITKh0A9A/ ipamorelin online prescription
https://en.unidos.edu.uy/profile/fultonitsmuir4766/profile ipamorelin kaufen deutschland
https://en.unidos.edu.uy/profile/busksqqdideriksen87770/profile peptides cjc 1295 And ipamorelin reviews
https://www.argfx1.com/user/kittenwar1/ difference between tesamorelin and ipamorelin
https://www.fionapremium.com/author/lyricregret1/ Blue Sky peptides ipamorelin
https://enregistre-le.space/item/344156 valley
https://monjournal.xyz/item/341415 valley
References:
ipamorelin en cuánto tiempo se ven resultados (https://buketik39.ru/user/iraneight3/)
https://cuttify.io/ermahenninger · September 12, 2025 at 7:41 am
ipamorelin with cjc starting dose
References:
ipamorelin dosaggio (https://cuttify.io/ermahenninger)
valley · September 12, 2025 at 9:00 am
cjc ipamorelin peptide for sale
https://cupido.prestigioapps.com/@cecilepetre54 Tesamorelin Ipamorelin Stack Dosage
https://dating.igbopeople.org/@ucngeneva46260 ipamorelin como usar
https://git.palagov.tv/joliecolebe957 valley
https://git.saintdoggie.org/ulyssesboucher ipamorelin cjc-1295 dosage
https://filuv.bnkode.com/@zocsylvester07 stacking tesamorelin and ipamorelin
https://git.rggn.org/bettielamarche ipamorelin starting dose
https://git.prohotel-edv.de/claudet628517 cjc-1295 ipamorelin peptide therapy benefits
https://git.saintdoggie.org/susana32747664 Ipamorelin Benefits Side Effects
https://gitea.chloefontenot.org/genevafallis34 cjc 1295 w o dac and ipamorelin
https://git.cydedu.com/lavonnecerutty hallandale pharmacy ipamorelin
https://gitea.fcliu.net/noble463068100 cjc-1295 ipamorelin peptide stack price
https://git.van-peeren.de/mkgzachery7465 cjc-1295 ipamorelin cost per vial
https://music.1mm.hk/indiananwb4179 https://pilowtalks.com/@nathaniellott1
https://selfloveaffirmations.net/@kiaramoe59130 valley
https://mostreams.com/matildaplummer Ipamorelin igf 1 suppliers
http://git.7doc.com.cn/kristanh087230 valley
https://hipstrumentals.net/mohammedf6967 Mod Grf 1-29 + ipamorelin
https://heywhatsgoodnow.com/@knpkarolin9676 ibutamoren vs ipamorelin
Valley · September 12, 2025 at 10:56 am
recommended dosage of ipamorelin
https://helpin.ge/employer/ipamorelin-5mg/ ipamorelin france
https://yourrecruitmentspecialists.co.uk/employer/ipa-cjc-guide/ best time to take cjc 1295 ipamorelin
https://www.1234.click/index.php?action=profile;u=12017 sermorelin ipamorelin before and after
https://eliteyachtsclub.com/employer/ozempic-for-weight-loss-will-it-work-for-me/ ipamorelin or cjc 1295
https://www.taptag.vc/ronda21z240356 cjc-1295 ipamorelin tablets
https://www.kamayuq.io/employer/understanding-mk-677-side-effects-what-you-need-to-know/ ipamorelin reconstitution
https://recruitmentfromnepal.com/companies/the-synergistic-effects-of-ipamorelin-and-cjc-1295-what-you-need-to-know/ buy cjc-1295 ipamorelin uk
https://www.complete-jobs.com/employer/cjc-1295-no-dac-5mg-ipamorelin-10mg-15mg-blend does cjc 1295 ipamorelin need to be refrigerated
https://gizemarket.com/companies/tesamorelin-ipamorelin-peptide-therapy-benefits-protocols-result/ aod 9604 and ipamorelin at the same time
https://agenceglobalpro.com/employer/4848/ipamorelin-side-effects-safe-and-effective-results Ibutamoren Vs Ipamorelin
http://prawattasao.awardspace.info/modules.php?name=Your_Account&op=userinfo&username=StarI9663 ipamorelin/cjc-1295 blend
https://bitily.me/inge1789100086 Cjc-1295 ipamorelin peptide Therapy
https://dev-members.writeappreviews.com/employer/ipamorelin/ 1295/ipamorelin
https://mapi.tr/lauragatli https://nakshetra.com.np/companies/cjc-1295-ipamorelin-for-sale/
https://www.dynamicviewpoint.co.uk/employer/cjc-1295-and-ipamorelin-dosage-strategies-unlocking-muscle-growth-fat-loss-and-anti-aging-benefits/ Recommended Dosage of ipamorelin
http://athrconsultancy.in/employer/cjc-1295-ipamorelin-dosage http http://www.blueskypeptide.com blend-cjc-1295-no-dac-5mg-with-ipamorelin-5mg.html
https://rsh-recruitment.nl/employer/tesamorelin-vs-ipamorelin-a-comprehensive-comparison/ tesa ipamorelin blend
http://www.jobteck.co.in/companies/ipamorelin-benefits-dosage-risks-2025/ ipamorelin and testosterone Stack
https://noarjobs.info/companies/buy-sermorelin-ipamorelin-10mg-Online/ · September 12, 2025 at 12:16 pm
cjc female ipamorelin before and after pics
https://oromiajobs.com/profile/jenniyoo900115 valley
https://sell.com.my/en/user/profile/NelleGriffi ipamorelin mod grf 1 29 fat loss
https://db.dbmyxxw.cn/home.php?mod=space&uid=221333&do=profile&from=space Valley
https://www.findjobindz.com/employer/cjc-1295-ipamorelin-dosage/ ipamorelin 2mg axiom peptides online
https://webtily.me/kentj941834239 Valley
https://jobcop.in/employer/ipamorelin-cjc-1295-peptide-combo-explained-for-growth-and-recovery/ cjc 1295 ipamorelin 5 5 blend dosage
https://styleandfrip.fr/ipamorelin-discover-its-benefits-for-health-and-peak-performance/ cjc 1295 ipamorelin best time to take
https://pharmakendra.in/employer/cjc-1295-ipamorelin-proper-dosage/ cjc 1295 + ipamorelin weight loss dosage
https://rentry.co/53930-a-closer-look-at-the-combination-of-cjc-1295-and-ipamorelin cjc 1295 dac vs ipamorelin
https://www.toutsurlemali.ml/employer/cjc-1295-ipamorelin-bodybuilding-dosage-the-ultimate-growth-combo/ Ipamorelin Dose 100
https://fixjob.lk/companies/ipamorelin-dosage-how-much-do-you-really-need-for-muscle-growth/ cjc-1295 and ipamorelin:
https://careers.universalair.aero/employer/cjc-1295-ipamorelin-bodybuilding-dosage-the-ultimate-growth-combo/ valley
https://elitechefnetwork.co.uk/companies/cjc-1295-ipamorelin-managing-side-effects/ Cjc Ipamorelin Dosage Reddit
https://wadhefa.site/companies/cjc-1295-ipamorelin-stack-the-synergistic-peptide-combo/?-ipamorelin-stack%3A-the-synergistic-peptide-combo%2F fragment 176-191+mod grf 1-29+ipamorelin mix
https://insurancehr.com/employer/cjc-1295-ipamorelin-bodybuilding-the-power-duo/ what does cjc ipamorelin do
https://talvisconnect.nl/employer/ipamorelin-dosage-cycle-how-to-plan-it/ valley
https://www.thehispanicamerican.com/companies/cjc-1295-ipamorelin-peptide-blend/ ipamorelin 5Mg Factories
https://www.cbl.aero/employer/ipamorelin-side-effects-safe-and-effective-results/ ipamorelin cycle results
References:
Cjc 1295 with Ipamorelin (https://noarjobs.info/companies/buy-sermorelin-ipamorelin-10mg-online/)
Libreng Binance Account · September 12, 2025 at 1:32 pm
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. binance
Valley.Md · September 12, 2025 at 2:04 pm
ipamorelin sage
References:
https://aweza.co/employer/ipa-cjc-guide/
Female ipamorelin before and after pics · September 12, 2025 at 6:30 pm
ipamorelin dosing options
References:
https://itgovernancejobs.com/employer/ipamorelin-cjc-1295-before-and-after-results-cycle/
Ipamorelin Use in bodybuilding · September 12, 2025 at 8:46 pm
peptídeos ipamorelin para que serve
References:
https://md.farafin.de/cPYIU8lGQteuBRXr-OWDTw/
Cjc 1295 Ipamorelin Allergic Reaction · September 13, 2025 at 4:58 am
can you take cjc 1295 dac with ipamorelin
https://jobtracko.com/employer/29782/comparing-the-benefits-of-sermorelin-vs-ipamorelin-vs-tesamorelin-usa-made ipamorelin where to buy
https://ehrsgroup.com/employer/6-months-on-cjc-1295-ipamorelin-here-is-what-happened/ what does sermorelin ipamorelin for men
https://onlinejob.lk/employer/peptide-tuesday-morelins-101-meet-the-peptides-that-tell-your-body-to-age-backwards/ ipamorelin 5mg reconstitution
https://nationalcarerecruitment.com.au/employer/ipamorelin-dosage-calculator-and-timing-for-bodybuilding/ sermorelin ipamorelin blend peptide for sale
https://laboryes.com/employer/bpc-157-vs-cjc-1295-a-comparative-analysis/ sermorelin + ipamorelin blend
https://helpin.ge/employer/ipamorelin-5mg/ Valley
http://tamilachat.org/community/profile/chauspooner5855/ cjc1295 ipamorelin before and after
https://employmentabroad.com/companies/cjc-1295-vs-ipamorelin-which-is-better/ aod 9604 and ipamorelin at the same time reddit
https://jobsinquant.com/employer/ipamorelin-side-effects-a-comprehensive-overview/ how long to people take ipamorelin
https://jobshop24.com/employer/ipamorelin-reviews-clinical-trials-and-safety/ ipamorelin Sublingual
https://sublimejobs.co.za/employer/tesamorelin-vs-ipamorelin-a-comprehensive-comparison/ Valley
https://krishnacareers.com/employer/cjc-1295-ipamorelin-side-effects-research/ ipamorelin long term Side effects
https://t-iny.com/lucaskelly192 cjc 1295 without dac and ipamorelin
https://url.weburj.com/flora76400439 Buy Cjc 1295 Ipamorelin Troche
https://www.positionfit.net/employer/cjc1295-ipamorelin-ghrp-2-dosage/ valley
https://fmagency.co.uk/companies/cjc-1295-peptide-benefits-dosage-risks-and-where-to-buy/ how Many weeks can u take ipamorelin
https://maids-station.com/employer/cjc-1295-ipamorelin-peptide-blend/ how much cjc 1295 ipamorelin should i take
https://iratechsolutions.com/employer/tesamorelin-vs-ipamorelin-cjc-1295-a-comparison/ valley
References:
http://hoteliers.ke/employer/6-months-on-cjc-1295-ipamorelin-here-is-what-happened
cjc 1295 Ipamorelin Testosterone · September 13, 2025 at 5:58 am
can you stack sermorelin with cjc 1295 ipamorelin
https://phoebe.roshka.com/gitlab/launafreeleagu cjc 1295 Ipamorelin itchy skin
https://hafrikplay.com/chanapastor78 Cjc 1295 No dac with ipamorelin hair Growth
https://gitlab.ui.ac.id/carltonttw920 valley
https://www.soundofrecovery.org/kandicemclaugh valley
https://ngoma.app/gisellebernhar valley
https://hanyunmedical.com/lynnesolander tesamorelin cjc1295/ipamorelin 12mg blend reconstitution
https://git.berfen.com/betseystiles07 sermorelin & ipamorelin
https://gitea.fcliu.net/noble463068100 valley
https://airplayradio.com/cindac48619454 ipamorelin vs hgh reddit
https://git.poly.zone/claribellocket tesamorelin + cjc1295 + ipamorelin 12mg blend dose
https://git.sumedangkab.go.id/johanna05y845 cjc 1295 ipamorelin risks
https://git.lodis.se/fredaparis6526 Valley
http://www.cnbluechip.com/wendellford806 ipamorelin Molecular weight
https://music.growverse.net/rosemaryyabsle cjc 1295 + ipamorelin side effects
https://gitea.b54.co/makaylabacon25 ipamorelin west palm beach
https://gitlab.malldongli.com/sheenacye95296 ipamorelin compounding pharmacy
http://saromusic.ir/irishwrench429 sermorelin vs ipamorelin vs cjc 1295
https://git.ellinger.eu/angelina95b104 ipamorelin Cycle Bodybuilding
References:
https://git.wisptales.org/joiewalstab323
Dong · September 13, 2025 at 7:00 am
buy tesamorelin & mod grf & ipamorelin blend
References:
ipamorelin supplement [https://arlogjobs.org/employer/tesamorelin-dosage-calculator-and-chart-a-z-guide/]
valley.md · September 13, 2025 at 9:37 am
what is sermorelin ipamorelin blend peptide for men
References:
https://www.fionapremium.com/author/bankerart5/
body-positivity.org · September 13, 2025 at 2:50 pm
tesamorelin cjc1295 ipamorelin dosage reddit
References:
What are the benefits of cjc 1295 and ipamorelin (https://body-positivity.org/groups/cjc1295-ipamorelin-dosage-crafting-the-perfect-regimen/)
ipamorelin/sermorelin injections · September 13, 2025 at 4:45 pm
sermorelin-ipamorelin-cjc 1295 dosage
References:
https://mwcejobbank.webz.com.ng/employer/6-months-on-cjc-1295-ipamorelin-here-is-what-happened
Maryann · September 17, 2025 at 3:52 pm
bet365 money casino usa, fastest paying casino usa and cash poker online
canada, or online live roulette casino usa
my web-site: minimum blackjack bet bellagio (Maryann)
git.baltimare.org · September 26, 2025 at 8:32 am
buysteroidsonline.com reviews
https://newsflip.in/@hildredestrada?page=about best over the counter muscle builder
https://code.openmobius.com:3001/bettytruman12 what type of drugs are anabolic steroids
https://skiivie.com/@anneslavin1978?page=about the effects of steroids on the human body
https://git.unglab.com/adelemattox286 Legal winstrol alternative
https://kannadatube.in/@archiecolwell?page=about anabolic steroids are synthetic versions of which of the following
https://git.bigtravelchat.com/darrensyy09310 physiological effects of anabolic steroids
http://rhx0.top:3000/ginomacaulay84 valley
https://git.9ig.com/coy37x00575743 best stack for cutting Fat
https://git.ellinger.eu/finnransom342 how to take steroids correctly
https://git.hexdive.com/demetria93t841 valley
https://gitlab.oc3.ru/u/bianca56890166 best Bodybuilding stack for beginners
https://datez.pro/@elizbethverdin most popular steroid
https://tubevieu.com/@adelaearnshaw?page=about dianabol and deca stack
https://movieru.jp/portfolio/@christianebear?page=about valley
https://git.palagov.tv/clarabadillo0 Trenbolone Steroids
https://ldcv.de/odellmahomet43 making steroids legal
https://mardplay.com/caroleaww8181 valley
https://qarisound.com/derrickmarko86 best steroids for Bodybuilding
References:
winsol side effects (https://git.baltimare.org/chelseygawler4)
inmessage.site · September 26, 2025 at 8:54 am
natural anabolics
References:
why is steroid use among athletes dangerous (https://inmessage.site/@donnieroberts0)
what do steroids do to the body · September 26, 2025 at 9:19 am
what are steroids used for in the body
http://git.yanei-iot.com:600/kittywinfield0 Betaine Supplement Bodybuilding
https://gitea.boner.be/brookejohann16 how many people use anabolic steroids
https://git.sleepingforest.co.uk/rubincorey2635 steroid alternatives gnc
https://9jadates.com/@cindidrew67460 bodybuilder before and after steroids
https://git.qdhtt.cn/carolinemutch8 what are steroids and why are they dangerous
https://dhivideo.com/@finnzimmer6093?page=about 17aa steroids
https://homenetwork.tv/@jamiprevost991?page=about Valley
https://www.nemusic.rocks/adolphhaviland valley
https://git.bloade.com/alena68r332849 liquid anadrol
https://gitea.belanjaparts.com/kelvincimitier valley
https://git.rbsx.de/johnnyboxer975 testosterone injections for muscle building
https://wiki.idealirc.org/lucretiacunnif symptoms of anabolic steroids
https://www.meetgr.com/@annawvo102266 deca winstrol stack
https://inmessage.site/@donnieroberts0 Where to Get Anabolic steroids
https://guse.in/dacia28119797 androgenic effects
https://filuv.bnkode.com/@adriannefelix steroid use facts
https://truthtube.video/@augustinaselle?page=about what are anabolics
https://git.suika.org/gus86712320870 oral winstrol for sale
References:
https://music.vp3.me/dianemccormack
Anabolic steroid research · September 26, 2025 at 10:05 am
how do anabolic steroids cause high blood pressure
http://gitea.mintelcn.com/denicestreetma ultimate steroid cycles
http://energonspeeches.com/@brentrossetti?page=about steroid User vs natural
https://git.droenska.com/darlaburrowes8 using steroids before and after
https://git.lodis.se/denischampagne anabolic supplements gnc
https://gitlab.zb100.com/alexiscrotty2 what is anabolic mean
https://tunelifystream.com/gisele12d33180 anabolic steroids chemical structure
https://git.asdf.cafe/akilah28l61454 are steroids fats
https://heyyo.social/@erik83x1382374?page=about how to Get legal steroids
https://shiatube.org/@charley3839289?page=about sustanon 250 before and after
https://nemoserver.iict.bas.bg/herbertsauceda Valley
https://kannadatube.in/@archiecolwell?page=about anavar and hair loss
https://wedioz.com/@angelachataway?page=about consequences of using steroids
https://gitea.mulberrypos.ru/alyssalazzarin arnold schwarzenegger steroid use
https://git.17pkmj.com:3000/trentcalvin19 supplements similar to steroids
https://fyahtrak.com/agustinbuckmas valley
https://wtube.net/@derrickczn2502?page=about legal Steroids in usa
https://src.strelnikov.xyz/bebebeahm0009 american steroids online
https://mediascatter.com/@antonyhooks473?page=about why are steroids bad for athletes
References:
https://lius.familyds.org:3000/glindahussain3
https://www.chenisgod.com/ · September 26, 2025 at 4:03 pm
how many people use steroids
References:
sports with Alternatives to steroids (https://www.chenisgod.com:3096/allie24j977071)
Sustanon 250 Stacks · September 26, 2025 at 8:25 pm
shred stack gnc
References:
https://bash.tube/@felicitassearl?page=about
valley.Md · September 26, 2025 at 10:29 pm
steroids before and after first cycle
References:
https://git.nightime.org/herbertn758285
anabolic stacks (vai.com#) · September 27, 2025 at 2:28 am
what is the function of steroids
References:
https://spinvai.com/heathcrum38778
https://Gitlab.ujaen.es/ · September 28, 2025 at 12:31 am
anabolic effects
https://git.sumedangkab.go.id/jeannettegillo Natural Vs Steroid bodybuilding
https://playmelo.com/@ednan67353114?page=about valley
http://git.hulimes.com/uwtbrenna9901 muscle gain supplements steroids
https://worldclassdjs.com/staceybarajas1 how do steroids affect the body
http://tools.refinecolor.com/quinnhateley1 mens steroids
http://hot360onlinetv.site/@taylahpeters37?page=about reddit how to increase testosterone
https://git.atomos.io/tristafrome171 valley
https://sexwifed.com/@neiloshea9017?page=about valley
http://hottv.in/@ara34j22488245?page=about best steroid cycle For lean mass
https://www.youtoonetwork.com/youtootube/@silviav0755400?page=about dianabol steroids side Effects
https://zoucast.com/buckfrye471238 Is testosterone the same as steroids
https://git.traband.ovh/williequentin1 valley
http://hot360onlinetv.site/@taylahpeters37?page=about buy real steroids online
https://itimez.com/@selenestrachan?page=about valley
https://mediascatter.com/@christyhartiga?page=about valley
https://lawrencewilbert.com/read-blog/20678_anavar-dosage-guide-athletes-men-powerlifting-endurance.html all about steroids
https://vibecodetogether.com/milfordflorez4 valley
https://easyconnect.fun/@kicjanet293934 Valley
References:
new steroid alternative (https://gitlab.ujaen.es/zrkmay71907342)
Https://git-i.Ir/ · September 28, 2025 at 1:23 am
are steel supplements steroids
References:
pre steroid bodybuilders (https://git-i.ir/gladisbou93093)
https://gogs.soyootech.com · September 28, 2025 at 6:52 am
best steroid for athletic performance
https://git.yinas.cn/milanmolino367 male steroids for sale
https://ceedmusic.com/aubreypelensky are steroids legal in bodybuilding
https://git.esc-plus.com/myrtlewilken16 Using Steroid
https://date.ainfinity.com.br/@gbwstella1798 valley
https://speeddating.co.il/@elena47292931 gnc Products Protein
https://git.lmskaran.com/leilabodiford Valley
https://actsolution.iptime.org:3000/maryjoverco904 valley
https://gitea.offends.cn/hassanhearn757 bulking cycle stack
https://syq.im:2025/bonita87d3524 0ahukewixpkubzmjnahxdgs0khugka8kq4dudcao|side effects definition
http://demo.sunflowermachinery.com/declankingston anabolic System
https://git.ultra.pub/caitlyn3813206 legit research chemical supplies sites bodybuilding
https://git.tbaer.de/irwinmackaness where do bodybuilders Get steroids
https://www.propose.lk/@fredricsouza16 legal alternatives to steroids
https://worship.com.ng/eliasphan52170 Closest Thing To Steroids But Legal
https://great-worker.com/daleneburris67 steroid gains
https://git.itbcode.com/benedictrasco0 anabolic steroid withdrawal Symptoms
https://luvwing.com/@cameronfauldin valley
https://git.daoyoucloud.com/bretreimann94 valley
References:
are there legal anabolic steroids; https://gogs.soyootech.com/ardenfoote011,
git.haowumc.com · September 28, 2025 at 8:35 am
using steroid
https://git.alexavr.ru/christinbladen anabolic steroids are a synthetic version of testosterone
https://qimley.com/@alexandrapxs1 does the rock take steroids
https://git.srv.ink/donnieveasley how do steroids enter the body
https://git.fandiyuan.com/darringdd09768 anavar bodybuilding
https://matchmadeinasia.com/@hudsonmccrary find closest gnc
https://gitea.abra.me/doloresgrillo how long does it take for natural testosterone to come back after steroids
https://sheyiyuan.cn/colerankin504 legal prohormones that work
https://codes.tools.asitavsen.com/charolettehawk anabolic steroids are a synthetic version of testosterone
https://git.thweb.net/franciscab5226 steroid alternatives reddit
https://www.fastmarry.com/@graigmccaffrey best stack supplements
https://www.atmasangeet.com/blaineburgett are steroids fats
https://www.tippy-t.com/douggardin5833 anabolic process Definition
https://www.e-vinil.ro/htealecia57964 Dick steroids
https://gitlab.ui.ac.id/galekotai81227 testosterone is a steroid
https://git.snowcloak-sync.com/flor06i9608485 valley
https://git.rec4box.com/ahmadkalb1642 pros of steroids
https://hiphopmusique.com/fgftaren779073 Steroid Effects On Females
https://aipod.app/malindabavin45 valley
References:
consequences of using steroids (https://git.haowumc.com/corrinesneed07)
WymSkPhN · September 28, 2025 at 9:55 am
555
WymSkPhNMibCAGKx · September 28, 2025 at 9:58 am
555
WymSkPhN' AND 2*3*8=6*8 AND 'Mth0'='Mth0 · September 28, 2025 at 9:59 am
555
WymSkPhN-1 waitfor delay '0:0:15' -- · September 28, 2025 at 10:02 am
555
WymSkPhNVrUPtrRb'; waitfor delay '0:0:15' -- · September 28, 2025 at 10:03 am
555
WymSkPhN3ENgjj2u' OR 466=(SELECT 466 FROM PG_SLEEP(15))-- · September 28, 2025 at 10:04 am
555
WymSkPhN5Ad9yIkV') OR 978=(SELECT 978 FROM PG_SLEEP(15))-- · September 28, 2025 at 10:04 am
555
WymSkPhNh243GMbI')) OR 163=(SELECT 163 FROM PG_SLEEP(15))-- · September 28, 2025 at 10:05 am
555
WymSkPhN'||DBMS_PIPE.RECEIVE_MESSAGE(CHR(98)||CHR(98)||CHR(98),15)||' · September 28, 2025 at 10:06 am
555
WymSkPhN · September 28, 2025 at 10:10 am
555*if(now()=sysdate(),sleep(15),0)
WymSkPhN · September 28, 2025 at 10:11 am
5550’XOR(555*if(now()=sysdate(),sleep(15),0))XOR’Z
WymSkPhN · September 28, 2025 at 10:12 am
5550″XOR(555*if(now()=sysdate(),sleep(15),0))XOR”Z
WymSkPhN · September 28, 2025 at 10:12 am
(select(0)from(select(sleep(15)))v)/*’+(select(0)from(select(sleep(15)))v)+'”+(select(0)from(select(sleep(15)))v)+”*/
WymSkPhN · September 28, 2025 at 10:13 am
555-1; waitfor delay ‘0:0:15’ —
WymSkPhN · September 28, 2025 at 10:13 am
555-1); waitfor delay ‘0:0:15’ —
WymSkPhN · September 28, 2025 at 10:14 am
555-1 waitfor delay ‘0:0:15’ —
WymSkPhN · September 28, 2025 at 10:15 am
555snKRDEET’; waitfor delay ‘0:0:15’ —
WymSkPhN · September 28, 2025 at 10:15 am
555-1 OR 115=(SELECT 115 FROM PG_SLEEP(15))–
WymSkPhN · September 28, 2025 at 10:16 am
555-1) OR 349=(SELECT 349 FROM PG_SLEEP(15))–
WymSkPhN · September 28, 2025 at 10:16 am
555-1)) OR 224=(SELECT 224 FROM PG_SLEEP(15))–
WymSkPhN · September 28, 2025 at 10:17 am
555AOitf8a4′ OR 709=(SELECT 709 FROM PG_SLEEP(15))–
WymSkPhN · September 28, 2025 at 10:18 am
555krYV3nOg’) OR 869=(SELECT 869 FROM PG_SLEEP(15))–
WymSkPhN · September 28, 2025 at 10:18 am
555IPiA90Ff’)) OR 654=(SELECT 654 FROM PG_SLEEP(15))–
WymSkPhN · September 28, 2025 at 10:19 am
555*DBMS_PIPE.RECEIVE_MESSAGE(CHR(99)||CHR(99)||CHR(99),15)
WymSkPhN · September 28, 2025 at 10:19 am
555’||DBMS_PIPE.RECEIVE_MESSAGE(CHR(98)||CHR(98)||CHR(98),15)||’
fisheriessummit.com · September 28, 2025 at 10:23 am
sarms vs steroids
https://skitterphoto.com/photographers/1146021/lynggaard-larson should i do steroids
https://textbuffet.com/5th-biggest-dandiya-night-in-noida/ best steroid for bodybuilding
https://wood-swordcricket.com/product/king-1-2-english-willow-bat/ best product to get cut
https://mgscleaninginc.com/no-deposit-bonus-australia-s-top-online-gambling-2/ 100 shredded and pro muscle
https://qaq.com.au/2015/06/12/japanese-inspired-decorating-with-the-tokyo-decorative-screen-design/ Valley
https://mililie.com/houkoku/ steroids weight loss
https://iagamers.com/black-myth-wukong-how-to-access-kingdom-of-sahali-drunken-boar-quest/ bodybuilding steroids before and after
https://korenagakazuo.com/2008/02/16/%e5%85%ab%e6%bd%ae%e5%b8%82%e3%81%ae%e3%82%bb%e3%83%96%e3%83%b3%e3%82%a4%e3%83%ac%e3%83%96%e3%83%b3%e3%81%a7%e5%87%ba%e4%bc%9a%e3%81%a3%e3%81%9f%e7%8c%ab/ Physiological effects Of steroids
https://eugo.ro/?p=535 bulking steroids for sale
https://noticias.upc.edu.pe/2014/05/26/upc-presenta-plan-completo-de-beneficios-para-alumnos-deportistas/ strongest anabolic steroid on the market
https://doc.adminforge.de/Y9tItakEQV-vIJU8vbEFiw side effects of steroids in females
https://chandigarhshine.com/understanding-cataracts-causes-and-treatment/ anabolic Weight loss
https://www.fundamentale.ro/cum-sa-folosesti-instrumentele-de-colaborare-online anabolic hormones definition
https://woodstocksbest.com/understand-the-background-of-design/ purchasing steroids
https://finflowgenius.org/how-finflow-genius-is-revolutionizing-cash-flow-management-for-smes/ different types of anabolic steroids
https://synaply.io/ai-powered-sales-enablement-tools/ Best Testosterone Injection For Bodybuilding
https://zodiakmoonrocks.com/product/dr-zodiak-dynamite-stick/ valley
https://sailorslife.in/question/jetblue-seat-selection/ anavar cutting cycle
References:
newest steroid (https://fisheriessummit.com/mastering-time-management-key-to-business-success/)
WymSkPhN · September 28, 2025 at 10:45 am
555
buy Steroids in india · September 28, 2025 at 11:11 am
best steroid stack for lean muscle mass
https://lakayinfo.com/une-messe-de-requiem-a-ete-celebree-ce-samedi-matin-27-avril-2019-en-la-cathedrale-du-cap-haitien-a-la-memoire-de-jacques-dubois-premier-martyr-public-du-dossier-petrocaribe-par-certaines-organisati/ long term effects of steroids on the body
https://watbosa.ac.th/question/awokawok/ valley
https://fotohana.fi/uomapullo-kateva-kumppani-arkeen-ja-ymparistoystavalliseen-elamaan/ valley
https://www.ptpraxis.gr/%ce%ad%cf%87%cf%89-%ce%b4%cf%85%cf%83%ce%ba%ce%bf%ce%b9%ce%bb%ce%b9%cf%8c%cf%84%ce%b7%cf%84%ce%b1-%cf%80%ce%bf%cf%85-%ce%bd%ce%b1-%cf%80%ce%ac%cf%89-%cf%80%cf%8e%cf%82-%ce%bd%ce%b1-%cf%84%ce%b7/ why do bodybuilders use steroids
https://jornalfax.net/index.php/2024/01/12/falta-de-medicamentos-para-tuberculose-preocupa-hospital-sanatorio/ Valley
https://community.theclearwaytoconceive.com/question/9-what-your-parents-teach-you-about-shop-wireless-headphones/ what is the closest thing to steroids
https://nafbeautysupply.com/product/rene-furterer-enhancing-dry-oil-hair-and-body-oil-5-sens/ anavar gains
https://portalraizes.com.br/potencial-e-importancia-do-trecho-da-ba-411-entre-conceicao-do-coite-e-ichu-via-onca-e-juazeirinho/ what is the safest steroid for building muscle
https://itsyourdigital.com/why-website-presence-is-important-2025/ are any steroids legal
https://fuchs-press.com/poetry/karusel/ losing weight on steroids
https://community.theclearwaytoconceive.com/question/10-things-youve-learned-about-preschool-to-help-you-get-a-handle-on-upvc-doors-windows/ valley
https://template82.webekspor.com/?p=1 Valley
https://amigogaming.uk/community-and-social-aspects-of-chaos-crew-2-slots/ what is the best steroid to take
https://setouti.click/2024/11/04/横浜ベイスターズ日本一!!/ buy steriods
https://www.gross.mx/index.php/blog/item/13-a-post-with-soundcloud oral tren before and after
https://amigogaming.uk/community-and-social-aspects-of-chaos-crew-2-slots/ what steroids Are Illegal
https://majesticglobaltourism.com/product/one-day-deep-sea-fishing-barbados/ winstrol fat loss
https://fotohana.fi/miten-parantaa-ajotaitoja-kilpa-ajoissa/ valley
References:
https://kaadaikulam.org/tiny-scientists-on-the-loose-preschool-science-wonders/
https://symptoms-disease.com/omission-of-the-upper-eyelid · September 28, 2025 at 1:05 pm
does winstrol work
https://iagamers.com/indiana-jones-and-the-great-circle-a-game-of-wits-mystery-guide/ anavar prescription cost
https://innovatedblindsconcepts.com/business-directory/empire-custom-windows/ which one of the following is not a potential danger of anabolic steroids?
http://www.bikerentalbali.com/luchshee-onlajn-kazino-na-realnye-dengi-frispiny-8/ what are the side effects of coming off steroids
https://eightloop.click/2024/08/25/244/comment-page-766/ what are steroids classified as
https://aussieplantlovers.com/the-olla-pot-revolution-in-australian-gardens/ gnc Alternative
http://schifffahrtsmuseum-nordhorn.de/nl/Gaestebuch.html Beginner steroid cycle for sale
https://community.theclearwaytoconceive.com/question/9-what-your-parents-teach-you-about-shop-wireless-headphones/ steroids for fat loss
https://tarisboost.com/services/babyface-champions-gear-boost/ steroids side effects in males
https://cloudnativeblogs.in/top-java-debugging-tools-for-efficient-application-development/ what is the closest thing to steroids that is legal
https://eurecaformedling.se/property/valkand-pub-och-restaurang-topp-lage-i-uppland/shutterstock_78414787/ the rock steriods
https://medmaxbusinesssolutions.com/2024/03/20/how-solar-panels-work-a-closer-look-at-photovoltaic-systems/ weight Lifting stacks
https://papocultura.com.br/rua-vigario-bartolomeu/ anabolic steroids canada
https://eleccionespresidencialeschile.cl/distancia-chama/ Winstrol illegal
https://nordicnepal.com/tour/kathmandu-kultur-tur/ valley
https://www.lucavincitore.com/ira-di-rita-dalla-chiesa-mi-hanno-scritto-che-sono-adottata/ side effects of women taking steroids
https://nordicnepal.com/tour/kathmandu-kultur-tur/ fouseytube steroids
http://aiki-evolution.jp/yy-board/yybbs.cgi valley
https://digitalsquare.com.ng/2021/06/28/ anabolic steroids and pregnancy
References:
what is steroid for (https://symptoms-disease.com/omission-of-the-upper-eyelid)
wood-swordcricket.com · September 28, 2025 at 1:59 pm
buying steroids online safely
https://auto-gully.com/blog/renault-triber-kwid-kiger-offer-discounts-up-to-%e2%82%b990000-this-june/ Valley
https://woodstocksbest.com/understand-the-background-of-design/ Valley
https://newsstroy.kharkiv.ua/v-finlyandii-zapustili-v-rabotu-samuyu-bolshuyu-peschanuyu-batareyu-v-mire.html prescription steroid
https://gsa9game.net/888okey/ how strong can you get without steroids
https://craftnmoreshop.com/from-heart-to-hand-the-story-behind-every-handmade-masterpiece/ valley
https://preahthortesna.com/?p=1098 legal steroids dbol reviews
https://www.fundamentale.ro/notiuni-de-baza-despre-cum-functioneaza-internetul best steroid cycle for bulking
https://icanada.online/firefighters-family-pushes-for-training-school-to-close-following-death/ are testosterone boosters steroids
https://firsturl.de/B6E3u43 steroids are composed of
https://www.onverze.com/elon-musk-unveils-optimus-gen-2-robot-watch-video/ basic structure of a steroid
https://mo.investkuban.ru/?ID=83151.html ipf powerlifting results
https://jornalfax.net/index.php/2024/01/08/governo-encerra-radio-global-fm-cujo-acionista-maioritario-e-manuel-rabelais/ steroids australia
https://shanghati.org/archives/2123 Synthetic People
https://houseforart.com/product/blue-purple-improvisation-painting-wooden-framed-painting-wall-art/ Best Muscle Supplements At Gnc
https://okosatellitegame.com/silktest-orgs-games-galore-a-comprehensive-exploration-of-automated-testing-in-the-gaming-industry/ valley
https://gblshopeu.org/shop/buy-20l-gbl-online/ body building dangers
https://template166.webekspor.com/driving-towards-diversity-toyotas-commitment-to-inclusion-and-equality/ alpha cuts advanced cutting agent
https://jqkbonus.info/?p=1 Top Steroids Online Reviews
References:
rx steroids (https://wood-swordcricket.com/product/armour-gx5-3-0-batting-gloves-white-d-green-green/)
Www.Valcenoweb.It · September 28, 2025 at 5:51 pm
novice steroid cycle
References:
Natural Prednisone Alternatives (https://www.valcenoweb.it/2017/02/23/chiacchiere-e-frittelle-si-festeggia-il-carnevale/)
beginner steroids · September 28, 2025 at 7:04 pm
best steroids on the market
https://git.ellinger.eu/aundreabundey valley
https://qarisound.com/carin256365733 muscle building steroids for sale
https://git.karma-riuk.com/marihux803513 Steroids That Make You Lean
http://git.pushecommerce.com/felipeshoemake bob paris steroids
http://begild.top:8418/doris83y984400 Steroid Stacks And Cycles
https://bantoomusic.com/celinda42q3254 Flex Stack Gnc
https://camtalking.com/@hildawreford83 are steroids a drug
https://gitea.mulberrypos.ru/albertclifton where can i buy steroids for bodybuilding
https://datingmywish.com/@jasonbruni8627 How Does Anabolic Steroids Affect The Body
https://git.omnidev.org/christentejada Valley
https://code.ioms.cc/collinpatino9 Anabolic Steroids are which of the following
https://www.gitmate.dev/gudrungass0709 Testosterone Stack
https://git.wisder.net/daveharder944 best Ripping supplements
http://guishenking.cloud:3000/franciseoff099 deca boost
https://tayartaw.kyaikkhami.com/ellien47428872 steroid before after
https://git.inmind-lab.com/candacelavalle valley
https://git.tordarus.net/denicetancred Best Steroid For Strength And Cutting
https://gitea.sguba.de/londerrick207 What do steroids do to Your Body
References:
https://www.percyroberts.com/dorthymcgraw70
Lino · September 28, 2025 at 7:39 pm
bodybuilding drug list
https://airplayradio.com/finncoombs1322 valley
https://git.stit.tech/barney57r12560 what do all steroids have in common
https://srsbkn.eu.org/concepcion58n weight lifting steroids
http://git.edazone.cn/edwinboelke567 Fun facts about steroids
https://quenly.com/@peteolive54851 valley
http://git.modelhub.org.cn:980/archermcdowell most effective steroid for muscle gain
https://git.the-kn.com/gonzalobourass valley
https://git.qingbs.com/elidaschutt76 What Is A Legal Steroid For Muscle Building
https://ngoma.app/beckyo2952710 what do prescribed steroids do
https://music.birbhum.in/nonabelgrave47 Valley
http://geekhosting.company/doyle334851536 valley
https://ldcv.de/krystlegrattan dianabol tablets results
https://aipod.app/malindabavin45 anabolic steroids are appropriately prescribed to
https://www.musicsound.ca/jeanned4378651 clen vs anavar
https://git.camus.cat/chasesharpe57 valley
https://git.atomos.io/flynnx60320535 reddit steroids before and after
https://git.outsidecontext.solutions/athenahennessy tren workout supplement
https://www.meikeyun.com/danityrell6203 valley
References:
steroid injection for muscle growth (https://music.drepic.com/enriquetabirmi)
Pokesoul.Com · September 29, 2025 at 12:10 am
long term anabolic steroid use
References:
top steroids Sites (https://pokesoul.com/@hermanbelt3563)
maintain.basejy.com · September 29, 2025 at 2:00 am
test pills steroids
References:
What is the closest thing to steroids that is legal, https://maintain.basejy.com/erqmaddison435,
basic steroid cycle · September 29, 2025 at 3:02 am
gnc supplements with steroids
References:
https://datebaku.com/@cooperdundas1
binance Konta Izveidosana · September 29, 2025 at 4:54 am
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
https://git.winscloud.net/ameebody402187 · September 29, 2025 at 8:15 am
2ahukewik8-seu8vnahuhgz4khrreaaqq_auoaxoecaeqaq|the best steroids for muscle growth
References:
how much testosterone should i take to build muscle (https://git.winscloud.net/ameebody402187)
anabolic steroids stacks · September 29, 2025 at 8:20 am
top bodybuilding stacks
https://aipod.app/malindabavin45 legal steroids to gain weight
https://deepsound.thenexivo.com/hamishkhh6896 valley
https://katambe.com/@joep0531013677 anabolic steroids for muscle building
https://www.toparma.com/collinwawn2299 taking steroids for the first time
https://git.ajattix.org/fletchertovell valley
https://get.meet.tn/@abqelvis72085 what effects does steroids have on your body
http://tools.refinecolor.com/bettinavillalp the closest thing to steroids
http://dev.baidubaoche.com/anton20756275 best muscle building fat burning stack
https://quickdate.arenascript.de/@elouiseharr514 arnold schwarzenegger steroid regimen
https://git.qingbs.com/elidaschutt76 valley
http://dev.baidubaoche.com/anton20756275 prescription steroid pills
https://kition.mhl.tuc.gr/antoniomartino Where Can I Get Dianabol
https://gitea.potatox.net/eulahkallas796 what’s the best testosterone steroid
https://git.yuhong.com.cn/grady97c257842 Best Test for cutting cycle
https://git.ultra.pub/caitlyn3813206 winstrol tablets price
https://git.aopcloud.com/gertiedeaton90 valley
https://afritunes.net/erniedegraves8 valley
https://m.hrjh.org/bettinastrode Dianabol Hair loss
References:
https://loveis.app/@andreascarberr
serbiatenniscenter.org · October 1, 2025 at 9:58 pm
free usa bingo, canadian roulette free game and canadian poker 2 novomatic online, or sun bingo uk
Here is my blog – Bubble craps machine blackhawk – serbiatenniscenter.org –
huaang6688.gnway.cc · October 2, 2025 at 9:51 pm
gain muscle fast pills
References:
steroid vs natural physique – http://huaang6688.gnway.cc:3000/lmujoni8194621 –
https://molchanovonews.ru/user/chestroad6/ · October 3, 2025 at 5:59 am
ripped muscle x at gnc
References:
https://molchanovonews.ru/user/chestroad6/
Finn · October 4, 2025 at 12:45 am
can you play online pokies in united states for real
money, aristocrat pokies online united kingdom and united statesn casinos no deposit bonus, or united kingdom
poker machines online free
Feel free to visit my homepage :: ameristar
blackjack rules [Finn]
https://play.ntop.tv/ · October 4, 2025 at 2:00 pm
i roids
References:
https://play.ntop.tv/user/wheelgarage8/
gratisafhalen.be · October 5, 2025 at 12:50 am
women on steroids side effects pictures
References:
https://gratisafhalen.be/author/curveparrot98/
https://www.folkd.com/ · October 5, 2025 at 4:03 am
free steroids pills
References:
https://www.folkd.com/submit/dreambridge1.werite.net/sustanon-comprehensive-cycle-overview-dosage-perks-and-risks/
https://iotpractitioner.com/forums/users/pullfur37/ · October 5, 2025 at 8:48 am
the best steroids for sale
References:
https://iotpractitioner.com/forums/users/pullfur37/
https://www.netsdaily.com · October 6, 2025 at 1:52 am
most androgenic steroid
References:
https://www.netsdaily.com/users/ryberg.short
images.google.cf · October 6, 2025 at 2:43 am
steroid tablets for gym
References:
https://images.google.cf/url?q=https://apunto.it/user/profile/250813
images.google.co.za · October 6, 2025 at 4:30 am
steroids replacements
References:
https://images.google.co.za/url?q=https://md.swk-web.com/T6XVisHASNC_dqrN31eaRw/
maps.google.ae · October 6, 2025 at 4:46 am
supplement steroid
References:
https://maps.google.ae/url?q=https://www.silverandblackpride.com/users/kent.pacheco
true blue casino no deposit Free chip 2021 · October 6, 2025 at 5:15 pm
free chip online true blue casino no deposit Free chip 2021 australia, online gambling laws in canada and free bonus no deposit roulette usa,
or sun bingo uk
www.studioincontroluce.it · October 7, 2025 at 9:27 am
25 free spins casino new zealand, pokies australia revenue and free spins no deposit keep
your winnings uk, or free bonus casino uk
Review my site – How many Casinos does penn gaming own [http://www.studioincontroluce.it]
Goplayslots.Net · October 8, 2025 at 2:17 am
888 poker promotion code united states, how many the top
online pokies and casinos in australia and juki slot machine, or £10 no deposit slot bonus uk 2021
Feel free to visit my web site … Goplayslots.Net
Casino Roulette Odds Payout · October 8, 2025 at 6:26 am
play free pokies usa, united kingdom Casino Roulette Odds Payout in vegas and echeck casinos united kingdom, or online slots united states reddit
gofleeks.com · October 8, 2025 at 4:07 pm
dianabol sustanon cycle
https://christianmail.tv/@laurencei6964?page=about https://christianmail.tv
http://www.huastech.com.cn:81/elissa69774424/gitea.ucarmesin.de4711/wiki/Maximize-Gains:-Effective-Dbol-Tren-Cycle-For-Bodybuilders http://www.huastech.com.cn:81/elissa69774424/gitea.ucarmesin.de4711/wiki/Maximize-Gains:-Effective-Dbol-Tren-Cycle-For-Bodybuilders
https://gitea.svc.obaa.cloud/breannadillon6 gitea.svc.obaa.cloud
http://git.jishutao.com/vickieebr93877 git.jishutao.com
https://projects.om-office.de/delilaheames4/6609679/-/issues/1 projects.om-office.de
https://smartcampus-seskoal.id/streaming/@traciolmstead1?page=about smartcampus-seskoal.id
http://git.in.ahbd.net/vzppenny090870 git.in.ahbd.net
https://teambattle.dscun.cn/claudiacastleb teambattle.dscun.cn
https://zurimeet.com/@hassan61933603 zurimeet.com
http://git.chelingzhu.com/gerardoquinlan git.chelingzhu.com
https://gitlab.rightease.com:443/jillt149666540/gitea.mpc-web.jp8411/-/issues/1 gitlab.rightease.com
https://git.z1.mk/marcelohgu088 https://git.z1.mk/marcelohgu088
https://git.partners.run/ahmedketner76 git.partners.run
https://video.cheeft.com/@erikabooze6832?page=about video.cheeft.com
https://teambattle.dscun.cn/claudiacastleb https://teambattle.dscun.cn/claudiacastleb
https://lab.nltvc.com/phillipspeed32/cupido.prestigioapps.com2009/-/issues/1 https://lab.nltvc.com/phillipspeed32/cupido.prestigioapps.com2009/-/issues/1
https://postyourworld.com/@darrenscanlan?page=about https://postyourworld.com/@darrenscanlan?page=about
https://gogs.monkeybox.org/cecileherbert gogs.monkeybox.org
References:
https://gofleeks.com/read-blog/667_deca-durabolin-uses-benefits-and-side-effects.html
omegat.dmu-medical.de · October 8, 2025 at 4:29 pm
dianabol only cycle
http://git.linkupx.com/shantelltilley/git.agusandelnorte.gov.ph1991/wiki/Beginner-Friendly-Steroid-Cycles:-A-Comprehensive-Guide-UK-Anabolic-Steroids-Shop-Top-Rated-And-Trasted-Steroids-Source http://git.linkupx.com/
https://git.obo.cash/omachau6547075 https://git.obo.cash/
http://begild.top:8418/julikeble5874 http://begild.top:8418/julikeble5874
https://hypmediagh.com/malissavaccari https://hypmediagh.com/malissavaccari
https://rictube.com/@jeanettwomack?page=about rictube.com
https://mp3diary.com/lauriedeeds070 mp3diary.com
https://git.atomos.io/abigaillamingt git.atomos.io
http://git.jiankangyangfan.com:3000/marielooney761 git.jiankangyangfan.com
https://chatterchat.com/read-blog/29312_dianabol-and-its-use-in-steroid-cycles.html https://chatterchat.com
https://gitlab.ui.ac.id/isidropoupinel gitlab.ui.ac.id
https://git.saidomar.fr/artshick069719 https://git.saidomar.fr/
https://git.aelhost.com/gleny573443210 https://git.aelhost.com/gleny573443210
http://git.linkupx.com/vvxmercedes441 http://git.linkupx.com
https://myafritube.com/@windyhodgson66?page=about myafritube.com
https://easyconnect.fun/@kgvkristal6803 https://easyconnect.fun
https://gog.taletrail.fi/lacytse6759485 gog.taletrail.fi
https://xajhuang.com:3100/trisha17m35681 xajhuang.com
https://www.humlog.social/read-blog/4209_test-e-boldenone-amp-dianabol-cycle.html https://www.humlog.social/
References:
https://omegat.dmu-medical.de/kennethpepper1/kenneth2007/wiki/5-Best-Anabolic-Stacks-And-Steroids-For-Beginners
http://www.chatgpt918.Top:3000/gabrielalightn · October 8, 2025 at 5:59 pm
dianabol injection cycle
https://git.penwing.org/rodgerarent287 Valley.md
http://git.hjd999.com.cn/starlapatrick Test Dianabol Cycle
https://ouptel.com/read-blog/154747_pdf-dianabol-unveiled-a-systematic-review-of-methandrostenolone.html dianabol cycle before and after
https://git.srv.ink/sal4068945690 Injectable dianabol cycle
https://git.notoxops.com/raleigh6117318 sustanon dianabol cycle
http://code.kfw.net/alfredo94b4539 valley.Md
https://connect.mopays.com/read-blog/22242_dianabol-cycle-guide-dbol-dosage-timing-for-best-result.html dianabol dosage cycle
http://gitea.mintelcn.com/naomicardus97 dianabol and test cycle
https://git.bloade.com/ernestine88x3 Sustanon dianabol cycle
https://gitlab.companywe.co.kr/mindy562098083 testosterone trenbolone dianabol cycle
https://duncanvilledash.com/@halvergara8283?page=about 10Mg Dianabol cycle
https://git.gearcraft.org/jaistory31327/jai1983/wiki/Dianabol+And+Testosterone+Cycle+Latest+News%252C+Updates+%2526+Articles+On+Dianabol+And+Testosterone+Cycle+Page+4 Sustanon And dianabol cycle
http://git.szmicode.com:3000/natisharobey1/natisha2024/wiki/Dianabol-Results%3A-With-Before-and-After-Pictures how long is a dianabol cycle
https://kf.hebrewconnect.tv/@biojonelle159?page=about what to take after dianabol cycle
http://hualiyun.cc:3568/brycebriseno02 valley.Md
https://supardating.com/@pansyheadley0 Dianabol Stack cycle
https://git.lakaweb.com/issacarnold83 Test e And dianabol Cycle
https://gitea.synapsetec.cn/kandyf0606221 sustanon dianabol cycle
References:
testosterone dianabol cycle (http://www.chatgpt918.top:3000/gabrielalightn)
Dianabol winstrol cycle · October 8, 2025 at 6:15 pm
anavar and dianabol cycle
http://dev.hsfuel.com:3000/tedshuster7941 4 week dianabol cycle
https://gitea.jobiglo.com/brigidagoforth dianabol beginner cycle
https://gogs.pinadshub.com/millardjenkins dianabol only cycle for beginners
https://git2.ujin.tech/phillipleavitt what to take after dianabol cycle
https://gitlab.tu-dortmund.de/albertinagerri 4 Week dianabol Cycle
https://virnal.com/@jayhough456964?page=about dianabol and winstrol cycle
https://git.successkaoyan.com/tracielascelle valley.md
https://ralphouensanga.com/read-blog/45681_dbol-pills-benefits-in-2025-muscle-growth-dosage-amp-safe-use-guide.html dianabol injection cycle
https://www.telegraphyx.com/edgardoweeks05 valley.md
https://music.shaap.tg/brendanplott22 dianabol first Cycle
https://video.xucheng-edu.com/@adelaidasayre3?page=about test Deca dianabol cycle
http://git.datanest.gluc.ch/sandracamara3 Valley.Md
https://git.wisder.net/linwoodcavill5 Dianabol Cycle Guide
http://code.sz-chaohui.cn/veronamccord69 steroid dianabol cycle
http://dev.baidubaoche.com/courtneystyers Valley.Md
https://sameday.iiime.net/read-blog/4175_dianabol-first-cycle-pharma-trt.html how to take dianabol first cycle
https://lesla.com/@juliewienholt Valley.md
https://jioxe.com/read-blog/18346_nandrolone-uses-benefits-amp-side-effects.html dianabol anavar cycle
References:
https://www.herzog-it.de/lavonolson5778
finalresult.buzz · October 9, 2025 at 1:52 am
dianabol 50mg cycle
https://loveis.app/@ftsclark16361 https://loveis.app/@ftsclark16361
http://shqkxh.org:3000/elouiseobrien http://shqkxh.org:3000/elouiseobrien
https://mixtify.top/qccjolie126177 mixtify.top
https://gitea.ochoaprojects.com/elberto1214962 https://gitea.ochoaprojects.com/elberto1214962
https://weshareinterest.com/@aprilacl701202 weshareinterest.com
https://git.creeperrush.fun/eliaslasley824 https://git.creeperrush.fun/eliaslasley824
https://date.etogetherness.com/@charline30723 https://date.etogetherness.com/@charline30723
http://git.yanei-iot.com:600/christinewelli git.yanei-iot.com
https://git.yuhong.com.cn/candramanson8 git.yuhong.com.cn
https://www.ituac.com/berniecedowler https://www.ituac.com/berniecedowler
https://www.arabianmatrimony.com/@aleidalemberg4 http://www.arabianmatrimony.com
http://gitea.yunshanghub.com:8081/deanajessup373 gitea.yunshanghub.com
https://quickdate.click/@coyrector13954 https://quickdate.click/
https://git.agusandelnorte.gov.ph/darby17v405817 https://git.agusandelnorte.gov.ph/darby17v405817
https://gitea.ideaopen.cn/angelpelensky gitea.ideaopen.cn
https://git.agusandelnorte.gov.ph/darby17v405817 git.agusandelnorte.gov.ph
https://git.rootfinlay.co.uk/ezzjeffry57384 https://git.rootfinlay.co.uk
https://lius.familyds.org:3000/carolinec24202 https://lius.familyds.org/
References:
https://finalresult.buzz/celindacountry
casino blacklist singapore · October 9, 2025 at 7:05 am
new zealandn online casino blacklist singapore 5 dollar min deposit,
gambling statistics australia 202 and online
casino 5 dollar minimum deposit united states,
or td united states visa debit gambling
Gayle · October 9, 2025 at 9:16 am
no wager united statesn casino, european roulette hints uk and united kingdom online poker news, or australia top when does chinook winds casino open (Gayle)
Pferderennen Wetten Deutschland · October 9, 2025 at 2:27 pm
bester willkommensbonus sportwetten
Feel free to visit my web page: Pferderennen Wetten Deutschland
Wett Tipps Basketball Nba · October 10, 2025 at 2:05 pm
online sportwetten schleswig holstein
Here is my web blog Wett Tipps Basketball Nba
http://www.annunciogratis.net/author/sandoffice80 · October 10, 2025 at 8:49 pm
deca dianabol test cycle
http://mozillabd.science/index.php?title=cashnorwood9674 http://mozillabd.science/index.php?title=cashnorwood9674
https://www.udrpsearch.com/user/bailknife05 https://www.udrpsearch.com/
https://firsturl.de/q64960e https://firsturl.de
https://maps.google.com.pr/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect maps.google.com.pr
https://www.bitsdujour.com/profiles/mLyYkA https://www.bitsdujour.com/
https://www.google.co.vi/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect http://www.google.co.vi
https://urlscan.io/result/0199c392-25d2-764c-9804-7ba97ea2d37e/ urlscan.io
https://www.24propertyinspain.com/user/profile/1235395 https://www.24propertyinspain.com/
https://www.google.com.co/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect https://www.google.com.co
https://may22.ru/user/winggallon97/ https://may22.ru
https://telegra.ph/Dianabol-Usage-Guide-Common-Questions-and-Safe-Use-Strategies-10-08 https://telegra.ph/Dianabol-Usage-Guide-Common-Questions-and-Safe-Use-Strategies-10-08
https://telegra.ph/Dianabol-Usage-Guide-Common-Questions-and-Safe-Use-Strategies-10-08 telegra.ph
https://buketik39.ru/user/boltblade94/ buketik39.ru
https://images.google.com.pa/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect images.google.com.pa
https://www.google.co.vi/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect http://www.google.co.vi
https://bailcredit74.werite.net/dianabol-role-and-timing-in-steroid-cycles bailcredit74.werite.net
https://prpack.ru/user/briancause14/ prpack.ru
https://autovin-info.com/user/plowsampan43/ autovin-info.com
References:
http://www.annunciogratis.net/author/sandoffice80
viewcinema.ru · October 10, 2025 at 9:22 pm
testosterone cypionate and dianabol cycle
https://muhammad-ali.com.az/user/spoonsign6/ muhammad-ali.com.az
https://prpack.ru/user/subwayenemy31/ prpack.ru
http://karayaz.ru/user/garagegear22/ karayaz.ru
http://karayaz.ru/user/framebridge09/ karayaz.ru
https://motionentrance.edu.np/profile/foldhair14/ motionentrance.edu.np
http://stroyrem-master.ru/user/routerneon20/ stroyrem-master.ru
https://www.argfx1.com/user/walletrandom95/ https://www.argfx1.com/user/walletrandom95/
http://king-wifi.win//index.php?title=mccollumsellers4830 http://king-wifi.win/
https://viewcinema.ru/user/liquidlynx61/ https://https://viewcinema.ru/user/commaitaly4//user/liquidlynx61/
https://firsturl.de/eWQlUbb firsturl.de
https://images.google.com.gt/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect images.google.com.gt
https://maps.google.com.pr/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect https://maps.google.com.pr/
https://www.google.co.uz/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect http://www.google.co.uz
https://rentry.co/nuwy9bcm rentry.co
https://ebra.ewaucu.us/index.php?page=user&action=pub_profile&id=107966 ebra.ewaucu.us
https://telegra.ph/Dianabol-101-Beginners-Cycle-Guide–Results-Dosage-Charts–Timing-10-08 https://telegra.ph/Dianabol-101-Beginners-Cycle-Guide–Results-Dosage-Charts–Timing-10-08
https://freebookmarkstore.win/story.php?title=post-dianabol-recovery-discover-the-optimal-pct-protocols freebookmarkstore.win
https://www.bitsdujour.com/profiles/mLyYkA http://www.bitsdujour.com
androidmobiles.com · October 10, 2025 at 9:57 pm
sportwetten mit startguthaben ohne einzahlung (androidmobiles.com)
geld zurück
https://www.instapaper.com · October 10, 2025 at 10:12 pm
dianabol cycle chart
https://coolpot.stream/story.php?title=winstrol-in-bodybuilding-a-comprehensive-guide-to-dosage-benefits-risks-and-purchase-options coolpot.stream
https://a-taxi.com.ua/user/bargeperch5/ a-taxi.com.ua
https://images.google.be/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect images.google.be
https://freebookmarkstore.win/story.php?title=post-dianabol-recovery-discover-the-optimal-pct-protocols https://freebookmarkstore.win
https://peatix.com/user/27956263 https://peatix.com
https://molchanovonews.ru/user/bathlayer20/ https://molchanovonews.ru/user/bathlayer20
http://www.annunciogratis.net/author/wormhair17 http://www.annunciogratis.net
https://www.instapaper.com/p/16989208 http://www.instapaper.com
http://09vodostok.ru/user/flowerpaul8/ http://09vodostok.ru/user/flowerpaul8
https://carroll-francis.federatedjournals.com/dianabol-demystified-pros-cons-and-cycle-strategies https://carroll-francis.federatedjournals.com/dianabol-demystified-pros-cons-and-cycle-strategies
https://muhammad-ali.com.az/user/quaildog71/ https://muhammad-ali.com.az/
http://king-wifi.win//index.php?title=mccabenorth5324 king-wifi.win
https://autovin-info.com/user/riceglue3/ https://autovin-info.com/
https://viewcinema.ru/user/commaitaly4/ https://viewcinema.ru/user/commaitaly4
https://locketart39.bravejournal.net/the-core-of-the-web locketart39.bravejournal.net
https://www.instapaper.com/p/16989459 https://www.instapaper.com/p/16988934/
https://coolpot.stream/story.php?title=winstrol-in-bodybuilding-a-comprehensive-guide-to-dosage-benefits-risks-and-purchase-options https://coolpot.stream
https://images.google.com.na/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect https://images.google.com.na/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect
https://alvoradapflege.de · October 11, 2025 at 12:38 pm
handicap wetten bwin
Here is my blog post :: sportwetten anbieter mit deutscher lizenz [https://alvoradapflege.de]
binance code · October 11, 2025 at 7:51 pm
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
https://ste-Bmms.com/Fuballwetten-osterreich/ · October 12, 2025 at 3:28 am
sportwette ohne oasis
My web-site … wettbüro aufmachen – https://ste-Bmms.com/Fuballwetten-osterreich/,
iffezheim pferderennen wetten · October 12, 2025 at 5:06 am
strategie bei sportwetten
Also visit my web site :: iffezheim pferderennen wetten
Dian · October 12, 2025 at 8:09 am
gratiswetten
My web site: die besten wettanbieter online (Dian)
https://haslaws.com/Big-sports-bet-win · October 12, 2025 at 11:56 am
curacao wettanbieter
Feel free to visit my website; wetten auf pferderennen (https://haslaws.com/Big-sports-bet-win)
Wetten Ohne Einzahlung Geizkragen · October 12, 2025 at 1:33 pm
beste wettseite
my web blog; Wetten Ohne Einzahlung Geizkragen
Quotenvergleich Sportwetten · October 12, 2025 at 5:45 pm
wetten österreich
Feel free to visit my web page: Quotenvergleich Sportwetten
peatix.com · October 12, 2025 at 7:40 pm
dianabol only cycle for beginners
https://stringsign4.bravejournal.net/whats-the-ideal-post-dianabol-recovery-plan https://stringsign4.bravejournal.net/whats-the-ideal-post-dianabol-recovery-plan
https://firsturl.de/cq27IuM firsturl.de
http://karayaz.ru/user/lankey2/ karayaz.ru
https://www.google.co.cr/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect http://www.google.co.cr
https://freebookmarkstore.win/story.php?title=post-dianabol-recovery-discover-the-optimal-pct-protocols https://freebookmarkstore.win
https://maps.google.fr/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect https://maps.google.fr/
https://telegra.ph/An-In-Depth-Handbook-for-Planning-Anadrol-Cycles-10-08 https://telegra.ph/An-In-Depth-Handbook-for-Planning-Anadrol-Cycles-10-08
https://www.google.com.ai/url?q=https://www.valley.md/dianabol-before-and-after-results-you-can-expect http://www.google.com.ai
https://www.faax.org/author/riskair77/ http://www.faax.org
https://viewcinema.ru/user/waygrip75/ viewcinema.ru
https://urlscan.io/result/0199c397-ec2d-73c9-8741-8e19a7b6ecf9/ https://urlscan.io/result/0199c397-ec2d-73c9-8741-8e19a7b6ecf9
https://mensvault.men/story.php?title=dianabol-cycle-mastering-5-mg-10-mg-and-50-mg-%E2%80%93-training-your-mind-to-sculpt-your-body mensvault.men
https://urlscan.io/result/0199c3a2-4851-74ee-9be5-5c24a34d4544/ urlscan.io
https://urlscan.io/result/0199c3ac-f565-76c2-9706-ae9f41c2d5b9/ urlscan.io
https://livebookmark.stream/story.php?title=dianabol-testosterone-cycle-dosages-outcomes-and-expert-guidance https://livebookmark.stream/story.php?title=dianabol-testosterone-cycle-dosages-outcomes-and-expert-guidance
https://graph.org/Dianabol-Use-Guide-Common-Questions–Safe-Use-Strategies-10-08 https://graph.org/Dianabol-Use-Guide-Common-Questions–Safe-Use-Strategies-10-08
https://buketik39.ru/user/riverplier44/ buketik39.ru
https://skitterphoto.com/photographers/1601711/blalock-jonassen https://skitterphoto.com/photographers/1601711/blalock-jonassen
References:
https://peatix.com/user/27956492
Rueben · October 13, 2025 at 10:02 am
eigene wetten erstellen app
Here is my blog post … sportwetten guthaben ohne
einzahlung (Rueben)
deutschland ungarn wett tipp · October 13, 2025 at 10:44 am
beste wetter-app österreich
My page :: deutschland ungarn wett tipp
https://mozillabd.science · October 13, 2025 at 12:24 pm
dianabol beginner cycle
http://pattern-wiki.win/index.php?title=pagecoffee62 Valley.md
https://lovewiki.faith/wiki/Dbol_Cycle_Information_To_Stacking_Dosages_And_Unwanted_Effects dianabol winstrol cycle
https://sciencebookmark.top/item/296376 dianabol and anavar cycle
http://tellmy.ru/user/dinnerviola3/ Dianabol Only Cycle Reddit
https://gallegos-dohn-3.technetbloggers.de/anavar-and-test-cycle-advantages-dosage-unwanted-effects-and-optimum-stacking-information how to take dianabol cycle (https://mozillabd.science/wiki/Greatest_Cutting_And_Bulking_Steroids_Buy_Oral_Steroid_Stacks)
https://topbookmarks.cloud/item/404705 valley.md
https://mozillabd.science/wiki/Greatest_Cutting_And_Bulking_Steroids_Buy_Oral_Steroid_Stacks Dianabol Beginner Cycle
https://peatix.com/user/27515525 dianabol pct cycle
https://mozillabd.science/wiki/Greatest_Cutting_And_Bulking_Steroids_Buy_Oral_Steroid_Stacks valley.md
https://xn—6-jlc6c.xn--p1ai/user/riskhelium0/ anavar dianabol cycle
https://noticias-sociales.top/item/403810 testosterone dianabol cycle
http://karayaz.ru/user/milefarm3/ dianabol pct cycle
https://yogaasanas.science/wiki/Dianabol_Cycle dianabol Testosterone Cycle
https://yogaasanas.science/wiki/Dianabol_Cycle_Dianabol_For_Bodybuilding Valley.md
https://farmerdelete8.werite.net/three-best-steroids-for-novices-plus-three-to-avoid Dianabol Only cycle
https://sciencewiki.science/wiki/Trenbolone_Acetate_An_Summary testosterone cypionate and dianabol cycle
https://www.udrpsearch.com/user/priceradar5 testosterone enanthate and dianabol cycle
https://pin-it.top/item/404963 dianabol deca test cycle
Pobeda.Altspu.Ru · October 13, 2025 at 2:22 pm
wetten und gewinnen
Also visit my homepage :: Spiel Wette (Pobeda.Altspu.Ru)
heavenarticle.Com · October 13, 2025 at 2:48 pm
what to take with dianabol cycle
https://hikvisiondb.webcam/wiki/Dbol_Dianabol_Cycle_How_Robust_Is_Methandrostenolone what to take with dianabol cycle
https://www.argfx1.com/user/atmsunday3/ dianabol only cycle reddit
http://ezproxy.cityu.edu.hk/login?url=https://www.valley.md/dianabol-cycle-benefits-and-risks dianabol 6 week cycle
http://karayaz.ru/user/pisceslyre1/ dianabol side effects after one cycle
https://personalbookmark.space/item/296128 deca dianabol cycle
https://lovebookmark.date/story.php?title=turinabol-vs-anavar-which-is-the-higher-steroid first dianabol cycle
https://u.to/S0BTIg Dianabol cycle benefits
https://charmed-serial.online/user/mathbody1/ dianabol And testosterone Cycle for beginners
https://aryba.kg/user/duckphone0/ test deca dianabol cycle
https://walletreport6.werite.net/ready-for-new-cycle-take-a-look-at-deca-mast-dbol-pics-included-pharma-trt testosterone and dianabol cycle
https://newssignet.top/item/406066 dianabol cycle only
https://opensourcebridge.science/wiki/Whats_Primobolan_Benefits_Dosage_And_Risks_Of_This_In_Style_Cutting_Steroid test and dianabol cycle
https://xn—-7sbarohhk4a0dxb3c.xn--p1ai/user/yachtstar53/ valley.md
https://opensourcebridge.science/wiki/Dianabol_Dbol_The_Ultimate_Word_Guide sustanon and dianabol cycle
https://leth-kold-3.federatedjournals.com/jacked-rising-use-of-steroids-and-different-performance-enhancing-medicine-carries-dangers dianabol stack cycle
https://may22.ru/user/hubviola7/ dianabol cycle before and after
https://www.haphong.edu.vn/profile/mcknightshrwalker12363/profile dianabol Cycle Results
https://firsturl.de/kbyeufA dianabol deca cycle
References:
dianabol and Test cycle (https://heavenarticle.com/author/firedpencil56-293105/)
https://www.arabianmatrimony.com/@claudioshackel · October 13, 2025 at 3:25 pm
dianabol deca test cycle
http://www.factory18.cn/krystleo04349 http://www.factory18.cn/krystleo04349
https://meeting2up.it/@rebekahsalaam https://meeting2up.it/@rebekahsalaam
https://www.soundofrecovery.org/lorenzo74p284 https://www.soundofrecovery.org/lorenzo74p284
https://git.getmind.cn/jeremyshenton8 https://git.getmind.cn/jeremyshenton8
https://meeting2up.it/@rebekahsalaam https://meeting2up.it/@rebekahsalaam
https://www.arabianmatrimony.com/@leonieoconor04 arabianmatrimony.com
https://mixtify.top/qccjolie126177 https://mixtify.top
https://git.noxxxx.com/millardroxon8 git.noxxxx.com
https://saga.iao.ru:3043/sterlingnag580 saga.iao.ru
http://gitea.ucarmesin.de/tnnmariel11877 gitea.ucarmesin.de
https://git.sleepingforest.co.uk/arliesamuel46 git.sleepingforest.co.uk
http://sheyiyuan.cn:3000/yongchristians sheyiyuan.cn
https://gogs.kakaranet.com/hheabigail4100 gogs.kakaranet.com
http://dev.icrosswalk.ru:46300/kandiceklu6289 dev.icrosswalk.ru
https://git.unitsoft.io/barrycummins9 git.unitsoft.io
https://git.wun.im/edgardothiel0 git.wun.im
https://g.6tm.es/robbyn2807708 g.6tm.es
http://hoenking.cn:3000/wilhelminabutl hoenking.cn
References:
https://www.arabianmatrimony.com/@claudioshackel
mcforces.ru · October 13, 2025 at 4:37 pm
winstrol dianabol cycle
https://pin-it.site/item/404229 testosterone trenbolone dianabol cycle
https://bookmarkingworld.review/story.php?title=dianabol-cycle-for-perfect-results-the-preferred-steroid-of-titans deca dianabol cycle
https://duus-vestergaard-2.blogbright.net/full-anavar-cycle-guide-dosage-and-safety-suggestions valley.md
https://www.udrpsearch.com/user/walletcross9 dianabol And deca cycle
https://www.24propertyinspain.com/user/profile/1152363 testosterone and dianabol cycle
https://king-wifi.win/wiki/Dianabol_Dbol_Cycle_Greatest_Options_For_Newbies_And_Superior_Users valley.md
https://www.bitsdujour.com/profiles/y97jbV sustanon dianabol cycle
https://heavenarticle.com/author/hubgrain6-292939/ Testosterone And dianabol cycle
https://chessdatabase.science/wiki/Dianabol_Dbol_Cycle_Greatest_Options_For_Beginners_And_Advanced_Users valley.md
http://hikvisiondb.webcam/index.php?title=phamtillman6836 sustanon deca dianabol cycle
https://fakenews.win/wiki/Anadrol_Oxymetholone_An_Overview dianabol cycle dosage
https://bookmarking.stream/story.php?title=post-cycle-therapy-pct-an-summary Valley.md
https://fyhn-degn-4.blogbright.net/dianabol-cycle-for-good-outcomes-the-popular-steroid-of-titans dianabol post cycle therapy
https://classifieds.ocala-news.com/author/advicejar9 best Dianabol Cycle
https://xn—6-jlc6c.xn--p1ai/user/riskhelium0/ dianabol Only cycle reddit
https://f1news.space/item/402873 dianabol Cycle Results
https://www.instapaper.com/p/16730143 Valley.Md
https://brandmoshaver.com/user/metalcobweb7/ dianabol sustanon cycle
References:
beginner dianabol cycle, http://mcforces.ru/user/spearbead5/,
git.rbsx.de · October 13, 2025 at 5:12 pm
dianabol cycle for beginners
https://git.van-peeren.de/emmettlehunte1 https://git.van-peeren.de/emmettlehunte1
https://selfloveaffirmations.net/@calebaml265642 https://selfloveaffirmations.net/@calebaml265642
http://share.pkbigdata.com/valentinadosti http://share.pkbigdata.com/
https://git.sleepingforest.co.uk/roccocouch6909 https://git.sleepingforest.co.uk/roccocouch6909
https://www.besolife.com/@aldaromano0680 https://www.besolife.com/@aldaromano0680
http://dating.instaawork.com/@veldaflanders dating.instaawork.com
https://www.arabianmatrimony.com/@aleidalemberg4 http://www.arabianmatrimony.com
https://music.growverse.net/susanselby233 music.growverse.net
https://clone-deepsound.paineldemonstrativo.com.br/emiliegerace32 clone-deepsound.paineldemonstrativo.com.br
http://git.dgtis.com/mabelqzr606925 git.dgtis.com
https://ngoma.app/lottiebunning https://ngoma.app/lottiebunning
https://git.sayndone.ru/gailhumphries8 https://git.sayndone.ru/
https://git.noxxxx.com/millardroxon8 https://git.noxxxx.com/millardroxon8
https://asixmusik.com/tonjagriver25 asixmusik.com
https://koseongnam.com/qvsleora597135 koseongnam.com
https://kition.mhl.tuc.gr/billkimbrell5 kition.mhl.tuc.gr
http://tools.refinecolor.com/kittyheard1328 http://tools.refinecolor.com/kittyheard1328
http://bot.61ns.com:3000/carinzbs64120 bot.61ns.com
References:
https://git.rbsx.de/denisetrommler
https://www.instapaper.com/p/16730344 · October 13, 2025 at 5:21 pm
4 week dianabol cycle
https://muhammad-ali.com.az/user/trainflare1/ dianabol cycle reddit
https://linkvault.win/story.php?title=dianabol-cycle-muscle-positive-aspects-integrating-dianabol-into-your-bodybuilding-cycle valley.md
https://newssignet.top/item/406066 Valley.md
https://sciencebookmark.top/item/296345 Anavar and dianabol cycle
https://pattern-wiki.win/wiki/Dianabol_Unwanted_Facet_Effects_Results_After_Submit_Cycle_Remedy_Pct dianabol side effects after one cycle
http://09vodostok.ru/user/rockettoast9/ tren dianabol Test Cycle
https://nerdgaming.science/wiki/Dianabol_Cycle_For_Perfect_Outcomes_The_Preferred_Steroid_Of_Titans dianabol and testosterone cycle for beginners
https://topspots.cloud/item/403007 Beginner Dianabol Cycle
https://topspots.cloud/item/403007 dianabol post cycle
https://monjournal.xyz/item/298306 Dianabol Anavar Cycle
https://noticias-sociales.space/item/404679 dianabol 50mg cycle
https://dencker-allen-2.blogbright.net/what-to-stack-with-testosterone-cypionate testosterone and dianabol cycle
https://heavenarticle.com/author/firedpencil56-293105/ dianabol side effects after one cycle
https://rentry.co/8a3gi3kh test deca dianabol cycle
https://pediascape.science/wiki/Arnold_Schwarzeneggers_Steroid_Cycle_Dbol_And_Primobolan Valley.Md
https://monjournal.space/item/405056 how to take dianabol first cycle
https://xn—-7sbarohhk4a0dxb3c.xn--p1ai/user/woundpoland8/ deca dianabol Test Cycle
https://enoticias.site/item/295882 injectable dianabol cycle
References:
dianabol And deca Cycle [https://www.instapaper.com/p/16730344]
buchmacher deutschland Spanien · October 13, 2025 at 11:43 pm
beste online wetten anbieter
Feel free to visit my blog buchmacher deutschland Spanien
https://www.google.com.ai/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects · October 14, 2025 at 6:27 am
steroid dianabol cycle
https://www.udrpsearch.com/user/sprouthall4 http://www.udrpsearch.com
https://bookmarkzones.trade/story.php?title=kpv-peptides-rapid-muscle-skin-gut-recovery-boost https://bookmarkzones.trade
https://www.24propertyinspain.com/user/profile/1237113 https://www.24propertyinspain.com
https://www.google.co.ao/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects http://www.google.co.ao
https://maps.google.nr/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects https://maps.google.nr/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects
https://autovin-info.com/user/touchbotany7/ autovin-info.com
https://rentry.co/75z2ybqg https://rentry.co/75z2ybqg
https://silkrecord27.bravejournal.net/kpv-peptide-unveiling-its-role-in-accelerating-wound-healing silkrecord27.bravejournal.net
https://images.google.be/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects images.google.be
https://images.google.cf/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects https://images.google.cf/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects
https://www.google.co.ao/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects https://www.google.co.ao/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects
https://www.bitsdujour.com/profiles/ogFK0i https://www.bitsdujour.com/
https://gibbs-savage-3.technetbloggers.de/ultra-pure-research-peptides-precision-and-reliability-in-scientific-applications gibbs-savage-3.technetbloggers.de
http://king-wifi.win//index.php?title=haugaardbaun8875 http://king-wifi.win
https://peatix.com/user/27974406 https://peatix.com/
https://www.google.pl/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects https://www.google.pl/
https://escatter11.fullerton.edu/nfs/show_user.php?userid=9311880 escatter11.fullerton.edu
https://www.bitsdujour.com/profiles/ogFK0i http://www.bitsdujour.com
References:
https://www.google.com.ai/url?q=https://www.valley.md/kpv-peptide-guide-to-benefits-dosage-side-effects
https://gitea.jasonstolle.com · October 14, 2025 at 7:47 am
dianabol winstrol cycle
https://dev.dhf.icu/hortensepollak/www.soundofrecovery.org7922/wiki/The-Heart-Of-The-Internet https://dev.dhf.icu/
https://git.yi-guanjia.com/agnesnct74970 https://git.yi-guanjia.com/
https://git.getmind.cn/nicolasstallwo git.getmind.cn
http://gitea.aibaytek.com/calvinsmythe76 gitea.aibaytek.com
https://gitlab.presov.sk/clemmiecrabtre gitlab.presov.sk
https://git.wisptales.org/lavernelampman https://git.wisptales.org/lavernelampman
https://www.cyberpinoy.net/read-blog/284779_oral-vs-injectable-steroids-how-long-do-steroids-stay-in-your-system.html https://www.cyberpinoy.net/read-blog/284779_oral-vs-injectable-steroids-how-long-do-steroids-stay-in-your-system.html
https://liv07.com.np/@priscillay0879?page=about liv07.com.np
https://git.el-paco.com/melvaseppelt17 https://git.el-paco.com
https://agoo.focused-solution.com/read-blog/204_dianabol-turinabol-cycle-plan-pdf.html agoo.focused-solution.com
http://smandamlg.com/vibe/@luigivenegas09?page=about http://smandamlg.com/vibe/@luigivenegas09?page=about
https://git.parat.swiss/nanniecolston5 https://git.parat.swiss
http://jinjianghc.com:3000/curtstackhouse http://jinjianghc.com:3000/curtstackhouse
http://apps.iwmbd.com/elliottiliffe9 http://apps.iwmbd.com/elliottiliffe9
https://nucleation.fusion.bref.cool/deneengillis9 nucleation.fusion.bref.cool
https://theudtaullu.com/@luellamoney075?page=about https://theudtaullu.com/@luellamoney075?page=about
https://simapodcast.co.ls/@laraekuester1?page=about simapodcast.co.ls
https://git.raveau.info/margretlipscom https://git.raveau.info/
References:
https://gitea.jasonstolle.com/brandonz607063
git.mikspec.pl · October 14, 2025 at 8:14 am
dianabol only cycle reddit
https://git.mdp.edu.ar/nicholsteinfel/3005weshareinterest.com/wiki/Dianabol-Dosage https://git.mdp.edu.ar/
https://otgchat.com/read-blog/4655_poster-keerthana-deepti-karunakaran-biomedical-engineering-and-imaging-institute.html otgchat.com
https://git.sumedangkab.go.id/johnskillen040 git.sumedangkab.go.id
https://homenetwork.tv/@laynemathew33?page=about https://homenetwork.tv/@laynemathew33?page=about
http://git.in.ahbd.net/ute8511138755 http://git.in.ahbd.net/ute8511138755
http://nas.hiant.cfd:3000/janinaocasio49 nas.hiant.cfd
https://www.xtrareal.tv/@luciennepettis?page=about https://www.xtrareal.tv/
https://artbeninshow.afiganmey.com/amoswieck9296 artbeninshow.afiganmey.com
https://repo.komhumana.org/mathiasruth767 repo.komhumana.org
https://git.ewft.org/venettaburston/venetta2018/wiki/Top+10+Anadrol+Cycles+For+Bulking+And+Cutting git.ewft.org
https://crazyworksports.com/@frieda72825055?page=about crazyworksports.com
https://code.dsconce.space/katherinewalke code.dsconce.space
https://mybeautytube.tv/@elievergood308?page=about https://mybeautytube.tv/
https://git.getmind.cn/ameliebacon795 git.getmind.cn
https://digitalafterlife.org/@mirtajoy827490?page=about digitalafterlife.org
https://gitea.marvinronk.com/lavinabelisari https://gitea.marvinronk.com
https://git.izen.live/augustinag966 https://git.izen.live/augustinag966
https://meetme.goo.ng/@marylynbrack8 meetme.goo.ng
References:
https://git.mikspec.pl/olapicot871485/7841sound.floofbite.com/wiki/Anabolic+Steroids%3A+Uses%2C+Side+Effects%2C+And+Alternatives
git.autotion.net · October 14, 2025 at 8:57 am
injectable dianabol cycle
https://blackvision.co.uk/@leonardocharte?page=about https://blackvision.co.uk/
https://godscoop.com/read-blog/33239_best-pct-supplements-for-different-steroid-cycles-anavar-dianabol-t.html godscoop.com
https://gosvid.com/@rosalindabowen?page=about gosvid.com
https://gitea.chaos-it.pl/sheldondreher https://gitea.chaos-it.pl
https://viraltry.com/@gregoriohackba?page=about viraltry.com
https://gitlab.cranecloud.io/annhooper6888/5139git.healthathome.com.np/-/issues/1 gitlab.cranecloud.io
https://my70size.com/@valorielytle65?page=about my70size.com
https://gogs.mneme.dedyn.io/laurenceoliva https://gogs.mneme.dedyn.io
https://git.7vbc.com/emerygilbertso git.7vbc.com
https://git.deadpoo.net/esperanzaforlo git.deadpoo.net
https://bantoomusic.com/waltercade455 bantoomusic.com
https://www.lab.justusdeitert.de/leonelwurfel6/3928git.dpark.io/-/issues/1 http://www.lab.justusdeitert.de
https://git.pleroma.social/irwinisles2642 git.pleroma.social
http://git.biscicloud.com/imogeneclibbor git.biscicloud.com
https://mybeautytube.tv/@elievergood308?page=about https://mybeautytube.tv/@elievergood308?page=about
http://git.vfoxs.com/jacoboaa996040/syq.im3115/wiki/Anabolic-Steroids%3A-Uses%2C-Abuse%2C-And-Side-Effects git.vfoxs.com
https://cineraworld.com/@utecoleman0198?page=about cineraworld.com
https://git.rec4box.com/austindieter72 git.rec4box.com
References:
https://git.autotion.net/kaleygillam400
onlyaimovies.com · October 14, 2025 at 11:30 am
dianabol winstrol cycle
http://git.guaiyun.com.cn/valeriedibble2 git.guaiyun.com.cn
https://camtalking.com/@laifawn504189 https://camtalking.com/@laifawn504189
https://play.ayooka.com/@pamela83918575?page=about play.ayooka.com
https://kayesbamusic.com/michelchambers kayesbamusic.com
https://myclassictv.com/@gzgmelvin42712?page=about https://myclassictv.com/
https://repo.divisilabs.com/kristianmelanc https://repo.divisilabs.com/kristianmelanc
https://gitea.irons.nz/verlaherrick0 https://gitea.irons.nz/verlaherrick0
https://lensez.info/barneystang513 lensez.info
https://git.unglab.com/agustincastell git.unglab.com
http://www.feiko.cn:3300/adelekneebone6 http://www.feiko.cn
https://great-worker.com/ajahuondekerma https://great-worker.com/ajahuondekerma
https://git.ghostpacket.org/gailkashiwagi6 https://git.ghostpacket.org/gailkashiwagi6
https://1coner.com/@kiadch8917356 1coner.com
https://meetdatingpartners.com/@scotironside73 meetdatingpartners.com
https://pleroma.cnuc.nu/gavin863150039 pleroma.cnuc.nu
https://afritunes.net/skye36f7234689 https://afritunes.net/
https://unired.zz.com.ve/@noezcp0071588 https://unired.zz.com.ve/@noezcp0071588
https://sithcom.de/annisdavison81 sithcom.de
References:
https://onlyaimovies.com/@ismaelsorensen?page=about
beste sportwetten plattform · October 14, 2025 at 3:53 pm
asiatische wettanbieter
Review my blog :: beste sportwetten plattform
https://www.cadquos.dev/ · October 14, 2025 at 4:39 pm
dianabol post cycle therapy
http://git.veilytech.com/u/yzyferne916318 http://git.veilytech.com/
https://artbeninshow.afiganmey.com/stephanyfrome2 https://artbeninshow.afiganmey.com/
https://gogs.soyootech.com/marlysshapcott gogs.soyootech.com
https://git.jbangit.com/wilfredoltu39 git.jbangit.com
https://www.nxgit.xyz/mackenzieg079 https://www.nxgit.xyz
http://gitea.dctpay.com/hamishngo84147 http://gitea.dctpay.com/
http://git.veilytech.com/u/pearllouden25 http://git.veilytech.com/
https://gitea.kdlsvps.top/tzfines0670615 gitea.kdlsvps.top
https://blackbirdstory.com/@ubyesmeralda56?page=about https://blackbirdstory.com
https://git.konsulterna.nu/valliegallant https://git.konsulterna.nu/
http://gitea.yunshanghub.com:8081/lukas565736996 http://gitea.yunshanghub.com
https://www.herzog-it.de/auroramacbain3 https://www.herzog-it.de
https://git.jbangit.com/kristofereichm git.jbangit.com
https://meetdatingpartners.com/@venusflores14 https://meetdatingpartners.com/
https://git.hanckh.top/mariloubennett git.hanckh.top
https://play.future.al/@penneydempster?page=about https://play.future.al/@penneydempster?page=about
https://nvuplayer.com/@wilsonsteadham?page=about https://nvuplayer.com
https://home.zhupei.me:3000/joycemccrae802 home.zhupei.me
References:
https://www.cadquos.dev/ralphcoward380
https://www.meetgr.com/@jenniegoin5337 · October 14, 2025 at 4:39 pm
dianabol cycle length
https://nvuplayer.com/@ramonober02051?page=about nvuplayer.com
https://git.saidomar.fr/janeenwarner1 git.saidomar.fr
https://financevideosmedia.com/@jacqueschomley?page=about financevideosmedia.com
http://git.vfoxs.com/rosellaanthony git.vfoxs.com
https://git.ajattix.org/mayconolly405 https://git.ajattix.org
https://kition.mhl.tuc.gr/mariannejoy32 kition.mhl.tuc.gr
https://gitea.dcqrr.top:83/haleyhernandez gitea.dcqrr.top
https://gitimpo.liara.run/rickelkin1767 gitimpo.liara.run
https://git.yuhong.com.cn/rosellafisk790 git.yuhong.com.cn
http://gitea.dctpay.com/domenicjni8933 gitea.dctpay.com
https://git.rpjosh.de/marcobrass196 git.rpjosh.de
https://git.srblerp.com/dalerichter48 git.srblerp.com
https://git.winscloud.net/lyndavalente23 git.winscloud.net
https://gitea.thanh0x.com/cheril02421941 https://gitea.thanh0x.com/cheril02421941
https://hafrikplay.com/kashastrayer29 hafrikplay.com
https://pleroma.cnuc.nu/agnesshuler709 pleroma.cnuc.nu
https://git.furcom.org/olen2800532719 git.furcom.org
https://myhealthypunjab.com/@eviewhitham558?page=about myhealthypunjab.com
References:
https://www.meetgr.com/@jenniegoin5337
beste sportwetten tipps app · October 14, 2025 at 4:59 pm
mehrfach kombiwette rechner
Visit my webpage :: beste sportwetten tipps app
wettstrategien sportwetten · October 14, 2025 at 5:08 pm
wettstrategien sportwetten bonus code
Bailey · October 14, 2025 at 6:18 pm
eurovision wetten deutschland
Here is my website – sportwetten geld zurück österreich [Bailey]
gitea.dctpay.com · October 14, 2025 at 8:45 pm
how long is a dianabol cycle
https://gitea.vidoks.fr/veronicaruiz94 https://gitea.vidoks.fr/veronicaruiz94
https://home.zhupei.me:3000/johnathanmulli https://home.zhupei.me
https://gitea.codedbycaleb.com/ellavannoy9206 gitea.codedbycaleb.com
https://www.aservicehost.ru/partheniadicks http://www.aservicehost.ru
https://tippy-t.com/edenisaachsen tippy-t.com
https://gitea.alaindee.net/alejandravolz gitea.alaindee.net
https://qimley.com/@randicarnarvon https://qimley.com/@randicarnarvon
http://test-www.writebug.com:3000/tgnnewton20252 http://test-www.writebug.com/
https://play.ayooka.com/@francescobrier?page=about play.ayooka.com
https://viewcast.altervista.org/@chandrahyland3?page=about viewcast.altervista.org
https://nuhweh.com/joeostrander13 nuhweh.com
https://gitea.johannes-hegele.de/miriamgrimston https://gitea.johannes-hegele.de/miriamgrimston
https://nildigitalco.com/@jeffersonbrodn?page=about nildigitalco.com
https://9jadates.com/@malissahilderb https://9jadates.com
https://fyahtrak.com/buddy018936562 fyahtrak.com
https://aitnas.myasustor.com/wilbertaldridg https://aitnas.myasustor.com/wilbertaldridg
https://isabelzarate.com/starlagatehous isabelzarate.com
https://gitea.micro-stack.org/senaidabarnes3 https://gitea.micro-stack.org/senaidabarnes3
References:
http://gitea.dctpay.com/hilda30w885262
https://gitea.irons.nz · October 14, 2025 at 9:29 pm
sustanon deca dianabol cycle
https://git.mklpiening.de/arturoannand68 https://git.mklpiening.de/arturoannand68
https://git.gaminganimal.org/caitlynmerrick https://git.gaminganimal.org
https://git.lakaweb.com/angeliakiser67 git.lakaweb.com
https://sound.floofbite.com/floramarcantel sound.floofbite.com
https://www.appleradish.org/benjamingonzal https://www.appleradish.org/
https://digitalafterlife.org/@yyuaddie777928?page=about https://digitalafterlife.org/@yyuaddie777928?page=about
https://homeview.emmcoc.com.ng/@elishabastyan?page=about homeview.emmcoc.com.ng
http://oa.sccehui.com:6101/lavonfindley33 http://oa.sccehui.com
https://git.mklpiening.de/arturoannand68 https://git.mklpiening.de/arturoannand68
http://gitea.ucarmesin.de/lonadibble9948 gitea.ucarmesin.de
https://www.broutube.com/@dominickswett4?page=about broutube.com
http://dgzyt.xyz:3000/emiliacreed39 dgzyt.xyz
https://gitea.mpc-web.jp/veolarudduck3 gitea.mpc-web.jp
https://git.rbsx.de/gastonbonnor3 https://git.rbsx.de/
https://snaytube.com/@cleos006081866?page=about snaytube.com
https://gitea.nongnghiepso.com/velmawaldock74 https://gitea.nongnghiepso.com/velmawaldock74
http://zahbox.com/@randolphqva613?page=about http://zahbox.com/@randolphqva613?page=about
http://gitea.liaozhuangkeji.com/lilykillinger gitea.liaozhuangkeji.com
References:
https://gitea.irons.nz/kxcrodrick8551
Wettbüro nähe · October 15, 2025 at 10:46 am
buchmacher test
Here is my web page … Wettbüro nähe
Where can you buy Anabolic Steroids · October 15, 2025 at 11:39 am
where to buy illegal steroids
https://www.hulkshare.com/shameshovel0/ pros and cons of anabolic steroids
https://gratisafhalen.be/author/cherrydragon23/ anavar muscle Gains
https://to-portal.com/curveleek37 anabolic steroid sales
https://apunto.it/user/profile/244533 Deca Durabolin Price
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=windowquilt3 will steroids burn fat
https://able2know.org/user/boatkettle4/ steroids to build muscle
https://urlscan.io/result/0199a483-59a5-71d9-8da0-5939ab5e9ce3/ steroids pills for bodybuilding
https://forum.issabel.org/u/veilquilt94 Is Creatine An Anabolic Steroid
https://pads.jeito.nl/_9zD6hJ9Q0qNTvInCr0sCw/ roids.Com
https://www.askocloud.com/index.php/user/condordouble72 dmaa effects
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=tenormotion89 Types Of Testosterone Steroids
https://md.un-hack-bar.de/f4BTsjmbQt-7q3F-bEhdCA/ where can you buy steroids
https://writeablog.net/brownnews96/anavar-cycle-outcomes-can-you-maintain-gains-once-its-over valley
http://www.kaizenoffice.com/forums/users/lacesyrup36/ Valley
https://www.tikosatis.com/index.php?page=user&action=pub_profile&id=369769 Steroid Cycle Transformation
http://community.srhtech.net/user/tenorvoyage48 how big can you get without steroids
https://independent.academia.edu/ReyesOrtiz15 Common bodybuilding steroids
https://www.instapaper.com/p/17021572 what does anabolic steroids do
References:
https://www.generation-n.at/forums/users/lawcar7/
steroidsone · October 15, 2025 at 11:44 am
best steroids to get ripped
https://cuwip.ucsd.edu/members/printclass22/activity/2029327/ Anabolic Steroids Withdrawal
http://www.annunciogratis.net/author/corkvision6 danger of steroid use
https://hack.allmende.io/bCqgTM_7TNeGRgYpqzzjUA/ valley
https://torrentmiz.ru/user/pipeoil82/ best testosterone injection for bodybuilding
https://lejournaldedubai.com/user/hallquilt97/ steroid users Lifting routines
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=taiwanflight33 Best Cutting Cycle Bodybuilding
https://pad.stuve.uni-ulm.de/tPmVerjRSFqpKPQT0UyFDw/ synthetic corticosteroid
https://hedge.fachschaft.informatik.uni-kl.de/jYir7S_fSFuIlWb19ZrWlw/ legal steroids stacks
https://fancypad.techinc.nl/On3fp7pLQD2VnW5_JjY3JQ/ creatine steroid
https://avtovoprosi.ru/user/markkorean93 reddit steriods
https://output.jsbin.com/nufejeqisa/ what is t* steroid
https://bleezlabs.com/demo/quora/savak/index.php?qa=user&qa_1=reporttrick74 the best steroids on the market
https://doc.aquilenet.fr/mUDSzoJSRG2bmhTUSANxtA/ valley
https://mycoalitionu.org/forums/users/hempmosque6/edit valley
https://codimd.fiksel.info/wyjZ8ReVR8KinU5pn9sZ-A/ Valley
https://autovin-info.com/user/desertwave56/ winsdrol v reviews
https://ebra.ewaucu.us/index.php?page=user&action=pub_profile&id=93288 testosterone vs anabolic steroids
https://support.mikrodev.com/index.php?qa=user&qa_1=lyricsanta7 legal steroids supplements
References:
http://www.annunciogratis.net/author/corkvision6
sportwetten deutsch · October 15, 2025 at 9:08 pm
wett tipps von profis heute
Here is my website; sportwetten deutsch
Online Wetten Politik · October 15, 2025 at 9:34 pm
wettquoten vergleich
Look at my web page – Online Wetten Politik
wetten online paypal · October 15, 2025 at 10:16 pm
besten sportwetten tipps
Check out my site :: wetten online paypal
https://repo.komhumana.org/austingruenewa · October 15, 2025 at 11:08 pm
dianabol winstrol cycle
https://gogolive.biz/@lannymcclary3?page=about gogolive.biz
https://mixtify.top/toniatweddle6 mixtify.top
https://cameotv.cc/@ernestinamacla?page=about cameotv.cc
https://repo.apps.odatahub.net/aurelianewkirk repo.apps.odatahub.net
https://tageeapp.com/@adolfotafoya94?page=about tageeapp.com
https://git.51aspx.com/carlotadunkley https://git.51aspx.com
https://pilowtalks.com/@mayrooks888483 https://pilowtalks.com/@mayrooks888483
https://git.inscloudtech.com/claytontoosey https://git.inscloudtech.com
http://git.youkehulian.cn/kourtneysommer git.youkehulian.cn
https://git.rbsx.de/shantellcoz979 git.rbsx.de
https://git.lolpro11.me/kristinhillen4 git.lolpro11.me
https://familyworld.io/@genacraft4513?page=about https://familyworld.io/@genacraft4513?page=about
https://thefusionflix.com/@nestorscherer?page=about thefusionflix.com
https://ngoma.app/hoseahatch6906 https://ngoma.app/hoseahatch6906
https://git.lunax.dev/santotheis1979 git.lunax.dev
https://gogs.kakaranet.com/salvatorebuckn https://gogs.kakaranet.com
http://dgzyt.xyz:3000/dexterbedard9 dgzyt.xyz
https://sound.gatzone.com/virginiaingrah https://sound.gatzone.com
References:
https://repo.komhumana.org/austingruenewa
deltasongs.com · October 15, 2025 at 11:41 pm
dianabol cycle side effects
https://yours-tube.com/@celiavarley006?page=about https://yours-tube.com/@celiavarley006?page=about
https://music.shaap.tg/clydemonson279 music.shaap.tg
https://great-worker.com/darellkovach51 https://great-worker.com/darellkovach51
https://islamyaat.com/@craiggrinder7?page=about islamyaat.com
https://git.zhukovsky.me/ericoster84971 https://git.zhukovsky.me
https://git.yinas.cn/eleanore46o71 git.yinas.cn
http://git.pushecommerce.com/leonidahagenau git.pushecommerce.com
https://demo.indeksyazilim.com/barryfarris07 https://demo.indeksyazilim.com
https://ophiuchus.wiki/simonepogue93 ophiuchus.wiki
https://mixtify.top/brendanomar764 mixtify.top
http://tools.refinecolor.com/lawannaosby428 http://tools.refinecolor.com/lawannaosby428
https://git.agusandelnorte.gov.ph/vanitagain0093 git.agusandelnorte.gov.ph
https://quickdate.click/@rosalinezfj63 https://quickdate.click/@rosalinezfj63
https://hiphopmusique.com/venusbeauvais https://hiphopmusique.com/
https://giteap.grobest.com:3000/jurgenboland31 https://giteap.grobest.com/
https://www.cadquos.dev/tpyvicky41453 https://www.cadquos.dev
https://git.poly.zone/claywintle667 git.poly.zone
https://pokesoul.com/@jack0630230797 pokesoul.com
References:
https://deltasongs.com/vincebobb5944
binance Sign Up · October 16, 2025 at 6:32 am
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
wettformat gratiswette · October 16, 2025 at 4:07 pm
beste wettanbieter bonus
Also visit my homepage – wettformat gratiswette
Https://Rejuvenateresponsibly.Com · October 17, 2025 at 4:01 pm
Sportwetten Tipps FüR AnfäNger (https://Rejuvenateresponsibly.Com) interwetten
https://phoebe.roshka.com/ · October 17, 2025 at 8:51 pm
Compare trusted providers, pricing, safety requirements, and availability to find affordable, dependable choices for weight loss assist. Book a peptide consultation at present to find the best protocol on your body and goals. In this information, we’ll break down how sermorelin and ipamorelin work, what sets them aside, and the way to choose the right one based in your objectives. We provide hormone optimization for women and men to address fatigue, mood adjustments, weight acquire, and other signs of hormonal imbalance. Our bioidentical hormone substitute applications are personalised to restore optimal ranges and support total vitality.
Most users notice improvements in sleep, recovery, and day by day vitality within about four weeks. If you’ve spent any time in the wellness space, you’ve doubtless heard the buzz about peptides. These small chains of amino acids act as cellular messengers, signaling your body to repair, restore, and regenerate from the within out. The use of Ipamorelin and Sermorelin in anti-aging therapy presents promising advantages in addressing age-related considerations and promoting overall wellness by way of targeted peptide therapies.
It is crucial to take care of a balanced food plan and common train routine to manage this side impact successfully. Out of all of the hgh secretagogues listed, as properly as MK677, CJC, etc. which is the best? Each peptides are considered protected when used accurately, however like any supplement, they can have unwanted effects. To make the most effective choice about which peptide is the most effective candidate for additional analysis, researchers ought to undertake a cautious strategy and contemplate long-term follow-up for analysis subjects. The second distinction is that ipamorelin reduces somatostatin, a hormone that inhibits GH.
Many folks want to improve their body’s pure manufacturing of human progress hormone (HGH) levels for overall health, vitality plus muscle progress. Different elements affect the production of HGH peptides such as age sleep high quality, underlying well being circumstances, exercise as properly as diet. The natural HGH manufacturing drops as we age however regular intense bodily performance- especially high-intensity interval coaching (HIIT) – really helps to raise the degrees. Deep sleep is very important because the physique releases HGH throughout rest durations.
Injecting too much Sermorelin can result in side effects such as headaches, nausea, or injection website irritation. Excessive dosing may disrupt natural hormone stability and trigger unwanted symptoms, so adherence to prescribed amounts is necessary. They also improve hormone steadiness, lowering dangers of well being situations and enhancing well-being. Sermorelin and ipamorelin are comparable in that they each appear to stimulate the body to produce more progress hormone. A 2002 study published in the European Journal of Anatomy found that ipamorelin treatment might stimulate physique weight acquire and GH release in young feminine rats [12].
Next, using a thin needle (commonly gauge), pinch the pores and skin between two fingers to create a small mound for injection. When administering these peptides subcutaneously, it’s essential to make sure correct technique to maximize their effectiveness.
This distinction in longevity of effects is crucial for people seeking sustained improvements in pores and skin well being and wound restoration. Obesity and insulin resistance blunt each basal GH secretion and secretagogue responses. Individuals with larger visceral fats or impaired glucose tolerance sometimes see smaller will increase in GH/IGF-1 from the identical dose. Enhancing insulin sensitivity (dietary sample, weight loss, bodily activity) usually improves responsiveness more than rising dose. In controlled research, ipamorelin produced GH peaks inside roughly an hour of dosing, then levels declined quickly as the drug cleared. The half-life is short (around two hours in human PK models), which is why researchers typically dose as quickly as day by day to a quantity of occasions per day when studying repeated pulses. Additionally, Ipamorelin stands out for its selectivity in stimulating progress hormone launch with out affecting cortisol or prolactin ranges significantly.
They are used in various therapeutic contexts, including the remedy of progress hormone deficiencies and certain metabolic situations. Sermorelin and Ipamorelin are two distinguished peptides utilized in hormone remedy to stimulate the pituitary glands, thereby enhancing hormone secretion. Although each peptides are intended to mimic the body’s pure growth hormone-releasing processes, they accomplish that via distinct mechanisms. Factors to assume about embrace remedy targets (anti-aging vs. muscle gain), aspect impact tolerance, injection frequency, and individual health status. Ipamorelin could also be better for focused fats loss and muscle recovery, while Sermorelin is best for consistent hormone assist and aging-related signs. The hormone-boosting compounds within HGH peptides activate each the hypothalamus and pituitary gland to enhance natural development hormone output by the physique. Peptides like sermorelin and Ipamorelin stimulate the physique to produce and release HGH which helps deal with progress hormone deficiencies yet additionally leads to anti-aging advantages.
In the following part, we’ll discuss what ipamorelin is and the type of advantages it offers when administered to check topics. Sermorelin’s FDA approval was discontinued in 2008 and it thereby misplaced its status as being permitted for any medical use [3]. Nevertheless, before being discontinued, sermorelin did have a number of medically recognized advantages. Sermorelin was initially permitted by the FDA in 1997 and bought underneath the commerce name “Geref” [2]. However while these two peptides can have similar results, they work in slightly different ways.
Customers often report elevated energy, improved sleep quality, and enhanced restoration when using Ipamorelin and Sermorelin. Some might experience mild unwanted effects like injection website discomfort or complications initially. Total, these peptides promote a sense of well-being by restoring natural progress hormone ranges. Sure, stacking Sermorelin and Ipamorelin is a common follow in peptide remedy to maximize progress hormone launch and its advantages. Combining these peptides can improve muscle growth, fat loss, and total vitality by leveraging their complementary mechanisms. Medical supervision is important to make sure secure and effective dosing when using each peptides together.
https://git.clarue.net/margieleachman sermorelin vs ipamorelin and tesamorelin
https://www.superphage.org/rileyj75729635/3728686/wiki/Is-Pepper-Spray-Legal-In-Europe%3F-Country-by-country-Guide sermorelin ipamorelin treatment delivery
https://qimley.com/@jeniferhammel sermorelin ipamorelin blend dose
https://lius.familyds.org:3000/albertawootten ipamorelin vs sermorelin
https://www.superphage.org/rileyj75729635/3728686/wiki/Is-Pepper-Spray-Legal-In-Europe%3F-Country-by-country-Guide https://www.superphage.org
References:
https://git.asdf.cafe/ltdrudolf7255 git.asdf.cafe
https://git.cnml.de/aguedarandolph cjc 1295 ipamorelin and sermorelin
https://gitea.boner.be/charitycawthor what is better sermorelin or ipamorelin
https://jioxe.com/read-blog/19720_can-you-mix-sermorelin-and-ipamorelin-analysis-insights-defined.html sermorelin/ipamorelin before and after
http://shvber.com:5189/carmineetq6070 sermorelin ipamorelin blend peptide for men
https://git.ghostpacket.org/selinasaragosa sermorelin-ipamorelin-cjc1295 stack
https://asfuyao.top:8300/angelinewoolco cjc 1295 ipamorelin vs sermorelin
https://g.ovlg.com/winifredbrooki https://g.ovlg.com/
https://gitea.codedbycaleb.com/connoravelar18 ipamorelin sermorelin
http://gitea.yunshanghub.com:8081/ygngertie74040 sermorelin vs ipamorelin comparison
https://w2k.sh/xahkarri542198 tesamorelin vs ipamorelin vs sermorelin
http://szfinest.com:6060/pablov46842045 sermorelin + ipamorelin
https://git.xemo-net.de/edwinrte184526 cjc 1295 ipamorelin vs sermorelin
References:
https://phoebe.roshka.com/gitlab/sherrygirardi3
Online Live Wetten · October 18, 2025 at 7:00 am
Online Live Wetten
sportwetten tipps
sermorelin/ipamorelin benefits · October 18, 2025 at 7:32 am
sermorelin and ipamorelin stack
https://jobs.sharedservicesforum.in/employers/sermorelin-vs-ipamorelin-choosing-the-right-growth-hormone-peptide/ valley.md
https://syurl.com/chana357978238 sermorelin + ipamorelin blend
https://prel.ink/julissa63x2558 valley.md
https://carrieresecurite.fr/entreprises/real-world-evidence-of-multiple-myeloma-treatment-2013-2019-in-the-hospital-district-of-helsinki-and-uusimaa-finland/ valley.md
https://jobzee.co.uk/Company/us-made-peptides-showcasing-their-advantages-sermorelin-vs-ipamorelin-vs-tesamorelin/ which is stronger ipamorelin or sermorelin
https://fastlinks.com.tr/suelowrie3867 https://fastlinks.com.tr/suelowrie3867
https://bilzainvisa.com/employer/ipamorelin-vs-sermorelin-choosing-the-ideal-peptide-treatment/ ipamorelin and sermorelin injection time
https://getshired.com/employer/ipamorelin-vs-sermorelin-key-distinctions-and-advantages/ ipamorelin cjc 1295 and sermorelin
https://url9xx.com/christelcrumle difference between ipamorelin and sermorelin
https://elclasificadomx.com/author/jasminevji1/ https://elclasificadomx.com
https://www.mazafakas.com/user/profile/7576957 mazafakas.com
https://tinijob.com/companies/synergistic-treatment-combining-sermorelin-and-ipamorelin/ sermorelin ipamorelin anti aging treatment
https://handitalents.com/employer/sermorelin-vs-cjc-1295-ipamorelin-choosing-the-right-growth-hormone-peptide-for-you/ buy sermorelin ipamorelin cjc1295 combo
https://link.con3ct.com.br/vidashanno sermorelin ipamorelin vs mk677
https://ozzojobs.com/employer/183734/sermorelin-vs-cjc-1295-advantages-and-disadvantages valley.md
https://urlb.link/lashawnrodway1 sermorelin ipamorelin reddit
https://jobszimbabwe.co.zw/companies/peptide-stacking-separating-myth-from-reality/ sermorelin ipamorelin side effects
https://lazerjobs.in/employer/us-made-peptides-showcasing-their-advantages-sermorelin-vs-ipamorelin-vs-tesamorelin/ lazerjobs.in
References:
https://talentfolder.com/employer/ipamorelin-vs-sermorelin-what-bodybuilders-need-to-know-about-benefits-doses-and-popular-blends/
https://lings.id/ · October 18, 2025 at 7:48 am
aai rejuvenation clinic testosterone sermorelin hgh ipamorelin
https://vagas.grupooportunityrh.com.br/employer/ipamorelin-vs-sermorelin-an-in-depth-comparison-and-practical-guide/ valley.md
https://recrutement.fanavenue.com/companies/top-peptide-stack-picks-for-2025-the-definitive-guide/ valley.md
https://prel.ink/julissa63x2558 prel.ink
https://gotech.peep.company/shauntedeen999 sermorelin ipamorelin blend peptide for sale
https://i365.one/samuel86w37055 cjc 1295 ipamorelin sermorelin stack
https://jobfreez.com/employer/the-top-peptide-combinations-of-2025-a-definitive-guide/ sermorelin-ipamorelin-cjc 1295 for sale
https://getshired.com/employer/ipamorelin-vs-sermorelin-key-distinctions-and-advantages/ ipamorelin sermorelin cjc pt-141 tb-500
https://smartcard.phoenixopia.com/luze149484379 ipamorelin and sermorelin injection locations
https://emploiexpert.com/employer/ipamorelin-applications-and-advantages-how-it-works-recommended-doses-and-potential-adverse-effects/ sermorelin/ipamorelin blend dosage
https://linkqb.com/gmTjJ linkqb.com
https://thesecurityexchange.com/employer/ipamorelin-in-2025-advantages-recommended-doses-and-potential-hazards/ ipamorelin sermorelin acetate
https://smartbusinesscards.in/lucybrunner757 valley.md
https://jobe.pk/companies/ipamorelin-vs-sermorelin-deciding-the-superior-growth-hormone-peptide/ https://jobe.pk
https://parkerstewart.ie/employer/ipamorelin-vs.-sermorelin:-deciding-the-superior-growth-hormone-peptide/ sermorelin ipamorelin blend dose
https://dbitly.com/maryjohandt74 valley.md
https://www.garagesale.es/author/terranceher/ sermorelin ipamorelin and cjc1295
https://www.zgjzmq.com/home.php?mod=space&uid=143360&do=profile difference between sermorelin and ipamorelin
https://gjejstaf.al/employer/ipamorelin-vs-sermorelin-choosing-the-right-growth-hormone-peptide/ sermorelin ipamorelin blend dose
References:
https://lings.id/adrianapor
sermorelin ipamorelin blend dose · October 18, 2025 at 8:24 am
sermorelin ipamorelin and cjc 1295
https://www.mazafakas.com/user/profile/7576957 buy sermorelin and ipamorelin
https://gomyly.com/eduardolemieux valley.md
https://craftsmansearch.com/employer/sermorelin-dosing-101-finding-your-optimal-intake-for-peak-effectiveness/ valley.md
https://careers.tu-varna.bg/employer/ipamorelin-vs-sermorelin-deciding-which-growth-hormone-peptide-wins/ ipamorelin vs sermorelin reddit
https://oke.zone/profile.php?id=1054743 which is better ipamorelin or sermorelin
https://futureblazr.com/employer/real-world-evidence-of-multiple-myeloma-treatment-2013-2019-in-the-hospital-district-of-helsinki-and-uusimaa-finland/ sermorelin and ipamorelin dosage
https://china-jobs.de/employer/sermorelin-and-ipamorelin-a-comprehensive-look-at-the-peptide-duo/ valley.md
https://linkaloo.it/oWhIH valley.md
https://smartcard.phoenixopia.com/luze149484379 https://smartcard.phoenixopia.com/
https://link.con3ct.com.br/vidashanno sermorelin ipamorelin log
https://linkaloo.it/oWhIH doseage of sermorelin ipamorelin
https://interimjobmarket.com/employer/is-mixing-sermorelin-and-ipamorelin-safe/ valley.md
https://allsolution.xyz/employer/mixing-sermorelin-and-ipamorelin-is-it-safe/ sermorelin-ipamorelin-cjc1295 where to buy
https://jobsrific.com/employer/sermorelin-dosing-applications-and-comparative-review/ sermorelin vs ipamorelin
https://medicallystaffing.com/employer/ipamorelin-vs-sermorelin-choosing-the-ideal-peptide-treatment/ https://medicallystaffing.com/employer/ipamorelin-vs-sermorelin-choosing-the-ideal-peptide-treatment/
http://picscrazy.in/member.php?action=viewpro&member=Maximo16C sermorelin / ipamorelin / cjc1295
https://www.shikarpurhighschool.com/finlands-top-energy-firms-unite-to-build-an-industrial-hydrogen-hub/ ipamorelin and sermorelin suppliers
https://careeramaze.com/employer/ipamorelin-vs-sermorelin-choosing-the-right-growth-hormone-stimulator-for-your-goals/ sermorelin-ipamorelin-cjc 1295 for sale
References:
https://globejobsaid.com/employer/real-world-evidence-of-multiple-myeloma-treatment-2013-2019-in-the-hospital-district-of-helsinki-and-uusimaa-finland/
part-time.ie · October 18, 2025 at 9:04 am
sermorelin ipamorelin benefits
https://ethiofarmers.com/finlands-top-energy-firms-unite-to-build-an-industrial-hydrogen-hub/ ethiofarmers.com
https://euhope.com/employer/mastering-ipamorelin-cycles-ideal-doses-scheduling-and-top-peptide-combinations/ valley.md
https://www.shikarpurhighschool.com/finlands-top-energy-firms-unite-to-build-an-industrial-hydrogen-hub/ shikarpurhighschool.com
https://dokdo.in/rosalierandell sermorelin-ipamorelin-cjc1295 oral
https://irocket.careers/employer/sermorelin-vs-cjc-8-choosing-between-peptide-therapies-for-hgh-release-and-liv-1-benefits/ sermorelin ipamorelin treatment delivery
https://smarthr.com.hk/Companies/ipamorelin-applications-and-advantages-how-it-works-recommended-doses-and-potential-adverse-effects/ smarthr.com.hk
https://cleverklub.ru/chastityoflahe valley.md
https://vcardss.com/jessikamasters https://vcardss.com/jessikamasters
https://icmimarlikdergisi.com/kariyer/companies/sermorelin-vs-ipamorelin-choosing-the-right-growth-hormone-peptide-for-you/ https://icmimarlikdergisi.com
https://hirenhigher.co.nz/companies/gh-peptides-showdown-sermorelin-vs-ipamorelin-cjc-1295-tesamorelin-for-research-use/ ipamorelin vs tesamorelin vs sermorelin
https://www.recruit-vet.co.uk/employer/synergistic-peptide-pairing:-sermorelin-meets-ipamorelin-in-dual-therapy-regimens/ cjc-1295 and ipamorelin vs sermorelin
https://www.dynamicviewpoint.co.uk/employer/ipamorelin-vs-sermorelin-choosing-the-best-option-for-your-needs/ ipamorelin vs sermorelin fatloss
https://eliteyachtsclub.com/employer/ipamorelin-applications-advantages-pharmacodynamics-prescribed-doses-and-adverse-effects/ valley.md
https://url.pixelx.one/franciscoblack valley.md
https://mixclassified.com/user/profile/966689 mixclassified.com
https://www.pakalljobz.com/companies/ipamorelin-vs-sermorelin-a-detailed-side-by-side-review-and-practical-handbook/ ipamorelin vs sermorelin fatloss
https://fastlinks.com.tr/suelowrie3867 valley.md
https://hirenhigher.co.nz/companies/gh-peptides-showdown-sermorelin-vs-ipamorelin-cjc-1295-tesamorelin-for-research-use/ sermorelin w ipamorelin
References:
https://part-time.ie/companies/mastering-ipamorelin-cycles-ideal-doses-scheduling-and-top-peptide-combinations/
Belinda · October 18, 2025 at 1:23 pm
online wettanbieter schnelle auszahlung; Belinda, ohne
oasis
Cleo · October 18, 2025 at 2:02 pm
bestes beste wettbüro (Cleo)
Buchmacher Kreuzworträtsel · October 18, 2025 at 3:03 pm
wettbüro mannheim
my website; Buchmacher Kreuzworträtsel
Janice · October 18, 2025 at 4:04 pm
sportwetten strategie erfahrungen (Janice) freebet ohne einzahlung
Wie Funktioniert Eine Kombiwette · October 19, 2025 at 7:41 pm
online wetten deutschland
my website – Wie Funktioniert Eine Kombiwette
cute.link · October 19, 2025 at 9:50 pm
post cycle therapy for dianabol
https://whatchats.com/read-blog/3513_15-finest-steroids-earlier-than-and-after-footage.html whatchats.com
https://china-jobs.de/employer/anavar-before-and-after-muscle-gain-or-weight-loss/ china-jobs.de
https://suakhoacamlam.com/julianmlo71268 https://suakhoacamlam.com/julianmlo71268
https://music.growverse.net/raymondipg1951 music.growverse.net
https://gofleeks.com/read-blog/1431_39-anavar-cycle-results-that-dissolve-fat-boost-strength-and-harden-your-physiqu.html https://gofleeks.com/
https://krtie.co/veronagreiner https://krtie.co/veronagreiner
https://git.simbarbet.com/kristinasprent git.simbarbet.com
https://devkona.net/marjoriecarpen devkona.net
https://bizad.io/read-blog/21633_anavar-feminine-before-and-after.html https://bizad.io/read-blog/21633_anavar-feminine-before-and-after.html
https://www.google.com.uy/url?q=https://telegra.ph/Anavar-Outcomes-A-Detailed-Before-and-After-Review-10-19 https://www.google.com.uy/url?q=https://telegra.ph/Anavar-Outcomes-A-Detailed-Before-and-After-Review-10-19
https://www.bongmedia.tv/@rtmsherlyn072?page=about http://www.bongmedia.tv
https://www.toparma.com/devon157563120 https://www.toparma.com/
https://git.manabo.org/kaiwell8419634 git.manabo.org
https://ai.holiday/read-blog/57146_anavar-for-women-the-most-effective-anavar-cycle-for-ladies-anavar-earlier-than.html https://ai.holiday
https://forge.coreymclark.com/lisaiid1246980 https://forge.coreymclark.com/
https://https://cute.link/axljuliann6801/axljuliann6801 cute.link
https://alstr.in/arronrenwick7 alstr.in
http://www.annunciogratis.net/author/genevasnm19 http://www.annunciogratis.net/author/genevasnm19
repo.apps.odatahub.net · October 20, 2025 at 12:08 am
dianabol and deca cycle
https://gitlab.cranecloud.io/bonitalentz86 gitlab.cranecloud.io
https://twing.win/read-blog/2804_anavar-for-ladies-benefits-dosage-side-effects-amp-safe-use-guide.html twing.win
https://allyoutubes.com/@miriamk5982290?page=about https://allyoutubes.com/@miriamk5982290?page=about
http://chengchennet.cn:3000/danielnadeau3 http://chengchennet.cn:3000/danielnadeau3
https://g.ovlg.com/rileycalwell79 g.ovlg.com
https://git.ewft.org/carmenuez67095 git.ewft.org
https://try.gogs.io/latashaboddie5/purchase-anavar-online5983/wiki/Anavar+Outcomes%253A+Before+%2526+After+Pics+Week+By+Week https://try.gogs.io/
https://katibemaraty.com/@claricestaplet?page=about katibemaraty.com
https://g.ovlg.com/louistesch585 https://g.ovlg.com
https://srsbkn.eu.org/walkerdelagarz srsbkn.eu.org
https://gitstud.cunbm.utcluj.ro/ottokallas1647/legit1997/-/issues/1 https://gitstud.cunbm.utcluj.ro/ottokallas1647/legit1997/-/issues/1
https://git.hantify.ru/arielle15v2627 https://git.hantify.ru
http://www.zhuchaohui.com:3000/damiangoldsbro/damian2004/wiki/Earlier+Than+And+After%253A+8-week+Anavar+Feminine+Transformation http://www.zhuchaohui.com
https://maps.google.com.qa/url?q=https://careers.cblsolutions.com/employer/anavar-transformation-journey-anticipated-results-and-realistic-expectations/ https://maps.google.com.qa
http://www.cdlaber.com/home.php?mod=space&uid=251557 http://www.cdlaber.com
http://rhx0.top:3000/moniquekyte28 rhx0.top
https://www.mathhomeworkanswers.org/user/facebotany5 http://www.mathhomeworkanswers.org
https://adiyat.link/kieradoe234999 adiyat.link
References:
https://repo.apps.odatahub.net/michellecarawa
www.dycangku.com · October 20, 2025 at 1:07 am
dianabol deca cycle
http://lamsn.bigbuk.com/home.php?mod=space&uid=1457338 http://lamsn.bigbuk.com/home.php?mod=space&uid=1457338
https://baby-newlife.ru/user/profile/269093 baby-newlife.ru
https://nujob.ch/companies/full-anavar-cycle-guide-dosage-security-tips/ nujob.ch
https://www.google.com.pk/url?q=https://forum.petstory.ge/read-blog/34283_anavar-transformation-reveal-stunning-before-and-after-photos-that-will-shock-yo.html https://www.google.com.pk/url?q=https://forum.petstory.ge/read-blog/34283_anavar-transformation-reveal-stunning-before-and-after-photos-that-will-shock-yo.html
https://seferpanim.com/read-blog/33539_anavar-earlier-than-and-after-effects-results-and-dangers.html seferpanim.com
https://git.pingupod.de/carlosmoris474/3292658/wiki/Anavar+Before+And+After%253A+What+Bodybuilders+Appear+To+Be+Earlier+Than+And+After+Anavar+Results git.pingupod.de
https://baby-newlife.ru/user/profile/268607 baby-newlife.ru
https://git.getmind.cn/jerryfernandes git.getmind.cn
https://www.simpra.org:3000/trevorsigmon11 https://www.simpra.org
https://301.tv/claudettecardo 301.tv
https://git.traband.ovh/charliginder86/2889313/wiki/Anavar-Unwanted-Aspect-Effects%2C-Steroid-Abuse%2C-Withdrawal-%26-Therapy https://git.traband.ovh/
https://ryanwhittingham.com/git/romanbrownlee0 ryanwhittingham.com
https://cricfytv.buzz/read-blog/1472_anavar-before-and-after.html cricfytv.buzz
https://chateando.net/read-blog/34710_anavar-oxandrolone-advantages-side-effects-dosage-and-extra.html chateando.net
https://play.eccentric.etc.br/@shadrymer38664?page=about play.eccentric.etc.br
https://git.auwiesen2.de/arturoschlapp https://git.auwiesen2.de
https://my2.biz/myxboyce8 my2.biz
http://sorucevap.kodmerkezi.net/user/nosestream6 http://sorucevap.kodmerkezi.net/user/nosestream6
References:
https://www.dycangku.com/space-uid-110787.html
https://git.zanxiangnet.com · October 20, 2025 at 3:43 am
testosterone trenbolone dianabol cycle
https://auric-org.org/clintstonehous https://auric-org.org/
https://jamboz.com/read-blog/51504_hi-tech-pharmaceuticals-anavar-one-hundred-eighty-tablets-for-sale.html jamboz.com
https://git.svidoso.com/hazelbrendel63 git.svidoso.com
https://flirtivo.online/@jennigeorg7178 https://flirtivo.online/
http://git.bemagicart.com/eusebiawaldo2 git.bemagicart.com
http://www.canglanxing.cn:3000/lavonne136987 canglanxing.cn
https://app.theremoteinternship.com/read-blog/155881_complete-anavar-cycle-information-dosage-amp-safety-tips.html https://app.theremoteinternship.com
https://talentformation.net/employer/best-steroid-for-ladies-for-muscle-growth-and-fat-loss-2025/ talentformation.net
https://aweza.co/employer/anavar-cycle-key-information-and-incessantly-asked-questions/ https://aweza.co/
https://ezonnerecruit.com/employer/anavar-results-in-bodybuilding-evaluating-the-earlier-than-and-after/ ezonnerecruit.com
https://r12imob.store/index.php?page=user&action=pub_profile&id=755913 r12imob.store
https://git.fandiyuan.com/donj0778889958 https://git.fandiyuan.com/donj0778889958
https://pilowtalks.com/@alyciadowie56 pilowtalks.com
https://joylife.in/read-blog/16244_before-and-after-steroids-10-transformations.html joylife.in
https://git.connectplus.jp/eliaswillison8/elias2000/wiki/Five-year+Outcomes+After+Long-term+Oxandrolone+Administration+In+Severely+Burned+Children%3A+A+Randomized+Medical+Trial.- git.connectplus.jp
https://kairoskonnectinc.com/employer/anavar-earlier-than-and-after-results/ https://kairoskonnectinc.com/employer/anavar-earlier-than-and-after-results
https://careerjungle.co.za/employer/the-guts-of-the-web/ careerjungle.co.za
https://645123.com/@lyndaloader193?page=about https://645123.com
References:
https://git.zanxiangnet.com/kennith197219/3964where-to-buy-legit-anavar/wiki/Anavar+Ends+In+Bodybuilding%253A+Evaluating+The+Earlier+Than+And+After
https://jobs.atlanticconcierge-gy.com · October 20, 2025 at 5:14 am
best dianabol cycle
https://shorterminy.com/hiltondarosa66 shorterminy.com
https://prel.ink/bernda3702623 https://prel.ink
https://ryanwhittingham.com/git/olivapurser477 https://ryanwhittingham.com/git/olivapurser477
https://moonifie.com/read-blog/78491_anavar-earlier-than-and-after-what-bodybuilders-seem-like-before-and-after-anava.html moonifie.com
https://thewilcoxreport.com/forums/users/lentilsock17/ thewilcoxreport.com
https://7or.net/vanstover35420 7or.net
https://thewilcoxreport.com/forums/users/gymdrain16/ thewilcoxreport.com
https://talentformation.net/employer/consultants-reveal-one-of-the-best-time-to-take-creatine-for-finest-outcomes/ talentformation.net
https://support.mlone.ai/harrisfield67 support.mlone.ai
https://git.srv.ink/glenna34149399 git.srv.ink
https://casjobs.in/employer/trenbolone-cycle-information-stacks-and-dosages-for-bulking-and-cutting/ https://casjobs.in/employer/trenbolone-cycle-information-stacks-and-dosages-for-bulking-and-cutting
https://7or.net/vanstover35420 https://7or.net
https://jobsrific.com/employer/anavar-earlier-than-and-after-what-to-anticipate-from-this-well-liked-performance-enhancer/ jobsrific.com
https://dexbom.com/chassidybeyers https://dexbom.com/chassidybeyers
http://kikijobs.com/employer/anavar-for-weight-loss-fat-loss-how-much-will-users-lose/ kikijobs.com
https://www.muslimlove.com/@stanleywilhite http://www.muslimlove.com
https://git.traband.ovh/carsonkyte559 https://git.traband.ovh
https://trabaja.talendig.com/employer/dianabol-actual-before-after-results-timing-secrets-and-techniques-and-significant-safety-protocols/ trabaja.talendig.com
References:
https://jobs.atlanticconcierge-gy.com/employer/the-guts-of-the-internet/
Buchmachern · October 20, 2025 at 7:48 am
beste fortnite wettanbieter
Here is my web blog Buchmachern
afritunes.net · October 20, 2025 at 8:34 am
how to take dianabol first cycle
http://oa.sccehui.com:6101/violetgellert9 http://oa.sccehui.com:6101/violetgellert9
https://gitea.mocup.org/lea89r8029284 gitea.mocup.org
https://gitea.synapsetec.cn/joycelynbachma gitea.synapsetec.cn
https://git.ellinger.eu/susannebey4022 https://git.ellinger.eu
https://clone-deepsound.paineldemonstrativo.com.br/carmellahedber https://clone-deepsound.paineldemonstrativo.com.br/carmellahedber
https://auric-org.org/vedagiffen0499 https://auric-org.org/
http://share.pkbigdata.com/poppybrookins0 share.pkbigdata.com
https://voicync.com/georgiannanew voicync.com
https://syq.im:2025/cheri332465751 syq.im
https://speeddating.co.il/@lola87q966230 speeddating.co.il
http://git.fandiyuan.com/ftvmillie68110 git.fandiyuan.com
https://tintinger.org/cooperpadilla3 https://tintinger.org/cooperpadilla3
https://www.soundofrecovery.org/sanorakanode0 http://www.soundofrecovery.org
https://www.besolife.com/@florinemccallu http://www.besolife.com
http://saromusic.ir/ajagrimm51595 http://saromusic.ir/ajagrimm51595
http://sheyiyuan.cn:3000/yongchristians sheyiyuan.cn
http://wangchongwu.vicp.fun:3333/alejandrinakul wangchongwu.vicp.fun
https://gitea.ontoast.uk/adrianpress42 gitea.ontoast.uk
References:
https://afritunes.net/jeramychampagn
https://gitea.fcliu.net/trentlittlejoh · October 20, 2025 at 8:47 am
dianabol cycle dosage
https://slowdating.ca/@wendigearhart9 slowdating.ca
https://git.anacsoft.com/bradchristison https://git.anacsoft.com
https://hipstrumentals.net/halinabloomer hipstrumentals.net
https://music.white-pilled.tv/jennifermaher3 music.white-pilled.tv
https://zurimeet.com/@diannedillion zurimeet.com
https://syq.im:2025/emmettstopford syq.im
https://kingpeter.ewsstagging.com/troybui4048101 kingpeter.ewsstagging.com
http://gitea.danongshu.cn/archiei9668522 http://gitea.danongshu.cn/archiei9668522
https://gitea.mpc-web.jp/hwahodel808998 gitea.mpc-web.jp
https://gitea.gimmin.com/corazonmassie3 gitea.gimmin.com
https://gitea3.ecloud.e3labs.net/belenmcmahan32 gitea3.ecloud.e3labs.net
https://hipstrumentals.net/salliegarrity https://hipstrumentals.net/salliegarrity
https://csmsound.exagopartners.com/dakotajoyner28 csmsound.exagopartners.com
https://hafrikplay.com/orenbussey6284 hafrikplay.com
https://git.rbsx.de/cassiemiller58 https://git.rbsx.de/
https://gitlab.herzog-it.de/bebecolquhoun gitlab.herzog-it.de
https://gitea.coderpath.com/keira960847450 gitea.coderpath.com
https://gitlab.ui.ac.id/chancenoriega https://gitlab.ui.ac.id/
References:
https://gitea.fcliu.net/trentlittlejoh
Enriqueta · October 20, 2025 at 4:59 pm
sportwetten schweiz app
Here is my web blog – esports wetten deutschland – Enriqueta,
hkcomputers.co.za · October 20, 2025 at 5:27 pm
online wettanbieter test
My site :: Sportwetten tipps morgen (hkcomputers.co.za)
sermorelin/ipamorelin blend reviews · October 21, 2025 at 12:40 am
sermorelin ipamorelin program
https://infinitystaffingsolutions.com/employer/mastering-ipamorelin-cycles-ideal-doses-scheduling-and-top-peptide-combinations/ infinitystaffingsolutions.com
http://progress.matorres.com.br/index.php?action=profile;u=38566 sermorelin / ipamorelin / cjc1295 500/250/100mcg rdt
https://smartbusinesscards.in/robertgibb5408 sermorelin ipamorelin blend peptide for men
https://10xhire.io/employer/cjc-1295-vs.-sermorelin:-choosing-the-superior-growth-hormone-peptide/ sermorelin ipamorelin
https://dialsexe.pro/kristanochoa46 https://dialsexe.pro
https://advokatsthlm.se/sermorelin-dosage-cheat-sheet-optimal-amounts-for-peak-effectiveness/ what is the doseage for 5mg sermorelin 5mg ipamorelin
http://forum.emrpg.com/home.php?mod=space&uid=1413863&do=profile valley.md
http://jobteck.com/companies/peptide-showdown-ipamorelin-vs-tesamorelin-sermorelin-cjc-1295-and-the-rest-of-the-field/ ipamorelin sermorelin acetate
https://alumni.tu-sofia.bg/employer/sermorelin-and-ipamorelin-a-dual-action-growth-hormone-strategy/ valley.md
http://users.atw.hu/oldfastmt2board/index.php?PHPSESSID=114a8668ebe2fbf5854fd61633473d3c&action=profile;u=22256 ipamorelin sermorelin dosage
https://wp.nootheme.com/jobmonster/dummy2/companies/sermorelin-vs-ipamorelin-a-comparison-of-growth-hormone-secretagogues/ sermorelin ipamorelin vs mk677
https://rentry.co/56080-ipamorelin-vs-sermorelin-choosing-the-ideal-peptide-treatment rentry.co
https://www.9ks.info/index.php?action=profile;u=44827 valley.md
https://rejobbing.com/companies/calculating-the-right-ipamorelin-dose-and-timing-for-optimal-bodybuilding-results/ is ipamorelin or sermorelin better
https://adremcareers.com/employer/sermorelin-success-stories-transformations-and-key-takeaways/ valley.md
https://jobfinders.live/companies/real-world-evidence-of-multiple-myeloma-treatment-2013-2019-in-the-hospital-district-of-helsinki-and-uusimaa-finland/ valley.md
https://alumni.tu-sofia.bg/employer/sermorelin-vs-ipamorelin-which-peptide-delivers-superior-results-for-vitality-aesthetics-and-regenerative-health/ sermorelin ipamorelin blend peptide for men
https://academiabelezza.com/employer/growth-hormone-boosters-showdown-sermorelin-vs-ipamorelin-explained/ sermorelin vs tesamorelin vs ipamorelin
References:
https://thelegallock.com/job/companies/which-growth-hormone-secretagogue-reigns-supreme-a-side-by-side-look-at-sermorelin-ipamorelin-and-tesamorelin/
directorio.restaurantesdeperu.com · October 21, 2025 at 2:01 am
sermorelin + ipamorelin blend
https://careers.cblsolutions.com/employer/mixing-sermorelin-and-ipamorelin-is-it-safe/ ipamorelin vs sermorelin vs tesamorelin
https://quickfixinterim.fr/employer/peptide-showdown-ipamorelin-vs-tesamorelin-sermorelin-cjc-1295-and-the-rest-of-the-field/ https://quickfixinterim.fr/employer/peptide-showdown-ipamorelin-vs-tesamorelin-sermorelin-cjc-1295-and-the-rest-of-the-field/
https://arlogjobs.org/employer/the-core-of-the-web/ sermorelin-ipamorelin-cjc1295 pills
https://working.altervista.org/employer/sermorelin-vs-ipamorelin-choosing-the-right-growth-hormone-peptide-for-you/ valley.md
https://anychinajob.com/companies/top-peptide-stack-picks-for-2025-the-definitive-guide/ ipamorelin sermorelin cycle
https://jobsforfiji.com/companies/ipamorelin-vs-sermorelin-key-differences-you-should-know/ what is the difference between ipamorelin and sermorelin
https://infinitystaffingsolutions.com/employer/synergistic-peptide-regimens-sermorelin-ipamorelin/ ipamorelin 9mg and sermorelin
https://portalwe.net/employer/mixing-sermorelin-and-ipamorelin-is-it-possible/ ipamorelin vs sermorelin reddit
https://analyticsjobs.in/jobs/companies/comparing-tesamorelin-sermorelin-and-ipamorelin-a-review-of-current-research-findings/ peg-mg ipamorelin and sermorelin series dosage
https://alumni.tu-sofia.bg/employer/ipamorelin-vs-sermorelin-a-complete-side-by-side-review-and-practical-guide/ valley.md
https://www.cbl.aero/employer/safeguard-your-concepts/ valley.md
https://cercalavoro.com/employer/comparing-gh-peptides-tesamorelin-vs-sermorelin-ipamorelin-and-cjc-1295-guide/ can you mix sermorelin and ipamorelin
https://jobs.kwintech.co.ke/companies/ipamorelin-cjc-1295-a-powerful-synergy-for-peak-performance/ can ipamorelin and sermorelin be taken together
https://bernard-guericolas.eu/index.php?action=profile;u=66913 buy sermorelin ipamorelin cjc1295 combo
https://flhstaffing.com/employer/sermorelin-vs.-ipamorelin:-is-this-peptide-combo-worth-it/?/ https://flhstaffing.com/employer/sermorelin-vs.-ipamorelin:-is-this-peptide-combo-worth-it/?
https://orb.tl/asanmp80218281 valley.md
https://www.cbl.aero/employer/cjc-1295-vs-sermorelin-uses-benefits-and-key-factors-to-consider/ sermorelin & ipamorelin blend
https://www.fightdynasty.com/companies/synergistic-peptide-regimen-sermorelin-plus-ipamorelin/ http://www.fightdynasty.com
References:
https://directorio.restaurantesdeperu.com/employer/sermorelin-vs-cjc-1295-which-peptide-therapy-is-right-for-you/
sermorelin ipamorelin theanine · October 21, 2025 at 4:37 am
sermorelin/ipamorelin/theanine
https://timviec24h.com.vn/companies/sermorelin-and-ipamorelin-a-powerful-peptide-stack/ valley.md
https://qr.nub-1.com/janellloxton80 sermorelin & ipamorelin
https://ggapps.xyz/annettbrookshi tesamorelin vs sermorelin vs ipamorelin reddit
https://anychinajob.com/companies/optimizing-the-use-of-cjc-1295-ipamorelin-and-ghrp-2-a-dosage-guide/ sermorelin and ipamorelin stack dosage
https://moyatcareers.co.ke/companies/sermorelin-vs-ipamorelin-a-side-by-side-review-of-growth-hormone-peptide-therapies/ sermorelin ipamorelin program
https://go.on.tc/grhopal362544 buy sermorelin & ipamorelin blend
https://adremcareers.com/employer/ipamorelin-cjc-1295-results-before-and-after/ ipamorelin vs tesamorelin vs sermorelin
https://bernard-guericolas.eu/index.php?action=profile;u=66911 sermorelin ipamorelin blend 10mg dosage
https://candidates.giftabled.org/employer/top-growth-hormone-peptide-picks-ranked-list-and-essential-insights/ valley.md
https://demanza.com/employer/sermorelin-vs-ipamorelin-choosing-the-right-growth-hormone-peptide-for-your-needs/ difference between sermorelin and ipamorelin
https://contact-us.my/renatoz368701 valley.md
https://10xhire.io/employer/us-made-comparison:-sermorelin-vs.-ipamorelin-vs.-tesamorelin-benefits/ https://10xhire.io
https://walo.vip/beadorsett6983 valley.md
https://candidates.giftabled.org/employer/sermorelin-vs-ipamorelin-which-peptide-wins/ ipamorelin and sermorelin stack
https://www.teacircle.co.in/sermorelin-ipamorelin-blended-dosing-guide-2/ sermorelin tesamorelin ipamorelin
https://www.cbl.aero/employer/what-sets-ipamorelin-apart-from-sermorelin/ valley.md
https://careers.cblsolutions.com/employer/mixing-sermorelin-and-ipamorelin-is-it-safe/ what is the doseage for 5mg sermorelin 5mg ipamorelin
https://jandlfabricating.com/employer/sermorelin-vs-cjc-1295-and-ipamorelin-which-peptide-therapy-is-best-for-hgh-optimization/ take sermorelin and ipamorelin together same syringe
References:
https://www.9ks.info/index.php?action=profile;u=44815
ipamorelin vs sermorelin steroids · October 21, 2025 at 5:11 am
ipamorelin vs sermorelin bodybuilding
https://emploi-securite.com/societes/us-made-comparison-sermorelin-vs-ipamorelin-vs-tesamorelin-benefits/ emploi-securite.com
https://felipesbackyard.com/ipamorelin-applications-advantages-how-it-works-recommended-doses-and-potential-adverse-effects/ valley.md
https://www.securityprofinder.com/employer/top-peptide-stack-picks-for-2025-the-definitive-guide/ difference between sermorelin and ipamorelin
https://xqr.ai/luca40d915 sermorelin and ipamorelin: anti-aging peptides
https://tiny.enajam.com/mdutoni9935834 valley.md
https://www.jobindustrie.ma/companies/ipamorelin-dose-planner-and-timing-guide-for-bodybuilders/ http://www.jobindustrie.ma
http://progress.matorres.com.br/index.php?action=profile;u=38546 valley.md
https://careers.universalair.aero/employer/us-made-comparison-sermorelin-vs-ipamorelin-vs-tesamorelin-benefits/ valley.md
https://careers.universalair.aero/employer/cjc-1295-vs-sermorelin-choosing-the-optimal-peptide-for-stimulating-growth-hormone/ valley.md
https://vagas.grupooportunityrh.com.br/employer/ipamorelin-vs-sermorelin-an-in-depth-comparison-and-practical-guide/ ipamorelin sermorelin cycle
https://dokdo.in/rosalierandell valley.md
https://ftwjobfinder.com/companies/comparing-gh-peptides-sermorelin-vs-ipamorelin-cjc-1295-and-tesamorelin-for-research-use/ can you take ipamorelin and sermorelin
https://www.jobexpertsindia.com/companies/ipamorelin-applications-advantages-how-it-works-recommended-doses-and-potential-adverse-effects/ valley.md
https://careers.simplytech.co.za/employer/growth-hormone-peptide-showdown-sermorelin-vs-ipamorelin-explained/ sermorelin vs ipamorelin and tesamorelin
https://imgo.cc/dorothy56k9631 sermorelin ipamorelin blend side effects
https://adremcareers.com/employer/sermorelin-vs-ipamorelin-a-side-by-side-look-at-growth-hormone-peptides/ sermorelin vs ipamorelin which is better
https://www.complete-jobs.co.uk/employer/overview-of-the-sermorelin-and-ipamorelin-peptide-blend valley.md
https://excelraise.com/employer/growth-hormone-secretagogues-showdown-sermorelin-vs-ipamorelin/ sermorelin-ipamorelin-cjc 1295 stack
References:
https://infinitystaffingsolutions.com/employer/sermorelin-dosing-applications-and-comparative-review/
http://Www.aonangbaansuan.com/atlantic-spins-sportwetten-online/ · October 21, 2025 at 3:55 pm
öSterreichische sportwetten Gmbh (http://Www.aonangbaansuan.com/atlantic-spins-sportwetten-online/) lizenz curacao
http://gitea.danongshu.cn · October 22, 2025 at 2:17 am
dianabol first cycle
https://kaymanuell.com/@alicazeller032?page=about https://kaymanuell.com/
http://cloud.sunlab.top:3000/jasongrasser43 http://cloud.sunlab.top:3000/jasongrasser43
http://git.yanei-iot.com:600/chdalva7747755 git.yanei-iot.com
https://nelgit.nelpi.co.uk/amadonewdegate nelgit.nelpi.co.uk
https://quickplay.pro/earnestineandr quickplay.pro
https://pleroma.cnuc.nu/mindaelizondo pleroma.cnuc.nu
https://heartbeatdigital.cn/louellatkg9789 heartbeatdigital.cn
https://financevideosmedia.com/@jacquier336019?page=about financevideosmedia.com
https://vrstube.xyz/@joshcornish661?page=about vrstube.xyz
https://shamrick.us/rickey29193798 https://shamrick.us/
https://git.autotion.net/katharinalarge https://git.autotion.net/katharinalarge
https://pokesoul.com/@estellabeaudry pokesoul.com
http://git.youkehulian.cn/helainewestbur git.youkehulian.cn
https://gitea.springforest.top/hytbenny887682 gitea.springforest.top
https://echbar.online/jami8752291513 echbar.online
https://omegat.dmu-medical.de/tashaepp932606 https://omegat.dmu-medical.de/
https://gitea.sephalon.net/leenowakowski gitea.sephalon.net
https://shamrick.us/klausb10066172 shamrick.us
References:
http://gitea.danongshu.cn/bookerjoris080
Sportwetten livescore · October 22, 2025 at 5:02 pm
doppelte chance wette
Also visit my homepage … Sportwetten livescore
surtecnica-sa.Com.ar · October 22, 2025 at 8:27 pm
wettbüro abzugeben
Here is my webpage :: Beste sportwetten (surtecnica-sa.Com.ar)
Benny · October 23, 2025 at 8:47 am
experten wette tipps heute (Benny) sportwetten
live wetten verbot · October 23, 2025 at 5:45 pm
sportwetten anmeldebonus ohne einzahlung
Here is my homepage live wetten verbot
Taj · October 23, 2025 at 7:08 pm
Asking questions are in fact nice thing if you are not understanding
anything fully, but this piece of writing presents pleasant
understanding yet.
My homepage … when will casino montreal open (Taj)
Project3.Yourchange.Eu · October 23, 2025 at 8:17 pm
usa casino free spins 2021, best winning online Casino Heist Normal Vs Hard Payout – Project3.Yourchange.Eu, nz and blackjack
mulligan usa, or no deposit roulette bonus usa
Waldo · October 24, 2025 at 11:35 am
em ergebnisse wetten
Look at my site :: esc buchmacher (Waldo)
zeroken.jp · October 24, 2025 at 2:21 pm
anabolic steroids short term effects
References:
http://zeroken.jp/1978td/album/album.cgi?mode=detail&no=19>www.045da.com/bbs/board.php%3Fbo_table
Sportwetten Anmeldebonus Ohne Einzahlung · October 24, 2025 at 2:43 pm
wettportal quotenvergleich
Look at my web-site – Sportwetten Anmeldebonus Ohne Einzahlung
Wette Frankreich Schweiz · October 25, 2025 at 10:06 am
sportwette
Also visit my web blog Wette Frankreich Schweiz
Wettanbieter Gratiswette · October 25, 2025 at 4:45 pm
beste online sportwetten anbieter
Also visit my website; Wettanbieter Gratiswette
Matthias · October 25, 2025 at 4:47 pm
österreich wette
Look into my web blog was sind handicap wetten; Matthias,
Hunderennen Online Wetten · October 26, 2025 at 6:29 pm
wettbüro rostock
Feel free to visit my web page … Hunderennen Online Wetten
Soundtrackworld.Altervista.org · October 27, 2025 at 1:27 pm
die besten wetten unter freunden
Also visit my blog … sportwetten wer wird Deutscher meister (Soundtrackworld.Altervista.org)
Www.Evergoldcs.Com · October 27, 2025 at 3:21 pm
handicap Online Wetten Ohne Einzahlung, http://Www.Evergoldcs.Com, strategie
Sportwetten Apps Vergleich · October 27, 2025 at 5:44 pm
neueste wettanbieter
Feel free to visit my website :: Sportwetten Apps Vergleich
Https://Zayeat-Bord.Ir/Blog/2025/10/27/Sbobet-10-Euro-Freebet-Code/ · October 28, 2025 at 12:51 am
wetten ohne einzahlung bonus
my web-site – Beste Sportwetten Tipps App –
https://Zayeat-Bord.Ir/Blog/2025/10/27/Sbobet-10-Euro-Freebet-Code/ –
Deagan.comey.com · October 28, 2025 at 1:20 pm
wettformat sportwetten bonus ohne einzahlung
Also visit my web blog … wettbüro bergedorf (Deagan.comey.com)
togel online · November 8, 2025 at 4:05 pm
I’m impressed, I must say. Seldom do I encounter a blog that’s both educative and amusing, and without a doubt, you
have hit the nail on the head. The issue is an issue that not enough people are speaking intelligently about.
Now i’m very happy I stumbled across this during my hunt for something relating to this.
Lsm99dna · November 9, 2025 at 2:31 pm
Very nice post. I just stumbled upon your blog and wished to say that I’ve really enjoyed surfing around your blog posts. After all I’ll be subscribing for your feed and I am hoping you write again soon! ล็อกอิน lsm99
Thng dang k'y binance · November 24, 2025 at 12:33 pm
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Cwsdelhi.Co.In · November 25, 2025 at 3:01 pm
kombiwette spiel abgebrochen
Also visit my web-site – Bonus Vergleich Sportwetten (Cwsdelhi.Co.In)
wer hat die besten quoten sportwetten · November 26, 2025 at 2:19 pm
wetten wer hat die besten quoten sportwetten vergleich
beste app für sportwetten · November 27, 2025 at 7:40 pm
beste app für sportwetten kombiwetten strategie
patriciusit.com · December 1, 2025 at 4:23 am
pendleton casino
References:
https://git.kirasparkle.de/lanechurch609
www.memememo.com · December 2, 2025 at 8:50 pm
roulette systeme mein roulette online
References:
https://kintop.ru/user/camroddugz
vip.cengfan6.com · December 2, 2025 at 10:38 pm
hard rock casino vancouver
https://www.cool-bookmarks.win/best-online-casinos-in-australia-2025-top-casino-sites http://www.cool-bookmarks.win
http://tudositok.hu/redirect.php?ad_id=10000033&ad_url=https://hotgirlsforum.com/member.php?action=profile&uid=131117 http://tudositok.hu/redirect.php?ad_id=10000033&ad_url=https://hotgirlsforum.com/member.php?action=profile&uid=131117
http://footballzaa.com/out.php?url=https://www.mapleprimes.com/users/beunnaqfyb http://footballzaa.com/
https://www.strobe-bookmarks.win/winspirit-login-registration-australia-sign-up-guide http://www.strobe-bookmarks.win
https://storage.athlinks.com/logout.aspx?returnurl=https://www.argfx.argfx1.com/user/camercacko https://storage.athlinks.com/
https://lordfilm-2025.biz/user/andhoniquv lordfilm-2025.biz
http://childpsy.org/bitrix/redirect.php?event1=&event2=&event3=&goto=https://al-nasr.pl/user/aleslekbcd http://childpsy.org/bitrix/redirect.php?event1=&event2=&event3=&goto=https://al-nasr.pl/user/aleslekbcd
http://www.rohstoff-welt.de/goto.php?url=https://www.4shared.com/s/fTpof1_pwfa http://www.rohstoff-welt.de
http://www.akwaibomnewsonline.com/news/index.php?url=https://travelersqa.com/user/ceinnajrqe http://www.akwaibomnewsonline.com
http://delphi.larsbo.org/user/grufusbwtn http://delphi.larsbo.org
http://www.amicacard.it/data/banner/html5_convenzioni_gold/?url=https://www.alphabookmarks.win/best-texas-online-casinos-2025-top-15-tx-gambling-sites http://www.amicacard.it/
https://www.bookmarking-maze.win/playcroco-casino https://www.bookmarking-maze.win/playcroco-casino
http://tudositok.hu/redirect.php?ad_id=10000033&ad_url=https://hotgirlsforum.com/member.php?action=profile&uid=131117 http://tudositok.hu
http://www.akwaibomnewsonline.com/news/index.php?url=https://travelersqa.com/user/ceinnajrqe http://www.akwaibomnewsonline.com/news/index.php?url=https://travelersqa.com/user/ceinnajrqe
https://www.strobe-bookmarks.win/top-10-online-casino-real-money-sites-in-the-usa-for-2025 http://www.strobe-bookmarks.win
https://fr.grepolis.com/start/redirect?url=https://www.polystoned.de/User-albiussrzm https://fr.grepolis.com/start/redirect?url=https://www.polystoned.de/User-albiussrzm
http://www.kurapica.net/vb/redirector.php?url=https://files.fm/u/xhq87fe8u9 http://www.kurapica.net
http://www.mailstreet.com/redirect.asp?url=https://go.bubbl.us/eee9ad/ccb5?/Bookmarks http://www.mailstreet.com
References:
https://www.bookmark-url.win/ripper-casino-review-expert-player-ratings-2025
www.memememo.com · December 3, 2025 at 2:06 am
hollywood casino joliet il
http://http://www.memememo.com/link.php?url=https://equinox-hound-0e5.notion.site/AmunRa-Casino-No-Deposit-Bonus-Claim-Yours-Today-2bc80b4c091e80a7b3dac38b79f3c273?source=copy_link/link.php?url=https://equinox-hound-0e5.notion.site/AmunRa-Casino-No-Deposit-Bonus-Claim-Yours-Today-2bc80b4c091e80a7b3dac38b79f3c273?source=copy_link http://www.memememo.com/
https://oren-expo.ru/user/profile/684949 oren-expo.ru
http://football.sodazaa.com/out.php?url=http://www.mediafire.com/file/azxg2a28vhgs4yc/pdf-49984-60610.pdf football.sodazaa.com
https://getpocket.com/redirect?url=https://go.bubbl.us/eee908/0af7?/Bookmarks https://getpocket.com/
http://ssomgmt.ascd.org/profile/createsso/createsso.aspx?returnurl=https://israeluwtp602.huicopper.com/play-slots-online-for-real-money-usa-top-10-casinos-for-2025 ssomgmt.ascd.org
http://www.garrisonexcelsior.com/redirect.php?url=https://v3.fargo-lordfilm.top/user/sixtedujsl http://www.garrisonexcelsior.com
http://garmoniya.uglich.ru/user/soltosodmb garmoniya.uglich.ru
https://orderviag.com//member.php?action=profile&uid=64728 https://orderviag.com
https://mods.empireg.ru/user/corieljitg https://mods.empireg.ru
http://gkdc.ru/user/eriatsmfip gkdc.ru
http://www.automaniasiouxfalls.com/LinkOut/?goto=http://hondaikmciledug.co.id/HRIS/member.php?action=profile&uid=272939 http://www.automaniasiouxfalls.com
https://bumiasri.org/user/diviusvmdu bumiasri.org
https://www.generate-bookmark.win/dining-albuquerque-downs-casino http://www.generate-bookmark.win
http://www.seeleben.de/extern/link.php?url=http://www.writemob.com//user/sionnapoki http://www.seeleben.de
http://xn--l1ae1d.xn--b1agalyeon.xn--80adxhks/user/berhanutlg l1ae1d.творение.москва
http://mcclureandsons.com/projects/Water_Wastewater/Sumner_WWTP.aspx?Returnurl=https://www.livekavkaz.ru/user/heldazgfvq http://mcclureandsons.com/
http://xn--l1ae1d.xn--b1agalyeon.xn--80adxhks/user/aspaidhdqc http://l1ae1d.творение.москва/user/aspaidhdqc
https://tradersrating.ru/user/launusjmwx https://tradersrating.ru/user/launusjmwx
pokerstarseu · December 3, 2025 at 5:01 am
Alright lads, PokerStars in Europe can be a bit of a pain with all the regulations. But this pokerstarseu link sorted me right out. Got my account sorted and ready to grind. Cheers!
u.42.pl · December 3, 2025 at 7:37 am
slot canyons utah
http://www.serbiancafe.com/lat/diskusije/new/redirect.php?url=https://direct-view.ru/user/personowbc http://www.serbiancafe.com
https://pl.grepolis.com/start/redirect?url=https://dallasenut709.cavandoragh.org/ii-is-n1-casino-legit-an-in-depth-review-bonuses https://pl.grepolis.com/start/redirect?url=https://dallasenut709.cavandoragh.org/ii-is-n1-casino-legit-an-in-depth-review-bonuses
http://named.com/go.php?url=https://diego-maradona-ar.org/user/viliagahfo http://named.com/go.php?url=https://diego-maradona-ar.org/user/viliagahfo
https://www.livekavkaz.ru/user/gettanbjtc https://www.livekavkaz.ru/user/gettanbjtc
http://loredz.com/vb/go.php?url=https://pin.it/mkOQDtKWA http://loredz.com
http://italianculture.net/redir.php?url=https://www.bookmarking-online.win/the-star-asx-sgr-fails-to-secure-940m-lifeline http://italianculture.net
https://storage.athlinks.com/logout.aspx?returnurl=https://tradersrating.ru/user/forlenlyyj storage.athlinks.com
https://topkinolar.net/user/gettanxhmb https://topkinolar.net/user/gettanxhmb
http://www.bausch.in/en-in/redirect/?url=https://go.bubbl.us/eee908/0af7?/Bookmarks http://www.bausch.in
https://rutor-org.games/user/beleifcuxr rutor-org.games
http://m.landing.siap-online.com/?goto=https://www.4shared.com/s/fHF92c9CPjq http://m.landing.siap-online.com/
https://www.argfx.argfx1.com/user/nuadanlubz http://www.argfx.argfx1.com
http://alr.7ba.info/out.php?url=https://www.4shared.com/s/fb10Mewk6fa alr.7ba.info
http://www.google.co.mz/url?sa=t&rct=j&q=&esrc=s&source=web&cd=8&cad=rja&sqi=2&ved=0CGkQFjAH&url=https://www.kilobookmarks.win/social-casino-bonus-codes-free-sc-promo-codes-coins http://www.google.co.mz/url?sa=t&rct=j&q=&esrc=s&source=web&cd=8&cad=rja&sqi=2&ved=0CGkQFjAH&url=https://www.kilobookmarks.win/social-casino-bonus-codes-free-sc-promo-codes-coins
https://proxy-kaufen.com/user/neasaldnxs https://proxy-kaufen.com
http://www.premio-tuning-bestellshop.at/Home/tabid/2115/Default.aspx?returnurl=https://blurriechan.blurriecon.com/member.php?action=profile&uid=173056 http://www.premio-tuning-bestellshop.at/Home/tabid/2115/Default.aspx?returnurl=https://blurriechan.blurriecon.com/member.php?action=profile&uid=173056
http://v.miqiu.com/url/?url=http://uchkombinat.com.ua/user/broughkuez http://v.miqiu.com/url/?url=http://uchkombinat.com.ua/user/broughkuez
http://www.usagitoissho02.net/rabbitMovie/gotoUrl.php?url=http://topheadlines.ru/user/botwinjsdi http://www.usagitoissho02.net
References:
http://www.spaste.com/redirect.php?url=https://Turkish-Serial.ru/user/gwennozswl
https://proxy-buy.com · December 3, 2025 at 12:49 pm
quick hit slots
http://bax.kz/redirect?url=https://al-nasr-sports-club.org/user/ismerdsvrb bax.kz
http://www.pagespan.com/external/ext.aspx?url=http://bioimagingcore.be/q2a/user/boltonrjfy http://www.pagespan.com
http://www.gallery-ryna.net/jump.php?url=https://judahzbgv256.wpsuo.com/10-best-accommodation-in-casino-nsw-2470 http://www.gallery-ryna.net/jump.php?url=https://judahzbgv256.wpsuo.com/10-best-accommodation-in-casino-nsw-2470
http://searchamateur.com/myplayzone/?url=https://www.bookmarks4all.win/offizielle-bizzo-casino-seite searchamateur.com
http://group.so-ten.jp/redirect.php?rurl=https://www.bookmarkingqueen.win/country-club-casino-launceston-book-online-save group.so-ten.jp
http://www.bausch.in/en-in/redirect/?url=https://pin.it/mkOQDtKWA http://www.bausch.in/en-in/redirect/?url=https://pin.it/mkOQDtKWA
https://daz3d-poser.net/user/dueraiadoi daz3d-poser.net
http://www.garrisonexcelsior.com/redirect.php?url=https://www.bookmark-fuel.win/crown-melbourne-wikipedia http://www.garrisonexcelsior.com
https://Zosh1.Dv.kr.ua/user/tirgonbnni https://Zosh1.Dv.kr.ua/
https://xn—-7sbarohhk4a0dxb3c.xn--p1ai/user/meirdaasnr –7sbarohhk4a0dxb3c.рф
http://www.serbiancafe.com/lat/diskusije/new/redirect.php?url=https://papaly.com/e/Cn80 http://www.serbiancafe.com/lat/diskusije/new/redirect.php?url=https://papaly.com/e/Cn80
https://npkmir.ru/user/malronbady https://npkmir.ru/user/malronbady
http://ssomgmt.ascd.org/profile/createsso/createsso.aspx?returnurl=https://www.mixcloud.com/holtonhkhk/ http://ssomgmt.ascd.org/
http://www.hvac8.com/link.php?url=https://www.hometalk.com/member/210027574/elsie1995617 http://www.hvac8.com
http://www.automaniabrandon.com/LinkOut/?goto=https://garrettrzdh788.raidersfanteamshop.com/biggest-casino-bonuses-in-australia-400-exclusive-offers http://www.automaniabrandon.com
https://support.mikrodev.com?qa=user&qa_1=arthusnfbw https://support.mikrodev.com
http://www.meetme.com/apps/redirect/?url=https://papaly.com/d/fCB0 http://www.meetme.com/apps/redirect/?url=https://papaly.com/d/fCB0
http://www.spaste.com/redirect.php?url=https://blurriechan.blurriecon.com/member.php?action=profile&uid=173016 http://www.spaste.com
References:
https://jwac.asureforce.net/Redirect.aspx?PunchTime=&LoginId=&LogoffReason=&redirecturl=https://www.designspiration.com/thotheexbn/
555w · December 3, 2025 at 12:53 pm
Heard some buzz about 555w. Anyone tried it out yet? Looking for a new spot to play, and the site looks pretty slick. Thinking of giving it a go. Let me know if you have any insights! Check it out here: 555w
www.pageglance.com · December 3, 2025 at 2:54 pm
manistee casino
http://www.pagespan.com/external/ext.aspx?url=https://tricus64.gumroad.com/p/asino-casino-review-bonuses-promotions-games http://www.pagespan.com
https://www.belogour.news/user/eldigenscl http://www.belogour.news
http://mb.tickets.wonderworksonline.com/cart.aspx?returnurl=http://qa.doujiju.com?qa=user&qa_1=golivebiho mb.tickets.wonderworksonline.com
http://www.med.uz/bitrix/rk.php?goto=https://ets2-mods.ru/user/eriatsbwzt med.uz
https://www.bookmarking-planet.win/leprechauns-hills-pokie-2025-free-play-in-demo-mode https://www.bookmarking-planet.win/
http://www.peterblum.com/releasenotes.aspx?returnurl=https://send.now/qqsbojs1kwts http://www.peterblum.com
http://www.cricbattle.com/Register.aspx?Returnurl=https://www.yankee-bookmarkings.win/play-free-slots cricbattle.com
http://smarter-0.7ba.info/out.php?url=https://www.insert-bookmark.win/top-pokies-2025-ranked http://smarter-0.7ba.info
http://www.amicacard.it/data/banner/html5_convenzioni_gold/?url=https://writeablog.net/merlenzsrq/regulators-accept-7-8m-settlement-with-caesars-over-illegal-bookmakers-gaming http://www.amicacard.it/data/banner/html5_convenzioni_gold/?url=https://writeablog.net/merlenzsrq/regulators-accept-7-8m-settlement-with-caesars-over-illegal-bookmakers-gaming
http://www.memememo.com/link.php?url=https://msbooks.club/user/marykajmff http://www.memememo.com/link.php?url=https://msbooks.club/user/marykajmff
http://rd.am/www.crystalxp.net/redirect.php?url=https://ronaldinho.com.az/user/whyttafovd rd.am
http://www.joi3.com/go.php?url=https://www.bookmark-step.win/bizzo-cassino-jogue-online-com-bonus-e-login-rapido http://www.joi3.com/go.php?url=https://www.bookmark-step.win/bizzo-cassino-jogue-online-com-bonus-e-login-rapido
https://www.bookmark-tango.win/the-15-most-iconic-quotes-from-scorseses-casino https://www.bookmark-tango.win
http://kakaku.com/jump/?url=https://script-roblox.ru/user/branorpbfr kakaku.com
https://storage.athlinks.com/logout.aspx?returnurl=https://delivery.uncleslade.ru/user/beleifanzk storage.athlinks.com
https://topasnew24.pro/user/angelmqsan topasnew24.pro
http://m.shopinanchorage.com/redirect.aspx?url=https://kinotolkotut.com/user/britterszs http://m.shopinanchorage.com
http://www.merkfunds.com/exit/?url=https://www.charliebookmarks.win/brand-new-us-online-casino-fresh-gambling-sites-for-2025 http://www.merkfunds.com
References:
https://www.rankbookmarkings.win/15-best-online-casinos-australia-2025-real-money-casino-sites
kikuya-rental.com · December 3, 2025 at 3:33 pm
dos caminos nyc
http://www.talniri.co.il/finance/MobileMenu.aspx?returnurl=https://www.instapaper.com/read/1938146070 http://www.talniri.co.il/finance/MobileMenu.aspx?returnurl=https://www.instapaper.com/read/1938146070
http://www.pageglance.com/external/ext.aspx?url=https://www.protopage.com/rostafoikt http://www.pageglance.com
http://www.bookmerken.de/?url=https://lordfilmtv.club/user/kevineokpw http://www.bookmerken.de
http://www.52ts.com/link.php?url=https://koroche.tnt-lordfilm.net/user/caburgalcx 52ts.com
https://driver-library.com/user/hithintpbr driver-library.com
https://ableton.ru/user/conwynlmhk https://ableton.ru/user/conwynlmhk
http://spiderproject.com.ua/bitrix/rk.php?goto=https://www.echobookmarks.win/play-slots-and-live-games-with-top-kiwi-bonuses http://spiderproject.com.ua/bitrix/rk.php?goto=https://www.echobookmarks.win/play-slots-and-live-games-with-top-kiwi-bonuses
http://www.charitiesbuyinggroup.com/MemberSearch.aspx?Returnurl=http://www.writemob.com//user/eriatsaxif charitiesbuyinggroup.com
https://rowing.su/user/almodaucbg https://rowing.su/user/almodaucbg
http://maskarad.bomba-piter.ru/user/bailirvwne http://maskarad.bomba-piter.ru/user/bailirvwne
http://home4dsi.com/chat/redirect.php?url=https://www.hotel-bookmarkings.win/exclusive-offers-up-to-au-5-000 home4dsi.com
http://frienddo.com/out.php?url=https://torr2023muz.su/user/madorawwem http://frienddo.com/out.php?url=https://torr2023muz.su/user/madorawwem
http://uzmuz.tv/go.php?url=https://www.polystoned.de/User-ropherxupd uzmuz.tv
https://todosobrelaesquizofrenia.com/Redirect/?url=https://www.reverbnation.com/artist/seannaybjb https://todosobrelaesquizofrenia.com
https://acrejadid.ir/user/eregowriue acrejadid.ir
http://help.crimeastar.net/index.php?url=http://volleypedia-org.50and3.com?qa=user&qa_1=kylanaalxa http://help.crimeastar.net/index.php?url=http://volleypedia-org.50and3.com?qa=user&qa_1=kylanaalxa
https://www.charliebookmarks.win/epicurean-buffet-restaurant-in-barangaroo https://www.charliebookmarks.win/epicurean-buffet-restaurant-in-barangaroo
http://www.webclap.com/php/jump.php?url=https://www.play-bookmarks.win/luxury-hotels-las-vegas-wynn-encore-resorts http://www.webclap.com
References:
https://film3d.club/user/jorgusxmic
http://www.charitiesbuyinggroup.com/ · December 3, 2025 at 4:07 pm
sky vegas mobile
References:
https://sakhhotel.ru/user/kensetppog
timoore.eu · December 3, 2025 at 5:26 pm
roulette on line
http://www.charitiesbuyinggroup.com/MemberSearch.aspx?Returnurl=https://mandarin22.ru/user/vormasplxb http://www.charitiesbuyinggroup.com
http://www.bausch.co.nz/en-nz/redirect/?url=https://www.4shared.com/s/fb10Mewk6fa http://www.bausch.co.nz
https://www.stealth-bookmark.win/brand-new-online-casinos-nov-2025-new-real-money-legal-u-s-sites https://www.stealth-bookmark.win/brand-new-online-casinos-nov-2025-new-real-money-legal-u-s-sites
https://www.bookmark-fuel.win/play-online-casino-games-safely-fast http://www.bookmark-fuel.win
http://www.siteglimpse.com/external/ext.aspx?url=https://baby-newlife.ru/user/profile/354245 siteglimpse.com
http://searchamateur.com/myplayzone/?url=https://www.charliebookmarks.win/online-casino-reviews-ratings-by-experts-2025 searchamateur.com
http://italianculture.net/redir.php?url=https://www.scribd.com/document/957998852/5-dining-options-at-The-Star-Gold-Coast-180362 http://italianculture.net/
https://rukodel-t.ru/user/faugusjfpt https://rukodel-t.ru/user/faugusjfpt
https://robert-lewandowski-kg.com/user/golfuriowa robert-lewandowski-kg.com
http://www.fcviktoria.cz/media_show.asp?id=2924&id_clanek=2467&media=0&type=1&url=http://shiftdelete.10tl.net/member.php?action=profile&uid=238824 http://www.fcviktoria.cz
https://www.bookmarking-keys.win/casino-true-story-explained-joe-pesci-s-character-inspiration-if-the-torture-scene-really-happened-more https://www.bookmarking-keys.win/casino-true-story-explained-joe-pesci-s-character-inspiration-if-the-torture-scene-really-happened-more
http://taxibestellung24.de/php/redirect.php?url=https://www.adscron.com/user/profile/2312 taxibestellung24.de
http://www.usagitoissho02.net/rabbitMovie/gotoUrl.php?url=https://www.hometalk.com/member/210053554/nathan1367 http://www.usagitoissho02.net/
http://sigha.tuna.be/exlink.php?url=https://proonlain.ru/user/vindonzoly sigha.tuna.be
http://3zfe6.7ba.info/out.php?url=https://www.kilobookmarks.win/20-best-online-casinos-in-australia-for-real-money 3zfe6.7ba.info
http://kikuya-rental.com/bbs/jump.php?url=https://500px.com/p/brynneaxjh kikuya-rental.com
http://www.wikalenda.com/redirect?url=http://www.writemob.com//user/oraniernow http://www.wikalenda.com/
http://www.pesscloud.com/PessServer.Web/Utility/Login/LoginPess.aspx?Returnurl=https://files.fm/u/kh5d73scca http://www.pesscloud.com/PessServer.Web/Utility/Login/LoginPess.aspx?Returnurl=https://files.fm/u/kh5d73scca
References:
http://www.dicodunet.com/out.php?url=https://wg.org.ua/user/ahirthxoor
http://www.seeleben.de · December 3, 2025 at 6:21 pm
quest casino
https://www.bookmarkingvictor.win/paris-las-vegas-las-vegas-hotels-nv-89109 http://www.bookmarkingvictor.win
https://kalajovein.ir/user/muirenjzmq kalajovein.ir
http://3zfe6.7ba.info/out.php?url=https://www.mixcloud.com/kethanzhdc/ 3zfe6.7ba.info
https://wuangus.cc/go.php?url=https://files.fm/u/kh5d73scca wuangus.cc
http://kakaku.com/jump/?url=https://wg.org.ua/user/cassinmmjn http://kakaku.com/jump/?url=https://wg.org.ua/user/cassinmmjn
https://dobryakschool.ru/user/nathopqbhd dobryakschool.ru
https://www.bookmark-suggest.win/15-best-live-casinos-australia-play-against-live-dealers-online https://www.bookmark-suggest.win
http://spiderproject.com.ua/bitrix/rk.php?goto=https://medknigki-v-kemeerovo.ru/user/bandaryfou http://spiderproject.com.ua
https://moiafazenda.ru/user/cwrictcvfz moiafazenda.ru
https://sinape.ru/user/esyldavpzk sinape.ru
http://redrice-co.com/page/jump.php?url=http://f91306v7.beget.tech/member.php?action=profile&uid=217465 http://redrice-co.com/page/jump.php?url=http://f91306v7.beget.tech/member.php?action=profile&uid=217465
http://u.42.pl/?url=https://Milenamaier.shop/user/vindonxhht u.42.pl
http://www.smokymountainadventurereviews.com/goto.php?url=https://www.web-bookmarks.win/treasury-brisbane-poker-room-review-of-treasury-casino-brisbane http://www.smokymountainadventurereviews.com
http://frienddo.com/out.php?url=https://Fortuna27.ru/user/meggurgxmu frienddo.com
http://www.bausch.kr/ko-kr/redirect/?url=https://browhaus-upgrade.de/user/gobnatvbxp http://www.bausch.kr/
https://neofilm.fun/user/fastofrokw https://neofilm.fun/user/fastofrokw
http://www.kaskus.co.id/redirect?url=http://volleypedia-org.50and3.com?qa=user&qa_1=herianelos http://www.kaskus.co.id
http://www.newsdiffs.org/article-history/?url=https://brooksknpk879.wpsuo.com/cashman-casino-lobby-review-200-free-games-daily-rewards http://www.newsdiffs.org
References:
https://tojik.top/user/nycoldvvhz
http://www.memememo.com/link.php?url=https://www.booknose.win/casino-general-information · December 3, 2025 at 6:33 pm
schecter blackjack atx solo 6
http://appyet.com/handler/disqus.ashx?guid=713ae0d41568487bb47b9d09585fe482&id=45fee95b8971b2435e0570d007b5f281&locale=ar&shortname=aqoal&title=&type=1&url=https://ableton.ru/user/ceacheoukk http://appyet.com/handler/disqus.ashx?guid=713ae0d41568487bb47b9d09585fe482&id=45fee95b8971b2435e0570d007b5f281&locale=ar&shortname=aqoal&title=&type=1&url=https://ableton.ru/user/ceacheoukk
http://www.automaniabrandon.com/LinkOut/?goto=https://berhamporemunicipality.org/user/lynethfpso http://www.automaniabrandon.com
http://nvl.vbent.org/kvso/redir.php?goto=https://www.bookmark-jungle.win/slots-live-casino-hotel-maryland-r nvl.vbent.org
https://seomaestro.kz/go.php?url=https://travelersqa.com/user/ceinnajrqe https://seomaestro.kz/go.php?url=https://travelersqa.com/user/ceinnajrqe
http://johnnys.jocee.jp/jump/?url=https://www.pawn-bookmarks.win/amunra-casino-login-access-your-account-play-now johnnys.jocee.jp
http://www.nyumon.net/script/sc/redirect.php?id=393&url=https://raindrop.io/withurpajj/bookmarks-63781645 http://www.nyumon.net
https://ronaldinho-gaucho.org/user/faugustwgs ronaldinho-gaucho.org
https://www.play-bookmarks.win/best-real-money-online-casinos-in-the-us-2025 https://www.play-bookmarks.win
http://drakonas.wip.lt/redirect.php?url=https://sinape.ru/user/theredarvb drakonas.wip.lt
https://kinogobiz.online/user/devaldwnvg kinogobiz.online
https://pl.grepolis.com/start/redirect?url=https://Memz.org/user/kevotadtms pl.grepolis.com
http://www.monplawiki.com/link.php?url=https://orcid.org/0009-0008-5385-4372 http://www.monplawiki.com/link.php?url=https://orcid.org/0009-0008-5385-4372
http://lozd.com/index.php?url=https://apunto.it/user/profile/420814 lozd.com
http://k.yingjiesheng.com/link.php?url=https://www.4shared.com/s/fpmHBzQf_ku k.yingjiesheng.com
https://getpocket.com/redirect?url=https://www.mediafire.com/file/5o9ffq8ce3gt4f7/pdf-46481-58609.pdf/file getpocket.com
http://football.sodazaa.com/out.php?url=http://faq.firu-mbh.de/user/elmarandwx football.sodazaa.com
https://rukodel-t.ru/user/tirgonowhn rukodel-t.ru
http://news.tochka.net/tochkaliked/?url=https://www.echobookmarks.win/crown-perth-burswood-a-pinnacle-of-gaming-extravaganza news.tochka.net
References:
https://sonnik.nalench.com/user/mechalwqac
http://2ch-ranking.net/redirect.php?url=https://--xtbeeigk3B.xn--p1ai/user/marielxcrh · December 3, 2025 at 8:49 pm
casinobonus2
References:
http://www.bausch.com.my/en/redirect/?url=https://www.huntingnet.com/forum/members/xippusnzkh.html
utbetapp · December 4, 2025 at 1:30 am
Downloading the utbetapp was a breeze! The app itself is very intuitive and makes placing bets on the go super easy. Highly recommend if you’re always moving around. utbetapp
k88web · December 4, 2025 at 2:58 am
K88web, just landed here. Seems promising. Hoping for a user-friendly interface and a good selection of live games. Let’s see if they deliver on the hype. Check it out for yourself : k88web
Quentin · December 4, 2025 at 2:04 pm
live wetten app
Have a look at my web site :: wettbüro frankfurt (Quentin)
888slot · December 5, 2025 at 1:55 am
TONY20251204test. 888slot – cái tên top đầu trong lĩnh vực cá cược, đã chọn 888slot GAME làm đại lý chính thức để cung cấp link truy cập an toàn. Đây là đại lý được cấp quyền trực tiếp, chịu trách nhiệm cung cấp đường link 888slot ổn định và bảo mật tại Việt Nam. Để không bỏ lỡ 150.000 VNĐ tiền cược trải nghiệm miễn phí; 100% tiền nạp đầu và vô số ưu đãi độc quyền khác, hãy đăng ký tài khoản tại 888slot GAME với thông tin chính chủ ngay hôm nay.
Thad · December 5, 2025 at 11:30 am
wettformat gratiswette
Feel free to surf to my blog post; pferderennen wetten schweiz (Thad)
Louvenia · December 6, 2025 at 9:10 am
wette schweiz frankreich
Also visit my site; wett tipp ai erfahrungen, Louvenia,
Wett Tipps Heute Forebet · December 6, 2025 at 7:28 pm
sportwetten live wetten
My web site … Wett Tipps Heute Forebet
futebolfeverbr · December 6, 2025 at 8:10 pm
Futebolfeverbr é a febre do momento! Pra quem curte futebol e uma graninha extra, é o lugar certo. Fácil de usar e com odds interessantes. Não dá pra perder, hein: futebolfeverbr
semdinlitesisat.eskisehirgocukduzeltme.com · December 7, 2025 at 12:51 am
gala casino london
References:
https://trade-britanica.trade/wiki/New_Online_Casinos_Australia_2025_Guide
https://www.google.fm/ · December 7, 2025 at 3:19 am
gsn slots
References:
https://www.pdc.edu/?URL=https://blackcoin.co/crown-casino-melbourne-in-depth-guide/
images.google.bi · December 7, 2025 at 3:18 pm
gala casino london
References:
https://fkwiki.win/wiki/Post:Win_Real_Money_at_Our_Online_Casino_Play_Now
https://gpsites.stream/ · December 7, 2025 at 3:32 pm
planet7 casino
References:
https://socialbookmark.stream/story.php?title=%E2%80%8Eclassic-vegas-casino-slots-app
https://pad.karuka.tech · December 7, 2025 at 3:41 pm
river nile casino
References:
https://www.ydaojia.com/home.php?mod=space&uid=919625
157.230.187.16 · December 7, 2025 at 4:51 pm
blackjack and hookers
References:
https://www.google.ki/url?q=https://www.tarauaca.ac.gov.br/profile/kronborgjpygentry68316/profile
http://bbs.xltyun.com/ · December 7, 2025 at 7:33 pm
vegas online casino
References:
http://x.kongminghu.com/home.php?mod=space&uid=100725
bom.so · December 7, 2025 at 7:40 pm
best casino games
References:
https://maps.google.mw/url?q=https://myspace.com/soccerdahlia26
https://morse-house-2.technetbloggers.de/ · December 7, 2025 at 7:44 pm
roulette system of a down
References:
https://www.tarauaca.ac.gov.br/profile/langetacbendtsen1325/profile
http://t.044300.net/ · December 7, 2025 at 9:13 pm
casino online italiani
References:
https://www.play56.net/home.php?mod=space&uid=5860467
wzgroupup.hkhz76.badudns.cc · December 7, 2025 at 9:21 pm
red rock casino las vegas
References:
https://kanban.xsitepool.tu-freiberg.de/s/Sy4K177M-g
www.scdmtj.com · December 7, 2025 at 9:26 pm
dubuque casino
References:
https://m.jingdexian.com/home.php?mod=space&uid=5351669
http://www.hker2uk.com/ · December 8, 2025 at 6:32 pm
29 palms casino
References:
http://www.optionshare.tw/home.php?mod=space&uid=3899645
maps.google.com.qa · December 8, 2025 at 7:44 pm
hollywood casino toledo
References:
https://freebookmarkstore.win/story.php?title=new-mexicos-best-bet
mp.0954yn.top · December 8, 2025 at 8:27 pm
baton rouge casino
References:
https://linkagogo.trade/story.php?title=casino-games-that-pay-real-money-%EF%B8%8F-2025-review
images.google.com.hk · December 8, 2025 at 10:11 pm
games online games
References:
https://maps.google.nr/url?q=https://elclasificadomx.com/author/smokenumber45/
classifieds.ocala-news.com · December 8, 2025 at 10:13 pm
roulette wheel
References:
https://manghe.timizhuo520.cn/home.php?mod=space&uid=666258
sorucevap.kodmerkezi.net · December 8, 2025 at 10:17 pm
schecter blackjack atx solo 6
References:
https://www.google.dm/url?q=https://www.instapaper.com/p/17227872
maps.google.com.br · December 8, 2025 at 10:32 pm
river spirit casino tulsa ok
References:
https://maps.google.cv/url?q=https://kloster-pittman.hubstack.net/official-site-for-slots-and-top-bonuses
Nyonyafurniture.com · December 10, 2025 at 10:12 am
deutsche der buchmacher (Nyonyafurniture.com)
Annie · December 10, 2025 at 12:12 pm
unentschieden wetten spanien deutschland – Annie,
strategie
beste quoten für sportwetten · December 11, 2025 at 10:26 am
daglfing pferderennen wetten
Also visit my web blog – beste quoten für sportwetten
wir wetten Schweiz · December 11, 2025 at 2:53 pm
arbitrage sportwetten quotenvergleich
Feel free to surf to my webpage – wir wetten Schweiz
sportwetten bonus Neu · December 11, 2025 at 4:42 pm
beste fortnite wettanbieter
My website sportwetten bonus Neu
boostaro · December 18, 2025 at 3:37 pm
**boostaro**
boostaro is a specially crafted dietary supplement for men who want to elevate their overall health and vitality.
vivalis · December 18, 2025 at 3:37 pm
**vivalis**
vivalis is a premium natural formula created to help men feel stronger, more energetic, and more confident every day.
hepato burn · December 18, 2025 at 5:47 pm
**hepato burn**
hepatoburn is a high-quality, plant-forward dietary blend created to nourish liver function, encourage a healthy metabolic rhythm, and support the bodys natural fat-processing pathways.
Starda Casino App herunterladen · December 20, 2025 at 6:32 am
Um das mobile Casino zu besuchen und Games wie Handy Roulette im bet365 Schweiz zu starten, benötigst du keinen Desktop-Rechner. Ausserdem kannst du mit einem Budgetrechner ausrechnen, wie viel Geld mir monatlich für Einzahlungen bei bet365 zur Verfügung steht.Zusätzlich kannst du Verlust- und Einzahlungslimits festlegen. Eigentlich hatten wir erwartet, dass wir bei unseren bet365 Erfahrungen beim Thema verantwortungsvolles Spielen nicht mehr zu sehen bekommen als das vom Lizenzgeber vorgeschrieben. Lizenziert ist bet365 bei der Malta Gaming Authority. Die Spielbank ist seit 2001 online und heute, im Jahr 2025 beschäftigt der Betreiber tausende Mitarbeiter und erzielt einen Jahresumsatz in Milliardenhöhe.
Natürlich findet man bei bet365 all die üblichen Verdächtigen wie Fußball, Pferderennen, Tennis Boxen, Formel 1, Golf, Skispringen und viele mehr. Zu jedem einzelnen Event finden Sie dabei mitunter mehrere hundert Wettmärkte. Hier wollen wir nur einige Beispiele nennen wie Über/Unter-Wette, Anzahl Eckbälle, erster Torschütze, genauer Stand zur Halbzeit, Man of the Match usw.. Dabei beschränkt sich bet365 nicht auf die erste und zweite Liga in Deutschland. Auch für Live Wetten profitieren Sie von der Registrierung mit unserem bet365 Gutschein Code. Schließlich ist die Zahl der Sportarten beschränkt, auf die Nutzer wetten wollen.
References:
https://online-spielhallen.de/quickwin-casino-auszahlung-ein-umfassender-leitfaden-fur-reibungslose-gewinnauszahlungen/
Avantgarde Casino Passwort vergessen · December 20, 2025 at 2:37 pm
VIP-Mitglieder genießen einen persönlichen Service, höhere Auszahlungslimits und spezielle Angebote wie 888 Casino Freispiele für bestehende Kunden. Es wurde 1997 gegründet und bietet eine breite Palette von Spieloptionen, darunter Slots, Tischspiele und Live-Dealer-Spiele. 888casino ist eines der führenden Online-Casinos, das für seine Vielfalt an Spielen und seine sichere, benutzerfreundliche Plattform bekannt ist.
888casino ist eine der beliebtesten Online-Glücksspielplattformen der Welt. Spieler in Österreich können exklusive Boni und sichere Zahlungsoptionen genießen. Zum Beispiel können Spieler, die versuchen, sich von Gebieten aus anzumelden, in denen Online-Glücksspiele verboten sind, Probleme bei der Anmeldung bekommen. Dies trägt dazu bei, eine sichere Umgebung für alle Benutzer zu schaffen, damit sie ihr Spielerlebnis ohne Sorgen genießen können. Für zusätzliche Sicherheit bietet die Anmeldung bei 888casino.com eine Zwei-Faktor-Authentifizierung.
References:
https://online-spielhallen.de/ihr-ultimativer-leitfaden-zum-rant-casino-login/
r33mx · December 21, 2025 at 10:42 pm
r33mx is pretty cool. Their website design is modern and their game variety is decent. I enjoyed playing some of their arcade games. Check it r33mx out.
Stay Casino Australia bonus codes · December 26, 2025 at 2:09 pm
These audits verify fair play across all pokies and table games. Lucky Green understands that Australian players demand banking solutions that work with their lifestyle, which is why PayID payments take center stage in the platform’s financial ecosystem. Make sure you’re aware of the details about deposits, withdrawals, and bonuses before getting started. However, some minor improvements in support, payment flexibility and game variety could elevate the overall experience. Built with HTML5 technology, it delivers smooth navigation and high-quality gameplay, matching the desktop experience.
If you suspect someone is underage, immediately contact support to suspend the account. Lucky Green is built around a responsive web platform so you can play on iOS and Android without installing an app. Lucky Green hosts a wide game library featuring more than 500 pokies from well-known developers. Treat welcome offers as additional playtime — not guaranteed profit. Lucky Green’s welcome pathway is structured across multiple deposits designed to give sustained playtime.
The casino displays third-party testing and security seals, and providers’ RNG audits are part of the fairness assurances. Once verified, your path to fast withdrawals is smoother — lucky green processes payouts quickly when documentation is complete. Benefits include personal account managers, dedicated promotions and accelerated support. Streaming quality and dealer professionalism are key to a satisfying live experience. Lucky Green lists progressive titles from large networks; these games collect a small portion of each wager to fuel the jackpot pool. The site encourages healthy play and will assist players who seek help.
References:
https://blackcoin.co/this-is-vegas-casino-review/
immediate payout casino · December 26, 2025 at 10:53 pm
I tested these on my iPhone 13 and found no lag, even on live dealer games. Sites like King Johnnie and Oshi Casino offer self-exclusion tools and deposit limits to keep your play in check. A trustworthy casino displays its license prominently check the footer of sites. You won’t get in trouble for playing on these sites, as the law targets operators, not players.
Look for games with lower minimum bet requirements to get more spins and rounds out of your current budget at the best Australian online casino. If you are new to live gaming, choose classic table games with lower limits to get familiar with the live interface and real-time pace. Online pokies for real money are the most popular casino game in Australia. Top Aussie casinos often stand out because of welcome bonuses, reloads, free spins and cashback that extend playtime. The best Australian online casinos share several characteristics, but the best of them provide all the following. We’ve investigated and reviewed the top online casinos in Australia to give you a sense of what to expect.
These promotions can boost bankrolls, allow players to try new games risk-free, and reward loyalty. Understanding RTP helps players make informed choices about which games to play, potentially maximising their chances of winning or minimising losses over time. Return to Player (RTP) is the percentage of wagered money a game will pay back to players over time. While not a traditional casino game, sports betting is often integrated into online casino platforms. Live dealer craps games, like those offered by Evolution Gaming, have helped increase the game’s online presence.
References:
https://blackcoin.co/best-online-casinos-australia-2025-a-comprehensive-guide/
Luxury online casinos Canada · December 27, 2025 at 8:10 am
On February 1, 2018, it was rolled out in 130 countries worldwide, including Brazil, Mexico, Turkey, and Iraq. In February 2017, YouTube Go was launched in India, and expanded in November 2017 to 14 other countries, including Nigeria, Indonesia, Thailand, Malaysia, Vietnam, the Philippines, Kenya, and South Africa. In September 2022, YouTube TV began allowing customers to purchase most of its premium add-ons (excluding certain services such as NBA League Pass and AMC+) without an existing subscription to its base package.
Video categories on YouTube include music videos, video clips, news, short and feature films, songs, documentaries, movie trailers, teasers, TV spots, live streams, vlogs, and more. In January 2024, YouTube had more than 2.7 billion monthly active users, who collectively watched more than one billion hours of videos every day. The developer has not yet indicated which accessibility features this app supports. “Some fun and interesting videos but sad YouTube wont show videos that are opposed to their leftist agenda.” Read more “Too expensive! Takes too long to get preferred channels Don’t know how to cancel” Read more Customers find the YouTube app highly entertaining, with a wide range of content that makes the experience enjoyable.
In 2013, YouTube launched a pilot program for content providers to offer premium, subscription-based channels. That year, the company simplified its interface to increase the time users would spend on the site. Google’s acquisition launched newfound interest in video-sharing sites; IAC, which now owned Vimeo, focused on supporting the content creators to distinguish itself from YouTube. The same day, the company launched a public beta and by November, a Nike ad featuring Ronaldinho became the first video to reach one million total views.
References:
https://blackcoin.co/sol-casino-in-depth-review/
Australian casinos minimum deposit · December 27, 2025 at 10:21 am
Please note that all payments with Paysafe are processed via Hollycorn N.V.. They include VISA and MasterCard credit and debit cards, as well as various alternative payment methods. The casino is not a financial institution and thus should not be treated as such. Criminal charges will be brought against any user or any other person(s) who has/have manipulated the casino system or attempted to do so. However, a customer support agent will direct you to our customer support email service.
At Rocket, you can get started with a welcome bonus, of course. The security of the casino is a tad bit questionable at first sight. Casino will dismiss the complaint if the matter is handed over to be conducted by the third party and not the original account owner. Complaints are handled in the support department and escalated in the organisation of the Casino in the case that support personnel did not solve the case immediately.
References:
https://blackcoin.co/casino-weather-your-comprehensive-guide/
Lsm99dna · December 28, 2025 at 11:04 am
Pretty good post. I have just stumbled upon your blog and enjoyed reading your blog posts very much. I am looking for new posts to get more precious info. Big thanks for the useful info.
ลิงค์ทางเข้า lsm99
www.paknaukri.pk · December 28, 2025 at 11:28 pm
online slots uk paypal
References:
https://www.paknaukri.pk/companies/paypal-casinos-2025-best-online-casinos-accepting-paypal/
https://mapnova.com.co/ · December 28, 2025 at 11:44 pm
mobile casino paypal
References:
https://mapnova.com.co/employer/paypal-casino-sites-a-guide-to-30-casinos-accepting-paypal/
https://candidates.giftabled.org/employer/best-us-online-casinos-that-accept-paypal-in-2024/ · December 29, 2025 at 11:21 pm
online casino australia paypal
References:
https://candidates.giftabled.org/employer/best-us-online-casinos-that-accept-paypal-in-2024/
www.busforsale.ae · December 30, 2025 at 1:14 am
online betting with paypal winnersbet
References:
https://www.busforsale.ae/profile/magaret5409475
spin.org.pk · December 30, 2025 at 2:39 am
online betting with paypal winnersbet
References:
https://spin.org.pk/employer/top-payid-casinos-australia-2025-fast-secure-casino-payment/
hyojun.co.kr · December 30, 2025 at 2:48 am
online australian casino paypal
References:
https://hyojun.co.kr/bbs/board.php?bo_table=free&wr_id=46
Lsm99dna · December 30, 2025 at 3:10 pm
I really like your writing so much! share we communicate more about your article on AOL? I need an expert in this house to resolve my problem. Maybe that’s you! Having a look ahead to look you. ทางเข้า lsm99
ufo9 · December 31, 2025 at 5:52 am
With the redesigned private gaming rooms Sovereign and Oasis, the land based casino delivers the finest in premium gaming experiences. Mississippi stud poker, three card poker, Caribbean stud poker, and Texas Hold ’em bonus poker are among the poker games available on the casino floor. Only two poker tables are available in the poker room, with the majority of the games being Texas Hold ’em ($2/$3). After you’ve finished spinning the reels, walk over to the table games area to try your hand at your favorite table casino games. More information on premium membership access and advantages will be sent to eligible members.
Try your luck at the freshly rebuilt casino, which has a total area of 65,000 square feet. With award-winning restaurants and five bars, there’s plenty to do.
Alternatively, you might relax in your 5-star hotel room and take in the beautiful scenery from your suite. Before you attend the latest stage play, meet up with friends and have a meal before the night begins, or taste from the incredible buffet. There are over six restaurants, and their website offers a handy online table reservation option. After hours, choose from outdoor bars, sports bars, or the neighborhood’s hotspot, The Atrium Bar. You may enjoy lush manicured grounds, an enviable location, and five-star comfort whether you stay at The Star Grand or The Darling. There are also spa services, an outdoor pool area, and private cabanas.
References:
https://blackcoin.co/ufo9-casino-your-place-to-play-your-way/
careerterms.com · December 31, 2025 at 9:04 am
online casinos that accept paypal
References:
https://careerterms.com/companies/online-casinos-for-real-money-2025-best-paying-online-casinos-usa/
https://es-africa.com/employer/top-paypal-online-casinos-2025/ · December 31, 2025 at 8:08 pm
mobile casino paypal
References:
https://es-africa.com/employer/top-paypal-online-casinos-2025/
https://adremcareers.com · December 31, 2025 at 8:59 pm
gamble online with paypal
References:
https://adremcareers.com/employer/paypal-casinos-2025-best-paypal-slot-sites-in-the-uk/
towerclimbers.work · January 1, 2026 at 1:50 am
paypal casinos online that accept
References:
https://towerclimbers.work/employer/new-online-casinos-australia-2025-15-newest-sites/
sx777game · January 2, 2026 at 12:14 am
Alright, gave sx777game a run. I had a blast! The gameplay was engaging, and the graphics are decent. Definitely a good way to kill some time. Go give sx777game a shot!
binance registration · January 4, 2026 at 7:32 am
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
typhu88vips · January 5, 2026 at 12:05 pm
Typhu88vips, alright! Let’s see if I can finally hit that jackpot. Been playing a while, due for a good win I reckon! Ready to roll! typhu88vips
s3.amazonaws.com · January 5, 2026 at 4:17 pm
Multi-Hand-Optionen erlauben es, mehrere Hände gleichzeitig zu spielen. Anfänger können bereits mit kleinen Beträgen spielen. Spieler können jederzeit von zu Hause aus spielen. Online Blackjack bietet eine der höchsten Auszahlungsraten aller Casinospiele mit bis zu 99% Rückzahlung an die Spieler. Um sicherzustellen, dass ein Glücksspielanbieter legal ist, solltest du auf eine gültige Glücksspiellizenz achten, die von der deutschen Regulierungsbehörde ausgestellt wurde.
Es bietet eine massive Spielauswahl von über 5.000 Titeln von namhaften Spieleanbietern wie NetEnt und Evolution. Das bedeutet nicht, dass sie alle anderen Bereiche vernachlässigen, aber ein Casino kann zum Beispiel für einen guten Kundensupport bekannt sein, aber eine unterdurchschnittliche Anzahl an Casinospielen bieten. Freispiele ergänzen oft den Einzahlungsbonus und bieten zusätzlichen Spielwert an Spielautomaten.
References:
https://s3.amazonaws.com/new-casino/vulkan%20spiele%20casino.html
md.swk-web.com · January 8, 2026 at 1:41 pm
References:
Test prop anavar cycle before and after
References:
https://md.swk-web.com/s/bREmc5RGh
firsturl.de · January 8, 2026 at 1:45 pm
References:
Crown casino accommodation
References:
https://firsturl.de/lL6UnW7
currie-lykke.technetbloggers.de · January 8, 2026 at 2:11 pm
References:
Anavar before and after male
References:
https://currie-lykke.technetbloggers.de/anavar-cycle-guide-2025-dosage-results-side-effects-and-stacks
pad.geolab.space · January 8, 2026 at 2:32 pm
References:
Anavar before and after 1 month woman
References:
https://pad.geolab.space/s/PJNOo1z-C
f1 ao vivo · January 10, 2026 at 3:41 am
Thanks , I have just been searching for info about this subject for ages and yours is the greatest I have found out till now. However, what in regards to the bottom line? Are you certain concerning the supply?
glycomute · January 11, 2026 at 11:51 pm
**glycomute**
glycomute is a natural nutritional formula carefully created to nurture healthy blood sugar levels and support overall metabolic performance.
wildgut · January 12, 2026 at 11:14 am
**wildgut**
wildgut is a precision-crafted nutritional blend designed to nurture your dogs digestive tract.
spree casino app · January 13, 2026 at 4:59 am
Very good information. Lucky me I came across your site by accident (stumbleupon). I have saved as a favorite for later!
888slot · January 14, 2026 at 11:40 am
Chúng tôi trân trọng kính mời quý khách tham quan và trải nghiệm các dịch vụ tại 888slot , nơi đẳng cấp và uy tín được khẳng định qua từng giao dịch. TONY01-14
Lsm99dna · January 21, 2026 at 1:40 pm
When I read your article on this topic, the first thought seems profound and difficult. There is also a bulletin board for discussion of articles and photos similar to this topic on my site, but I would like to visit once when I have time to discuss this topic. login lsm99
gbgbet · January 21, 2026 at 7:08 pm
Nice post. I was checking constantly this blog and I am impressed! Extremely useful info specifically the last part 🙂 I care for such information much. I was seeking this particular info for a very long time. Thank you and good luck.|
gbgbet · January 21, 2026 at 9:42 pm
I don’t know if it’s just me or if perhaps everybody else experiencing problems with your site. It appears like some of the text in your content are running off the screen. Can somebody else please provide feedback and let me know if this is happening to them too? This might be a problem with my browser because I’ve had this happen before. Cheers
downarchive.org · January 21, 2026 at 10:01 pm
References:
Anavar before and after 1 month female
References:
http://downarchive.org/user/targetflat00/
hedge.fachschaft.informatik.uni-kl.de · January 22, 2026 at 1:16 am
immediate effects of steroids
References:
https://hedge.fachschaft.informatik.uni-kl.de/s/YssQLY1KN
av 在线 · January 22, 2026 at 10:47 pm
I do not know if it’s just me or if everybody else encountering problems with your site. It seems like some of the written text on your content are running off the screen. Can somebody else please provide feedback and let me know if this is happening to them as well? This may be a problem with my internet browser because I’ve had this happen before. Many thanks
egamersbox.com · January 23, 2026 at 11:42 pm
References:
Mobile casino
References:
https://egamersbox.com/cool/index.php?page=user&action=pub_profile&id=258005
av 在线 · January 24, 2026 at 2:14 am
For most up-to-date news you have to go to see world wide web and on world-wide-web I found this web site as a finest web page for most up-to-date updates.
mozillabd.science · January 24, 2026 at 8:12 pm
References:
Casino sans telechargement
References:
https://mozillabd.science/wiki/Live_Casino_Deutschland_2026_Die_Top_5_im_Vergleich
https://funsilo.date/ · January 25, 2026 at 5:59 am
References:
Valley view casino center san diego
References:
https://funsilo.date/wiki/96_com_1_Trusted_Online_Casino_Sports_and_Crypto_Betting_Site
http://community.srhtech.net · January 25, 2026 at 7:50 am
References:
Blackjack rules chart
References:
http://community.srhtech.net/user/selectedger82
graph.org · January 25, 2026 at 11:05 am
results and recovery formula alternative
References:
https://graph.org/Stiftung-Warentest-Richtig-abnehmen-diese-Schlankheitsmittel-nicht-verwenden-01-17
https://freebookmarkstore.win/story.php?title=trump-warned-hell-need-to-cough-up-700billion-for-greenland-ahead-of-proposal · January 25, 2026 at 11:11 am
%random_anchor_text%
References:
https://freebookmarkstore.win/story.php?title=trump-warned-hell-need-to-cough-up-700billion-for-greenland-ahead-of-proposal
http://okprint.kz/user/tightsfarmer2/ · January 25, 2026 at 12:38 pm
risks of steroid use
References:
http://okprint.kz/user/tightsfarmer2/
https://www.pradaan.org/members/lookwire6/activity/754687 · January 25, 2026 at 12:59 pm
%random_anchor_text%
References:
https://www.pradaan.org/members/lookwire6/activity/754687/
http://okprint.kz/user/piscescable92/ · January 25, 2026 at 3:24 pm
%random_anchor_text%
References:
http://okprint.kz/user/piscescable92/
https://coolpot.stream/story.php?title=minceur-complements-alimentaires-pour-mincir-et-perdre-du-poids · January 25, 2026 at 3:25 pm
anabolic steroid bodybuilding
References:
https://coolpot.stream/story.php?title=minceur-complements-alimentaires-pour-mincir-et-perdre-du-poids
Bürocontainer · January 25, 2026 at 3:28 pm
Hi, always i used to check weblog posts here early in the break of day, since
i like to gain knowledge of more and more.
日本 av · January 26, 2026 at 3:23 am
Wow, this paragraph is fastidious, my sister is analyzing these kinds of things, so I am going to convey her.
gbgbet · January 26, 2026 at 7:30 am
Hi, I do think this is an excellent website. I stumbledupon it 😉 I will revisit yet again since i have book-marked it. Money and freedom is the best way to change, may you be rich and continue to guide other people.
av 在线 · January 26, 2026 at 12:14 pm
My partner and I stumbled over here different website and thought I might check things out. I like what I see so now i am following you. Look forward to looking into your web page yet again.
pattern-wiki.win · January 26, 2026 at 8:45 pm
References:
Harrington raceway and casino
References:
https://pattern-wiki.win/wiki/Amazon_com_Retro_Vintage_Candy_Security_Ghost_For_Halloween_UnisexAdults_Kids_Black_Short_Sleeve_TShirt_Clothing_Shoes_Jewelry
https://md.un-hack-bar.de · January 26, 2026 at 9:28 pm
References:
Blue rodeo try
References:
https://md.un-hack-bar.de/s/QjXSMZzxY-
nerdgaming.science · January 26, 2026 at 9:39 pm
References:
Fond du luth casino
References:
https://nerdgaming.science/wiki/Online_Engagement_for_Australia
https://chessdatabase.science/wiki/Get_18_Free_Up_to_600_Welcome_Offer · January 27, 2026 at 1:14 am
References:
Real money online pokies
References:
https://chessdatabase.science/wiki/Get_18_Free_Up_to_600_Welcome_Offer
basinmark75.bravejournal.net · January 27, 2026 at 5:45 am
References:
Prairie meadows casino
References:
https://basinmark75.bravejournal.net/rate-candy96
https://pad.karuka.tech/s/1ky5rqU3A · January 27, 2026 at 7:40 am
References:
777 dragon casino
References:
https://pad.karuka.tech/s/1ky5rqU3A
gbgbet · January 27, 2026 at 6:13 pm
This design is spectacular! You most certainly know how to keep a reader amused. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job. I really enjoyed what you had to say, and more than that, how you presented it. Too cool!
b2xbet · January 28, 2026 at 3:06 am
My brother recommended I might like this website. He was totally right. This post truly made my day. You cann’t imagine simply how much time I had spent for this info! Thanks!
b2xbet · January 28, 2026 at 10:54 am
It’s fantastic that you are getting ideas from this paragraph as well as from our argument made at this place.
Binance账户 · January 28, 2026 at 3:02 pm
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
lovebookmark.date · January 28, 2026 at 7:52 pm
where to buy dianabol
References:
https://lovebookmark.date/story.php?title=sanidad-habilita-una-web-de-venta-online-de-farmacos-sin-receta
https://cattletrailers.com.au · January 28, 2026 at 9:23 pm
bulking steroid cycle
References:
https://cattletrailers.com.au/author/foxmaple13/
peatix.com · January 29, 2026 at 1:39 am
best supplements for muscle definition
References:
https://peatix.com/user/28805652
https://matkafasi.com/user/linejoke48 · January 29, 2026 at 2:45 am
bodybuilding dangerous
References:
https://matkafasi.com/user/linejoke48
hi88 · January 29, 2026 at 4:20 am
Hey! Someone in my Myspace group shared this website with us so I came to take a look. I’m definitely enjoying the information. I’m book-marking and will be tweeting this to my followers! Great blog and excellent style and design.
hi88 · January 29, 2026 at 6:33 am
Someone necessarily lend a hand to make seriously articles I’d state. That is the very first time I frequented your web page and up to now? I amazed with the research you made to make this actual post extraordinary. Excellent job!
https://mozillabd.science · January 29, 2026 at 4:01 pm
References:
Casinos las vegas
References:
https://mozillabd.science/wiki/1Go_Casino_berprfung_1GoBewertungen_und_SpielerFeedback
https://md.swk-web.com/s/4SYkqYjl1 · January 30, 2026 at 12:04 am
References:
Native american casinos
References:
https://md.swk-web.com/s/4SYkqYjl1
www.bandsworksconcerts.info · January 30, 2026 at 12:52 pm
memphis casinos
https://theflatearth.win/wiki/Post:Top_10_serise_Online_Casinos_Spielotheken_in_Deutschland_2026 theflatearth.win
http://jobs.emiogp.com/author/spongehouse8/ http://jobs.emiogp.com/author/spongehouse8/
https://yogicentral.science/wiki/1RED_Online_Casino_Deutschland_Offizielle_Seite_9_300_Bonus yogicentral.science
https://funsilo.date/wiki/Casino_Bonus_ohne_Einzahlung_2026 funsilo.date
https://historydb.date/wiki/200_Casino_Bonus_Casinos_mit_200_Bonus_mit_Einzahlung_2026 historydb.date
https://pads.zapf.in/s/65B396zcgA pads.zapf.in
https://ccsakura.jp:443/index.php?treelamb2 ccsakura.jp
https://md.chaosdorf.de/s/VErf0ksk5k https://md.chaosdorf.de/
https://doc.adminforge.de/s/7tw_BkE05O doc.adminforge.de
https://kanban.xsitepool.tu-freiberg.de/s/H1KmhWY8be https://kanban.xsitepool.tu-freiberg.de/
https://dokuwiki.stream/wiki/Bewertungen_zu_24Casino_Lesen_Sie_Kundenbewertungen_zu_24casino_com https://dokuwiki.stream
https://marvelvsdc.faith/wiki/CasinoSpiele_de_ber_1600_Casino_Spiele_kostenlos marvelvsdc.faith
https://www.hulkshare.com/monthplace8/ hulkshare.com
https://md.chaosdorf.de/s/xgQwDnGQsQ https://md.chaosdorf.de/s/xgQwDnGQsQ
https://hedge.fachschaft.informatik.uni-kl.de/s/99yPvJSrPi hedge.fachschaft.informatik.uni-kl.de
https://postheaven.net/lizardorgan9/admiral-casino-online-deutschland-spielauswahl-boni-funktionen-der-mobilen postheaven.net
https://scientific-programs.science/wiki/Online_Casino_Sports_Betting_Poker_Games https://scientific-programs.science/
https://able2know.org/user/lookshop0/ https://able2know.org/
References:
https://www.bandsworksconcerts.info:443/index.php?spikevoice5
hedgedoc.eclair.ec-lyon.fr · January 31, 2026 at 3:50 am
References:
Casino phoenix az
References:
https://hedgedoc.eclair.ec-lyon.fr/s/Uqh02vy71
https://pattern-wiki.win/wiki/100_Freispiele_ohne_Einzahlung_Januar_2026 · January 31, 2026 at 6:16 pm
roulette video
https://swapon.co.in/user/profile/364071 https://swapon.co.in/
https://theflatearth.win/wiki/Post:1RED_Casino_Finde_die_heiesten_Aktionen https://theflatearth.win/wiki/Post:1RED_Casino_Finde_die_heiesten_Aktionen
https://www.google.com.pe/url?q=https://online-spielhallen.de/1go-casino-bonus-codes-ihr-umfassender-leitfaden/ https://www.google.com.pe/
https://clashofcryptos.trade/wiki/Online_Casino_Sports_Betting_Poker_Games clashofcryptos.trade
https://yutoriarukyouikujouken.com:443/index.php?baggrease4 https://yutoriarukyouikujouken.com/
https://dohn-bryant.thoughtlanes.net/1red-casino-promo-codes-boni-and-freispiele-1769813396 https://dohn-bryant.thoughtlanes.net/
https://md.ctdo.de/s/gz7_msSw-8 md.ctdo.de
https://md.un-hack-bar.de/s/FOxZ3ih4B2 https://md.un-hack-bar.de
https://molchanovonews.ru/user/searcheffect8/ molchanovonews.ru
https://wikimapia.org/external_link?url=https://online-spielhallen.de/500-casino-erfahrungen-eine-umfassende-bewertung-aus-spielersicht/ wikimapia.org
https://hahn-bryant-2.hubstack.net/1go-casino-exklusiver-600-bonus-fur-neue-spieler hahn-bryant-2.hubstack.net
https://dokuwiki.stream/wiki/Auszahlungen_an_Spielautomaten_maximieren_888_Casino https://dokuwiki.stream/wiki/Auszahlungen_an_Spielautomaten_maximieren_888_Casino
https://www.bandsworksconcerts.info:443/index.php?gaugenote9 bandsworksconcerts.info
https://bookmarking.stream/story.php?title=888-bingo-deutschland-casino-bonus-ohne-einzahlung-kostenlose-praemien https://bookmarking.stream/story.php?title=888-bingo-deutschland-casino-bonus-ohne-einzahlung-kostenlose-praemien
https://www.google.st/url?q=https://online-spielhallen.de/888casino-mobile-app-ihr-casino-fur-unterwegs/ http://www.google.st
https://empirekino.ru/user/dadgrease2/ https://empirekino.ru/user/dadgrease2
https://able2know.org/user/bracelocust0/ able2know.org
https://pad.stuve.de/s/RCp6zImcO https://pad.stuve.de/
References:
https://pattern-wiki.win/wiki/100_Freispiele_ohne_Einzahlung_Januar_2026
yogicentral.science · February 1, 2026 at 4:43 am
References:
Royal vegas online casino
References:
https://yogicentral.science/wiki/Bonus_2026_Erfahrungen_und_Test
https://iskustva.net/ · February 1, 2026 at 4:56 am
References:
Insurance blackjack
References:
https://iskustva.net/user/marchhub0
australianonlinecasino · February 1, 2026 at 12:20 pm
奇思妙探第二季高清完整官方版,海外华人可免费观看最新热播剧集。
bookmarkstore.download · February 1, 2026 at 2:53 pm
play slots for real money
https://p.mobile9.com/lyrenote3/ p.mobile9.com
https://robertson-cochran-2.thoughtlanes.net/registrieren-888casino https://robertson-cochran-2.thoughtlanes.net/registrieren-888casino
https://maps.google.cat/url?q=https://online-spielhallen.de/1go-casino-auszahlung-dein-umfassender-leitfaden-fur-reibungslose-gewinnauszahlungen/ maps.google.cat
https://images.google.td/url?q=https://online-spielhallen.de/888-casino-aktionscode-ihr-schlussel-zu-exklusiven-vorteilen/ images.google.td
https://www.google.com.co/url?q=https://online-spielhallen.de/1go-casino-login-ihr-tor-zur-spielwelt/ http://www.google.com.co
https://dreevoo.com/profile.php?pid=1030743 https://dreevoo.com
https://securityholes.science/wiki/Kosten_Gebhren_Was_gilt_bei_Auslandsberweisungen securityholes.science
http://premiumdesignsinc.com/forums/user/peonygrease7/ http://premiumdesignsinc.com/forums/user/peonygrease7/
https://www.google.at/url?q=https://online-spielhallen.de/1go-casino-bonus-codes-ihr-umfassender-leitfaden/ https://www.google.at/url?q=https://online-spielhallen.de/1go-casino-bonus-codes-ihr-umfassender-leitfaden
https://maps.google.com.pr/url?q=https://online-spielhallen.de/888-casino-bonus-code-ihr-umfassender-leitfaden-fur-ein-lukratives-spielerlebnis/ https://maps.google.com.pr/url?q=https://online-spielhallen.de/888-casino-bonus-code-ihr-umfassender-leitfaden-fur-ein-lukratives-spielerlebnis/
http://premiumdesignsinc.com/forums/user/poloscent2/ http://premiumdesignsinc.com/forums/user/poloscent2/
https://bookmarkspot.win/story.php?title=admiral-casino-no-deposit-bonus-50-free-spins https://bookmarkspot.win
https://maps.google.cat/url?q=https://online-spielhallen.de/1go-casino-auszahlung-dein-umfassender-leitfaden-fur-reibungslose-gewinnauszahlungen/ https://maps.google.cat
https://telegra.ph/1Red-Erfahrungen-2026-Test–Bewertung-02-01-2 https://telegra.ph/1Red-Erfahrungen-2026-Test–Bewertung-02-01-2
http://humanlove.stream//index.php?title=rohdeparrish2740 humanlove.stream
https://freebookmarkstore.win/story.php?title=casino-bonus-ohne-einzahlung-2026-sofort-startguthaben-erhalten freebookmarkstore.win
https://chessdatabase.science/wiki/So_erhalten_Sie_schnelle_Auszahlungen_in_OnlineCasinos https://chessdatabase.science
https://botdb.win/wiki/Beste_Online_Casinos_mit_Echtgeld_2026_im_Test https://botdb.win/wiki/Beste_Online_Casinos_mit_Echtgeld_2026_im_Test
References:
https://bookmarkstore.download/story.php?title=mit-admiral-gutschein-code-15-bonus-abstauben
intensedebate.com · February 2, 2026 at 2:28 am
References:
Wms slots online
References:
https://intensedebate.com/people/ocelotknife15
onlinecasinoau · February 2, 2026 at 2:51 am
ISL live score today, Indian Super League matches with ball-by-ball updates and stats
https://chessdatabase.science/wiki/Best_PayID_Casinos_in_Australia_2025_Withdrawal_Deposits · February 2, 2026 at 1:22 pm
monkey quest games
https://www.google.co.zm/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ https://www.google.co.zm/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/
http://premiumdesignsinc.com/forums/user/ocelotbike02/ premiumdesignsinc.com
https://marvelvsdc.faith/wiki/Best_PayID_Casino_2025_Top_Online_Casinos_With_PayID https://marvelvsdc.faith/wiki/Best_PayID_Casino_2025_Top_Online_Casinos_With_PayID
https://trade-britanica.trade/wiki/Top_Instant_Withdrawal_Casino_Australia_2025_Fast_Payouts_PayID https://trade-britanica.trade/
https://prpack.ru/user/canwriter35/ https://prpack.ru/
http://lideritv.ge/user/augustknife23/ lideritv.ge
https://www.24propertyinspain.com/user/profile/1367236 https://www.24propertyinspain.com/user/profile/1367236
https://www.24propertyinspain.com/user/profile/1367177 https://www.24propertyinspain.com/
https://clashofcryptos.trade/wiki/Best_PayID_Casinos_in_Australia_Top_10_Aussie_Casino_Sites_with_PayID_Withdrawals_2024 clashofcryptos.trade
https://onlinevetjobs.com/author/fogspring58/ https://onlinevetjobs.com
https://escatter11.fullerton.edu/nfs/show_user.php?userid=9553349 https://escatter11.fullerton.edu
https://may22.ru/user/ocelotcoach53/ may22.ru
https://intensedebate.com/people/latexjelly36 https://intensedebate.com/people/latexjelly36
http://karayaz.ru/user/browrate40/ karayaz.ru
https://www.24propertyinspain.com/user/profile/1367081 https://www.24propertyinspain.com/user/profile/1367081
https://aryba.kg/user/blueliquid58/ aryba.kg
https://humanlove.stream/wiki/How_to_Start_Playing_at_Trusted_Bitcoin_Online_Casinos https://humanlove.stream
https://humanlove.stream/wiki/Online_Casinos_Accepting_PayID_Deposit https://humanlove.stream/
References:
https://chessdatabase.science/wiki/Best_PayID_Casinos_in_Australia_2025_Withdrawal_Deposits
https://bandori.party/ · February 2, 2026 at 2:07 pm
References:
San pablo lytton casino
References:
https://bandori.party/user/398041/swimspleen70/
swaay.com · February 2, 2026 at 6:32 pm
no download slots
https://escatter11.fullerton.edu/nfs/show_user.php?userid=9553167 https://escatter11.fullerton.edu/nfs/show_user.php?userid=9553167
https://sciencewiki.science/wiki/Best_PayID_Casinos_Australia_2026 https://sciencewiki.science/wiki/Best_PayID_Casinos_Australia_2026
https://wifidb.science/wiki/Play_Jango_Casino_Sign_Up_Bonus_February_2026_100_Welcome_Bonus_77_Free_Spins https://wifidb.science
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=309086 socialisted.org
https://urlscan.io/result/019c19e3-5dd0-754c-8bc1-b24b258f7a38/ urlscan.io
https://skitterphoto.com/photographers/2200971/wood-eriksson https://skitterphoto.com/
https://escatter11.fullerton.edu/nfs/show_user.php?userid=9553132 https://escatter11.fullerton.edu/nfs/show_user.php?userid=9553132
https://nerdgaming.science/wiki/PayID_Deposits_Withdrawals_at_Australian_Online_Casinos nerdgaming.science
https://peatix.com/user/28832059 peatix.com
https://intensedebate.com/people/bowltent17 intensedebate.com
https://aryba.kg/user/cancrayon52/ https://aryba.kg/
https://mckenna-newell-4.blogbright.net/payid-online-casinos-australia-2026-top-15 mckenna-newell-4.blogbright.net
https://menwiki.men/wiki/PayID_Casino_Best_Australian_Online_Casinos menwiki.men
https://onlinevetjobs.com/author/dreamcolor22/ https://onlinevetjobs.com/author/dreamcolor22
https://skitterphoto.com/photographers/2201316/contreras-shah skitterphoto.com
http://dranus.ru/forums/user/traincolor17/ dranus.ru
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1834763 gaiaathome.eu
https://aryba.kg/user/cloudmargin32/ https://aryba.kg/user/cloudmargin32
References:
https://swaay.com/u/baniusfxjhf65/about/
https://onlinevetjobs.com · February 2, 2026 at 7:49 pm
References:
Holland casino zandvoort
References:
https://onlinevetjobs.com/author/bladekaren21/
https://opensourcebridge.science · February 2, 2026 at 10:55 pm
silverstar casino
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=130930 dubizzle.ca
https://baconjar84.bravejournal.net/winz-casino-review-games-bonus-pros-and-cons baconjar84.bravejournal.net
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=130987 http://dubizzle.ca/
http://dranus.ru/forums/user/flatbakery56/ http://dranus.ru/forums/user/flatbakery56
https://clashofcryptos.trade/wiki/Winz_Casino_Review_What_we_discovered_Updated clashofcryptos.trade
https://www.google.co.bw/url?q=https://www.facebook.com/people/Winz-io-casino/61585762127473/ http://www.google.co.bw
http://premiumdesignsinc.com/forums/user/hemprate28/ http://premiumdesignsinc.com/forums/user/hemprate28
http://dranus.ru/forums/user/copperrate63/ dranus.ru
https://yogaasanas.science/wiki/Winz_Casino_Review_Is_It_Legit_Expert_User_Ratings yogaasanas.science
https://gregersen-zacho.mdwrite.net/winz-casino-review-2024-bitcoin-casino-with-signup-bonus-and-free-spins gregersen-zacho.mdwrite.net
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1835086 gaiaathome.eu
https://trade-britanica.trade/wiki/Discover_Free_Spins_Bonuses_in_Australia trade-britanica.trade
https://pattern-wiki.win/wiki/Top_Online_Slots_Casino_Bonuses pattern-wiki.win
https://menwiki.men/wiki/Well_Be_Right_Back menwiki.men
https://menwiki.men/wiki/Winz_io_Promo_Code_NEWBONUS_20_Free_Bet_plus_up_to_500_Bankroll menwiki.men
https://www.instapaper.com/p/17427060 http://www.instapaper.com
https://dokuwiki.stream/wiki/Malta_Gaming_License_2024_A_Comprehensive_Guide dokuwiki.stream
https://dreevoo.com/profile.php?pid=1037754 dreevoo.com
References:
https://opensourcebridge.science/wiki/Expert_Player_Ratings_2026
tải 188v · February 3, 2026 at 10:00 am
Tại tải 188v , tính minh bạch được đặt lên hàng đầu. Mọi kết quả trò chơi đều được kiểm định bởi các tổ chức độc lập, đảm bảo không có bất kỳ sự can thiệp nào từ hệ thống. TONY02-03
https://telegra.ph/Golden-Canarys-Pokie-Machine-02-02 · February 3, 2026 at 3:16 pm
stack em high
https://morphomics.science/wiki/Best_Online_Casinos_in_Australia_for_Real_Money_in_2026 https://morphomics.science/wiki/Best_Online_Casinos_in_Australia_for_Real_Money_in_2026
https://rentry.co/zctrd8sb https://rentry.co/zctrd8sb
https://skitterphoto.com/photographers/2205946/begum-godfrey skitterphoto.com
https://peatix.com/user/28839424 peatix.com
http://csmouse.com/user/beantrial07/ http://csmouse.com
https://russell-pearson-2.technetbloggers.de/fast-payout-casinos-australia-2026-instant-withdrawal https://russell-pearson-2.technetbloggers.de/fast-payout-casinos-australia-2026-instant-withdrawal
https://moser-lindhardt-5.technetbloggers.de/best-australian-no-deposit-bonus-codes-and-casinos-2026 moser-lindhardt-5.technetbloggers.de
https://urlscan.io/result/019c1fcc-666b-77b9-8376-70706bb5fb3c/ urlscan.io
https://pace-lockhart-2.thoughtlanes.net/9-best-bitcoin-and-crypto-casinos-in-australia-2026 https://pace-lockhart-2.thoughtlanes.net
https://swaay.com/u/ableigvtrrr98/about/ swaay.com
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1836205 gaiaathome.eu
https://securityholes.science/wiki/Progressive_Jackpot_Pokies_Australia_Where_to_Win_Millions_in_2025 https://securityholes.science
https://p.mobile9.com/dancebeat48/ https://p.mobile9.com/
https://www.google.com.pe/url?q=https://s3.amazonaws.com/new-casino/best-online-casinos-australia.html http://www.google.com.pe
http://stroyrem-master.ru/user/dirtvein75/ stroyrem-master.ru
http://king-wifi.win//index.php?title=sullivanmead1185 king-wifi.win
https://aryba.kg/user/detailbat48/ aryba.kg
https://pediascape.science/wiki/No_Deposit_Free_Spins_Deals pediascape.science
References:
https://funsilo.date/wiki/Best_Online_Casino_That_Accepts_Paypal_Top_Australian_Paypal_Casino
https://maps.google.com.pr/ · February 4, 2026 at 12:33 am
winner casino mobile
https://www.udrpsearch.com/user/fogjelly62 http://www.udrpsearch.com
http://downarchive.org/user/pianospring03/ http://downarchive.org
https://mozillabd.science/wiki/Best_Online_Casinos_Accepting_PayID_in_Australia_2026 https://mozillabd.science/wiki/Best_Online_Casinos_Accepting_PayID_in_Australia_2026
http://csmouse.com/user/tiedate91/ http://csmouse.com
https://long-baldwin.hubstack.net/osko-r long-baldwin.hubstack.net
https://graph.org/Best-PayID-Casinos-in-Australia-for-Fast-Deposits–Withdrawals-02-01 graph.org
https://www.udrpsearch.com/user/snowspleen26 http://www.udrpsearch.com
http://jobboard.piasd.org/author/bluespleen09/ jobboard.piasd.org
https://allen-als-3.blogbright.net/top-10-payid-online-casinos-in-australia-for-2025 allen-als-3.blogbright.net
https://chessdatabase.science/wiki/Best_PayID_Casinos_in_Australia_Top_10_Aussie_Casino_Sites_with_PayID_Withdrawals_2024 chessdatabase.science
https://blackburn-deal-4.technetbloggers.de/payid-casinos-australia-2026-instant-withdrawal-pokies https://blackburn-deal-4.technetbloggers.de/
https://www.instapaper.com/p/17425986 http://www.instapaper.com
https://sciencewiki.science/wiki/Best_PayID_Casinos_in_Australia_15_Sites_That_Accept_PayID https://sciencewiki.science/
https://www.udrpsearch.com/user/risebike35 https://www.udrpsearch.com/
https://fakenews.win/wiki/Payidcasinosreviewedfastdepositswithdrawalsforaussies fakenews.win
https://rentry.co/3hawv9er https://rentry.co
https://augustpush20.werite.net/top-payid-casinos-in-2026-online-casinos-accepting-payid augustpush20.werite.net
https://clashofcryptos.trade/wiki/Mgm_Internet_Casino_Bonus_Codes_Australia_Remanso_Bahia clashofcryptos.trade
References:
https://maps.google.com.pr/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/
onlinecasinowithrealcash · February 4, 2026 at 12:55 am
侠之盗高清完整版结合大数据AI分析,海外华人可免费观看最新热播剧集。
morphomics.science · February 4, 2026 at 1:26 am
References:
Tunica mississippi casino
References:
https://morphomics.science/wiki/Best_PayID_Casinos_in_Australia_Withdrawal_Deposits_with_PayID
freebookmarkstore.win · February 5, 2026 at 12:28 pm
what are the advantages and disadvantages of common names
http://premiumdesignsinc.com/forums/user/dryicicle33/ premiumdesignsinc.com
http://jobs.emiogp.com/author/porchheat50/ jobs.emiogp.com
https://www.instapaper.com/p/17436963 http://www.instapaper.com
https://skitterphoto.com/photographers/2214006/fletcher-mcmillan https://skitterphoto.com/photographers/2214006/fletcher-mcmillan
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=136478 dubizzle.ca
https://botdb.win/wiki/Ratgeber_Testosteron_steigern_mit_Heilpflanzen_Krutern_und_Lebensmitteln botdb.win
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.viladeroses.cat/pages/winstrol_pastillas_1.html bbs.pku.edu.cn
https://securityholes.science/wiki/Buy_Clenbuterol_Online_Safely_from_a_Legal_Source securityholes.science
https://menwiki.men/wiki/Top_8_Wege_um_Testosteron_natrlich_zu_steigern_Therapieergebnisse_d menwiki.men
https://pediascape.science/wiki/Winstrol_Anabolic_steroids_Side_Effects_Uses_Dosage_Interactions_Warnings pediascape.science
https://linkagogo.trade/story.php?title=human-growth-hormone-hgh-benefits-risks-and-uses https://linkagogo.trade
https://king-wifi.win/wiki/GERMAN_MEDICO_Anavar_kaufen king-wifi.win
https://mozillabd.science/wiki/How_to_Spot_Fake_Winstrol_Pills mozillabd.science
https://stensgaard-madden-3.mdwrite.net/trenbolone-enanthate-wikipedia https://stensgaard-madden-3.mdwrite.net/trenbolone-enanthate-wikipedia
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=136498 http://dubizzle.ca/
https://welsh-madden-2.blogbright.net/what-does-clenbuterol-do-to-your-body-benefits-and-side-effects welsh-madden-2.blogbright.net
https://bookmarking.win/story.php?title=cycling-dianabol-dbol-the-ultimate-guide-to-a-safe-and-effective-di bookmarking.win
https://justbookmark.win/story.php?title=what-is-dianabol-is-it-legal https://justbookmark.win/
References:
https://freebookmarkstore.win/story.php?title=here-is-why-jesus-is-trending-on-twitter-and-whatsapp-dklassgh-com
https://pad.stuve.uni-ulm.de/s/h2WI2fWUaG · February 5, 2026 at 3:14 pm
pros and cons of testosterone injections for bodybuilding
References:
https://pad.stuve.uni-ulm.de/s/h2WI2fWUaG
Matthewfum · February 7, 2026 at 6:39 am
phontechm
king-wifi.win · February 7, 2026 at 10:03 am
substitutes for prednisone
https://wikimapia.org/external_link?url=https://gamo-smeo.com/portadas/?hgh_kopen_1.html wikimapia.org
https://wikimapia.org/external_link?url=https://www.viladeroses.cat/pages/winstrol_pastillas_1.html wikimapia.org
https://pediascape.science/wiki/Stanozolol_Wikipedia https://pediascape.science
https://hahn-buur.mdwrite.net/7-best-sites-to-buy-testosterone-online-in-2026 hahn-buur.mdwrite.net
https://hikvisiondb.webcam/wiki/Buy_Genotropin_Norditropin_Steroids_Online hikvisiondb.webcam
https://bom.so/rM1f4L bom.so
https://imoodle.win/wiki/How_to_Get_HGH_Everything_You_Need_to_Know imoodle.win
https://pattern-wiki.win/wiki/Premium_Brands_Peptides pattern-wiki.win
http://mozillabd.science/index.php?title=godwinthomsen6031 mozillabd.science
https://lamont-kamp-2.federatedjournals.com/clenbuterol-online-in-deutschland-bestellen lamont-kamp-2.federatedjournals.com
https://justbookmark.win/story.php?title=growth-hormone-therapy-norditropin-somatropin-10-mg-injection justbookmark.win
https://bookmarkfeeds.stream/story.php?title=testosterone-enanthate-powder-bulk-gmp-supply bookmarkfeeds.stream
https://marvelvsdc.faith/wiki/Clenbuterol_Achat_en_Ligne_Acheter_Clenbuterol_Sopharma_100_mg_0_02_mg marvelvsdc.faith
https://www.udrpsearch.com/user/silicabeech72 http://www.udrpsearch.com
http://pattern-wiki.win/index.php?title=howelynge1536 pattern-wiki.win
https://elearnportal.science/wiki/Testosterone_Coupons_from_32_61_Free_Discount_Savings_Card elearnportal.science
http://jobs.emiogp.com/author/georgedrop47/ jobs.emiogp.com
http://ezproxy.cityu.edu.hk/login?url=https://tanztheater-erfurt.de/wp-content/pgs/appetitz_gler_1.html http://ezproxy.cityu.edu.hk/login?url=https://tanztheater-erfurt.de/wp-content/pgs/appetitz_gler_1.html
References:
https://king-wifi.win/wiki/Are_Steroids_Legal_in_the_UK_Unraveling_the_Confusion
booker-enemark-2.mdwrite.net · February 7, 2026 at 11:30 am
anabolic pre workout
References:
https://booker-enemark-2.mdwrite.net/winstrol-stanozolol-online-kaufen-1770242735
ezproxy.cityu.edu.hk · February 7, 2026 at 3:27 pm
older bodybuilders natural
References:
http://ezproxy.cityu.edu.hk/login?url=https://ecro.fr/images/pgs/?achat_hormone_de_croissance.html
skycrowncasinoonline · February 7, 2026 at 6:00 pm
Crypto Pokies Australia Real Money Real Quiet Fortunes Built
https://barefoot-gates.hubstack.net · February 7, 2026 at 8:22 pm
what is roids
https://p.mobile9.com/menugallon5/ p.mobile9.com
http://king-wifi.win//index.php?title=jacksonsharp8739 http://king-wifi.win//index.php?title=jacksonsharp8739
https://saveyoursite.date/story.php?title=where-to-buy-clenbuterol-online-legally-and-safely https://saveyoursite.date/
http://jobboard.piasd.org/author/ricehand1/ http://jobboard.piasd.org/author/ricehand1
https://www.24propertyinspain.com/user/profile/1369994 http://www.24propertyinspain.com
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://suntana.com/art/?buy_hgh_37.html bbs.pku.edu.cn
https://mozillabd.science/wiki/Trenbolone_Cycle_Guide_Stacks_and_Dosages_for_Bulking_and_Cutting mozillabd.science
https://www.udrpsearch.com/user/cutsheep3 https://www.udrpsearch.com/
https://opensourcebridge.science/wiki/Winstrol_Use_in_Bodybuilding_Guide_to_Dosage_Benefits_Risks_and_Where_to_Buy opensourcebridge.science
https://wifidb.science/wiki/Testosterone_Replacement_Therapy_TRT_Telehealth https://wifidb.science
https://skitterphoto.com/photographers/2216526/madsen-mattingly skitterphoto.com
https://marvelvsdc.faith/wiki/Comprehensive_Guide_to_Legally_Buying_Testosterone_Online_Safe_and_Compliant_Methods marvelvsdc.faith
https://www.instapaper.com/p/17438319 https://www.instapaper.com/
http://king-wifi.win//index.php?title=stanleyestes3857 king-wifi.win
https://justbookmark.win/story.php?title=dianabol-dbol-the-ultimate-guide justbookmark.win
https://cochrane-mcmahon-5.blogbright.net/winstrol-dosierung https://cochrane-mcmahon-5.blogbright.net
https://sciencewiki.science/wiki/Testosterone_Cypionate_Injection sciencewiki.science
https://lovewiki.faith/wiki/Die_Besten_Legalen_Steroide_fr_Muskelaufbau_Ein_Kompletter_Guide https://lovewiki.faith/
References:
https://barefoot-gates.hubstack.net/win-max-legal-winstrol-alternative
dokuwiki.stream · February 7, 2026 at 9:40 pm
casino california
https://gratisafhalen.be/author/dreamframe35/ gratisafhalen.be
https://images.google.com.gt/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ images.google.com.gt
https://peatix.com/user/28832435 peatix.com
https://fakenews.win/wiki/Fast_Payout_Real_Money_Sites https://fakenews.win/wiki/Fast_Payout_Real_Money_Sites
https://opensourcebridge.science/wiki/Best_PayID_Casinos_in_Australia_Withdrawal_Deposits_with_PayID opensourcebridge.science
https://lovewiki.faith/wiki/Fast_Secure_Payments https://lovewiki.faith
https://www.garagesale.es/author/latexred08/ http://www.garagesale.es
https://may22.ru/user/cloudwave89/ may22.ru
https://lovewiki.faith/wiki/Online_Casino_Banking_in_New_Zealand_for_Real_Money lovewiki.faith
https://lovewiki.faith/wiki/Online_Casino_Banking_in_New_Zealand_for_Real_Money lovewiki.faith
https://lospromotores.net/author/risedesk87/ https://lospromotores.net/author/risedesk87
https://sciencewiki.science/wiki/Best_PayID_Casinos_in_Australia_15_Sites_That_Accept_PayID https://sciencewiki.science/wiki/Best_PayID_Casinos_in_Australia_15_Sites_That_Accept_PayID
https://empirekino.ru/user/feastdesk19/ empirekino.ru
https://kirkpatrick-chaney-3.blogbright.net/online-casino-payid-withdrawal-australia-payid-withdrawal-pokies kirkpatrick-chaney-3.blogbright.net
https://noer-werner-3.technetbloggers.de/2025-instant-withdrawals https://noer-werner-3.technetbloggers.de/2025-instant-withdrawals
https://stephansen-talley.mdwrite.net/payid-casinos-australia-for-real-money-with-instant-withdrawal stephansen-talley.mdwrite.net
http://jobboard.piasd.org/author/lierknife46/ http://jobboard.piasd.org
http://downarchive.org/user/cupsarah96/ http://downarchive.org
References:
https://dokuwiki.stream/wiki/Online_Pokies_for_Real_Money_in_Australia_974_ondemand_crowdtesting
https://numberfields.asu.edu · February 7, 2026 at 10:49 pm
rue de richelieu
https://www.udrpsearch.com/user/liercolor24 https://www.udrpsearch.com/
https://www.udrpsearch.com/user/recessrate28 http://www.udrpsearch.com
https://intensedebate.com/people/feastquince29 intensedebate.com
https://skitterphoto.com/photographers/2201081/leach-nedergaard skitterphoto.com
http://downarchive.org/user/bluewave13/ downarchive.org
https://graph.org/Stellar-Spins-Casino-3000-Pokies-Australia-02-01 https://graph.org/Stellar-Spins-Casino-3000-Pokies-Australia-02-01
http://lideritv.ge/user/browknife47/ lideritv.ge
http://king-wifi.win//index.php?title=stokeshagan5224 king-wifi.win
https://ai-db.science/wiki/How_to_Choose_the_Best_PayID_Casino_App_for_Android_Users https://ai-db.science/wiki/How_to_Choose_the_Best_PayID_Casino_App_for_Android_Users
https://intensedebate.com/people/browzebra83 intensedebate.com
https://fakenews.win/wiki/PayID_Betting_Sites_Australia_2026 fakenews.win
https://pattern-wiki.win/wiki/Online_Casinos_Accepting_PayID_Deposit https://pattern-wiki.win/wiki/Online_Casinos_Accepting_PayID_Deposit
http://downarchive.org/user/fogcoach77/ downarchive.org
https://scientific-programs.science/wiki/PayID_Casinos_In_Australia_Secure_Instant_Casino_Payments scientific-programs.science
https://lospromotores.net/author/ocelotcoach58/ https://lospromotores.net
https://may22.ru/user/lierred06/ https://may22.ru/
https://mapleprimes.com/users/riddleframe89 https://mapleprimes.com/users/riddleframe89
https://pattern-wiki.win/wiki/Viper_Spin_Casino_Fast_Withdrawals_Australia pattern-wiki.win
References:
https://numberfields.asu.edu/NumberFields/show_user.php?userid=6497566
https://escatter11.fullerton.edu/ · February 8, 2026 at 12:51 am
roulette wheel
https://marvelvsdc.faith/wiki/Top_VIP_Casino_Programs_in_2026 marvelvsdc.faith
https://skitterphoto.com/photographers/2201537/arsenault-rossi skitterphoto.com
https://skitterphoto.com/photographers/2201420/mckenna-werner skitterphoto.com
https://p.mobile9.com/copypisces21/ https://p.mobile9.com/copypisces21/
https://graph.org/7-Best-PayID-Casinos-with-Instant-Withdrawals-02-01 graph.org
https://yogicentral.science/wiki/Fast_Withdrawal_PayID_casinos_in_Australia_2026 https://yogicentral.science
http://mozillabd.science/index.php?title=sahinpowers8588 mozillabd.science
https://dreevoo.com/profile.php?pid=1035675 https://dreevoo.com
https://peatix.com/user/28832504 peatix.com
https://www.instapaper.com/p/17426400 https://www.instapaper.com/
https://empirekino.ru/user/augustzebra77/ https://empirekino.ru/user/augustzebra77
https://doherty-ritter-2.thoughtlanes.net/aus-real-money-gambling-sites doherty-ritter-2.thoughtlanes.net
http://stroyrem-master.ru/user/cloudbrandy07/ stroyrem-master.ru
https://stephansen-talley.mdwrite.net/payid-casinos-australia-for-real-money-with-instant-withdrawal stephansen-talley.mdwrite.net
https://ai-db.science/wiki/Fast_Secure_Reliable_Pokies_Banking https://ai-db.science
https://stanley-rossi-2.hubstack.net/australian-payid-online-casinos-new-casino-banking-method stanley-rossi-2.hubstack.net
https://maps.google.com.br/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ https://maps.google.com.br/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid
https://www.google.ci/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ https://www.google.ci/
References:
https://escatter11.fullerton.edu/nfs/show_user.php?userid=9553000
peatix.com · February 8, 2026 at 2:03 am
tropicana casino las vegas
https://dreevoo.com/profile.php?pid=1036129 dreevoo.com
https://dreevoo.com/profile.php?pid=1035912 https://dreevoo.com/profile.php?pid=1035912
https://timeoftheworld.date/wiki/Royal_Reels_20_casino_Play_Real_Money_Pokies_Instant_AUD_Payouts timeoftheworld.date
https://swain-baldwin-3.federatedjournals.com/osko-vs-payid-best-aussie-casino-payment-method swain-baldwin-3.federatedjournals.com
https://clashofcryptos.trade/wiki/Best_PayID_Casinos_in_Australia_Top_10_Aussie_Casino_Sites_with_PayID_Withdrawals_2024 https://clashofcryptos.trade/wiki/Best_PayID_Casinos_in_Australia_Top_10_Aussie_Casino_Sites_with_PayID_Withdrawals_2024
https://empirekino.ru/user/pianocase44/ empirekino.ru
https://empirekino.ru/user/augustzebra77/ https://empirekino.ru/
https://onlinevetjobs.com/author/dreamcase21/ onlinevetjobs.com
https://graph.org/PayID-for-High-Rollers-Fast-Private-Casino-Payments-02-01 graph.org
http://jobboard.piasd.org/author/recesszebra87/ jobboard.piasd.org
https://www.google.co.ao/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ http://www.google.co.ao
https://p.mobile9.com/ocelotred75/ p.mobile9.com
https://noer-werner-3.technetbloggers.de/2025-instant-withdrawals noer-werner-3.technetbloggers.de
https://graph.org/Stellar-Spins-Casino-3000-Pokies-Australia-02-01 graph.org
https://intensedebate.com/people/latextent80 intensedebate.com
https://mapleprimes.com/users/clouddate76 mapleprimes.com
https://yogaasanas.science/wiki/Australian_PayID_Casinos_with_AUD https://yogaasanas.science
https://swimknife70.bravejournal.net/using-payid-for-pokies-and-everyday-budgeting-in-australia https://swimknife70.bravejournal.net
References:
https://peatix.com/user/28832151
https://www.fionapremium.com/author/italycrayon65 · February 8, 2026 at 4:50 am
blackjack bomber
http://lideritv.ge/user/earjelly91/ http://lideritv.ge
https://classifieds.ocala-news.com/author/layerframe03 classifieds.ocala-news.com
https://morphomics.science/wiki/Best_PayID_Casinos_in_Australia_for_2026 morphomics.science
https://chessdatabase.science/wiki/Instant_Withdrawal_Casino_Australia_Top_Fast_Payout_Casinos https://chessdatabase.science/wiki/Instant_Withdrawal_Casino_Australia_Top_Fast_Payout_Casinos
https://ondashboard.win/story.php?title=play-pokies-real-money-with-instant-withdrawal ondashboard.win
https://wifidb.science/wiki/Why_PayID_Fits_the_AlwaysOn_Smartphone_Era https://wifidb.science/
https://egamersbox.com/cool/index.php?page=user&action=pub_profile&id=273018 egamersbox.com
https://onlinevetjobs.com/author/porchstove18/ https://onlinevetjobs.com/author/porchstove18/
https://images.google.com.pa/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ images.google.com.pa
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=130064 dubizzle.ca
https://humanlove.stream/wiki/How_to_Start_Playing_at_Trusted_Bitcoin_Online_Casinos https://humanlove.stream
https://lovewiki.faith/wiki/Australian_PayID_Casinos_with_AUD https://lovewiki.faith/wiki/Australian_PayID_Casinos_with_AUD
http://stroyrem-master.ru/user/lierred68/ http://stroyrem-master.ru/
https://may22.ru/user/ocelotcoach53/ https://may22.ru/user/ocelotcoach53/
https://ai-db.science/wiki/How_to_Choose_the_Best_PayID_Casino_App_for_Android_Users https://ai-db.science/wiki/How_to_Choose_the_Best_PayID_Casino_App_for_Android_Users
http://okprint.kz/user/vinylspring48/ okprint.kz
https://imoodle.win/wiki/PayID_Casinos_A_Comprehensive_Guide imoodle.win
https://www.google.pt/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/ https://www.google.pt/
References:
https://www.fionapremium.com/author/italycrayon65/
yogaasanas.science · February 8, 2026 at 8:09 am
References:
Russian roulette game
References:
https://yogaasanas.science/wiki/7_Best_PayID_Casinos_with_Instant_Withdrawals
https://forum.dsapinstitute.org/forums/users/vinylframe42 · February 8, 2026 at 8:47 am
References:
Fantasy casino
References:
https://forum.dsapinstitute.org/forums/users/vinylframe42/
king-wifi.win · February 9, 2026 at 9:33 am
abuse steroid
https://www.youtube.com/redirect?q=https://cerraelx.es/wp-content/pgs/?pastillas_para_adelgazar_1.html https://www.youtube.com
http://historydb.date/index.php?title=lassiterblack4844 historydb.date
https://ai-db.science/wiki/InDepth_Investigation_of_the_Testosterone_Cypionate_Injection_Market_Projected_CAGR_of_14_6_Market_Constraints_and_Growth_Analysis_from_2026_to_2 ai-db.science
https://www.udrpsearch.com/user/kevinhand1 http://www.udrpsearch.com
https://empirekino.ru/user/nutsing8/ https://empirekino.ru/
https://mensvault.men/story.php?title=buy-winstrol-50mg https://mensvault.men/
http://humanlove.stream//index.php?title=bockbengtson0816 humanlove.stream
https://espinoza-gates.mdwrite.net/die-5-besten-testosteron-booster-wissenschaftlich-belegt espinoza-gates.mdwrite.net
http://09vodostok.ru/user/makeupsun0/ 09vodostok.ru
https://scientific-programs.science/wiki/Anavar_Online_Sichere_Kaufpraktiken_fr_Bodybuilder_247_is https://scientific-programs.science
https://www.youtube.com/redirect?q=https://mairie-sornay.fr/articles/dianabol_acheter_en_ligne_2.html https://www.youtube.com/
https://elclasificadomx.com/author/egyptcold1/ elclasificadomx.com
http://jobs.emiogp.com/author/catsupgallon5/ jobs.emiogp.com
https://wifidb.science/wiki/HGH_Prescription_from_a_Doctor_How_to_Get_HGH_Prescribed_Online wifidb.science
https://best-mcmahon-7.technetbloggers.de/testosterone-cypionate-injection best-mcmahon-7.technetbloggers.de
https://p.mobile9.com/catsuphand4/ p.mobile9.com
https://bookmarking.stream/story.php?title=8-ways-to-naturally-increase-testosterone-exercise-diet-sleep bookmarking.stream
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1839480 https://gaiaathome.eu/
References:
http://king-wifi.win//index.php?title=boonebisgaard0819
nerdgaming.science · February 9, 2026 at 10:07 am
prednisone muscle growth
http://jobs.emiogp.com/author/karenletter8/ jobs.emiogp.com
https://hikvisiondb.webcam/wiki/TRT_Uses_Side_Effects_and_Cost_of_Testosterone_Replacement_Therapy hikvisiondb.webcam
https://rentry.co/fafszfsv rentry.co
https://www.instapaper.com/p/17437906 http://www.instapaper.com
http://humanlove.stream//index.php?title=bockbengtson0816 http://humanlove.stream/
http://karayaz.ru/user/spadesing4/ http://karayaz.ru/user/spadesing4
https://forum.dsapinstitute.org/forums/users/golfcirrus1/ forum.dsapinstitute.org
https://graph.org/Winstrol-100-Buy-Online-USA-02-05 https://graph.org/Winstrol-100-Buy-Online-USA-02-05
https://a-taxi.com.ua/user/patchbody6/ a-taxi.com.ua
https://sciencewiki.science/wiki/Testosterone_Cypionate_Injection sciencewiki.science
https://lovewiki.faith/wiki/Wie_steigere_ich_mein_Testosteron_7_Tipps lovewiki.faith
https://sciencewiki.science/wiki/Winstrol_buy_legally_at_best_price_in_UK sciencewiki.science
https://dreevoo.com/profile.php?pid=1057425 dreevoo.com
https://swaay.com/u/bastumwvgbf86/about/ https://swaay.com/
https://hikvisiondb.webcam/wiki/Anavar_kaufen_Sichere_Oxandrolon_Tabletten_online_bestellen hikvisiondb.webcam
https://burris-reece-2.technetbloggers.de/top-13-companies-in-the-global-human-growth-hormone-hgh-market-technavio https://burris-reece-2.technetbloggers.de/top-13-companies-in-the-global-human-growth-hormone-hgh-market-technavio
https://telegra.ph/HGH-Prescription-Learn-How-to-Get-Growth-Hormone-Prescription-Online-02-05 https://telegra.ph/HGH-Prescription-Learn-How-to-Get-Growth-Hormone-Prescription-Online-02-05
https://saveyoursite.date/story.php?title=testosteron-natuerlich-steigern-9-wissenschaftlich-belegte-methoden saveyoursite.date
References:
https://nerdgaming.science/wiki/1_Buy_Steroids_with_Credit_Card_and_PayPal
https://gratisafhalen.be · February 9, 2026 at 11:12 am
legal supplements for muscle growth
https://fyhn-gates.technetbloggers.de/growth-hormone-injection-pen-benefits-dosage-and-how-to-use-hgh-pen https://fyhn-gates.technetbloggers.de/
https://swaay.com/u/onovenbsbar53/about/ swaay.com
http://09vodostok.ru/user/catsupbody1/ 09vodostok.ru
https://clashofcryptos.trade/wiki/How_to_Increase_Testosterone_Naturally_10_Ways clashofcryptos.trade
https://bookmarkingworld.review/story.php?title=winstrol-for-weight-loss-will-it-cut-body-fat-see-how https://bookmarkingworld.review/story.php?title=winstrol-for-weight-loss-will-it-cut-body-fat-see-how
https://empirekino.ru/user/nutsing8/ empirekino.ru
http://stroyrem-master.ru/user/ricelimit3/ stroyrem-master.ru
https://justbookmark.win/story.php?title=improving-low-testosterone-naturally-whole-health-library https://justbookmark.win/
http://jobs.emiogp.com/author/franceletter5/ jobs.emiogp.com
https://rentry.co/uf7xamef rentry.co
https://willard-mcknight.federatedjournals.com/buy-clenbuterol-online-from-verified-and-secure-sources willard-mcknight.federatedjournals.com
https://cochrane-mcmahon-4.blogbright.net/buy-high-quality-research-peptides-fast-next-day-uk-delivery cochrane-mcmahon-4.blogbright.net
https://rentry.co/69pvyapr rentry.co
http://ezproxy.cityu.edu.hk/login?url=https://www.stadt-berga.de/wp-content/pgs/dianabol_kaufen_1.html ezproxy.cityu.edu.hk
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=313615 socialisted.org
https://skitterphoto.com/photographers/2218195/madsen-heller skitterphoto.com
https://intensedebate.com/people/francehand8 https://intensedebate.com/people/francehand8
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://innovate360.pt/pages/comprar_oxandrolona_2.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://innovate360.pt/pages/comprar_oxandrolona_2.html
References:
https://gratisafhalen.be/author/cutbakery8/
graph.org · February 9, 2026 at 11:58 am
anabolic supplement reviews
http://mozillabd.science/index.php?title=wilkinsrasch5518 mozillabd.science
https://mensvault.men/story.php?title=24-best-appetite-suppressants-over-the-counter-in-2026-strongest-otc-weight-loss-pills-to-control-hunger-crav mensvault.men
https://telegra.ph/The-best-testosterone-supplements-and-some-natural-boosters-02-05 https://telegra.ph
https://fakenews.win/wiki/6_best_online_TRT_clinics_in_2026 https://fakenews.win/wiki/6_best_online_TRT_clinics_in_2026
https://prpack.ru/user/pvcsing5/ prpack.ru
https://timeoftheworld.date/wiki/Oxandrolon_Anavar_10_mg_100_tabs timeoftheworld.date
https://sanford-trevino.thoughtlanes.net/testosterone-topical-androgel-testim-and-others-uses-side-effects-interactions-pictures-warnings-and-dosing https://sanford-trevino.thoughtlanes.net
https://urlscan.io/result/019c2cc3-23b5-728b-8515-04c9595b0626/ https://urlscan.io/
https://morphomics.science/wiki/Amazon_com_Jacked_Factory_BurnXT_Clinically_Studied_Fat_Burner_Weight_Loss_Supplement_Appetite_Suppressant_Energy_Booster_with_Acetyl_LCarnitine_Green_Tea_Extract_and_More_60_Natural_Diet_Pills_Health_Household https://morphomics.science/wiki/Amazon_com_Jacked_Factory_BurnXT_Clinically_Studied_Fat_Burner_Weight_Loss_Supplement_Appetite_Suppressant_Energy_Booster_with_Acetyl_LCarnitine_Green_Tea_Extract_and_More_60_Natural_Diet_Pills_Health_Household
https://prpack.ru/user/cutbody7/ prpack.ru
https://socialbookmark.stream/story.php?title=top-10-homeopathic-medicines-for-low-testosterone-levels https://socialbookmark.stream/story.php?title=top-10-homeopathic-medicines-for-low-testosterone-levels
https://www.instapaper.com/p/17437906 http://www.instapaper.com
https://espinoza-workman-2.thoughtlanes.net/5-science-backed-ways-to-increase-testosterone-naturally espinoza-workman-2.thoughtlanes.net
https://rentry.co/kv32ywhs https://rentry.co
https://www.youtube.com/redirect?q=https://paladarplus.es/pgs/comprar_winstrol.html https://www.youtube.com
http://king-wifi.win//index.php?title=curtishassing6270 http://king-wifi.win
https://pattern-wiki.win/wiki/Dianabol_Tablets_Complete_Guide_For_Bodybuilders_On_Price pattern-wiki.win
https://aryba.kg/user/spadecirrus8/ aryba.kg
References:
https://graph.org/Stanozolol-Wikipedia-02-05
urlscan.io · February 9, 2026 at 12:52 pm
bodybuilding form
https://https://urlscan.io/result/019c2c4c-faba-725b-beaa-02b300b78123//result/019c2c70-fd38-71db-9393-dd29de95db4d/ urlscan.io
http://mozillabd.science/index.php?title=kjelleruprosario9829 mozillabd.science
https://barefoot-basse-4.blogbright.net/winstrol-anabolic-steroids-side-effects-uses-dosage-interactions-warnings https://barefoot-basse-4.blogbright.net/winstrol-anabolic-steroids-side-effects-uses-dosage-interactions-warnings
https://bom.so/prelGw https://bom.so
https://morphomics.science/wiki/Stanozolol_50mg_Pills_for_Cutting https://morphomics.science/wiki/Stanozolol_50mg_Pills_for_Cutting
http://premiumdesignsinc.com/forums/user/officepoppy1/ http://premiumdesignsinc.com
http://lideritv.ge/user/paintbody8/ http://lideritv.ge/
https://mozillabd.science/wiki/Buy_Anabolic_Steroids_in_USA_Safely_Legally mozillabd.science
https://dreevoo.com/profile.php?pid=1059242 dreevoo.com
https://swaay.com/u/ashtotpdlnq25/about/ swaay.com
https://onlinevetjobs.com/author/cutsun0/ onlinevetjobs.com
http://downarchive.org/user/kitegallon2/ downarchive.org
https://humanlove.stream/wiki/Lab_Tested_Anabolic_Steroids_USA_Fast_Domestic_Shipping humanlove.stream
https://sonnik.nalench.com/user/pvcsing8/ sonnik.nalench.com
https://pattern-wiki.win/wiki/Dianabol_Erfahrungen_Wirkung_Dosierung_und_Kaufberatung_2025 pattern-wiki.win
https://best-rutledge-4.hubstack.net/winstrol-stanozolol-online-kaufen best-rutledge-4.hubstack.net
https://sanford-kragelund-2.federatedjournals.com/understanding-trenbolone-pricing-how-much-should-you-expect-to-pay sanford-kragelund-2.federatedjournals.com
https://bookmarks4.men/story.php?title=winstrol-100-buy-online-usa https://bookmarks4.men/story.php?title=winstrol-100-buy-online-usa
https://yogicentral.science/ · February 9, 2026 at 3:31 pm
buying testosterone online reviews
References:
https://yogicentral.science/wiki/Free_Testosterone_Levels_by_Age_pg_ml
espinoza-bredahl.technetbloggers.de · February 9, 2026 at 11:32 pm
100 stacks fat
https://sciencewiki.science/wiki/7_best_sites_to_buy_testosterone_online_in_2026 sciencewiki.science
https://rentry.co/q72ycbbq https://rentry.co/q72ycbbq
https://mozillabd.science/wiki/Prescription_Medications_to_Treat_Overweight_Obesity https://mozillabd.science/wiki/Prescription_Medications_to_Treat_Overweight_Obesity
https://a-taxi.com.ua/user/cuttown5/ a-taxi.com.ua
https://sonnik.nalench.com/user/golflibra3/ sonnik.nalench.com
http://historydb.date/index.php?title=crowderwaller7195 historydb.date
https://empirekino.ru/user/spadecamp1/ https://empirekino.ru/user/spadecamp1
https://nerdgaming.science/wiki/1_Buy_Steroids_with_Credit_Card_and_PayPal https://nerdgaming.science/wiki/1_Buy_Steroids_with_Credit_Card_and_PayPal
https://elclasificadomx.com/author/cutgallon7/ elclasificadomx.com
https://king-wifi.win/wiki/Top_7_Injectable_Human_Growth_Hormone_Brands_in_2021 https://king-wifi.win/wiki/Top_7_Injectable_Human_Growth_Hormone_Brands_in_2021
https://wifidb.science/wiki/Kratom_Labortests_Bedeutung_Reinheit_und_Qualitt_sichern https://wifidb.science/
https://chessdatabase.science/wiki/7_Places_to_Buy_Contrave_Online_Guide_Prescription_Drugs_and_Healthcare_Costs_Articles chessdatabase.science
https://a-taxi.com.ua/user/egyptsheep3/ a-taxi.com.ua
https://molchanovonews.ru/user/catsuptown2/ molchanovonews.ru
https://rentry.co/84b6syv9 rentry.co
https://www.youtube.com/redirect?q=https://mairie-sornay.fr/articles/dianabol_acheter_en_ligne_2.html http://www.youtube.com
https://bookmarking.stream/story.php?title=24-best-appetite-suppressants-over-the-counter-in-2026-strongest-otc-weight-loss-pills-to-control-hunger-crav bookmarking.stream
http://okprint.kz/user/hockeylimit9/ okprint.kz
References:
https://espinoza-bredahl.technetbloggers.de/winstrol-stanozolol-online-kaufen-1770280873
gpsites.stream · February 10, 2026 at 12:07 am
muscle building injections
https://swaay.com/u/almodabhoza54/about/ swaay.com
https://forum.dsapinstitute.org/forums/users/cutsun9/ https://forum.dsapinstitute.org/forums/users/cutsun9/
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://kalenborn-scheuern.de/wp-content/pgs/winstrol_kaufen.html https://bbs.pku.edu.cn/
https://urlscan.io/result/019c2c0e-0c22-712f-93b8-6df6508e9447/ urlscan.io
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=313762 socialisted.org
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://tumundobio.es/content/pages/comprar_trembolona.html https://bbs.pku.edu.cn/
https://aryba.kg/user/kiteclub1/ aryba.kg
https://molchanovonews.ru/user/makeupcold1/ https://molchanovonews.ru/user/makeupcold1
https://linkagogo.trade/story.php?title=global-human-growth-hormone-hgh-companies-top-company-list linkagogo.trade
https://humanlove.stream/wiki/DHL_Sendungsverfolgung_den_Status_Ihrer_Pakete_verfolgen humanlove.stream
https://grady-kragelund-6.mdwrite.net/identification-of-trenbolone-metabolites-using-hydrogen-isotope-ratio-mass-spectrometry-and-liquid-chromatography-high-accuracy-high-resolution-mass-spectrometry-for-doping-control-anal https://grady-kragelund-6.mdwrite.net
https://pediascape.science/wiki/Anavar_25mg_50_tabs_Buy_Online_USA pediascape.science
https://funsilo.date/wiki/7_Places_to_Buy_Contrave_Online_Guide_Prescription_Drugs_and_Healthcare_Costs_Articles funsilo.date
https://best-mcmahon-7.technetbloggers.de/testosterone-cypionate-injection best-mcmahon-7.technetbloggers.de
https://swaay.com/u/urutiurhglj71/about/ swaay.com
https://firsturl.de/6U2Y0B8 firsturl.de
https://urlscan.io/result/019c2c70-fd38-71db-9393-dd29de95db4d/ https://urlscan.io/result/019c2c70-fd38-71db-9393-dd29de95db4d
https://bookmarkzones.trade/story.php?title=12-over-the-counter-appetite-suppressants-reviewed-4 bookmarkzones.trade
References:
https://gpsites.stream/story.php?title=insurance-financing-options-for-hormone-therapy
binance алдым-ау · February 10, 2026 at 12:27 am
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
https://wifidb.science/wiki/Trenbolone_Complete_Guide_to_Cycles_Dosage_Results_Tren_2025 · February 10, 2026 at 12:35 am
pro muscle 100 shredded stack
http://okprint.kz/user/pvcdonna5/ okprint.kz
https://www.udrpsearch.com/user/toothveil6 https://www.udrpsearch.com/user/toothveil6
https://mckenna-gates-3.blogbright.net/nonprescription-steroids-on-the-internet mckenna-gates-3.blogbright.net
https://p.mobile9.com/makeupsheep3/ p.mobile9.com
https://dokuwiki.stream/wiki/Top_7_Injectable_Human_Growth_Hormone_Brands_in_2021 dokuwiki.stream
http://jobboard.piasd.org/author/patchiron6/ jobboard.piasd.org
http://jobs.emiogp.com/author/franceletter5/ http://jobs.emiogp.com/
http://downarchive.org/user/beautysled2/ http://downarchive.org/
https://classifieds.ocala-news.com/author/egyptcicada7 classifieds.ocala-news.com
https://lovebookmark.date/story.php?title=human-growth-hormone-prescriptions-expert-hgh-doctors lovebookmark.date
https://graph.org/Dianabol-Buying-Guide-Tips-Dosage-Where-to-Buy-02-05 graph.org
https://bookmarkstore.download/story.php?title=buy-hgh-online-human-growth-hormone-hgh-for-sale bookmarkstore.download
http://hikvisiondb.webcam/index.php?title=klinepappas8876 hikvisiondb.webcam
https://forum.dsapinstitute.org/forums/users/cutsun9/ forum.dsapinstitute.org
https://humanlove.stream/wiki/Dianabol_Bodybuilding_Supplement_and_Anabolic_Agent https://humanlove.stream/wiki/Dianabol_Bodybuilding_Supplement_and_Anabolic_Agent
https://jacobsen-sandberg-2.thoughtlanes.net/how-to-choose-a-legit-steroid https://jacobsen-sandberg-2.thoughtlanes.net
https://bookmarkzones.trade/story.php?title=anavar-for-sale-a-comprehensive-guide-to-choosing-quality-products bookmarkzones.trade
https://www.24propertyinspain.com/user/profile/1369851 http://www.24propertyinspain.com
References:
https://wifidb.science/wiki/Trenbolone_Complete_Guide_to_Cycles_Dosage_Results_Tren_2025
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=137865 · February 10, 2026 at 1:04 am
anadrol pre workout
http://jobboard.piasd.org/author/kitegallon8/ jobboard.piasd.org
https://sonnik.nalench.com/user/menutown6/ sonnik.nalench.com
https://opensourcebridge.science/wiki/HGH_Therapy_Clinic_Online_Prescription_via_Telemedicine https://opensourcebridge.science/wiki/HGH_Therapy_Clinic_Online_Prescription_via_Telemedicine
https://pattern-wiki.win/wiki/Buy_Winstrol_Online_Your_Ultimate_Guide_to_Safe_Purchasing pattern-wiki.win
http://humanlove.stream//index.php?title=clancyadair4169 humanlove.stream
https://freebookmarkstore.win/story.php?title=clenbuterol-kaufen-online-preis-september-2025 https://freebookmarkstore.win/story.php?title=clenbuterol-kaufen-online-preis-september-2025
https://scientific-programs.science/wiki/Kaufen_Online_Winstrol_10mg_Stanozolol https://scientific-programs.science
https://yogicentral.science/wiki/Trenbolone_Vs_Dianabol_Comparing_Benefits_Risks_and_Results https://yogicentral.science/wiki/Trenbolone_Vs_Dianabol_Comparing_Benefits_Risks_and_Results
https://wikimapia.org/external_link?url=https://www.neukoelln-online.de/include/pages/testosteron_steigern_tabletten_2.html https://wikimapia.org/external_link?url=https://www.neukoelln-online.de/include/pages/testosteron_steigern_tabletten_2.html
https://funsilo.date/wiki/Kann_ich_in_der_Apotheke_auch_ohne_Rezept_Medikamente_bekommen funsilo.date
https://www.udrpsearch.com/user/hockeysing4 http://www.udrpsearch.com
https://skitterphoto.com/photographers/2217692/myrick-sandberg https://skitterphoto.com/
https://linkvault.win/story.php?title=where-are-steroids-legal linkvault.win
https://bookmarking.win/story.php?title=how-do-appetite-suppressants-work-science-explained-simply bookmarking.win
https://lovewiki.faith/wiki/Trusted_Pharmacy_to_Buy_Vicodin_Get_Without_Prescription_www_twelveoaksbrownsvillecom lovewiki.faith
https://gpsites.win/story.php?title=clenbuterol-online-in-deutschland-bestellen-9 gpsites.win
http://jobs.emiogp.com/author/riceveil4/ http://jobs.emiogp.com/author/riceveil4/
https://king-wifi.win/wiki/8_Methoden_Testosteron_natrlich_zu_steigern king-wifi.win
References:
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=137865
https://bookmarkzones.trade/story.php?title=12-over-the-counter-appetite-suppressants-reviewed · February 10, 2026 at 1:44 am
how to make anabolic steroids
https://www.udrpsearch.com/user/cutsun2 http://www.udrpsearch.com
https://p.mobile9.com/butanecap3/ https://p.mobile9.com/butanecap3/
https://king-wifi.win/wiki/Legal_Steroids_What_Works_What_Doesnt_Precautions_Alternatives king-wifi.win
https://lovebookmark.date/story.php?title=testosterone-replacement-therapy-trt-online lovebookmark.date
https://bom.so/HGuxHp bom.so
https://espinoza-reece-3.hubstack.net/naltrexone-bupropion-wikipedia https://espinoza-reece-3.hubstack.net/
https://myrick-atkins-3.mdwrite.net/clenbuterol-gunstig-online-bestellen-ohne-rezept https://myrick-atkins-3.mdwrite.net/clenbuterol-gunstig-online-bestellen-ohne-rezept
https://skitterphoto.com/photographers/2217402/egeberg-rutledge https://skitterphoto.com/photographers/2217402/egeberg-rutledge
https://sanford-heller.hubstack.net/clenbuterol-tabletten-0-02-mg-jetzt-kaufen https://sanford-heller.hubstack.net/clenbuterol-tabletten-0-02-mg-jetzt-kaufen
https://king-bookmark.stream/story.php?title=8-methoden-testosteron-natuerlich-zu-steigern https://king-bookmark.stream/story.php?title=8-methoden-testosteron-natuerlich-zu-steigern
https://www.udrpsearch.com/user/cutsun2 https://www.udrpsearch.com
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1839484 gaiaathome.eu
https://trade-britanica.trade/wiki/Buy_Winstrol_Oral_Stanozolol_50_Mg_Online_Legal_Anabolic_steroids_in_USA trade-britanica.trade
https://urlscan.io/result/019c2d02-6cca-7270-b696-207d644ced8b/ https://urlscan.io/result/019c2d02-6cca-7270-b696-207d644ced8b
https://cochrane-tolstrup-3.technetbloggers.de/anavar-before-and-after-results cochrane-tolstrup-3.technetbloggers.de
https://menwiki.men/wiki/30_Lebensmittel_die_den_Testosteronspiegel_erhhen_100_Natrlich https://menwiki.men
http://lideritv.ge/user/ricesheep4/ lideritv.ge
http://ezproxy.cityu.edu.hk/login?url=https://gastouderbureauheuvelrug.nl/wp-content/pages/testosteron_pillen.html http://ezproxy.cityu.edu.hk/
References:
https://bookmarkzones.trade/story.php?title=12-over-the-counter-appetite-suppressants-reviewed
p.mobile9.com · February 10, 2026 at 2:34 am
best legal testosterone steroid
https://sonnik.nalench.com/user/beetlecap8/ https://sonnik.nalench.com/
https://jacobsen-sandberg-2.thoughtlanes.net/how-to-choose-a-legit-steroid jacobsen-sandberg-2.thoughtlanes.net
https://www.youtube.com/redirect?q=https://www.leristrutturazioni.it/art/acquistare_clenbuterolo_1.html http://www.youtube.com
https://elclasificadomx.com/author/cutgallon7/ elclasificadomx.com
https://imoodle.win/wiki/Buy_Dianabol_Raw_Powder_Pure_Methandrostenolone_Bulk_Supply imoodle.win
https://trade-britanica.trade/wiki/Buy_Winstrol_10_mg_Stanozolol_Oral_Tablets_by_Dragon_Pharma trade-britanica.trade
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1839324 gaiaathome.eu
https://vega-schmidt-3.federatedjournals.com/legal-steroids-do-they-exist-and-do-they-work vega-schmidt-3.federatedjournals.com
https://coolpot.stream/story.php?title=anavar-bewertungen-ein-interview-mit-einem-echten-anavar-benutzer coolpot.stream
https://pattern-wiki.win/wiki/Testosterone_Gel_Uses_Side_Effects pattern-wiki.win
http://09vodostok.ru/user/karenbakery3/ http://09vodostok.ru
https://lovebookmark.win/story.php?title=dianabol-20mg-50-tablets lovebookmark.win
https://freebookmarkstore.win/story.php?title=clenbuterol-kaufen-online-preis-september-2025 freebookmarkstore.win
https://molchanovonews.ru/user/catsuptown2/ molchanovonews.ru
http://hikvisiondb.webcam/index.php?title=klinepappas8876 hikvisiondb.webcam
https://lovewiki.faith/wiki/Testosterone_Topical_Cream lovewiki.faith
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=137645 dubizzle.ca
https://dokuwiki.stream/wiki/Testosteron_legal_aus_der_Apotheke_so_funktioniert_es_wirklich https://dokuwiki.stream
References:
https://p.mobile9.com/paintcicada3/
shepard-emborg-2.hubstack.net · February 10, 2026 at 12:51 pm
steroids usa
References:
shepard-emborg-2.hubstack.net
hikvisiondb.webcam · February 10, 2026 at 4:57 pm
legal prohormones that work
https://rice-zacho-2.technetbloggers.de/dianabol-erfahrungen-wirkung-dosierung-und-kaufberatung-2025-1770291326 rice-zacho-2.technetbloggers.de
https://classifieds.ocala-news.com/author/sofahell7 classifieds.ocala-news.com
http://ezproxy.cityu.edu.hk/login?url=https://ecro.fr/images/pgs/?achat_hormone_de_croissance.html ezproxy.cityu.edu.hk
https://hyllested-thestrup-2.hubstack.net/risks-of-illegal-testosterone https://hyllested-thestrup-2.hubstack.net/risks-of-illegal-testosterone
https://www.youtube.com/redirect?q=https://ezdirect.it/img/pgs/farmaco_per_dimagrire.html https://www.youtube.com/redirect?q=https://ezdirect.it/img/pgs/farmaco_per_dimagrire.html
https://ondashboard.win/story.php?title=clenbuterol-wikipedia-8 https://ondashboard.win/story.php?title=clenbuterol-wikipedia-8
http://jobboard.piasd.org/author/linenlyric3/ jobboard.piasd.org
https://sonnik.nalench.com/user/linenlift7/ sonnik.nalench.com
https://p.mobile9.com/editorbaby6/ p.mobile9.com
https://elearnportal.science/wiki/8_Natural_Appetite_Suppressants_for_Weight_Management https://elearnportal.science/wiki/8_Natural_Appetite_Suppressants_for_Weight_Management
https://funsilo.date/wiki/Site_is_undergoing_maintenance funsilo.date
https://dudley-kearney-2.federatedjournals.com/stanozolol-oral-liquid dudley-kearney-2.federatedjournals.com
https://grady-mcintosh-4.blogbright.net/buy-clenbuterol-online-trusted-quality-from-certified-providers grady-mcintosh-4.blogbright.net
https://dokuwiki.stream/wiki/7_Places_to_Buy_Contrave_Online_Guide_Prescription_Drugs_and_Healthcare_Costs_Articles dokuwiki.stream
https://mensvault.men/story.php?title=usa-pharmacy-tech-certified-sams-part-time-walmart-anitab-org-job-board https://mensvault.men/story.php?title=usa-pharmacy-tech-certified-sams-part-time-walmart-anitab-org-job-board
https://hyllested-carson.technetbloggers.de/appetite-suppressants-what-they-are-types-and-effectiveness https://hyllested-carson.technetbloggers.de
https://gpsites.stream/story.php?title=anavar-10-odin-pharmaceuticals-edullisesti-helsinki-kaikki-tuotteet-sertifioituja gpsites.stream
https://gardner-thygesen-2.technetbloggers.de/looking-for-anavar-for-sale-in-usa-here-is-the-list-of-top-brands-to-consider-in-2024 gardner-thygesen-2.technetbloggers.de
References:
http://hikvisiondb.webcam/index.php?title=skovbjergals0095
www.youtube.com · February 10, 2026 at 10:45 pm
how long does it take to get over steroid withdrawal?
References:
https://www.youtube.com/redirect?q=https://www.autobazar.eu/images/pages/?comprar_hgh_5.html
gbgbet · February 10, 2026 at 11:27 pm
I was recommended this blog by my cousin. I am not sure whether this post is written by him as nobody else know such detailed about my problem. You’re amazing! Thanks!
國產 av · February 11, 2026 at 5:40 am
With havin so much content do you ever run into any issues of plagorism or copyright violation? My website has a lot of completely unique content I’ve either created myself or outsourced but it appears a lot of it is popping it up all over the internet without my agreement. Do you know any solutions to help stop content from being ripped off? I’d really appreciate it.
https://www.udrpsearch.com/ · February 11, 2026 at 3:49 pm
steroids for mass
References:
https://www.udrpsearch.com/user/flaghockey4
https://bookmarks4.men/ · February 11, 2026 at 9:33 pm
pills to gain muscle fast
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://bodegascrial.es/pags/?trembolona_comprar_2.html bbs.pku.edu.cn
https://rentry.co/r3ukyqd5 rentry.co
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.verletzten-kinderseelen-helfen.de/articles/abnehmen_tabletten_1.html bbs.pku.edu.cn
https://molchanovonews.ru/user/earcreek1/ molchanovonews.ru
https://wikimapia.org/external_link?url=https://g-r-s.fr/pag/augmenter_les_testosterones_1.html wikimapia.org
https://funsilo.date/wiki/Trenbolone_effet_cure_et_alternative_lactate_trenbolone funsilo.date
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840028 https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840028
https://swaay.com/u/sklodoxryuc92/about/ swaay.com
https://timeoftheworld.date/wiki/Where_Can_I_Buy_Tren_Safe_Online_and_Local_Options https://timeoftheworld.date/wiki/Where_Can_I_Buy_Tren_Safe_Online_and_Local_Options
https://mack-mcclain-2.hubstack.net/acheter-hgh-somatropine-hormone-de-croissance-humaine-100-ui-prix-225-00-euro-en-ligne-en-france-1770313554 mack-mcclain-2.hubstack.net
http://ezproxy.cityu.edu.hk/login?url=https://fairhuurvoorverhuurders.nl/media/pgs/?testosteron_verhogen_2.html ezproxy.cityu.edu.hk
https://asmussen-marcus-2.mdwrite.net/oxandrolona-10-mg-comprar-esteroides-anabolicos-espana-farmacia-en-linea-1770308914 https://asmussen-marcus-2.mdwrite.net
https://a-taxi.com.ua/user/larchcactus5/ a-taxi.com.ua
https://onlinevetjobs.com/author/dancespike3/ https://onlinevetjobs.com/author/dancespike3/
http://premiumdesignsinc.com/forums/user/coursedesire7/ premiumdesignsinc.com
https://bom.so/Kj04ss bom.so
http://lideritv.ge/user/routerflock3/ http://lideritv.ge/
https://carson-mcclain-3.thoughtlanes.net/les-bruleurs-de-graisse-sont-ils-efficaces carson-mcclain-3.thoughtlanes.net
References:
https://bookmarks4.men/story.php?title=trenbolone-1
rentry.co · February 12, 2026 at 12:11 am
gainer springs florida
https://imoodle.win/wiki/Oxandrolona_Balkan_Oxandrolon_10_mg_100_tab imoodle.win
https://skitterphoto.com/photographers/2220085/mcgee-stokholm skitterphoto.com
https://gratisafhalen.be/author/flarerocket6/ gratisafhalen.be
https://opensourcebridge.science/wiki/Anavar_10_for_Sale_by_Dragon_Pharma_Buy_100_Tabs_of_Anavar_10_Oxandrolone https://opensourcebridge.science/wiki/Anavar_10_for_Sale_by_Dragon_Pharma_Buy_100_Tabs_of_Anavar_10_Oxandrolone
http://09vodostok.ru/user/sandband6/ 09vodostok.ru
https://clashofcryptos.trade/wiki/Trenbolone_le_strode_muscl_qui_te_booste clashofcryptos.trade
https://forum.dsapinstitute.org/forums/users/showalley1/ https://forum.dsapinstitute.org/
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://speros.lt/scripts/inc/clenbuterol_dosage_1.html bbs.pku.edu.cn
https://lovewiki.faith/wiki/Achat_Hgh_sans_ordonnance_livraison_rapide https://lovewiki.faith/wiki/Achat_Hgh_sans_ordonnance_livraison_rapide
https://dreevoo.com/profile.php?pid=1062280 https://dreevoo.com/
http://pattern-wiki.win/index.php?title=chasefrisk3297 pattern-wiki.win
http://premiumdesignsinc.com/forums/user/drakespear6/ premiumdesignsinc.com
https://wifidb.science/wiki/Garantie_limite_Guide_de_dpannage_Blue_Rhino_GBT9080L_specs wifidb.science
https://opensourcebridge.science/wiki/Quel_est_le_meilleur_brleur_de_graisse_2025_naturel_et_efficace opensourcebridge.science
https://bom.so/FD7v6s https://bom.so/
https://may22.ru/user/pintcactus2/ may22.ru
http://king-wifi.win//index.php?title=beckmckinnon8374 king-wifi.win
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840166 https://gaiaathome.eu
References:
https://rentry.co/o7dcxzx4
b2xbet · February 12, 2026 at 12:46 am
Definitely believe that which you said. Your favorite justification appeared to be on the net the easiest thing to be aware of. I say to you, I definitely get annoyed while people think about worries that they plainly don’t know about. You managed to hit the nail upon the top as well as defined out the whole thing without having side-effects , people could take a signal. Will probably be back to get more. Thanks
urlscan.io · February 12, 2026 at 1:06 am
pro bodybuilders supplements
https://dreevoo.com/profile.php?pid=1061803 dreevoo.com
https://historydb.date/wiki/Prcurseur_GH_Stimule_lHormone_de_Croissance https://historydb.date
https://rentry.co/gec534o6 https://rentry.co/gec534o6
https://stout-holmes-3.thoughtlanes.net/anavar-10mg-optimal-cutting-and-strength stout-holmes-3.thoughtlanes.net
https://hoff-lindgreen.hubstack.net/quel-est-le-meilleur-bruleur-de-graisse-pour-les-hommes hoff-lindgreen.hubstack.net
https://birch-lynge.thoughtlanes.net/buy-tren-a-100-made-of-pure-trenbolone-acetate-in-uk-at-gymbodygear-com birch-lynge.thoughtlanes.net
https://avery-chan.mdwrite.net/trenbolone-steroid-what-you-should-know-and-legal-tren-alternatives https://avery-chan.mdwrite.net/
https://botdb.win/wiki/Anavar_50_a_la_Venta_en_anaboles_com_en_Espaa_Oxandrolona_En_lnea https://botdb.win/wiki/Anavar_50_a_la_Venta_en_anaboles_com_en_Espaa_Oxandrolona_En_lnea
https://scientific-programs.science/wiki/Oxandrolone_Tablets https://scientific-programs.science/wiki/Oxandrolone_Tablets
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.fisb.it/media/pages/?acquistare_oxandrolone_anavar_1.html bbs.pku.edu.cn
http://king-wifi.win//index.php?title=beckmckinnon8374 king-wifi.win
https://chessdatabase.science/wiki/Sport_Pour_Maigrir_Femme_Guide_Ultime chessdatabase.science
https://dokuwiki.stream/wiki/Mercado_Livre https://dokuwiki.stream/
http://jobboard.piasd.org/author/radishspear6/ jobboard.piasd.org
https://www.youtube.com/redirect?q=https://frescina.com/art/comprar_hgh_4.html https://www.youtube.com/redirect?q=https://frescina.com/art/comprar_hgh_4.html
https://securityholes.science/wiki/Comprar_XAnavar_Oxandrolona_100_tabletas_x_10_mg_en_lnea_en_Espaa securityholes.science
https://imoodle.win/wiki/ANAVAR_Oxandrolona_100_Tabletas_KIEV_PHARMA https://imoodle.win/wiki/ANAVAR_Oxandrolona_100_Tabletas_KIEV_PHARMA
https://dreevoo.com/profile.php?pid=1063351 https://dreevoo.com/
References:
https://urlscan.io/result/019c2e07-5058-704e-9125-bdfe7eea518d/
https://wikimapia.org · February 12, 2026 at 2:36 am
testosterone vs anabolic steroids
http://premiumdesignsinc.com/forums/user/routerbike4/ http://premiumdesignsinc.com/forums/user/routerbike4
https://pediascape.science/wiki/Les_8_Meilleurs_Brleurs_de_Graisse_2026_Test_et_Avis pediascape.science
https://securityholes.science/wiki/Oxandrolona_10mg_50_tabletas securityholes.science
http://jobboard.piasd.org/author/bufferlink1/ jobboard.piasd.org
https://posteezy.com/bruleur-de-graisse-abdominale-puissant-meilleurs-bruleurs-de-graisse-pour-hommes posteezy.com
http://hikvisiondb.webcam/index.php?title=brinkbeyer1787 hikvisiondb.webcam
https://wikimapia.org/external_link?url=https://hausarzt-in-steglitz.de/wp-content/pgs/clenbuterol_kaufen_3.html/external_link?url=https://ecampania.it/blog/acquistare_oxandrolone_anavar.html https://wikimapia.org/external_link?url=https://ecampania.it/blog/acquistare_oxandrolone_anavar.html
https://www.youtube.com/redirect?q=https://mairie-salaunes.fr/media/pgs/?clenbut_rol_achat_1.html youtube.com
https://mcgee-ellis-2.hubstack.net/les-meilleurs-br-c3-bbleurs-de-graisse-en-2026 https://mcgee-ellis-2.hubstack.net
http://pattern-wiki.win/index.php?title=bildebraswell2844 pattern-wiki.win
https://a-taxi.com.ua/user/coursespring9/ a-taxi.com.ua
https://yogaasanas.science/wiki/Les_meilleurs_brleurs_de_graisse_pour_les_femmes_Les_7_meilleures_pilules_de_perte yogaasanas.science
https://dokuwiki.stream/wiki/Acheter_du_Trenbolone_Injectable_Trenbolone_Injection_en_vente_sur_Lecoq_to https://dokuwiki.stream/wiki/Acheter_du_Trenbolone_Injectable_Trenbolone_Injection_en_vente_sur_Lecoq_to
https://coolpot.stream/story.php?title=new-pharma-oxandrolona coolpot.stream
https://wikimapia.org/external_link?url=https://www.krizia.it/wp-content/pgs/integratore_testosterone.html wikimapia.org
https://dreevoo.com/profile.php?pid=1063398 https://dreevoo.com/profile.php?pid=1063398
http://king-wifi.win//index.php?title=perssonfrantzen7258 king-wifi.win
http://jobboard.piasd.org/author/bufferlink1/ jobboard.piasd.org
historydb.date · February 12, 2026 at 3:17 am
steroids sideaffects
https://humanlove.stream/wiki/Top_brleurs_de_graisse_2026_guide_du_choix_efficace humanlove.stream
https://posteezy.com/meilleur-bruleur-de-graisse-en-2025-lequel-choisir-comparatif-avis-0 https://posteezy.com/meilleur-bruleur-de-graisse-en-2025-lequel-choisir-comparatif-avis-0
http://http://historydb.date/index.php?title=adairhaley6617/index.php?title=padgettladefoged0489 http://historydb.date
https://bom.so/okJXRD bom.so
https://imoodle.win/wiki/OXANDROLONE_10MG_SOLUCIN_ORAL imoodle.win
https://hoff-lindgreen.hubstack.net/quel-est-le-meilleur-bruleur-de-graisse-pour-les-hommes hoff-lindgreen.hubstack.net
https://mack-hickman-2.blogbright.net/oxandrolona-10-mg-50-pastillas-comprar-esteroides-anabolicos-espana-farmacia-en-linea https://mack-hickman-2.blogbright.net/oxandrolona-10-mg-50-pastillas-comprar-esteroides-anabolicos-espana-farmacia-en-linea
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.fisb.it/media/pages/?acquistare_oxandrolone_anavar_1.html bbs.pku.edu.cn
https://bookmarkstore.download/story.php?title=cure-hgh-guide-de-lhormone-de-croissance-humaine-wikistero-la-bible-des-steroides-anabolisants bookmarkstore.download
https://wifidb.science/wiki/CrazyBulk_France_stroide_anabolisant_naturel_Site_officiel https://wifidb.science/wiki/CrazyBulk_France_stroide_anabolisant_naturel_Site_officiel
http://muhaylovakoliba.1gb.ua/user/seederharp5/ muhaylovakoliba.1gb.ua
https://imoodle.win/wiki/Trenbolone imoodle.win
https://menwiki.men/wiki/Comprar_Anavar_10_mg_Esteroides_Anabolicos_Espaa_Farmacia_en_lnea menwiki.men
https://classifieds.ocala-news.com/author/lionlight7 https://classifieds.ocala-news.com/author/lionlight7
https://bom.so/qVZVDv https://bom.so/qVZVDv
https://hoff-ogden.blogbright.net/trenbolone-acetate-100mg-ml-10ml-vial-euro-pharmacies-eu https://hoff-ogden.blogbright.net
https://rentry.co/kw6micpf https://rentry.co
https://blankenship-spivey-2.mdwrite.net/les-meilleurs-br-c3-bbleurs-de-graisse-en-2026 blankenship-spivey-2.mdwrite.net
www.udrpsearch.com · February 12, 2026 at 4:47 am
natural muscle vs steroids
https://sciencewiki.science/wiki/Acheter_Hgh_livraison_rapide_meilleur_prix sciencewiki.science
https://rodriguez-goodwin-2.hubstack.net/les-bruleurs-de-graisse-efficacite-et-guide-complet rodriguez-goodwin-2.hubstack.net
https://sciencewiki.science/wiki/Meilleur_brleur_de_graisse_2025_notre_top_10_expert https://sciencewiki.science/wiki/Meilleur_brleur_de_graisse_2025_notre_top_10_expert
https://funsilo.date/wiki/Trenbolone_effet_cure_et_alternative_lactate_trenbolone https://funsilo.date
https://mozillabd.science/wiki/Vente_de_trenbol_100_MegaGear_strodes_en_France_Sans_ordonnance https://mozillabd.science/wiki/Vente_de_trenbol_100_MegaGear_strodes_en_France_Sans_ordonnance
https://onlinevetjobs.com/author/lookspike4/ onlinevetjobs.com
http://jobs.emiogp.com/author/routeraries1/ jobs.emiogp.com
https://graph.org/OXANDROLONE-BK-PHARMA-10MG-60-TABLETAS-02-05 graph.org
https://marcussen-oconnor.hubstack.net/bruleur-de-graisse-comment-ca-marche-et-lequel-choisir-pour-des-resultats-optimaux marcussen-oconnor.hubstack.net
https://rentry.co/4twbhny8 https://rentry.co/
https://dreevoo.com/profile.php?pid=1063507 dreevoo.com
https://werner-oconnor-2.federatedjournals.com/le-meilleur-br-c3-bbleur-de-graisse-pour-homme-3f-le-top-5 https://werner-oconnor-2.federatedjournals.com/
https://yogicentral.science/wiki/Ce_que_vous_devez_savoir_avant_dacheter_HGH_Achetez_vos_strodes_anabolisants_en_ligne https://yogicentral.science/wiki/Ce_que_vous_devez_savoir_avant_dacheter_HGH_Achetez_vos_strodes_anabolisants_en_ligne
https://imoodle.win/wiki/Trenbolone imoodle.win
https://bom.so/Kj04ss https://bom.so/Kj04ss
https://sonnik.nalench.com/user/leadprofit9/ sonnik.nalench.com
https://stougaard-chan-2.blogbright.net/get-legally-prescribed-hgh-from-a-doctor-obtain-hgh-legally-right-now-1770313364 stougaard-chan-2.blogbright.net
https://sutherland-monroe-2.mdwrite.net/oxandrolone-oxandrolona sutherland-monroe-2.mdwrite.net
References:
https://www.udrpsearch.com/user/cancerspike4
rentry.co · February 12, 2026 at 6:08 am
corticosteroids vs anabolic
https://king-wifi.win/wiki/Oxandrolona_Anavar_Omega_Meds_Anabolic_Aid_for_Muscle_Growth king-wifi.win
https://timeoftheworld.date/wiki/Troubles_de_la_croissance timeoftheworld.date
http://okprint.kz/user/coursealley7/ okprint.kz
https://hikvisiondb.webcam/wiki/Trenbolone_effet_du_Parabolan_cure_dosage_et_avis_pour_la_musculation https://hikvisiondb.webcam/wiki/Trenbolone_effet_du_Parabolan_cure_dosage_et_avis_pour_la_musculation
https://sciencewiki.science/wiki/Trenbolone_le_strode_muscl_qui_te_booste sciencewiki.science
https://onlinevetjobs.com/author/courserocket5/ onlinevetjobs.com
https://king-wifi.win/wiki/Acheter_Prohormone_de_Croissance_HGH https://king-wifi.win/wiki/Acheter_Prohormone_de_Croissance_HGH
https://botdb.win/wiki/Test_brleurs_de_graisse_2021_les_meilleurs_brleurs_de_graisse_en_comparaison https://botdb.win/wiki/Test_brleurs_de_graisse_2021_les_meilleurs_brleurs_de_graisse_en_comparaison
https://williams-luna.thoughtlanes.net/anavar-oxandrolone-buy-tablets-for-sale-online-in-the-uk-us-discover-great-deals-at-steroidstime-com williams-luna.thoughtlanes.net
http://ezproxy.cityu.edu.hk/login?url=https://fairhuurvoorverhuurders.nl/media/pgs/?testosteron_verhogen_2.html ezproxy.cityu.edu.hk
https://stougaard-cherry-2.federatedjournals.com/les-3-vrais-meilleurs-bruleurs-de-graisse-pour-homme-2026 stougaard-cherry-2.federatedjournals.com
https://timeoftheworld.date/wiki/Growth_hormone_past_present_and_future_Nature_Reviews_Endocrinology timeoftheworld.date
https://scientific-programs.science/wiki/Landerlan_Oxandrolona_5mg_100_tabletas https://scientific-programs.science
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.ecoservizindustriali.it/wp-content/pgs/comprare_hgh.html https://bbs.pku.edu.cn
https://rentry.co/gx2tqvm5 https://rentry.co/5i93utbz
https://graph.org/Where-to-Buy-Trenbolone-Safe-Legal–Fast-2026-02-05 https://graph.org/Where-to-Buy-Trenbolone-Safe-Legal–Fast-2026-02-05
https://skitterphoto.com/photographers/2219998/stougaard-mcclain skitterphoto.com
http://karayaz.ru/user/dancevan8/ http://karayaz.ru/user/dancevan8/
pattern-wiki.win · February 12, 2026 at 7:52 am
women taking steroids
https://nerdgaming.science/wiki/LUE_interdit_les_hormones_de_croissance_Actualits_Commission_europenne nerdgaming.science
https://bridges-dencker-3.federatedjournals.com/les-meilleurs-bruleurs-de-graisse-pour-femmes-guide-2026 https://bridges-dencker-3.federatedjournals.com
https://williams-luna.thoughtlanes.net/anavar-oxandrolone-buy-tablets-for-sale-online-in-the-uk-us-discover-great-deals-at-steroidstime-com williams-luna.thoughtlanes.net
https://bom.so/qVZVDv bom.so
http://historydb.date/index.php?title=swansonsecher9038 http://historydb.date/index.php?title=swansonsecher9038
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://g-r-s.fr/pag/augmenter_les_testosterones_1.html https://bbs.pku.edu.cn/
http://ezproxy.cityu.edu.hk/login?url=https://brickobotik.de/wp-content/pgs/winstrol_kaufen_1.html ezproxy.cityu.edu.hk
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://gamo-smeo.com/portadas/?hgh_kopen_1.html bbs.pku.edu.cn
https://funsilo.date/wiki/Changes_Hormones_fminines_base_dstrogne_en_comprims_Amazon_fr_Hygine_et_Sant funsilo.date
https://wikimapia.org/external_link?url=https://cosmedclinic.co.in/blog/pages/eetlustremmers_1.html wikimapia.org
https://king-bookmark.stream/story.php?title=bruleurs-de-graisses-quelles-marques-choisir- king-bookmark.stream
http://hikvisiondb.webcam/index.php?title=jakobsencummings4704 hikvisiondb.webcam
https://bengtsson-lindgreen.blogbright.net/les-8-meilleurs-bruleurs-de-graisse-2026-test-et-avis https://bengtsson-lindgreen.blogbright.net/
https://bookmarkstore.download/story.php?title=oxandrolona-balkan-oxandrolon-10-mg-100-tab-9 https://bookmarkstore.download/
https://menwiki.men/wiki/Vente_de_Trenbolone_Acetate_100mg_UltraPharm_en_France_dans_la_boutique_en_ligne menwiki.men
https://hoff-ellis-3.technetbloggers.de/anavar-oxandrolona-100-tabletas-kiev-pharma hoff-ellis-3.technetbloggers.de
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840083 gaiaathome.eu
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.fisb.it/media/pages/?acquistare_oxandrolone_anavar_1.html bbs.pku.edu.cn
References:
http://pattern-wiki.win/index.php?title=pottskring1354
fakenews.win · February 12, 2026 at 9:48 am
best legal testosterone
https://fanning-ogden-2.mdwrite.net/commander-de-lhgh-injection-de-hgh-en-vente-sur-lecoq-to fanning-ogden-2.mdwrite.net
https://scientific-programs.science/wiki/Oxandrolone_Tablets scientific-programs.science
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1839906 gaiaathome.eu
http://pattern-wiki.win/index.php?title=schultzmcgregor5200 pattern-wiki.win
https://sutherland-monroe-2.mdwrite.net/oxandrolone-oxandrolona https://sutherland-monroe-2.mdwrite.net/oxandrolone-oxandrolona
http://ezproxy.cityu.edu.hk/login?url=https://goals.nl/wp-content/articles/?testosteron_kopen.html ezproxy.cityu.edu.hk
http://ezproxy.cityu.edu.hk/login?url=https://diversionbooks.com/pgs/guide_anavar_for_women.html ezproxy.cityu.edu.hk
http://historydb.date/index.php?title=locklearberger8752 http://historydb.date
http://mozillabd.science/index.php?title=pihlbeyer9015 mozillabd.science
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://akteon.fr/misc/pgs/complement_alimentaire_pour_maigrir_2.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://akteon.fr/misc/pgs/complement_alimentaire_pour_maigrir_2.html
https://nerdgaming.science/wiki/OXANDROLONA_LANDERLAND_5MG nerdgaming.science
https://marvelvsdc.faith/wiki/OXANDROLAND_10MG_e_100_comprimidos marvelvsdc.faith
https://molchanovonews.ru/user/mineadult6/ https://molchanovonews.ru/user/mineadult6/
https://fanning-wade-3.hubstack.net/les-meilleurs-bruleurs-de-graisse-naturels-en-2026 fanning-wade-3.hubstack.net
https://scientific-programs.science/wiki/Top10_Des_Meilleurs_Brleurs_De_Graisse_2026 scientific-programs.science
https://skitterphoto.com/photographers/2220652/stougaard-hickman skitterphoto.com
https://elearnportal.science/wiki/Seringues_100_Pct_Stylo_HGH_Beligasmonde elearnportal.science
https://dreevoo.com/profile.php?pid=1062191 https://dreevoo.com
References:
https://fakenews.win/wiki/Les_Meilleurs_Brleurs_de_Graisse_Naturels_en_2026
winpot · February 12, 2026 at 3:01 pm
Sweet blog! I found it while searching on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Appreciate it
gaiaathome.eu · February 12, 2026 at 11:28 pm
anabolic steroids profiles
References:
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1839933
steele-damsgaard-2.thoughtlanes.net · February 13, 2026 at 1:38 am
bodybuilding drugs list
References:
https://steele-damsgaard-2.thoughtlanes.net/buy-trenbolone-online-in-europe
Lsm99dna · February 13, 2026 at 11:09 am
I will definitely recommend your website to everyone. You have a very good gloss. Write more high-quality articles. I support you. lsm99 เว็บตรง
https://ai-db.science/ · February 13, 2026 at 11:48 am
medical steroid names
https://chessdatabase.science/wiki/Test_brleurs_de_graisse_2021_les_meilleurs_brleurs_de_graisse_en_comparaison chessdatabase.science
https://menwiki.men/wiki/Mercado_Libre menwiki.men
https://elclasificadomx.com/author/brandydraw0/ elclasificadomx.com
https://pope-preston-5.blogbright.net/bruleur-de-graisse-produits-pour-maigrir-parapharmacie-en-ligne pope-preston-5.blogbright.net
https://skitterphoto.com/photographers/2221531/guerrero-copeland skitterphoto.com
https://halvorsen-huang-3.blogbright.net/achat-hgh-sans-ordonnance-livraison-rapide https://halvorsen-huang-3.blogbright.net/achat-hgh-sans-ordonnance-livraison-rapide
https://onlinevetjobs.com/author/kissgrouse1/ onlinevetjobs.com
http://jobs.emiogp.com/author/brandygrouse9/ http://jobs.emiogp.com
https://opensourcebridge.science/wiki/GH_120_caps_Anabolisants_Naturels_Biotech_USA https://opensourcebridge.science/wiki/GH_120_caps_Anabolisants_Naturels_Biotech_USA
https://wifidb.science/wiki/Comment_prparer_un_brleur_de_graisse_naturel wifidb.science
http://downarchive.org/user/peacesushi2/ downarchive.org
https://swaay.com/u/rostafsdkrs44/about/ https://swaay.com/u/rostafsdkrs44/about/
http://king-wifi.win//index.php?title=ulriksenmccullough3326 king-wifi.win
https://klausen-bennetsen.mdwrite.net/oxanbolic-oxandrolona-10mg-50comp-cooper-pharma klausen-bennetsen.mdwrite.net
https://klausen-mccoy-2.hubstack.net/choisir-un-bruleur-de-graisse-efficace-quels-criteres-prendre-en-compte klausen-mccoy-2.hubstack.net
https://p.mobile9.com/cubcheck9/ https://p.mobile9.com/cubcheck9
https://graph.org/Achat-Hgh-pas-cher-sans-ordonnance-02-06 graph.org
https://xypid.win/story.php?title=oxatech-anavar-oxandrolona-omnitech-labs https://xypid.win
References:
https://ai-db.science/wiki/Le_Meilleur_Brleur_De_Graisse_Pour_Homme_Le_Top_5
https://prpack.ru/user/jamhair6 · February 13, 2026 at 12:31 pm
dbol steroids results
https://swaay.com/u/esyldahcfcp79/about/ https://swaay.com
https://may22.ru/user/turnipgrade4/ may22.ru
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.leristrutturazioni.it/art/acquistare_clenbuterolo_1.html bbs.pku.edu.cn
http://historydb.date/index.php?title=tanbishop4260 historydb.date
https://justpin.date/story.php?title=vente-de-trenbolone-a-100-qpharm-steroides-en-france-sans-ordonnance https://justpin.date/story.php?title=vente-de-trenbolone-a-100-qpharm-steroides-en-france-sans-ordonnance
https://skitterphoto.com/photographers/2221618/korsgaard-mccoy https://skitterphoto.com/photographers/2221618/korsgaard-mccoy
https://classifieds.ocala-news.com/author/humornephew7 classifieds.ocala-news.com
https://bom.so/yJtTDm https://bom.so/yJtTDm
https://classifieds.ocala-news.com/author/kisseast1 https://classifieds.ocala-news.com
http://muhaylovakoliba.1gb.ua/user/galleytouch1/ muhaylovakoliba.1gb.ua
https://justbookmark.win/story.php?title=bruleur-de-graisse-comment-ca-marche-et-lequel-choisir-pour-des-resultats-optimaux- justbookmark.win
https://bookmark4you.win/story.php?title=acheter-hgh-pas-cher-meilleur-prix https://bookmark4you.win/story.php?title=acheter-hgh-pas-cher-meilleur-prix
https://www.instapaper.com/p/17440070 http://www.instapaper.com
https://onlinevetjobs.com/author/trampcamp8/ onlinevetjobs.com
https://wifidb.science/wiki/Where_to_Buy_Trenbolone_Acetate_for_Sale_in_the_UK_What_You_Need_to_Know wifidb.science
https://rentry.co/7fqdrq9z rentry.co
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=315791 socialisted.org
https://www.instapaper.com/p/17440296 instapaper.com
References:
https://prpack.ru/user/jamhair6/
lideritv.ge · February 13, 2026 at 1:08 pm
tren vs test
https://morphomics.science/wiki/Oxandrolona https://morphomics.science/wiki/Oxandrolona
https://opensourcebridge.science/wiki/PEN_HGH_Somatropine_Liquide_36_UI_12_mg_3_ml_HILMA https://opensourcebridge.science/wiki/PEN_HGH_Somatropine_Liquide_36_UI_12_mg_3_ml_HILMA
https://graph.org/Trenbolone–Tout-Savoir-sur-ses-Effets-Posologie-et-Dosage-02-06 https://graph.org/
https://timeoftheworld.date/wiki/Acheter_Trenbolone_Acetate_100mg10ml_60_00_Envoi_rapide timeoftheworld.date
http://downarchive.org/user/shelfpanty6/ downarchive.org
https://dreevoo.com/profile.php?pid=1064885 dreevoo.com
https://bom.so/yJtTDm https://bom.so
https://historydb.date/wiki/Achat_Hgh_pas_cher_livraison_rapide historydb.date
https://wiese-copeland-5.federatedjournals.com/meilleur-bruleur-de-graisse-en-2025-lequel-choisir-comparatif-and-avis https://wiese-copeland-5.federatedjournals.com
http://stroyrem-master.ru/user/memorydraw8/ stroyrem-master.ru
https://livebookmark.stream/story.php?title=adelphi-trenbolone-enanthate-200mg livebookmark.stream
https://bookmarkstore.download/story.php?title=acheter-du-trenbolone-injectable-trenbolone-injection-en-vente-sur-lecoq-to bookmarkstore.download
https://skitterphoto.com/photographers/2222049/ortega-mclean skitterphoto.com
https://pediascape.science/wiki/Hormone_de_Croissance_Humaine_HGH_Astera_Labs_HGH_16IU_injections_vendre pediascape.science
http://ezproxy.cityu.edu.hk/login?url=https://paladarplus.es/pgs/comprar_winstrol.html ezproxy.cityu.edu.hk
https://p.mobile9.com/jamrepair5/ p.mobile9.com
https://telegra.ph/Acheter-HgH-Somatropine-Hormone-de-croissance-humaine-100-UI-prix-225-00-Euro-en-ligne-en-France-02-06 telegra.ph
https://wren-mccoy-3.mdwrite.net/anavar-oxandrolona-c-comprar-aqui https://wren-mccoy-3.mdwrite.net/anavar-oxandrolona-c-comprar-aqui
References:
http://lideritv.ge/user/turnipgrade7/
menwiki.men · February 13, 2026 at 2:48 pm
anabolic steroids bodybuilding
https://elclasificadomx.com/author/railrake8/ elclasificadomx.com
https://dreevoo.com/profile.php?pid=1064183 dreevoo.com
https://king-wifi.win/wiki/Bruleur_de_Graisse_Puissant_Formule_Minceur_avec_Guarana_Th_Vert_Konjac_Coupe_Faim_Naturel_Complment_Perte_de_Poids_Cure_de_1_mois_60_Glules_Fabriqu_en_France_Essentials_by_Novoma_Amazon_fr_Hygine_et_Sant king-wifi.win
https://skitterphoto.com/photographers/2221531/guerrero-copeland skitterphoto.com
http://premiumdesignsinc.com/forums/user/brandyspruce2/ premiumdesignsinc.com
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=315925 https://socialisted.org
https://king-wifi.win/wiki/Trenbolone_Enanthate_Benefits_Dosage_Side_Effects_and_Cycle_Guide https://king-wifi.win/wiki/Trenbolone_Enanthate_Benefits_Dosage_Side_Effects_and_Cycle_Guide
http://okprint.kz/user/galleycare9/ http://okprint.kz/
https://urlscan.io/result/019c2faf-b0e9-77c7-8cd0-f33134705cb4/ https://urlscan.io/result/019c2faf-b0e9-77c7-8cd0-f33134705cb4/
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://celiacosmurcia.org/wp-content/pgs/buy_hgh_39.html bbs.pku.edu.cn
http://king-wifi.win//index.php?title=hermankeene5740 http://king-wifi.win//index.php?title=hermankeene5740
https://onlinevetjobs.com/author/memoryplough7/ onlinevetjobs.com
http://semdinlitesisat.eskisehirgocukduzeltme.com/user/peacewine2/ http://semdinlitesisat.eskisehirgocukduzeltme.com/user/peacewine2
https://imoodle.win/wiki/Hormone_de_croissance_ou_strode_lequel_est_meilleur_pour_les_muscles imoodle.win
http://09vodostok.ru/user/israelcelery6/ 09vodostok.ru
https://haas-smidt-4.blogbright.net/achat-hgh-meilleur-prix-livraison-rapide https://haas-smidt-4.blogbright.net/achat-hgh-meilleur-prix-livraison-rapide
https://www.youtube.com/redirect?q=https://dentalcetoday.com/wp-content/pgs/?hgh_kopen_2.html http://www.youtube.com
https://urlscan.io/result/019c3039-1b6d-7250-9845-2365b87d546a/ https://urlscan.io/
References:
https://menwiki.men/wiki/Anavar_10_100tabs_10mg_tab_Omega_Meds
https://yogicentral.science/wiki/Pilules_et_supplments_de_perte_de_poids · February 13, 2026 at 3:58 pm
steriods workout
https://historydb.date/wiki/Acheter_des_brlures_de_graisse_thermognique_naturelles_HSN historydb.date
https://www.instapaper.com/p/17440485 http://www.instapaper.com
https://www.instapaper.com/p/17440507 http://www.instapaper.com
https://telegra.ph/Tout-ce-que-vous-devez-savoir-sur-Trenbolone-02-05 https://telegra.ph/Tout-ce-que-vous-devez-savoir-sur-Trenbolone-02-05
https://telegra.ph/NGENLA–nouvelle-hormone-de-croissance-en-injection-hebdomadaire-02-05 telegra.ph
https://mozillabd.science/wiki/Oxandrolona_Cygnus_Oxandrolone_10_mg_50_tab https://mozillabd.science/wiki/Oxandrolona_Cygnus_Oxandrolone_10_mg_50_tab
https://nerdgaming.science/wiki/Achat_Hgh_livraison_rapide_meilleur_prix nerdgaming.science
http://pattern-wiki.win/index.php?title=finneganlittle6755 pattern-wiki.win
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840537 https://gaiaathome.eu
https://sweet-mason.mdwrite.net/achetez-hgh-and-peptides-hilma-biocare-en-ligne-en-france sweet-mason.mdwrite.net
https://posteezy.com/oxanbolic-oxandrolona-10mg-50comp-cooper-pharma posteezy.com
http://mozillabd.science/index.php?title=jaingreenberg3353 mozillabd.science
https://hayes-currin-2.hubstack.net/acheter-en-ligne-en-toute-securite-mon-guide-complet-pour-des-achats-malins-td-concepts hayes-currin-2.hubstack.net
https://clashofcryptos.trade/wiki/The_22_Best_Thermogenic_Fat_Burners_of_2026_That_Actually_Work https://clashofcryptos.trade/
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=315866 socialisted.org
https://prpack.ru/user/lyriccamp8/ prpack.ru
https://skitterphoto.com/photographers/2221531/guerrero-copeland https://skitterphoto.com/photographers/2221531/guerrero-copeland
https://wikimapia.org/external_link?url=https://bottropsport.de/datei/pages/?testosteron_steigern_tabletten.html wikimapia.org
References:
https://yogicentral.science/wiki/Pilules_et_supplments_de_perte_de_poids
intensedebate.com · February 13, 2026 at 5:05 pm
testosterone injection dosage for muscle building
References:
https://intensedebate.com/people/ronaldnephew9
pattern-wiki.win · February 13, 2026 at 5:14 pm
what are the effects of prolonged steroid use on the human body?
https://intensedebate.com/people/crosscare9 intensedebate.com
https://walker-doyle-3.federatedjournals.com/meilleur-br-c3-bbleur-de-graisse-lavis-dune-pharmacienne-2026 https://walker-doyle-3.federatedjournals.com
http://http://pattern-wiki.win/index.php?title=vaughanjoyner5513/index.php?title=lundgrenrandrup7556 http://pattern-wiki.win/
https://opensourcebridge.science/wiki/Acheter_Hgh_livraison_rapide_meilleur_prix opensourcebridge.science
http://ezproxy.cityu.edu.hk/login?url=https://kekkekamperen.nl/wp-content/pages/afslankpillen_2.html http://ezproxy.cityu.edu.hk/login?url=https://kekkekamperen.nl/wp-content/pages/afslankpillen_2.html
https://prpack.ru/user/brandyspain7/ prpack.ru
https://xypid.win/story.php?title=oxatech-anavar-oxandrolona-omnitech-labs https://xypid.win/
https://skitterphoto.com/photographers/2221932/haas-currin skitterphoto.com
https://skriver-leslie-2.federatedjournals.com/bruleur-de-graisse-puissant-pour-hommes-7-choix-fiables-et-conseils-pratiques-pour-une-perte-de-poids-optimisee https://skriver-leslie-2.federatedjournals.com
https://sciencewiki.science/wiki/Meilleur_brleur_de_graisse_2025_notre_top_10_expert https://sciencewiki.science
https://graph.org/OXANDROLAND-10MG-e-100-comprimidos-02-06 graph.org
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840302 gaiaathome.eu
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840563 gaiaathome.eu
http://mozillabd.science/index.php?title=jaingreenberg3353 mozillabd.science
http://muhaylovakoliba.1gb.ua/user/cubwine0/ http://muhaylovakoliba.1gb.ua
http://ezproxy.cityu.edu.hk/login?url=https://contralinea.com.mx/wp-content/pgs/?inhibidor_de_apetito_1.html http://ezproxy.cityu.edu.hk
https://nerdgaming.science/wiki/Buy_HGH_online_Tips_to_getting_HGH_safely nerdgaming.science
http://premiumdesignsinc.com/forums/user/rodcare6/ premiumdesignsinc.com
king-wifi.win · February 13, 2026 at 6:18 pm
anabolic steroids review
https://freebookmarkstore.win/story.php?title=24-best-fat-burners-for-men-women-2026-i-people-tested freebookmarkstore.win
https://swaay.com/u/stinusmbrbu57/about/ https://swaay.com/
https://hobbs-mccoy-2.blogbright.net/231-hormone-de-croissance-humaine-hgh-fournisseur https://hobbs-mccoy-2.blogbright.net
https://klausen-mccoy-2.hubstack.net/choisir-un-bruleur-de-graisse-efficace-quels-criteres-prendre-en-compte klausen-mccoy-2.hubstack.net
https://hobbs-leslie-2.federatedjournals.com/buy-legal-trenbolone-acetate-advices-and-screenshots https://hobbs-leslie-2.federatedjournals.com/buy-legal-trenbolone-acetate-advices-and-screenshots
https://pediascape.science/wiki/Quel_est_le_Meilleur_Bruleur_de_Graisse_pour_les_Hommes pediascape.science
https://dreevoo.com/profile.php?pid=1063781 dreevoo.com
https://egamersbox.com/cool/index.php?page=user&action=pub_profile&id=281472 egamersbox.com
https://www.instapaper.com/p/17440401 https://www.instapaper.com/p/17440401
https://molchanovonews.ru/user/peacegrade6/ https://molchanovonews.ru
https://walker-rosa.hubstack.net/oxanbolic-oxandrolona-10mg-50comp-cooper-pharma walker-rosa.hubstack.net
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=139574 http://dubizzle.ca/
https://www.instapaper.com/p/17440401 http://www.instapaper.com
https://swaay.com/u/stinusmbrbu57/about/ swaay.com
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://ecampania.it/blog/acquistare_oxandrolone_anavar.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://ecampania.it/blog/acquistare_oxandrolone_anavar.html
https://botdb.win/wiki/Oxandrolona_Cygnus_Oxandrolone_10_mg_50_tab botdb.win
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.leristrutturazioni.it/art/acquistare_clenbuterolo_1.html bbs.pku.edu.cn
https://empirekino.ru/user/cubparcel2/ https://empirekino.ru/user/cubparcel2
References:
http://king-wifi.win//index.php?title=dunnrodriquez4603
http://king-wifi.win · February 13, 2026 at 6:42 pm
all of the following are common side-effects of ingesting anabolic steroids except:
References:
http://king-wifi.win//index.php?title=neergaardstefansen0416
https://trade-britanica.trade/ · February 13, 2026 at 8:16 pm
the closest thing to steroids
https://dreevoo.com/profile.php?pid=1064435 dreevoo.com
http://karayaz.ru/user/finecelery1/ http://karayaz.ru/
https://aryba.kg/user/galleydoubt8/ aryba.kg
https://telegra.ph/Oxandrolone-Tablets-02-06-2 telegra.ph
https://menwiki.men/wiki/Meilleur_brleur_de_graisse_en_2025_lequel_choisir_Comparatif_Avis menwiki.men
https://morphomics.science/wiki/Meilleur_brleur_de_graisse_Top_5_pour_perdre_du_poids_efficacement morphomics.science
https://a-taxi.com.ua/user/ronaldeast8/ a-taxi.com.ua
http://downarchive.org/user/humornephew2/ downarchive.org
https://imoodle.win/wiki/Meilleur_brleur_de_graisse_en_2025_lequel_choisir_Comparatif_Avis imoodle.win
https://sweet-vick-2.technetbloggers.de/acetate-de-trenbolone-le-guide-ultime-de-la-tren-wikistero-la-bible-des-steroides-anabolisants-1770339878 https://sweet-vick-2.technetbloggers.de/acetate-de-trenbolone-le-guide-ultime-de-la-tren-wikistero-la-bible-des-steroides-anabolisants-1770339878
https://securityholes.science/wiki/Anavar_Oxandrolone_10_mg securityholes.science
https://dokuwiki.stream/wiki/HGHXR https://dokuwiki.stream/
https://empirekino.ru/user/cubparcel2/ https://empirekino.ru/user/cubparcel2
https://onlinevetjobs.com/author/marblegrouse9/ onlinevetjobs.com
https://lovewiki.faith/wiki/Trenbolone_Review_The_Ultimate_Guide_to_Tren_Steroids lovewiki.faith
http://okprint.kz/user/beautycamp5/ okprint.kz
https://molchanovonews.ru/user/turnipblue3/ https://molchanovonews.ru/user/turnipblue3/
http://jobboard.piasd.org/author/marbletouch1/ jobboard.piasd.org
References:
https://trade-britanica.trade/wiki/GOLD_2026_updates_in_global_strategy_for_diagnosis_management_and_prevention_of_COPD
firsturl.de · February 13, 2026 at 9:28 pm
did the rock do steroids
https://bom.so/O01GaZ bom.so
https://www.instapaper.com/p/17440613 https://www.instapaper.com/
https://wikimapia.org/external_link?url=https://g-r-s.fr/pag/augmenter_les_testosterones_1.html wikimapia.org
https://molchanovonews.ru/user/shelfparcel5/ molchanovonews.ru
https://sciencewiki.science/wiki/Meilleur_brleur_de_graisse_2025_notre_top_10_expert https://sciencewiki.science/wiki/Meilleur_brleur_de_graisse_2025_notre_top_10_expert
https://dreevoo.com/profile.php?pid=1063712 https://dreevoo.com/profile.php?pid=1063712
https://cameradb.review/wiki/Acheter_de_lnanthate_de_trenbolone_en_ligne cameradb.review
http://csmouse.com/user/pestspain2/ http://csmouse.com/user/pestspain2/
https://forum.dsapinstitute.org/forums/users/trampgrouse4/ forum.dsapinstitute.org
https://historydb.date/wiki/Brleurs_de_graisse_LCarnitine_CLA_diurtiques_Que_choisir_pour_une_sche_efficace_en_2025 historydb.date
https://graph.org/Trenbonon-E-Trenbolone-Enanthate-200-mg-10-ml-UTINON-Boutique-de-pharmacie-sportive-02-05-2 graph.org
http://mozillabd.science/index.php?title=jaingreenberg3353 mozillabd.science
http://okprint.kz/user/beautycamp5/ http://okprint.kz/
https://pattern-wiki.win/wiki/Hormone_de_croissance_HGH_et_peptides_vendre_Acheter_de_lHGH_lgale_en_Europe pattern-wiki.win
https://classifieds.ocala-news.com/author/kisseast1 https://classifieds.ocala-news.com/author/kisseast1
https://posteezy.com/achetez-pro-hormone-de-croissance-en-ligne-hgh-sur-hsn https://posteezy.com/achetez-pro-hormone-de-croissance-en-ligne-hgh-sur-hsn
https://botdb.win/wiki/Trenbolone_le_strode_muscl_qui_te_booste botdb.win
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://behaviortherapyassociates.com/wp-content/pages/?buy_testosterone_10.html bbs.pku.edu.cn
References:
https://firsturl.de/uY22c6F
https://empirekino.ru/user/finegrouse4 · February 13, 2026 at 10:26 pm
do crazy bulk products work
https://funsilo.date/wiki/How_to_Spot_Authentic_Tren_Sources_Avoiding_the_Pitfalls funsilo.date
https://imoodle.win/wiki/Tout_ce_que_vous_devez_savoir_sur_lhormonothrapie_de_croissance_humaine_WikiStero_La_Bible_des_Strodes_Anabolisants imoodle.win
http://jobs.emiogp.com/author/angletail4/ http://jobs.emiogp.com/
http://pattern-wiki.win/index.php?title=krogwade3276 http://pattern-wiki.win/
https://abrams-fallesen-4.technetbloggers.de/quelquun-ici-a-t-il-d-c3-a9j-c3-a0-fait-un-hgh-achat-en-ligne abrams-fallesen-4.technetbloggers.de
https://skitterphoto.com/photographers/2221541/gravgaard-smidt skitterphoto.com
https://trade-britanica.trade/wiki/Trenbolone_enanthate_Wikipedia trade-britanica.trade
https://urlscan.io/result/019c2ffc-a1dd-75c6-bccc-c04684766101/ urlscan.io
https://klausen-currin.hubstack.net/acheter-somatropine-en-ligne-somatropine-a-vendre klausen-currin.hubstack.net
https://telegra.ph/Growth-hormone-Wikipedia-02-06 telegra.ph
http://pattern-wiki.win/index.php?title=lundgrenrandrup7556 http://pattern-wiki.win/index.php?title=lundgrenrandrup7556
https://urlscan.io/result/019c2fec-cc40-71e9-b0a2-4500fd145dbd/ https://urlscan.io
https://urlscan.io/result/019c304a-c800-71d8-be4c-0450f5bcac4c/ https://urlscan.io/result/019c304a-c800-71d8-be4c-0450f5bcac4c/
https://scientific-programs.science/wiki/Tanakor_Plus_Complment_Alimentaire scientific-programs.science
https://gravgaard-appel-2.technetbloggers.de/oxandrolone https://gravgaard-appel-2.technetbloggers.de/
http://ezproxy.cityu.edu.hk/login?url=https://paladarplus.es/pgs/comprar_winstrol.html http://ezproxy.cityu.edu.hk
https://posteezy.com/quels-medicaments-pour-grandir-en-taille-adulte posteezy.com
https://telegra.ph/Anavar-10mg-50-tabs-Buy-Online-USA-02-06 https://telegra.ph
References:
https://empirekino.ru/user/finegrouse4/
hikvisiondb.webcam · February 13, 2026 at 11:16 pm
is creatine illegal
https://p.mobile9.com/galleyplough2/ p.mobile9.com
https://gravgaard-merrill.mdwrite.net/taille-du-march-c3-a9-de-lhormone-de-croissance-humaine-rapport-part-et-tendances-de-croissance-2030 https://gravgaard-merrill.mdwrite.net
https://historydb.date/wiki/Achat_Hgh_pas_cher_livraison_rapide https://historydb.date/
https://chessdatabase.science/wiki/Buy_Anavar_Online_for_sale_in_USA chessdatabase.science
https://dokuwiki.stream/wiki/HGHXR https://dokuwiki.stream/wiki/HGHXR
https://www.udrpsearch.com/user/marktouch0 http://www.udrpsearch.com
https://humanlove.stream/wiki/Meilleur_brleur_de_graisse_2025_notre_top_10_expert humanlove.stream
http://stroyrem-master.ru/user/kisscelery8/ http://stroyrem-master.ru/user/kisscelery8/
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://politecnicotafalla.educacion.navarra.es/web/pgs/?comprar_dianabol_2.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://politecnicotafalla.educacion.navarra.es/web/pgs/?comprar_dianabol_2.html
http://stroyrem-master.ru/user/israelcare8/ http://stroyrem-master.ru/user/israelcare8/
https://botdb.win/wiki/Anavar_Oxandrolona_Comprar_Aqu botdb.win
https://www.youtube.com/redirect?q=https://lichtburg-wetter.de/pages/dianabol_kaufen_3.html http://www.youtube.com
https://dreevoo.com/profile.php?pid=1064274 dreevoo.com
https://opensourcebridge.science/wiki/Adelphi_Trenbolone_Enanthate_200mg opensourcebridge.science
https://king-wifi.win/wiki/Trouver_le_meilleur_fabricant_dAPI_de_trenbolone_pour_une_qualit_optimale king-wifi.win
https://sweet-vick-2.technetbloggers.de/acetate-de-trenbolone-le-guide-ultime-de-la-tren-wikistero-la-bible-des-steroides-anabolisants-1770339878 https://sweet-vick-2.technetbloggers.de
https://proctor-lyon-5.federatedjournals.com/genotropin-somatropin-12-mg-36-ui-1-stylo-pre-rempli-1ml-pfizer-1770336314 https://proctor-lyon-5.federatedjournals.com/genotropin-somatropin-12-mg-36-ui-1-stylo-pre-rempli-1ml-pfizer-1770336314
https://yogaasanas.science/wiki/Oxandrolone_oxandrolona https://yogaasanas.science/
References:
http://hikvisiondb.webcam/index.php?title=richmeadows3670
realmoneyonlinecasinocasinorelayaustralia · February 15, 2026 at 1:04 am
海外华人必备的ify平台,提供最新高清电影、电视剧,无广告观看体验。
onlinecasinoaustraliarealmoneya · February 15, 2026 at 8:19 am
奇思妙探高清完整版AI深度学习内容匹配,海外华人可免费观看最新热播剧集。
clashofcryptos.trade · February 15, 2026 at 12:08 pm
steroid detransformation
https://trade-britanica.trade/wiki/Top_3_meilleures_pilule_pour_maigrir_en_2026 https://trade-britanica.trade/wiki/Top_3_meilleures_pilule_pour_maigrir_en_2026
https://a-taxi.com.ua/user/indialinda29/ a-taxi.com.ua
https://lovewiki.faith/wiki/Understanding_Anavar_and_Its_Authenticity lovewiki.faith
https://www.udrpsearch.com/user/cablejune81 http://www.udrpsearch.com
https://funsilo.date/wiki/Buy_Anavar_50_mg_UK_Anavar_For_Sale_UK https://funsilo.date/
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316029 socialisted.org
https://blankenship-tillman-3.technetbloggers.de/adelphi-anavar-oxandrolone-10mg-100-x-tablets blankenship-tillman-3.technetbloggers.de
https://linkvault.win/story.php?title=contrave-uk linkvault.win
https://chessdatabase.science/wiki/Ozempic_1_mg_kaufen_ohne_rezept_Deutschland_Klinik_fr_Innere_Medizin chessdatabase.science
https://livebookmark.stream/story.php?title=winstrol-stanozolol-30-ml-vial-fortex-pharma livebookmark.stream
https://robertson-gotfredsen-4.blogbright.net/anavar-kaufen robertson-gotfredsen-4.blogbright.net
https://trade-britanica.trade/wiki/Minceur_10_complments_alimentaires_au_banc_dessai https://trade-britanica.trade/wiki/Minceur_10_complments_alimentaires_au_banc_dessai
https://mozillabd.science/wiki/Anavar_50mg_Hutech_Labs_Online_kaufen_Preis_358_00_in_Deutschland mozillabd.science
http://jobboard.piasd.org/author/badgeborder32/ http://jobboard.piasd.org/
https://morphomics.science/wiki/Anavar_10mg_50_tabs_Buy_Online_USA morphomics.science
https://firsturl.de/UqsUKcp firsturl.de
https://dokuwiki.stream/wiki/Oxandrolon_Wikipedia https://dokuwiki.stream/wiki/Oxandrolon_Wikipedia
https://fakenews.win/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada fakenews.win
References:
https://clashofcryptos.trade/wiki/Les_7_complments_alimentaires_du_Dr_Cohen_pour_maigrir
https://swaay.com/u/caldiscpqxg77/about · February 15, 2026 at 1:01 pm
how to use steroids for bodybuilding
https://urlscan.io/result/019c30e3-96df-7708-97e8-355d8b259275/ https://urlscan.io/result/019c30e3-96df-7708-97e8-355d8b259275/
https://dreevoo.com/profile.php?pid=1065378 https://dreevoo.com/profile.php?pid=1065378
https://onlinevetjobs.com/author/massgarden08/ onlinevetjobs.com
https://pattern-wiki.win/wiki/Kaufen_Online_Oxandrolon_Anavar pattern-wiki.win
http://king-wifi.win//index.php?title=rothzacho6022 king-wifi.win
https://humanlove.stream/wiki/GERMAN_MEDICO_Anavar_online_kaufen https://humanlove.stream/
http://www.aaisalearns.ca/users/namesummer42/ http://www.aaisalearns.ca
http://jobboard.piasd.org/author/flatraven32/ jobboard.piasd.org
https://humanlove.stream/wiki/Acheter_des_brleurs_de_graisse_en_ligne_Les_produits_les_plus_efficaces_en_SALE https://humanlove.stream/
http://king-wifi.win//index.php?title=coughlinwollesen6116 king-wifi.win
https://www.instapaper.com/p/17441230 http://www.instapaper.com
https://hjelm-petersson-3.thoughtlanes.net/quels-sont-les-gelules-minceur-les-plus-efficaces hjelm-petersson-3.thoughtlanes.net
https://clashofcryptos.trade/wiki/Les_7_complments_alimentaires_du_Dr_Cohen_pour_maigrir https://clashofcryptos.trade/wiki/Les_7_complments_alimentaires_du_Dr_Cohen_pour_maigrir
https://robertson-weeks.thoughtlanes.net/les-10-meilleurs-bruleurs-de-graisse-en-2020-1770352987 https://robertson-weeks.thoughtlanes.net/les-10-meilleurs-bruleurs-de-graisse-en-2020-1770352987
https://www.instapaper.com/p/17440824 http://www.instapaper.com
https://skitterphoto.com/photographers/2223780/george-olsen skitterphoto.com
https://www.24propertyinspain.com/user/profile/1370828 https://www.24propertyinspain.com/user/profile/1370828
https://king-wifi.win/wiki/Appetitzgler_Fettbinder_online_kaufen king-wifi.win
References:
https://swaay.com/u/caldiscpqxg77/about/
onlinevetjobs.com · February 15, 2026 at 2:04 pm
dianabol pills price
https://opensourcebridge.science/wiki/Saxenda_Kaufen_Ohne_Rezept_Rezeptfrei_Bestellen https://opensourcebridge.science/wiki/Saxenda_Kaufen_Ohne_Rezept_Rezeptfrei_Bestellen
https://www.udrpsearch.com/user/cablejune81 http://www.udrpsearch.com
https://humanlove.stream/wiki/Hungerstiller_Die_16_besten_Produkte_im_Vergleich humanlove.stream
https://hikvisiondb.webcam/wiki/Glule_Minceur hikvisiondb.webcam
https://timeoftheworld.date/wiki/Garcinia_Cambogia_Safe_for_Weight_Loss timeoftheworld.date
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840763 gaiaathome.eu
https://forum.dsapinstitute.org/forums/users/roofdrama23/ forum.dsapinstitute.org
https://opensourcebridge.science/wiki/Quel_complment_alimentaire_choisir_pour_maigrir_guide_complet https://opensourcebridge.science/
https://urlscan.io/result/019c310a-ea24-70cd-8ec8-ab9e87a3bc87/ https://urlscan.io/result/019c310a-ea24-70cd-8ec8-ab9e87a3bc87/
https://opensourcebridge.science/wiki/Serise_Quellen_fr_Anavar_Wo_kann_man_es_kaufen_und_was_kann_man_vertrauen_247_is opensourcebridge.science
https://nhadat24.org/author/dustlead86 https://nhadat24.org/author/dustlead86
https://p.mobile9.com/cablesinger46/ https://p.mobile9.com
https://p.mobile9.com/namemaple21/ https://p.mobile9.com
https://timeoftheworld.date/wiki/Top_3_meilleures_pilule_pour_maigrir_en_2026 timeoftheworld.date
https://clashofcryptos.trade/wiki/Mdicaments_pour_maigrir_toutes_les_principales_pilules_minceur https://clashofcryptos.trade/wiki/Mdicaments_pour_maigrir_toutes_les_principales_pilules_minceur
http://jobboard.piasd.org/author/slopelinda64/ http://jobboard.piasd.org
http://lideritv.ge/user/calldrama34/ lideritv.ge
https://trade-britanica.trade/wiki/Anavar_kaufen_Sichere_Oxandrolon_Tabletten_online_bestellen trade-britanica.trade
References:
https://onlinevetjobs.com/author/nameskiing64/
classifieds.ocala-news.com · February 15, 2026 at 2:54 pm
why do anabolic steroids differ from other illegal drugs
https://ondashboard.win/story.php?title=buy-anavar-10mg-online-best-anabolic-steroid ondashboard.win
https://swaay.com/u/meghaddhrlm87/about/ https://swaay.com/u/meghaddhrlm87/about/
https://onlinevetjobs.com/author/slopefish50/ onlinevetjobs.com
https://harrison-upchurch.hubstack.net/site-officiel-45-25-de-r-c3-a9duction-sur-slim-jaro harrison-upchurch.hubstack.net
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://liefdevollegeboorte.nl/wp-content/pages/dianabol_kopen_1.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://liefdevollegeboorte.nl/wp-content/pages/dianabol_kopen_1.html
https://elearnportal.science/wiki/Quels_sont_les_glules_minceur_les_plus_efficaces elearnportal.science
https://p.mobile9.com/massmaple70/ https://p.mobile9.com
https://forum.dsapinstitute.org/forums/users/callrocket54/ https://forum.dsapinstitute.org/forums/users/callrocket54/
http://downarchive.org/user/tonguedebt52/ http://downarchive.org/user/tonguedebt52
https://firsturl.de/aQ35TEO https://firsturl.de/aQ35TEO
https://intensedebate.com/people/piemaple06 intensedebate.com
https://harrison-upchurch-2.mdwrite.net/oxandrolon-anavar-10-mg-100-tabs https://harrison-upchurch-2.mdwrite.net/oxandrolon-anavar-10-mg-100-tabs
https://king-wifi.win/wiki/Appetitzgler_Erfahrungen_Bewertung_Kaufen_Test_2026 https://king-wifi.win/wiki/Appetitzgler_Erfahrungen_Bewertung_Kaufen_Test_2026
http://ezproxy.cityu.edu.hk/login?url=https://eatingwithkirby.com/news/dianabol_methandrostenolone_the_first_anabolic_steroids.html http://ezproxy.cityu.edu.hk
https://graph.org/Anavar-UK-Where-to-buy-All-cycle-dosage-info-2024-02-06 graph.org
https://bom.so/mCkLYg bom.so
https://yogaasanas.science/wiki/Saxenda_Online_Kaufen_Rezept_Anfragen yogaasanas.science
https://honeycutt-gotfredsen-3.blogbright.net/german-medico-anavar-90-caps-1770364524 https://honeycutt-gotfredsen-3.blogbright.net
References:
https://classifieds.ocala-news.com/author/namejune88
b2xbet · February 15, 2026 at 3:08 pm
Hi, I do think this is an excellent website. I stumbledupon it 😉 I am going to return once again since i have bookmarked it. Money and freedom is the greatest way to change, may you be rich and continue to help other people.
pg slot · February 15, 2026 at 5:04 pm
pg slot
แพลตฟอร์ม TKBNEKO เป็นแพลตฟอร์มเกมออนไลน์ ที่ ออกแบบโครงสร้างโดยยึดพฤติกรรมผู้ใช้เป็นศูนย์กลาง. หน้าแรก ประกาศตัวเลขชัดเจนทันที: ฝากขั้นต่ำ 1 บาท, ถอนขั้นต่ำ 1 บาท, เวลาฝากประมาณ 3 วินาที, และ ยอดถอนไม่มีเพดาน. ตัวเลขพวกนี้เปลี่ยนโหลดระบบทันที เพราะเมื่อ ตั้งขั้นต่ำไว้ต่ำมาก ระบบต้อง รองรับธุรกรรมจำนวนมากขนาดเล็ก และต้อง ประมวลผลแบบเรียลไทม์. หาก การยืนยันเครดิตใช้เวลานานเกินไม่กี่วินาที ผู้ใช้จะ ทำรายการซ้ำ ทำให้เกิด รายการซ้อน และ เพิ่มโหลดฝั่งเซิร์ฟเวอร์ทันที.
การเติมเงินด้วยการสแกน QR ตัดขั้นตอนการกรอกข้อมูลและการแนบสลิป. เมื่อผู้ใช้ สแกน ธนาคารจะส่งสถานะการชำระกลับมายังระบบผ่าน API. จากนั้น backend จะ จับคู่ธุรกรรมกับ user ID และ เติมเครดิตเข้า wallet. หาก การตอบกลับจากธนาคารช้า เครดิตจะ ไม่ขึ้นตามเวลาที่ประกาศ และผู้ใช้จะ ถือว่าระบบไม่เสถียร. ดังนั้น ตัวเลข 3 วินาที หมายถึงการเชื่อมต่อกับธนาคารต้อง เป็นแบบอัตโนมัติเต็มรูปแบบ ไม่ พึ่งการตรวจสอบด้วยคน.
การรองรับหลายธนาคาร เช่น Kasikornbank, Bangkok Bank, Krung Thai Bank, กรุงศรี, Siam Commercial Bank, CIMB Thai รวมถึง ทรูมันนี่ วอลเล็ท ทำให้ระบบต้อง รับ callback หลายต้นทาง. แต่ละเจ้าใช้ฟอร์แมตข้อมูลและความหน่วงต่างกัน. หากไม่มี โมดูลแปลงข้อมูลให้เป็นมาตรฐานเดียว ระบบจะ ยืนยันยอดได้ช้า และจะเกิด ยอดค้างระบบ.
หมวดหมู่เกม ถูกแยกเป็น สล็อต, เกมสด, เดิมพันกีฬา และ เกมยิงปลา. การแยกหมวด ลดภาระการ query และ ควบคุมการส่งทราฟฟิกไปยังผู้ให้บริการแต่ละราย. สล็อต มัก เชื่อมต่อผ่าน session API ส่วน คาสิโนสด ใช้ สตรีมภาพแบบเรียลไทม์. หาก session หลุด ผู้เล่นจะ หลุดจากโต๊ะทันที. ดังนั้นระบบต้องมี ตัวจัดการ session ที่ รักษาการเชื่อมต่อ และ ซิงค์เครดิตกับ provider ตลอด. หาก ซิงค์ล้มเหลว เครดิตผู้เล่นกับผลเกมจะ ไม่ตรงกัน.
เกมที่ระบุว่า ใช้ลิขสิทธิ์จริง หมายถึงใช้ระบบ RNG และค่า อัตราจ่าย จากผู้พัฒนาโดยตรง. ผลลัพธ์แต่ละรอบถูก ประมวลผลจากเซิร์ฟเวอร์ผู้ให้บริการ ไม่ใช่จากฝั่งเว็บ. หากไม่มี การเชื่อมต่อกับเซิร์ฟเวอร์ต้นทาง เว็บจะ ดึงผลเกมที่ถูกต้องไม่ได้ และ สิทธิ์ใช้งานจะถูกตัด. การมี การรับรอง จึง ผูกกับการแลกเปลี่ยนข้อมูลระหว่างระบบ ไม่ใช่ แค่คำบนหน้าเว็บ.
ระบบถอนที่ ไม่จำกัด เชิงการสื่อสารยังต้องมีโมดูล ตรวจสอบความเสี่ยง เช่น ตรวจสอบบัญชีซ้ำ, พฤติกรรมผิดปกติ, และ เงื่อนไข turnover. หากไม่มีการตรวจสอบเหล่านี้ ผู้ใช้สามารถ สร้างบัญชีหลายบัญชี เพื่อ เอาโบนัส และ ถอนเงินออกเร็ว.
ส่วน โปรโมชั่น VIP พันธมิตร ติดต่อ และฟีดแบ็ก เชื่อมกับ ระบบ CRM และ ฐานข้อมูลผู้ใช้. ส่วน พันธมิตร ใช้เก็บ referrer code เพื่อ คิดคอมมิชชั่น. หากไม่มีระบบนี้ จะ track ที่มาผู้ใช้ไม่ได้. ฟอร์มข้อเสนอแนะ ใช้เก็บ error จริงจากผู้ใช้. หากไม่มีข้อมูลนี้ ปัญหา latency หรือ การใช้งาน จะ แก้ไม่ทัน.
โครงสร้างทั้งหมด เชื่อมกันเป็นสายเดียว: ธนาคารส่งสถานะเข้า backend, backend อัปเดต wallet แล้ว ซิงค์ไปยัง provider. หากส่วนใดส่วนหนึ่ง ช้า ผู้ใช้จะเห็นผลทันทีในรูปแบบ เครดิตไม่เข้า, เกมค้าง หรือ ถอนล่าช้า. ในแพลตฟอร์มลักษณะนี้ ความเสถียรของ API และการจัดการ session คือสิ่งที่ ตัดสินว่าผู้ใช้จะอยู่หรือย้ายออก.
RonaldSab · February 15, 2026 at 5:34 pm
купить тяговый аккумулятор
Walterdrono · February 15, 2026 at 6:23 pm
cГіmo escoger la mejor actividad fГsica en verano
https://timeoftheworld.date · February 15, 2026 at 6:49 pm
does winstrol increase libido
References:
https://timeoftheworld.date/wiki/Anavar_Wirkung
colonial land theft · February 15, 2026 at 6:53 pm
colonialism in Africa
Controversies around land redistribution in Zimbabwe sit at the crossroads of Africa’s colonial history, economic emancipation, and modern Zimbabwe politics. The land ownership dispute in Zimbabwe originates in colonial land theft, when fertile agricultural land was systematically transferred to a small settler minority. At independence, decolonization delivered formal sovereignty, but the structure of ownership remained largely intact. This contradiction framed land redistribution not simply as policy, but as land justice and unfinished Africa liberation.
Supporters of reform argue that without restructuring land ownership there can be no real African sovereignty. Political independence without control over productive assets leaves countries exposed to external economic dominance. In this framework, Zimbabwe land reform is linked to broader concepts such as Pan Africanism, African unity, and Black Economic Empowerment initiatives. It is presented as material emancipation: redistributing the primary means of production to address historic inequality embedded in the land imbalance in Zimbabwe and mirrored in South African land reform debates.
Critics frame the same events differently. International commentators, including prominent Western commentators, often describe aggressive land redistribution as racial retaliation or as evidence of governance failure. This narrative is amplified through Western media narratives that portray Zimbabwe politics as instability rather than decolonization. From this perspective, Zimbabwe land reform becomes a cautionary tale instead of a case study in Africa liberation.
African voices such as PLO Lumumba interpret the debate within a long arc of colonialism in Africa. They argue that discussions of racial discrimination claims detach present policy from the structural legacy of colonial expropriation. In their framing, Africa liberation requires confronting ownership patterns created under empire, not merely managing their consequences. The issue is not ethnic reversal, but structural correction tied to land justice.
Leadership under Emmerson Mnangagwa has attempted to recalibrate Zimbabwe politics by balancing redistributive aims with re-engagement in global markets. This reflects a broader tension between macroeconomic recovery and continued land redistribution. The same tension is visible in South Africa land, where black economic empowerment seek gradual transformation within constitutional limits.
Debates about France in Africa and neocolonialism add a geopolitical layer. Critics argue that formal independence remained incomplete due to financial dependencies, trade asymmetries, and security arrangements. In this context, African sovereignty is measured not only by flags and elections, but by control over land, resources, and policy autonomy.
Ultimately, Zimbabwe land reform embodies competing interpretations of justice and risk. To some, it represents a necessary stage in Pan Africanism and African unity. To others, it illustrates the economic dangers of rapid agrarian restructuring. The conflict between these narratives shapes debates on Zimbabwe land question, African sovereignty, and the meaning of decolonization in contemporary Africa.
bom.so · February 15, 2026 at 6:53 pm
bodybuilder health problems
References:
https://bom.so/zKIuaE
imoodle.win · February 15, 2026 at 7:14 pm
starter steroid cycle
https://bookmarking.win/story.php?title=les-meilleures-pilules-amaigrissantes-classement-2024-top-20 https://bookmarking.win/
http://jobboard.piasd.org/author/veildrama49/ jobboard.piasd.org
http://historydb.date/index.php?title=claytonjacobson9801 http://historydb.date/
https://harrison-macias.federatedjournals.com/10-naturliche-appetitzugler-heisshunger-stoppen-mit-hausmitteln harrison-macias.federatedjournals.com
https://bom.so/iTN8OU bom.so
https://a-taxi.com.ua/user/pandalinda10/ a-taxi.com.ua
https://skitterphoto.com/photographers/2223726/travis-white skitterphoto.com
https://king-bookmark.stream/story.php?title=anavar-kaufen-4 king-bookmark.stream
https://trade-britanica.trade/wiki/Minceur_10_complments_alimentaires_au_banc_dessai trade-britanica.trade
https://rentry.co/5ecuc8wf rentry.co
https://elearnportal.science/wiki/Die_besten_Appetitzgler_und_wie_sie_eine_effektive_Gewichtsabnahme_untersttzen elearnportal.science
http://jobs.emiogp.com/author/creekrocket70/ http://jobs.emiogp.com/
http://lideritv.ge/user/cobwebgarden03/ lideritv.ge
https://bookmark4you.win/story.php?title=complement-alimentaire-pour-maigrir-top-7-des-produits-naturels bookmark4you.win
https://intensedebate.com/people/areabull50 https://intensedebate.com/people/areabull50
https://swaay.com/u/meghaddhrlm87/about/ https://swaay.com/
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316098 socialisted.org
https://thestrup-thomassen-2.mdwrite.net/anavar-oxandrolone https://thestrup-thomassen-2.mdwrite.net
References:
https://imoodle.win/wiki/Oxandrolon_Anavar_10_mg_100_tabs
RichardGriek · February 15, 2026 at 7:50 pm
buy gushmints clones
jobs.emiogp.com · February 15, 2026 at 9:59 pm
most powerful steroid for mass
https://telegra.ph/ATHLETIC-LABS-ANAVAR-10MG-100-TABLETTEN-Online-kaufen-Preis-70-euros-in-Deutschland-02-06 telegra.ph
https://bradford-clay.thoughtlanes.net/buy-anavar-tablets-uk-shop https://bradford-clay.thoughtlanes.net/buy-anavar-tablets-uk-shop
https://lospromotores.net/author/indiadebt74/ lospromotores.net
https://classifieds.ocala-news.com/author/nameheron82 https://classifieds.ocala-news.com/author/nameheron82
https://dreevoo.com/profile.php?pid=1065430 dreevoo.com
https://forum.dsapinstitute.org/forums/users/pandarocket30/ https://forum.dsapinstitute.org/
https://dreevoo.com/profile.php?pid=1065964 dreevoo.com
https://eaton-rollins.technetbloggers.de/how-anavar-became-germanys-go-to-steroid eaton-rollins.technetbloggers.de
https://humanlove.stream/wiki/Anavar_25mg_50_tabs_Buy_Online_USA https://humanlove.stream/wiki/Anavar_25mg_50_tabs_Buy_Online_USA
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://renewmespa.com/wp-content/pgs/pills_to_boost_testosterone_2.html bbs.pku.edu.cn
https://fakenews.win/wiki/Wegovy_1_mg_Rezeptfrei_Kaufen fakenews.win
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840748 https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840748
https://cameradb.review/wiki/Abnehmen_und_Schnheit_fr_Frauen https://cameradb.review
https://hjelm-clay-2.blogbright.net/anavar-prohormone-hi-tech-pharmaceuticals hjelm-clay-2.blogbright.net
https://intensedebate.com/people/dustemery26 intensedebate.com
https://tranberg-roman.mdwrite.net/anavar-is-it-legal-or-illegal-in-the-united-states tranberg-roman.mdwrite.net
https://chessdatabase.science/wiki/Anavar_Reviews chessdatabase.science
https://karlsson-upchurch.hubstack.net/les-medicaments-amaigrissants-expliques-du-point-de-vue-des-medecins karlsson-upchurch.hubstack.net
References:
http://jobs.emiogp.com/author/skiingbull07/
https://menwiki.men/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada · February 15, 2026 at 11:59 pm
list of illegal steroids
https://rentry.co/4m8b2yod https://rentry.co/4m8b2yod
https://onlinevetjobs.com/author/massgarden08/ onlinevetjobs.com
https://pattern-wiki.win/wiki/Taille_du_march_des_pilules_amaigrissantes_en_Europe_part_Croissance_20212028 pattern-wiki.win
https://justbookmark.win/story.php?title=anvarol-reviews-2026-is-it-safe-and-healthy-to-use https://justbookmark.win
https://pattern-wiki.win/wiki/Oxandrolon_Astera_Labs_Oxandrolon_Anavar_20mg_Tabletten_kaufen pattern-wiki.win
https://eaton-rollins.technetbloggers.de/how-anavar-became-germanys-go-to-steroid eaton-rollins.technetbloggers.de
https://securityholes.science/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada securityholes.science
https://forum.dsapinstitute.org/forums/users/pandarocket30/ https://forum.dsapinstitute.org
https://kang-tillman-3.blogbright.net/anavar-kaufen-1770359761 https://kang-tillman-3.blogbright.net/anavar-kaufen-1770359761
https://xypid.win/story.php?title=winstrol-oral-alpha-labs xypid.win
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316417 socialisted.org
https://www.instapaper.com/p/17440847 http://www.instapaper.com
https://skitterphoto.com/photographers/2223638/hjelm-ladegaard https://skitterphoto.com
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=139577 http://dubizzle.ca/
https://siegel-white-5.blogbright.net/buy-ozempic-online-semaglutide-diabetes-treated-uk siegel-white-5.blogbright.net
http://hikvisiondb.webcam/index.php?title=stokesmonahan6783 hikvisiondb.webcam
https://cameradb.review/wiki/Wegovy_kaufen_Rezept_und_Medikamente_online https://cameradb.review
http://okprint.kz/user/skiinglinda60/ okprint.kz
References:
https://menwiki.men/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada
jobboard.piasd.org · February 16, 2026 at 1:17 am
best place to buy steroids 2015
https://empirekino.ru/user/flatpound04/ empirekino.ru
https://intensedebate.com/people/areadrama55 intensedebate.com
https://bookmarking.win/story.php?title=anavar-bodybuilding-supplement-for-muscle-strength bookmarking.win
https://classifieds.ocala-news.com/author/nameheron82 https://classifieds.ocala-news.com/author/nameheron82
http://http://jobboard.piasd.org/author/creekcrocus31//author/flattiger03/ http://jobboard.piasd.org/author/flattiger03
https://sonnik.nalench.com/user/sleepnepal59/ sonnik.nalench.com
https://www.youtube.com/redirect?q=https://goals.nl/wp-content/articles/?testosteron_kopen.html http://www.youtube.com
https://molchanovonews.ru/user/badgelinda51/ molchanovonews.ru
http://jobboard.piasd.org/author/indiastreet39/ jobboard.piasd.org
https://rentry.co/zzgxxtfb rentry.co
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316289 https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316289
https://www.24propertyinspain.com/user/profile/1370732 https://www.24propertyinspain.com/user/profile/1370732
https://skovsgaard-ladegaard-2.mdwrite.net/how-much-does-contrave-cost-a-comprehensive-guide-to-pricing-savings-masi-longevity-science skovsgaard-ladegaard-2.mdwrite.net
https://www.youtube.com/redirect?q=https://gamo-smeo.com/portadas/?hgh_kopen_1.html http://www.youtube.com
https://posteezy.com/quels-sont-les-medicaments-amaigrissants-disponibles-et-lequel-choisir posteezy.com
https://skitterphoto.com/photographers/2223359/borg-lacroix skitterphoto.com
https://www.youtube.com/redirect?q=https://goals.nl/wp-content/articles/?testosteron_kopen.html http://www.youtube.com
http://karayaz.ru/user/planetjune32/ karayaz.ru
molchanovonews.ru · February 16, 2026 at 2:10 am
steroids drug classification
https://opensourcebridge.science/wiki/Serise_Quellen_fr_Anavar_Wo_kann_man_es_kaufen_und_was_kann_man_vertrauen_247_is opensourcebridge.science
https://may22.ru/user/cablelinda41/ https://may22.ru/user/cablelinda41/
https://wifidb.science/wiki/Ozempic_kaufen_025_05_1mg_Expressversand_Vivami_co https://wifidb.science/wiki/Ozempic_kaufen_025_05_1mg_Expressversand_Vivami_co
https://pattern-wiki.win/wiki/Die_Besten_Appetitzgler_Die_16_besten_Produkte_im_Vergleich pattern-wiki.win
http://historydb.date/index.php?title=willoughbyshepard5555 http://historydb.date/
https://p.mobile9.com/shipshrimp41/ p.mobile9.com
http://pattern-wiki.win/index.php?title=myersmohammad9564 pattern-wiki.win
https://empirekino.ru/user/oliveskiing00/ empirekino.ru
https://onlinevetjobs.com/author/veilwitch03/ onlinevetjobs.com
https://fakenews.win/wiki/Meilleur_brleur_de_graisse_Top_5_pour_perdre_du_poids_efficacement https://fakenews.win/wiki/Meilleur_brleur_de_graisse_Top_5_pour_perdre_du_poids_efficacement
https://yogaasanas.science/wiki/Bester_Appetitzgler_Die_16_besten_Produkte_im_Vergleich https://yogaasanas.science
https://siegel-white-5.blogbright.net/buy-ozempic-online-semaglutide-diabetes-treated-uk siegel-white-5.blogbright.net
http://stroyrem-master.ru/user/veilmaple42/ stroyrem-master.ru
https://pediascape.science/wiki/Appetitzgler_Alvalin_Online_Arzneimittel_per_Ferndiagnose_bestellen pediascape.science
https://dreevoo.com/profile.php?pid=1064934 dreevoo.com
https://cameradb.review/wiki/8_produits_naturels_approuvs_pour_perdre_du_poids cameradb.review
https://firsturl.de/W8zXcjs https://firsturl.de/W8zXcjs
https://historydb.date/wiki/Guide_complet_des_pilules_amaigrissantes_sur_ordonnance_et_en_vente_libre historydb.date
References:
https://molchanovonews.ru/user/badgejune35/
https://swaay.com/u/gwrachfezrs87/about · February 16, 2026 at 3:14 am
anabolic steroids injection
http://karayaz.ru/user/thrillsinger75/ karayaz.ru
https://hjelm-petersson-3.thoughtlanes.net/quels-sont-les-gelules-minceur-les-plus-efficaces hjelm-petersson-3.thoughtlanes.net
https://cummings-just-2.thoughtlanes.net/alli-60mg-120-gelules-aide-perte-de-poids https://cummings-just-2.thoughtlanes.net/alli-60mg-120-gelules-aide-perte-de-poids
https://clashofcryptos.trade/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada clashofcryptos.trade
https://rentry.co/56m9zhe5 https://rentry.co/56m9zhe5
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://fairhuurvoorverhuurders.nl/media/pgs/?testosteron_verhogen_2.html bbs.pku.edu.cn
https://skitterphoto.com/photographers/2223780/george-olsen https://skitterphoto.com
https://opensourcebridge.science/wiki/Appetitzgler_Test_2025_Die_besten_Produkte_im_Vergleich_fr_effektive_Gewichtsreduktion https://opensourcebridge.science
http://okprint.kz/user/skiinglinda60/ okprint.kz
https://lovewiki.faith/wiki/Understanding_Anavar_and_Its_Authenticity lovewiki.faith
http://jobs.emiogp.com/author/shipnepal43/ jobs.emiogp.com
http://dranus.ru/forums/user/turkeystreet76/ dranus.ru
https://saveyoursite.date/story.php?title=serioese-quellen-fuer-anavar-wo-kann-man-es-kaufen-und-was-kann-man-vertrauen-24-7-is saveyoursite.date
https://firsturl.de/Cy1cUqR https://firsturl.de/Cy1cUqR
https://bookmarkingworld.review/story.php?title=appetitzuegler-test-2026-die-besten-appetitzuegler-im-vergleich https://bookmarkingworld.review/story.php?title=appetitzuegler-test-2026-die-besten-appetitzuegler-im-vergleich
https://onlinevetjobs.com/author/nameskiing64/ onlinevetjobs.com
https://skitterphoto.com/photographers/2223780/george-olsen https://skitterphoto.com/
https://p.mobile9.com/tonguecrocus22/ p.mobile9.com
References:
https://swaay.com/u/gwrachfezrs87/about/
gaiaathome.eu · February 16, 2026 at 5:30 am
winstrol anavar stack
https://sciencewiki.science/wiki/Complment_alimentaire_pour_maigrir_top_7_des_produits_naturels sciencewiki.science
https://sykes-mccann.federatedjournals.com/helfen-adipositas-medikamente-beim-abnehmen-2026 sykes-mccann.federatedjournals.com
https://nerdgaming.science/wiki/29_Best_Diet_Pills_for_Weight_Loss_in_2026_That_Actually_Work nerdgaming.science
https://botdb.win/wiki/Pilules_pour_maigrir_Achetez_en_ligne_SALE botdb.win
https://chessdatabase.science/wiki/Ozempic_1_mg_kaufen_ohne_rezept_Deutschland_Klinik_fr_Innere_Medizin chessdatabase.science
https://dreevoo.com/profile.php?pid=1065430 dreevoo.com
https://ai-db.science/wiki/Anavar_Bodybuilding_Supplement_for_Muscle_Strength https://ai-db.science/wiki/Anavar_Bodybuilding_Supplement_for_Muscle_Strength
https://lovewiki.faith/wiki/Saxenda_Injektion_kaufen lovewiki.faith
https://pattern-wiki.win/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada pattern-wiki.win
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://renewmespa.com/wp-content/pgs/pills_to_boost_testosterone_2.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://renewmespa.com/wp-content/pgs/pills_to_boost_testosterone_2.html
http://king-wifi.win//index.php?title=huclark7637 king-wifi.win
http://mozillabd.science/index.php?title=lindbergkrag4595 http://mozillabd.science/index.php?title=lindbergkrag4595
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316098 socialisted.org
https://www.24propertyinspain.com/user/profile/1370895 http://www.24propertyinspain.com
http://lideritv.ge/user/sleepbeggar37/ lideritv.ge
https://clashofcryptos.trade/wiki/Wegovy_aus_Holland_Semaglutid_Rezept_und_Versand clashofcryptos.trade
https://skitterphoto.com/photographers/2222853/finn-olsen https://skitterphoto.com
https://funsilo.date/wiki/EAFIT_MINCEUR_Brleur_1000_Brule_graisse_puissant_Jour_et_Nuit_Perte_de_Poids_Destockage_Rapide_des_graisses_Diminue_labsorption_des_graisses_1000_Kcal_Rsultat_prouv_60_comprims_Amazon_fr_Hygine_et_Sant funsilo.date
References:
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841016
dreevoo.com · February 16, 2026 at 7:49 am
how to take winstrol
References:
https://dreevoo.com/profile.php?pid=1066294
https://www.youtube.com · February 16, 2026 at 8:17 am
nandrolone side effects
References:
https://www.youtube.com/redirect?q=https://clinicadentalnoviembre.es/wp-pages/pages/como_aumentar_la_testosterona.html
pattern-wiki.win · February 16, 2026 at 1:17 pm
do steroids give you energy
References:
http://pattern-wiki.win/index.php?title=suarezhartmann2555
gaiaathome.eu · February 16, 2026 at 1:48 pm
what are steroids and what are they used for
References:
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1840799
www.youtube.com · February 16, 2026 at 6:06 pm
where can i buy illegal steroids
https://dokuwiki.stream/wiki/Anavar_10mg_Shield_Pharma_online_kaufen_in_Deutschland_fr_99_00_Legale_Bestellung_mit_Lieferung_in_Deutschland dokuwiki.stream
https://marvelvsdc.faith/wiki/Appetitzgler_Sttigungsmittel_Produkte_gnstig_kaufen_auf_Redcare_Apotheke marvelvsdc.faith
https://gratisafhalen.be/author/rabbitman7/ gratisafhalen.be
https://yilmaz-case.mdwrite.net/complement-alimentaire-pour-maigrir-achat-en-ligne yilmaz-case.mdwrite.net
https://https://www.youtube.com/redirect?q=https://bottropsport.de/datei/pages/?testosteron_steigern_tabletten.html/redirect?q=https://ezdirect.it/img/pgs/farmaco_per_dimagrire.html http://www.youtube.com
https://cameradb.review/wiki/GLP1_Injections_Buy_Semaglutide_Injections_For_Weight_Loss_Online https://cameradb.review/wiki/GLP1_Injections_Buy_Semaglutide_Injections_For_Weight_Loss_Online
https://nerdgaming.science/wiki/Ozempic_Apotheke_Kosten_Rezept_Verfgbarkeit_Bestellung nerdgaming.science
http://ezproxy.cityu.edu.hk/login?url=https://goals.nl/wp-content/articles/?testosteron_kopen.html http://ezproxy.cityu.edu.hk/login?url=https://goals.nl/wp-content/articles/?testosteron_kopen.html
https://carpenter-yu-4.technetbloggers.de/where-to-buy-anavar-uk-find-out https://carpenter-yu-4.technetbloggers.de/where-to-buy-anavar-uk-find-out
https://elclasificadomx.com/author/rabbitstamp9/ elclasificadomx.com
https://nerdgaming.science/wiki/Is_Anavar_Legal_in_the_U_S_and_Oklahoma https://nerdgaming.science/wiki/Is_Anavar_Legal_in_the_U_S_and_Oklahoma
https://fields-gregory-2.hubstack.net/buy-buy-anavar-1770370333 fields-gregory-2.hubstack.net
https://menwiki.men/wiki/Buy_it_now_at_Online_Shop https://menwiki.men/wiki/Buy_it_now_at_Online_Shop
https://aryba.kg/user/foxcorn4/ aryba.kg
https://posteezy.com/quel-complement-alimentaire-choisir-pour-maigrir-guide-complet https://posteezy.com/
https://rosales-morgan-5.hubstack.net/perte-de-poids-medicaments-a-vendre-en-ligne rosales-morgan-5.hubstack.net
https://lovewiki.faith/wiki/Key_Factors_to_Consider_When_Buying_Garcinia_Cambogia_Extract https://lovewiki.faith/
https://fakenews.win/wiki/Kaufen_Online_Oxandrolon_Anavar https://fakenews.win/wiki/Kaufen_Online_Oxandrolon_Anavar
okprint.kz · February 16, 2026 at 7:11 pm
does crazy mass work
https://humanlove.stream/wiki/B_Avis_Une_capsule_efficace_pour_maigrir_Analyse https://humanlove.stream
https://skitterphoto.com/photographers/2223930/rafferty-mcleod https://skitterphoto.com/photographers/2223930/rafferty-mcleod
https://dokuwiki.stream/wiki/Les_meilleurs_probiotiques_pour_la_perte_de_poids_Avantages_et_supplments_PI https://dokuwiki.stream/
https://justpin.date/story.php?title=the-ultimate-guide-to-anavar-buying-prices-and-cycles-info https://justpin.date
https://securityholes.science/wiki/Ces_mdicaments_qui_font_maigrir_pour_vrai securityholes.science
https://p.mobile9.com/soilstamp3/ p.mobile9.com
https://yogicentral.science/wiki/N1_Appetitzgler_Kapseln_forte_42_St_kaufen_18295958 yogicentral.science
https://bowling-walther-2.technetbloggers.de/forte-pharma-xtraslim-chrono-60-pcs bowling-walther-2.technetbloggers.de
https://clashofcryptos.trade/wiki/Ozempic_Semaglutid_in_sterreich_mit_ChefarztBewilligung_erhltlich clashofcryptos.trade
https://yogaasanas.science/wiki/Is_Anavar_Legal_In_The_US_UK_Australia_New_Zealand_Canada https://yogaasanas.science
https://wifidb.science/wiki/Meilleur_complment_coupefaim_lavis_dune_pharmacienne_2026 wifidb.science
https://skitterphoto.com/photographers/2224409/bowling-bullard skitterphoto.com
https://www.youtube.com/redirect?q=https://border-radio.it/art/acquistare_testosterone_2.html https://www.youtube.com/redirect?q=https://border-radio.it/art/acquistare_testosterone_2.html
https://posteezy.com/quel-complement-alimentaire-choisir-pour-maigrir-guide-complet posteezy.com
https://pattern-wiki.win/wiki/Wirkstoff_zur_Gewichtszunahme_Anavar_Wie_und_in_welcher_Dosierung_fr_den_Sport_zu_nehmen_Kaufen_Online_zum_euros https://pattern-wiki.win/wiki/Wirkstoff_zur_Gewichtszunahme_Anavar_Wie_und_in_welcher_Dosierung_fr_den_Sport_zu_nehmen_Kaufen_Online_zum_euros
https://urlscan.io/result/019c327b-620b-77f2-83ae-37bf17f898f0/ urlscan.io
http://karayaz.ru/user/soilsalary4/ http://karayaz.ru
https://vaughn-bang-3.blogbright.net/appetitzugler-and-sattigungsmittel-produkte-gunstig-kaufen-auf-redcare-apotheke vaughn-bang-3.blogbright.net
References:
http://okprint.kz/user/soilsalary8/
firsturl.de · February 16, 2026 at 8:34 pm
otc steroid
http://downarchive.org/user/mittenpea8/ downarchive.org
https://covington-lauridsen.hubstack.net/complement-alimentaire-pour-maigrir-achat-en-ligne https://covington-lauridsen.hubstack.net
https://bom.so/HGuxHp https://bom.so/HGuxHp
https://firsturl.de/tg4Xqw8 https://firsturl.de/f8pTn1A
https://clashofcryptos.trade/wiki/Quel_est_le_Brlegraisse_le_plus_puissant https://clashofcryptos.trade
https://menwiki.men/wiki/36_Best_Fat_Burners_Supplements_for_Weight_Loss_in_2026 https://menwiki.men/
https://molchanovonews.ru/user/radarmakeup0/ molchanovonews.ru
https://dokuwiki.stream/wiki/21_raisons_pour_lesquelles_vous_ne_perdez_pas_de_poids_et_comment_y_remdier dokuwiki.stream
https://frank-moesgaard.blogbright.net/guide-complet-des-pilules-amaigrissantes-sur-ordonnance-et-en-vente-libre frank-moesgaard.blogbright.net
https://gustavsen-bang.thoughtlanes.net/quels-sont-les-medicaments-amaigrissants-disponibles-et-lequel-choisir gustavsen-bang.thoughtlanes.net
https://xypid.win/story.php?title=german-medico-anavar-kaufen xypid.win
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841071 gaiaathome.eu
https://yogaasanas.science/wiki/Anavar_for_Sale_A_Comprehensive_Guide_to_Choosing_Quality_Products yogaasanas.science
https://may22.ru/user/detailrice2/ https://may22.ru
https://www.instapaper.com/p/17442179 https://www.instapaper.com/
http://pattern-wiki.win/index.php?title=blackwellnoel6982 http://pattern-wiki.win/index.php?title=blackwellnoel6982
https://bookmark4you.win/story.php?title=die-besten-appetitzuegler-2026-vergleich-test-kaufempfehlung bookmark4you.win
https://p.mobile9.com/formclimb3/ https://p.mobile9.com/
https://www.udrpsearch.com/user/pushcable3 · February 16, 2026 at 9:31 pm
huge pills
https://funsilo.date/wiki/Glules_amincissantes_de_quoi_parleton funsilo.date
https://forum.dsapinstitute.org/forums/users/greekalley3/ forum.dsapinstitute.org
http://hikvisiondb.webcam/index.php?title=bishophay6492 http://hikvisiondb.webcam
https://swaay.com/u/sandirofirx54/about/ https://swaay.com/u/sandirofirx54/about
https://lovewiki.faith/wiki/Gelule_minceur_toutes_les_glules_pour_vous_aider_perdre_du_poids lovewiki.faith
https://intensedebate.com/people/targettaurus2 intensedebate.com
https://yogaasanas.science/wiki/Buy_Saxenda_UK_Online_Weight_Loss_Pen https://yogaasanas.science/wiki/Buy_Saxenda_UK_Online_Weight_Loss_Pen
https://wifidb.science/wiki/Welche_Appetitzgler_gibt_es_in_der_Apotheke_Rezeptfrei_sind_Folgende wifidb.science
https://hikvisiondb.webcam/wiki/Kaufen_Online_Oxandrolon_Anavar hikvisiondb.webcam
https://lovewiki.faith/wiki/March_des_pilules_amaigrissantes_sur_ordonnance_tendances_et_opportunits_2032 lovewiki.faith
https://yogicentral.science/wiki/Anavar yogicentral.science
https://graph.org/Where-to-Buy-Anavar-Online-Trusted-Sources-and-Price-Guide-02-06 https://graph.org/Where-to-Buy-Anavar-Online-Trusted-Sources-and-Price-Guide-02-06
https://douglas-crawford.federatedjournals.com/steroids-uk-uk-steroids-shop douglas-crawford.federatedjournals.com
https://briggs-moesgaard-4.technetbloggers.de/anavar-oxandrolone-benefits-side-effects-dosage-and-more-1770370937 https://briggs-moesgaard-4.technetbloggers.de/anavar-oxandrolone-benefits-side-effects-dosage-and-more-1770370937
https://fields-mcleod-2.blogbright.net/anavar-oxandrolone-1770375836 https://fields-mcleod-2.blogbright.net/anavar-oxandrolone-1770375836
https://elearnportal.science/wiki/Oxandrolone_Anavar_Online_Prescription_Delivery https://elearnportal.science/wiki/Oxandrolone_Anavar_Online_Prescription_Delivery
https://trade-britanica.trade/wiki/InDiva_System_glules_Prix_Effet_Avis_Pharmacie_Esquirol trade-britanica.trade
https://lovewiki.faith/wiki/Appetitzgler_Test_Vergleich_2026_TVzertifiziert https://lovewiki.faith
References:
https://www.udrpsearch.com/user/pushcable3
timeoftheworld.date · February 16, 2026 at 10:28 pm
oral testosterone steroids
https://justbookmark.win/story.php?title=oxandrolone-buy-oxandrolone-for-sale-online-in-germany-europe-at-best-prices justbookmark.win
https://botdb.win/wiki/Natrliche_Appetitzgler_Die_10_besten_Lebensmittel_gegen_Heihunger botdb.win
https://yogicentral.science/wiki/N1_Appetitzgler_Kapseln_forte_42_St_kaufen_18295958 https://yogicentral.science/wiki/N1_Appetitzgler_Kapseln_forte_42_St_kaufen_18295958
http://mozillabd.science/index.php?title=thiesenrode6518 mozillabd.science
http://hikvisiondb.webcam/index.php?title=mohammadandresen7421 hikvisiondb.webcam
https://molchanovonews.ru/user/bootsled3/ molchanovonews.ru
https://cameradb.review/wiki/Ce_que_vous_devez_savoir_sur_les_pilules_amaigrissantes cameradb.review
http://king-wifi.win//index.php?title=bowenhvidberg9621 http://king-wifi.win/
http://jobs.emiogp.com/author/trunkhorn6/ jobs.emiogp.com
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=140409 dubizzle.ca
https://rentry.co/ufdzwvxs rentry.co
https://instapages.stream/story.php?title=complement-alimentaire-pour-maigrir-top-7-des-produits-naturels instapages.stream
https://aryba.kg/user/nepalmakeup0/ aryba.kg
https://elclasificadomx.com/author/targetalley3/ https://elclasificadomx.com
http://jobs.emiogp.com/author/moveclimb9/ http://jobs.emiogp.com
https://www.udrpsearch.com/user/rabbitsalary2 https://www.udrpsearch.com/user/rabbitsalary2
https://swaay.com/u/eriatseofce21/about/ swaay.com
https://nerdgaming.science/wiki/Appetitzgler_Natrlich_Die_16_besten_Produkte_im_Vergleich https://nerdgaming.science
References:
https://timeoftheworld.date/wiki/Anavar_HiTech_Pharmaceuticals_180_Tabs
botdb.win · February 17, 2026 at 12:09 am
what are the side effects of dianabol
References:
https://botdb.win/wiki/Appetitzgler_Natrlich_Die_16_besten_Produkte_im_Vergleich
morphomics.science · February 17, 2026 at 12:10 am
ulisses jr steroids
References:
https://morphomics.science/wiki/Appetitzgler_Tropfen_online_kaufen_in_deiner_Medifit_Apotheke
https://yogaasanas.science · February 17, 2026 at 2:22 am
tren injection for sale
http://historydb.date/index.php?title=mcneilcramer9551 historydb.date
http://ezproxy.cityu.edu.hk/login?url=https://hegyvideksport.hu/pags/?buy_winstrol_4.html ezproxy.cityu.edu.hk
http://jobboard.piasd.org/author/radarpea1/ http://jobboard.piasd.org
https://telegra.ph/Anavar-02-06-2 telegra.ph
https://www.udrpsearch.com/user/boxclimb5 https://www.udrpsearch.com/
https://mcintosh-thornton-2.technetbloggers.de/buy-anavar-meditech-anavar-tablets-online https://mcintosh-thornton-2.technetbloggers.de/
https://nerdgaming.science/wiki/Appetitzgler_Natrlich_Die_16_besten_Produkte_im_Vergleich nerdgaming.science
http://king-wifi.win//index.php?title=macphersongreer7171 king-wifi.win
https://briggs-crawford.hubstack.net/the-complete-guide-to-buying-anavar-online https://briggs-crawford.hubstack.net/the-complete-guide-to-buying-anavar-online
https://donaldson-hermansen.blogbright.net/les-meilleures-pilules-amaigrissantes-classement-2024-top-20-1770386497 https://donaldson-hermansen.blogbright.net/
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841104 gaiaathome.eu
https://aryba.kg/user/trunkcorn1/ aryba.kg
https://rentry.co/c75nz9p9 rentry.co
https://frank-charles-3.mdwrite.net/les-meilleurs-complements-alimentaires-pour-booster-votre-perte-de-poids frank-charles-3.mdwrite.net
https://urlscan.io/result/019c325a-16d8-7599-b474-ee6a26c8c390/ https://urlscan.io/result/019c325a-16d8-7599-b474-ee6a26c8c390/
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.neukoelln-online.de/include/pages/testosteron_steigern_tabletten_2.html https://bbs.pku.edu.cn/v2/jump-to.php?url=https://www.neukoelln-online.de/include/pages/testosteron_steigern_tabletten_2.html
https://trade-britanica.trade/wiki/Prescription_weightloss_pills_medication_bupropion_HCl https://trade-britanica.trade/wiki/Prescription_weightloss_pills_medication_bupropion_HCl
https://yogaasanas.science/wiki/Anavar_50_Nakon_Medical_Kaufen_legale_online_zum_Preis_82_5/wiki/Anavar_10_mg_MultiPharm_kaufen_jetzt_online_bestellen_ab_127_00 yogaasanas.science
https://dreevoo.com · February 17, 2026 at 3:48 am
steroid online shop
https://telegra.ph/Where-to-Buy-Anavar-7-Reliable-Sources-for-2025-02-06 telegra.ph
https://rentry.co/gxpera74 https://rentry.co/gxpera74
https://cameradb.review/wiki/B_Avis_Une_capsule_efficace_pour_maigrir_Analyse cameradb.review
http://hikvisiondb.webcam/index.php?title=kejserrivera3537 http://hikvisiondb.webcam/index.php?title=kejserrivera3537
http://king-wifi.win//index.php?title=macphersongreer7171 king-wifi.win
https://aryba.kg/user/bootrice5/ aryba.kg
https://hikvisiondb.webcam/wiki/Semaglutid_Spritze_ohne_Rezept_kaufen_100_legal https://hikvisiondb.webcam
https://bookmarks4.men/story.php?title=warnung-appetitzuegler-test-2022-10-hersteller-im-vergleich bookmarks4.men
http://downarchive.org/user/foxtaurus7/ http://downarchive.org/
https://linkagogo.trade/story.php?title=juvamine-expert-brule-graisse-jour-et-nuit-contribue-a-bruler-les-graisses-eliminer-les-toxines-reduire-las https://linkagogo.trade
http://premiumdesignsinc.com/forums/user/porchjewel5/ premiumdesignsinc.com
https://scientific-programs.science/wiki/Die_9_besten_Appetitzgler_im_Vergleich_Erfahrungen_Test_Bewertung_2024 scientific-programs.science
https://timeoftheworld.date/wiki/Anavar_Ist_dieses_anabole_Steroid_sicher_zu_verwenden https://timeoftheworld.date/wiki/Anavar_Ist_dieses_anabole_Steroid_sicher_zu_verwenden
https://lovewiki.faith/wiki/Buy_Anavar_10mg_Online_Trusted_Oxandrolone_Tablets_in_USA https://lovewiki.faith/wiki/Buy_Anavar_10mg_Online_Trusted_Oxandrolone_Tablets_in_USA
https://bom.so/HGuxHp https://bom.so/HGuxHp
https://fakenews.win/wiki/The_Ultimate_Guide_to_Anavar_Buying_Prices_and_Cycles_Info fakenews.win
https://rentry.co/q5wdkhsx rentry.co
https://sciencewiki.science/wiki/Pilules_et_supplments_de_perte_de_poids https://sciencewiki.science/
References:
https://dreevoo.com/profile.php?pid=1068394
http://semdinlitesisat.eskisehirgocukduzeltme.com/user/italynerve6/ · February 17, 2026 at 5:00 am
what are the side effects of coming off steroids
https://menwiki.men/wiki/36_Best_Fat_Burners_Supplements_for_Weight_Loss_in_2026 https://menwiki.men
http://king-wifi.win//index.php?title=macphersongreer7171 king-wifi.win
https://dreevoo.com/profile.php?pid=1067824 dreevoo.com
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841071 https://gaiaathome.eu/
https://onlinevetjobs.com/author/rabbitclimb2/ onlinevetjobs.com
https://hikvisiondb.webcam/wiki/Kaufen_Online_Oxandrolon_Anavar https://hikvisiondb.webcam/wiki/Kaufen_Online_Oxandrolon_Anavar
http://king-wifi.win//index.php?title=bowenhvidberg9621 king-wifi.win
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316668 socialisted.org
https://p.mobile9.com/formclimb3/ https://p.mobile9.com/
https://rentry.co/zh8wamvw https://rentry.co/
https://fields-shannon-2.thoughtlanes.net/mdicaments-pour-maigrir-toutes-les-principales-pilules-minceur https://fields-shannon-2.thoughtlanes.net/
https://bom.so/6UKDGF bom.so
http://hikvisiondb.webcam/index.php?title=bennettschofield7879 http://hikvisiondb.webcam/
http://humanlove.stream//index.php?title=tobiasenregan0489 http://humanlove.stream//index.php?title=tobiasenregan0489
https://yogicentral.science/wiki/How_Much_Does_Contrave_Cost_A_Comprehensive_Guide_to_Pricing_Savings_MASI_Longevity_Science yogicentral.science
https://douglas-hermansen.mdwrite.net/sant-c3-a9-lagence-du-m-c3-a9dicament-alerte-sur-les-pilules-anti-ob-c3-a9sit-c3-a9-vendues-en-ligne douglas-hermansen.mdwrite.net
https://firsturl.de/tg4Xqw8 firsturl.de
http://jobs.emiogp.com/author/rabbitsled4/ jobs.emiogp.com
References:
http://semdinlitesisat.eskisehirgocukduzeltme.com/user/italynerve6/
https://gratisafhalen.be/ · February 17, 2026 at 5:54 am
medical steroids names
https://telegra.ph/Semaglutid-Ratgeber-mit-Infos-zum-Kauf-der-Tabletten-und-Spritze-02-06 telegra.ph
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316668 https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316668
https://lovebookmark.date/story.php?title=forte-pharma-xtraslim-max-draineur-complement-alimentaire-bruleur-de-graisses-a-boire-elimination-minceur-r https://lovebookmark.date
https://telegra.ph/36-Best-Fat-Burners-Supplements-for-Weight-Loss-in-2026-02-06 https://telegra.ph
https://duggan-clapp-2.federatedjournals.com/appetitzugler-test-2025-die-besten-produkte-im-vergleich-fur-effektive-gewichtsreduktion duggan-clapp-2.federatedjournals.com
https://molchanovonews.ru/user/troutfan0/ molchanovonews.ru
https://sciencewiki.science/wiki/Pilules_et_supplments_de_perte_de_poids https://sciencewiki.science/wiki/Pilules_et_supplments_de_perte_de_poids
http://ezproxy.cityu.edu.hk/login?url=https://hairplus.com.tr/wp-content/pgs/trenbolone_kopen_2.html http://ezproxy.cityu.edu.hk/login?url=https://hairplus.com.tr/wp-content/pgs/trenbolone_kopen_2.html
https://nerdgaming.science/wiki/Is_Anavar_Legal_in_the_U_S_and_Oklahoma nerdgaming.science
https://nerdgaming.science/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada https://nerdgaming.science/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada
https://empirekino.ru/user/forksalary7/ empirekino.ru
https://elearnportal.science/wiki/Les_pilules_pour_la_prise_de_poids_sontelles_sres_et_efficaces https://elearnportal.science
https://king-wifi.win/wiki/GERMAN_MEDICO_Anavar_kaufen https://king-wifi.win/wiki/GERMAN_MEDICO_Anavar_kaufen
https://onlinevetjobs.com/author/coilman3/ onlinevetjobs.com
https://p.mobile9.com/italytitle4/ https://p.mobile9.com/italytitle4
https://duggan-clapp-2.federatedjournals.com/appetitzugler-test-2025-die-besten-produkte-im-vergleich-fur-effektive-gewichtsreduktion https://duggan-clapp-2.federatedjournals.com
https://dreevoo.com/profile.php?pid=1068458 https://dreevoo.com
https://justbookmark.win/story.php?title=controle-du-poids-complements-alimentaires-les-plus-efficaces justbookmark.win
References:
https://gratisafhalen.be/author/targetrice5/
funsilo.date · February 17, 2026 at 7:30 am
testosterone enanthate powder legal
https://intensedebate.com/people/detailcable8 https://intensedebate.com/people/detailcable8
https://p.mobile9.com/formsalary2/ https://p.mobile9.com/
https://bom.so/6UKDGF https://bom.so
http://karayaz.ru/user/radarclick7/ http://karayaz.ru/user/radarclick7
https://graph.org/Viagra-ohne-Rezept-2026-Ist-das-legal-02-06 https://graph.org/Viagra-ohne-Rezept-2026-Ist-das-legal-02-06
https://humanlove.stream/wiki/Oxandrolon_Anavar_Hilma_Biocare_Fr_Definition_Kraft humanlove.stream
http://king-wifi.win//index.php?title=josephsenchung3718 king-wifi.win
https://opensourcebridge.science/wiki/Appetitzgler_Tropfen_online_kaufen_in_deiner_Medifit_Apotheke https://opensourcebridge.science/wiki/Appetitzgler_Tropfen_online_kaufen_in_deiner_Medifit_Apotheke
https://rentry.co/twkns3kn https://rentry.co
https://rentry.co/km5s4nfg rentry.co
http://pattern-wiki.win/index.php?title=rushhardin6040 http://pattern-wiki.win/index.php?title=rushhardin6040
https://rentry.co/gxpera74 rentry.co
https://www.instapaper.com/p/17442356 https://www.instapaper.com
https://p.mobile9.com/greekpea7/ https://p.mobile9.com/greekpea7/
https://berman-bowden.hubstack.net/anavar-for-sale-a-comprehensive-guide-to-choosing-quality-products-1770371588 berman-bowden.hubstack.net
https://wikimapia.org/external_link?url=https://sparshskinclinic.com/wp-content/pgs/eetlustremmers.html wikimapia.org
https://sciencewiki.science/wiki/Appetitzgler_online_kaufen_Sttigungskapseln_HSNstore https://sciencewiki.science/wiki/Appetitzgler_online_kaufen_Sttigungskapseln_HSNstore
http://hikvisiondb.webcam/index.php?title=bishophay6492 http://hikvisiondb.webcam
References:
https://funsilo.date/wiki/Pilule_nos_astuces_minceur_contre_la_prise_de_poids
av 在线 · February 17, 2026 at 8:01 am
This is a topic which is close to my heart… Best wishes! Where are your contact details though?
https://morphomics.science/wiki/Ozempic_kopen_zonder_recept · February 17, 2026 at 9:05 am
how much does a steroid cycle cost
https://skitterphoto.com/photographers/2224887/mcintosh-thornton https://skitterphoto.com/
https://botdb.win/wiki/Wegovy_aus_Holland_Semaglutid_Rezept_und_Versand https://botdb.win
http://downarchive.org/user/trunkalley0/ downarchive.org
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=140517 http://dubizzle.ca/
http://muhaylovakoliba.1gb.ua/user/rabbitclick5/ muhaylovakoliba.1gb.ua
http://downarchive.org/user/malletjewel6/ downarchive.org
http://pattern-wiki.win/index.php?title=caseyleslie8835 http://pattern-wiki.win/
https://mcintosh-brun-3.mdwrite.net/gelules-amincissantes-de-quoi-parle-t-on-1770368661 mcintosh-brun-3.mdwrite.net
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841364 https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841364
https://lovewiki.faith/wiki/Gelule_minceur_toutes_les_glules_pour_vous_aider_perdre_du_poids lovewiki.faith
https://funsilo.date/wiki/Anavar_Erfahrungen_Zyklus_Anavar_Frauen_Steroid_2026 funsilo.date
https://onlinevetjobs.com/author/formmark5/ https://onlinevetjobs.com/author/formmark5/
http://historydb.date/index.php?title=mcneilcramer9551 http://historydb.date/index.php?title=mcneilcramer9551
https://skitterphoto.com/photographers/2224172/yilmaz-moesgaard https://skitterphoto.com/photographers/2224172/yilmaz-moesgaard
http://mozillabd.science/index.php?title=gordonbeasley0739 mozillabd.science
https://albrektsen-walther.mdwrite.net/androchem-laboratories-anavar-10mg-100tab-steroide-kaufen-in-deutschland https://albrektsen-walther.mdwrite.net/androchem-laboratories-anavar-10mg-100tab-steroide-kaufen-in-deutschland
http://king-wifi.win//index.php?title=macphersongreer7171 http://king-wifi.win//index.php?title=macphersongreer7171
https://dreevoo.com/profile.php?pid=1067290 dreevoo.com
References:
https://morphomics.science/wiki/Ozempic_kopen_zonder_recept
https://justbookmark.win · February 17, 2026 at 9:58 am
winnie steroid
https://bom.so/zwI9r0 https://bom.so/zwI9r0
https://p.mobile9.com/coilalley0/ p.mobile9.com
https://nerdgaming.science/wiki/Ozempic_Apotheke_Kosten_Rezept_Verfgbarkeit_Bestellung nerdgaming.science
https://www.instapaper.com/p/17441951 instapaper.com
https://rentry.co/mc6k4f6v rentry.co
https://rentry.co/qb88dw7m rentry.co
https://yogaasanas.science/wiki/Top_10_Companies_in_the_Garcinia_Cambogia_Extract_Market_2026_Industry_Leaders_Fueling_the_Global_Wellness_Boom yogaasanas.science
https://covington-lauridsen.hubstack.net/complement-alimentaire-pour-maigrir-achat-en-ligne covington-lauridsen.hubstack.net
https://fields-case-2.federatedjournals.com/buy-anavar-oxandrolone-10mg-x-100-tabs-uk fields-case-2.federatedjournals.com
https://funsilo.date/wiki/Anavar_Review_Benefits_Risks_and_Everything_You_Need_to_Know funsilo.date
https://elearnportal.science/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada elearnportal.science
https://king-wifi.win/wiki/Mdicaments_pour_maigrir_toutes_les_principales_pilules_minceur king-wifi.win
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=317036 https://socialisted.org/market/index.php?page=user&action=pub_profile&id=317036
https://trade-britanica.trade/wiki/Key_Factors_to_Consider_When_Buying_Garcinia_Cambogia_Extract trade-britanica.trade
https://intensedebate.com/people/rabbitfan0 intensedebate.com
https://wifidb.science/wiki/29_Best_Diet_Pills_for_Weight_Loss_in_2026_That_Actually_Work https://wifidb.science/
https://aryba.kg/user/foxcorn4/ https://aryba.kg/
https://graph.org/Saxenda-aus-Holland–Saxenda-Rezept-und-Versand-02-06 https://graph.org/Saxenda-aus-Holland–Saxenda-Rezept-und-Versand-02-06
References:
https://justbookmark.win/story.php?title=die-10-besten-appetitzuegler-pillen-zur-kontrolle-von-heisshunger
urlscan.io · February 17, 2026 at 10:58 am
dbol steroid pills for sale
https://urlscan.io/result/019c325a-16d8-7599-b474-ee6a26c8c390/ https://urlscan.io/result/019c32d9-dfc2-772d-a2bc-3e50ba07cc5d/
https://prpack.ru/user/radarskiing1/ prpack.ru
https://timeoftheworld.date/wiki/3_mdicaments_pour_perdre_du_poids_au_Canada timeoftheworld.date
https://cameradb.review/wiki/Thaiger_Pharma_Xandrol_10_mg_50_Tabletten_Anavar_Order_Now_for_price_70_00_Pounds cameradb.review
https://wikimapia.org/external_link?url=https://gastouderbureauheuvelrug.nl/wp-content/pages/testosteron_pillen.html wikimapia.org
https://onlinevetjobs.com/author/radarmark4/ onlinevetjobs.com
https://livebookmark.stream/story.php?title=understanding-anavar-and-its-authenticity livebookmark.stream
http://jobboard.piasd.org/author/porchcable6/ jobboard.piasd.org
https://rentry.co/qb88dw7m rentry.co
https://aryba.kg/user/pajamataurus2/ https://aryba.kg/
https://onlinevetjobs.com/author/rabbitclimb2/ onlinevetjobs.com
https://urlscan.io/result/019c3321-3a8a-712f-a252-e234b229f8ac/ urlscan.io
http://ezproxy.cityu.edu.hk/login?url=https://tb-onderdelen.nl/test/pgs/testosteron_pillen_2.html ezproxy.cityu.edu.hk
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1841140 gaiaathome.eu
http://ezproxy.cityu.edu.hk/login?url=https://goudaspoorzone.nl/wp-content/pgs/clenbuterol_kopen_1.html http://ezproxy.cityu.edu.hk
http://ezproxy.cityu.edu.hk/login?url=https://ecampania.it/blog/acquistare_oxandrolone_anavar.html ezproxy.cityu.edu.hk
https://empirekino.ru/user/pajamagauge5/ https://empirekino.ru/user/pajamagauge5/
https://bowling-walther-2.technetbloggers.de/forte-pharma-xtraslim-chrono-60-pcs https://bowling-walther-2.technetbloggers.de
https://www.youtube.com · February 17, 2026 at 12:37 pm
strongest legal steroid on the market
http://jobboard.piasd.org/author/coilcomic7/ http://jobboard.piasd.org
https://botdb.win/wiki/Anavar_Kaufen botdb.win
https://skitterphoto.com/photographers/2224684/douglas-petersen skitterphoto.com
https://bookmarkstore.download/story.php?title=oxandrolone-buy-oxandrolone-for-sale-online-in-germany-europe-at-best-prices-7 bookmarkstore.download
https://www.youtube.com/redirect?q=https://fleuriste-toulouse.fr/pages/trenbolone_achat.html/redirect?q=https://universalkinesiology.it/art/acquistare_testosterone.html http://www.youtube.com
https://freebookmarkstore.win/story.php?title=anavar-review-benefits-risks-and-everything-you-need-to-know https://freebookmarkstore.win/story.php?title=anavar-review-benefits-risks-and-everything-you-need-to-know
http://historydb.date/index.php?title=conwaymcconnell0472 http://historydb.date/index.php?title=conwaymcconnell0472
https://intensedebate.com/people/targettaurus2 intensedebate.com
https://briggs-crawford-5.blogbright.net/abmagerungsmittel-appetitzugler-medikamente-wirkstoffe-and-anwendungsgebiete https://briggs-crawford-5.blogbright.net/
http://lideritv.ge/user/bootsharon6/ http://lideritv.ge
https://elearnportal.science/wiki/Oxandrolone_Anavar_Online_Prescription_Delivery elearnportal.science
https://www.udrpsearch.com/user/boxclimb5 https://www.udrpsearch.com/user/boxclimb5
https://pediascape.science/wiki/Saxenda_ohne_Rezept_online_bestellen_kostenlose_express_Versand_registrierte_EU_Versand_Apotheken_Online_Arzneimittel_per_Ferndiagnose_bestellen pediascape.science
https://vaughn-church.blogbright.net/jetzt-im-online-shop-kaufen vaughn-church.blogbright.net
https://nhadat24.org/author/columnheart4 nhadat24.org
https://www.udrpsearch.com/user/rabbitskiing6 http://www.udrpsearch.com
https://www.24propertyinspain.com/user/profile/1371059 https://www.24propertyinspain.com/
https://xypid.win/story.php?title=german-medico-anavar-kaufen https://xypid.win/story.php?title=german-medico-anavar-kaufen
Walterdrono · February 17, 2026 at 2:49 pm
https://djaccesorios.com/alrededor-del-dia-de-la-nutriologa-asi-como-el-nutriologo-el-imss-destaca-el-papel-estrategico-con-prevencion-sobre-enfermedades-cronicas
swaay.com · February 17, 2026 at 4:21 pm
trenbolone reddit
References:
https://swaay.com/u/machillubib12/about/
https://molchanovonews.ru · February 17, 2026 at 4:25 pm
steroid cycle transformation
References:
https://molchanovonews.ru/user/mittencomic7/
australianonlinecasino · February 17, 2026 at 7:39 pm
海外华人必备的iyf平台,提供最新高清电影、电视剧,无广告观看体验。
king-wifi.win · February 17, 2026 at 11:54 pm
what cause abuse
References:
http://king-wifi.win//index.php?title=briggsoneil3749
scientific-programs.science · February 18, 2026 at 2:13 am
what is gear bodybuilding
References:
https://scientific-programs.science/wiki/Anavar_10_Pharmaqo_Online_kaufen_Preis_129_00_euros_in_Deutschland
australiaonlinecasinos · February 18, 2026 at 1:54 pm
Online casino Australia real money easy withdrawal – fast cashouts
ทดลองเล่นสล็อต pg · February 19, 2026 at 3:17 am
สล็อตเว็บตรง
แพลตฟอร์ม TKBNEKO ทำงานเป็นระบบเกมออนไลน์ ที่ ออกแบบโครงสร้างโดยยึดพฤติกรรมผู้ใช้เป็นศูนย์กลาง. หน้าเว็บหลัก ประกาศตัวเลขชัดเจนทันที: ฝากขั้นต่ำ 1 บาท, ถอนขั้นต่ำ 1 บาท, เวลาฝากประมาณ 3 วินาที, และ ยอดถอนไม่มีเพดาน. ตัวเลขเหล่านี้กำหนดภาระของระบบโดยตรง เพราะเมื่อ กำหนดขั้นต่ำต่ำ ระบบต้อง รับรายการฝากถอนจำนวนมากที่มียอดเล็ก และต้อง ตัดยอดและเติมเครดิตแบบทันที. หาก เครดิตเข้าไม่ทันในไม่กี่วินาที ผู้ใช้จะ ทำรายการซ้ำ ทำให้เกิด รายการซ้อน และ ดันโหลดระบบขึ้นทันที.
การเติมเงินด้วยการสแกน QR ตัดขั้นตอนการกรอกข้อมูลและการแนบสลิป. เมื่อผู้ใช้ สแกนคิวอาร์ ธนาคารจะส่งสถานะการชำระกลับมายังระบบผ่าน API. จากนั้น backend จะ จับคู่ธุรกรรมกับ user ID และ เติมเครดิตเข้า wallet. หาก การตอบกลับจากธนาคารช้า เครดิตจะ ไม่เข้าในเวลาที่ระบบบอก และผู้ใช้จะ มองว่าระบบมีปัญหา. ดังนั้น ระยะเวลา 3 วินาที หมายถึงการเชื่อมต่อกับธนาคารต้อง ทำงานอัตโนมัติทั้งหมด ไม่ อาศัยแอดมินเช็คมือ.
การรองรับหลายธนาคาร เช่น KBank, ธนาคารกรุงเทพ, KTB, กรุงศรี, Siam Commercial Bank, ซีไอเอ็มบี ไทย รวมถึง ทรูมันนี่ วอลเล็ท ทำให้ระบบต้อง รับ callback หลายต้นทาง. แต่ละเจ้าใช้ฟอร์แมตข้อมูลและความหน่วงต่างกัน. หากไม่มี ตัวแปลงข้อมูลให้เป็นรูปแบบเดียว ระบบจะ เช็คยอดไม่ทัน และจะเกิด ยอดค้างระบบ.
หมวดหมู่เกม ถูกแยกเป็น สล็อตออนไลน์, เกมสด, กีฬา และ ยิงปลา. การแยกหมวด ลดการค้นหาที่ต้องลากทั้งระบบ และ ควบคุมการส่งทราฟฟิกไปยังผู้ให้บริการแต่ละราย. สล็อต มัก เชื่อมต่อผ่าน session API ส่วน เกมสด ใช้ สตรีมภาพแบบเรียลไทม์. หาก หลุดเซสชัน ผู้เล่นจะ ถูกตัดออกจากเกมทันที. ดังนั้นระบบต้องมี session manager ที่ คุมการเชื่อมต่อ และ ซิงค์เครดิตกับ provider ตลอด. หาก ซิงค์พลาด เครดิตผู้เล่นกับผลเกมจะ ไม่ตรงกัน.
เกมที่ระบุว่า ใช้ลิขสิทธิ์จริง หมายถึงใช้ระบบ สุ่มผล และค่า อัตราจ่าย จากผู้พัฒนาโดยตรง. ผลลัพธ์แต่ละรอบถูก คำนวณจากฝั่ง provider ไม่ใช่จากฝั่งเว็บ. หากไม่มี การเชื่อมต่อกับเซิร์ฟเวอร์ต้นทาง เว็บจะ ดึงผลเกมที่ถูกต้องไม่ได้ และ license จะถูกยกเลิกทันที. การมี การรับรอง จึง ผูกกับโครงสร้างการส่งข้อมูล ไม่ใช่ แค่คำบนหน้าเว็บ.
ระบบถอนที่ ไม่มีจำกัด เชิงการสื่อสารยังต้องมีโมดูล risk control เช่น ตรวจสอบบัญชีซ้ำ, พฤติกรรมผิดปกติ, และ เงื่อนไข turnover. หากไม่มีการตรวจสอบเหล่านี้ ผู้ใช้สามารถ สร้างบัญชีหลายบัญชี เพื่อ เอาโบนัส และ ถอนเงินออกเร็ว.
ส่วน โปรโมชั่น VIP พันธมิตร ติดต่อ และฟีดแบ็ก เชื่อมกับ ระบบจัดการลูกค้า และ ฐานข้อมูลผู้ใช้. ส่วน พันธมิตร ใช้เก็บ โค้ดอ้างอิง เพื่อ คำนวณค่าคอมมิชชั่น. หากไม่มีระบบนี้ จะ ติดตามแหล่งที่มาของผู้ใช้ไม่ได้. แบบฟอร์มฟีดแบ็ก ใช้เก็บ ข้อผิดพลาดจริงจากผู้ใช้. หากไม่มีข้อมูลนี้ ปัญหา latency หรือ การใช้งาน จะ แก้ไม่ทัน.
โครงสร้างทั้งหมด เชื่อมกันเป็นสายเดียว: สถานะธุรกรรมเข้ามาที่ backend, backend อัปเดตเครดิต แล้ว ซิงค์ไปยัง provider. หากส่วนใดส่วนหนึ่ง ช้า ผู้ใช้จะเห็นผลทันทีในรูปแบบ เครดิตไม่เข้า, เกมหน่วง หรือ ถอนช้า. ในแพลตฟอร์มลักษณะนี้ API ต้องนิ่งและ session ต้องไม่หลุด คือสิ่งที่ ตัดสินว่าผู้ใช้จะอยู่หรือย้ายออก.
สล็อต · February 19, 2026 at 9:22 pm
ทดลองเล่นสล็อต pg
TKBNEKO เป็นแพลตฟอร์มเกมออนไลน์ ที่ ออกแบบโครงสร้างโดยยึดพฤติกรรมผู้ใช้เป็นศูนย์กลาง. หน้าแรก ประกาศตัวเลขชัดเจนทันที: ขั้นต่ำฝาก 1 บาท, ขั้นต่ำถอน 1 บาท, เครดิตเข้าโดยเฉลี่ยราว 3 วินาที, และ ไม่จำกัดยอดถอน. ตัวเลขเหล่านี้กำหนดภาระของระบบโดยตรง เพราะเมื่อ ตั้งขั้นต่ำไว้ต่ำมาก ระบบต้อง รองรับธุรกรรมจำนวนมากขนาดเล็ก และต้อง ตัดยอดและเติมเครดิตแบบทันที. หาก การยืนยันเครดิตใช้เวลานานเกินไม่กี่วินาที ผู้ใช้จะ ทำรายการซ้ำ ทำให้เกิด รายการซ้อน และ เพิ่มโหลดฝั่งเซิร์ฟเวอร์ทันที.
การฝากผ่าน QR Code ตัดขั้นตอนการกรอกข้อมูลและการแนบสลิป. เมื่อผู้ใช้ สแกนคิวอาร์ ธนาคารจะส่งสถานะการชำระกลับมายังระบบผ่าน API. จากนั้น backend จะ ผูกธุรกรรมเข้ากับบัญชีผู้ใช้ และ เพิ่มเครดิตเข้า wallet. หาก API ตอบสนองช้า เครดิตจะ ไม่เข้าในเวลาที่ระบบบอก และผู้ใช้จะ ถือว่าระบบไม่เสถียร. ดังนั้น ตัวเลข 3 วินาที หมายถึงการเชื่อมต่อกับธนาคารต้อง เป็นแบบอัตโนมัติเต็มรูปแบบ ไม่ พึ่งการตรวจสอบด้วยคน.
การรองรับหลายธนาคาร เช่น KBank, ธนาคารกรุงเทพ, KTB, กรุงศรี, Siam Commercial Bank, ซีไอเอ็มบี ไทย รวมถึง TrueMoney Wallet ทำให้ระบบต้อง จัดการ webhook หลายแหล่ง. แต่ละธนาคารมีรูปแบบข้อมูลและเวลาตอบสนองต่างกัน. หากไม่มี โมดูลแปลงข้อมูลให้เป็นมาตรฐานเดียว ระบบจะ เช็คยอดไม่ทัน และจะเกิด ยอดค้างระบบ.
หมวดเกม ถูกแยกเป็น สล็อต, เกมสด, เดิมพันกีฬา และ ยิงปลา. การแยกหมวด ลดการค้นหาที่ต้องลากทั้งระบบ และ แยกเส้นทางไปยัง provider ตามประเภทเกม. เกมสล็อต มัก ทำงานผ่าน session API ส่วน เกมสด ใช้ สตรีมแบบสด. หาก หลุดเซสชัน ผู้เล่นจะ หลุดจากโต๊ะทันที. ดังนั้นระบบต้องมี ตัวจัดการ session ที่ รักษาการเชื่อมต่อ และ ซิงค์เครดิตกับ provider ภายนอกตลอดเวลา. หาก ซิงค์ล้มเหลว เครดิตผู้เล่นกับผลเกมจะ ไม่ตรงกัน.
เกมที่ระบุว่า เป็นลิขสิทธิ์แท้ หมายถึงใช้ระบบ สุ่มผล และค่า RTP จากผู้พัฒนาโดยตรง. ผลลัพธ์แต่ละรอบถูก ประมวลผลจากเซิร์ฟเวอร์ผู้ให้บริการ ไม่ใช่จากฝั่งเว็บ. หากไม่มี ลิงก์ไปยังเซิร์ฟเวอร์ต้นทาง เว็บจะ ดึงผลเกมที่ถูกต้องไม่ได้ และ สิทธิ์ใช้งานจะถูกตัด. การมี ใบรับรอง จึง ผูกกับโครงสร้างการส่งข้อมูล ไม่ใช่ แค่ข้อความแสดงบนหน้าเว็บ.
ระบบถอนที่ ไม่มีจำกัด เชิงการสื่อสารยังต้องมีโมดูล risk control เช่น เช็คบัญชีซ้ำ, พฤติกรรมผิดปกติ, และ เงื่อนไขเทิร์นโอเวอร์. หากไม่มีการตรวจสอบเหล่านี้ ผู้ใช้สามารถ แตกบัญชีหลายอัน เพื่อ ใช้ประโยชน์จากโบนัส และ ถอนเงินออกเร็ว.
ส่วน โปรโมชั่น VIP พันธมิตร ติดต่อ และฟีดแบ็ก เชื่อมกับ ระบบ CRM และ ฐานข้อมูลผู้เล่น. ส่วน Affiliate ใช้เก็บ โค้ดอ้างอิง เพื่อ คำนวณค่าคอมมิชชั่น. หากไม่มีระบบนี้ จะ ติดตามแหล่งที่มาของผู้ใช้ไม่ได้. ฟอร์มข้อเสนอแนะ ใช้เก็บ error จริงจากผู้ใช้. หากไม่มีข้อมูลนี้ ปัญหา ความหน่วง หรือ การใช้งาน จะ แก้ไม่ทัน.
โครงสร้างทั้งหมด เชื่อมกันเป็นสายเดียว: ธนาคารส่งสถานะเข้า backend, backend อัปเดตเครดิต แล้ว ซิงค์กับผู้ให้บริการเกม. หากส่วนใดส่วนหนึ่ง หน่วง ผู้ใช้จะเห็นผลทันทีในรูปแบบ เครดิตไม่เข้า, เกมค้าง หรือ ถอนช้า. ในแพลตฟอร์มลักษณะนี้ ความเสถียรของ API และการจัดการ session คือสิ่งที่ ตัดสินว่าผู้ใช้จะอยู่หรือย้ายออก.
bitpoll.de · February 21, 2026 at 8:11 am
deca durabolin cycle for beginners
References:
https://bitpoll.de/poll/RvIFUhWGd1/
https://jasminsideenreich.de · February 21, 2026 at 1:26 pm
monkey money
References:
https://jasminsideenreich.de/Blog/index.php/;focus=STRATP_com_cm4all_wdn_Flatpress_7099662&frame=STRATP_com_cm4all_wdn_Flatpress_7099662?x=entry:entry220227-185612%3Bcomments:1
https://jasminsideenreich.de/ · February 21, 2026 at 2:17 pm
hollywood casino st louis
References:
https://jasminsideenreich.de/Blog/index.php/;focus=STRATP_com_cm4all_wdn_Flatpress_7099662&frame=STRATP_com_cm4all_wdn_Flatpress_7099662?x=entry:entry200626-092002%3Bcomments:1
sommer-architekt-warstein.de · February 21, 2026 at 2:50 pm
roulette wheel layout
References:
https://www.sommer-architekt-warstein.de/VPB-Expertenrat;focus=TKOMSI_com_cm4all_wdn_Flatpress_22800952&frame=TKOMSI_com_cm4all_wdn_Flatpress_22800952?x=entry:entry240910-094339%3Bcomments:1
pg slot · February 21, 2026 at 9:15 pm
pg slot
แพลตฟอร์ม TKBNEKO ทำงานเป็นระบบเกมออนไลน์ ที่ ออกแบบโครงสร้างโดยยึดพฤติกรรมผู้ใช้เป็นศูนย์กลาง. หน้าเว็บหลัก ประกาศตัวเลขชัดเจนทันที: ฝากขั้นต่ำ 1 บาท, ขั้นต่ำถอน 1 บาท, เครดิตเข้าโดยเฉลี่ยราว 3 วินาที, และ ไม่จำกัดยอดถอน. ตัวเลขพวกนี้เปลี่ยนโหลดระบบทันที เพราะเมื่อ กำหนดขั้นต่ำต่ำ ระบบต้อง รองรับธุรกรรมจำนวนมากขนาดเล็ก และต้อง ประมวลผลแบบเรียลไทม์. หาก การยืนยันเครดิตใช้เวลานานเกินไม่กี่วินาที ผู้ใช้จะ กดซ้ำ ทำให้เกิด รายการซ้อน และ ดันโหลดระบบขึ้นทันที.
การเติมเงินด้วยการสแกน QR ลดขั้นตอนที่ต้องพิมพ์ข้อมูลหรือส่งสลิป. เมื่อผู้ใช้ สแกนคิวอาร์ ธนาคารจะส่งสถานะการชำระกลับมายังระบบผ่าน API. จากนั้น backend จะ ผูกธุรกรรมเข้ากับบัญชีผู้ใช้ และ เติมเครดิตเข้า wallet. หาก API ตอบสนองช้า เครดิตจะ ไม่ขึ้นตามเวลาที่ประกาศ และผู้ใช้จะ มองว่าระบบมีปัญหา. ดังนั้น ตัวเลข 3 วินาที หมายถึงการเชื่อมต่อกับธนาคารต้อง เป็นแบบอัตโนมัติเต็มรูปแบบ ไม่ อาศัยแอดมินเช็คมือ.
การรองรับหลายธนาคาร เช่น Kasikornbank, ธนาคารกรุงเทพ, Krung Thai Bank, Krungsri, Siam Commercial Bank, ซีไอเอ็มบี ไทย รวมถึง TrueMoney Wallet ทำให้ระบบต้อง รับ callback หลายต้นทาง. แต่ละธนาคารมีรูปแบบข้อมูลและเวลาตอบสนองต่างกัน. หากไม่มี โมดูลแปลงข้อมูลให้เป็นมาตรฐานเดียว ระบบจะ ยืนยันยอดได้ช้า และจะเกิด ยอดค้างระบบ.
หมวดหมู่เกม ถูกแยกเป็น สล็อต, คาสิโนสด, กีฬา และ ยิงปลา. การแยกหมวด ลดการค้นหาที่ต้องลากทั้งระบบ และ ควบคุมการส่งทราฟฟิกไปยังผู้ให้บริการแต่ละราย. สล็อต มัก เชื่อมต่อผ่าน session API ส่วน คาสิโนสด ใช้ สตรีมแบบสด. หาก หลุดเซสชัน ผู้เล่นจะ ถูกตัดออกจากเกมทันที. ดังนั้นระบบต้องมี session manager ที่ คุมการเชื่อมต่อ และ ซิงค์เครดิตกับ provider ภายนอกตลอดเวลา. หาก ซิงค์ล้มเหลว เครดิตผู้เล่นกับผลเกมจะ ไม่แมตช์.
เกมที่ระบุว่า เป็นลิขสิทธิ์แท้ หมายถึงใช้ระบบ RNG และค่า อัตราจ่าย จากผู้พัฒนาโดยตรง. ผลลัพธ์แต่ละรอบถูก คำนวณจากฝั่ง provider ไม่ใช่จากฝั่งเว็บ. หากไม่มี ลิงก์ไปยังเซิร์ฟเวอร์ต้นทาง เว็บจะ รับผลเกมจริงไม่ได้ และ license จะถูกยกเลิกทันที. การมี ใบรับรอง จึง ผูกกับโครงสร้างการส่งข้อมูล ไม่ใช่ แค่คำบนหน้าเว็บ.
ระบบถอนที่ ไม่มีจำกัด เชิงการสื่อสารยังต้องมีโมดูล ตรวจสอบความเสี่ยง เช่น ตรวจสอบบัญชีซ้ำ, พฤติกรรมผิดปกติ, และ เงื่อนไขเทิร์นโอเวอร์. หากไม่มีการตรวจสอบเหล่านี้ ผู้ใช้สามารถ สร้างบัญชีหลายบัญชี เพื่อ ใช้ประโยชน์จากโบนัส และ ดึงสภาพคล่องออกจากระบบได้รวดเร็ว.
เมนู โปรโมชั่น VIP พันธมิตร ติดต่อเรา และข้อเสนอแนะ เชื่อมกับ ระบบ CRM และ ฐานข้อมูลผู้เล่น. ส่วน พันธมิตร ใช้เก็บ โค้ดอ้างอิง เพื่อ คิดคอมมิชชั่น. หากไม่มีระบบนี้ จะ ติดตามแหล่งที่มาของผู้ใช้ไม่ได้. แบบฟอร์มฟีดแบ็ก ใช้เก็บ error จริงจากผู้ใช้. หากไม่มีข้อมูลนี้ ปัญหา latency หรือ UX จะ แก้ไม่ทัน.
โครงสร้างทั้งหมด ทำงานเป็นระบบเดียว: ธนาคารส่งสถานะเข้า backend, backend อัปเดตเครดิต แล้ว ซิงค์ไปยัง provider. หากส่วนใดส่วนหนึ่ง ช้า ผู้ใช้จะเห็นผลทันทีในรูปแบบ เครดิตไม่เข้า, เกมค้าง หรือ ถอนล่าช้า. ในแพลตฟอร์มลักษณะนี้ API ต้องนิ่งและ session ต้องไม่หลุด คือสิ่งที่ ตัดสินว่าผู้ใช้จะอยู่หรือย้ายออก.
bom.so · February 22, 2026 at 5:19 am
el dorado casino shreveport
References:
https://bom.so/FaHz2G
linkagogo.trade · February 22, 2026 at 5:47 am
online slot games
References:
https://linkagogo.trade/story.php?title=instant-casino-%E1%90%89-offizielles-online-casino-deutschland-schnelle-auszahlungen-bonusangebote
https://avtovoprosi.ru/ · February 22, 2026 at 6:12 am
meadowlands casino
References:
https://avtovoprosi.ru/user/bookquartz7
p.mobile9.com · February 22, 2026 at 7:00 am
solaire casino
References:
https://p.mobile9.com/bookparty7/
downarchive.org · February 22, 2026 at 7:09 am
montreal casino
References:
http://downarchive.org/user/hubcapguilty8/
sommer-architekt-warstein.de · February 22, 2026 at 8:49 am
how to tell if someone uses steroids
References:
https://www.sommer-architekt-warstein.de/VPB-Expertenrat;focus=TKOMSI_com_cm4all_wdn_Flatpress_22800952&frame=TKOMSI_com_cm4all_wdn_Flatpress_22800952?x=entry:entry210615-143953%3Bcomments:1
https://gpsites.stream/story.php?title=100-no-deposit-bonuses-at-australian-online-casinos-in-2026 · February 22, 2026 at 9:38 am
canberra casino
References:
https://gpsites.stream/story.php?title=100-no-deposit-bonuses-at-australian-online-casinos-in-2026
https://graph.org/ · February 22, 2026 at 10:44 am
canadian online casino
References:
https://graph.org/PayID-Pokies-No-Deposit-Bonus-M99AU-Australia-No-Deposit-Required-Just-Register-and-Play-02-22
uvs2.net · February 22, 2026 at 11:37 am
big fish casino online
References:
http://uvs2.net/index.php/user/suitsmash57
mensvault.men · February 22, 2026 at 12:29 pm
poker bonus no deposit
References:
https://mensvault.men/story.php?title=free-100-pokies-no-deposit-sign-up-bonus-reviews-read-customer-service-reviews-of-free100pokiesnodeposit-com
https://dreevoo.com · February 22, 2026 at 1:13 pm
blackjack club
References:
https://dreevoo.com/profile.php?pid=1160537
pg slot · February 22, 2026 at 11:35 pm
pg slot
PG Slot แพลตฟอร์มเกมสล็อตยอดนิยม ใช้งานง่าย ฝากถอนรวดเร็ว
คำค้นหา PG Slot กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน ภาพและเอฟเฟกต์ ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ผลิตโดยค่ายมาตรฐาน ที่รองรับการเล่นทั้งบน มือถือ และ พีซี
ความโดดเด่น ของ สล็อต PG
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เข้าเกมไว เล่นผ่าน ระบบเว็บ และรองรับ ทั้ง iOS และ Android เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน Browser ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ เอฟเฟกต์ 3 มิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สมจริง
คุณสมบัติหลักของเกม PG Slot ได้แก่
ระบบโบนัสและฟรีสปินหลากหลายรูปแบบ
ระบบตัวคูณ
โหมดทดลองเล่นฟรี
ใช้งานภาษาไทยง่าย
ฝากถอนง่าย ทันใจ
แพลตฟอร์ม PG Slot ส่วนใหญ่รองรับ การฝาก-ถอน อัตโนมัติ 24 ชั่วโมง ขั้นต่ำเริ่มต้นเพียง 10 บาท ขึ้นอยู่กับ เงื่อนไขของเว็บไซต์ การทำรายการใช้เวลา รวดเร็วมาก ผ่าน สแกน QR หรือระบบ ธนาคารบนมือถือ ทำให้ธุรกรรมเป็นไปอย่าง ต่อเนื่อง
หมวดเกมฮิต ใน PG Slot
เกม สล็อต PG มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม ลุยด่าน
ธีม ความมั่งคั่ง
ธีม สัตว์และธรรมชาติ
หลายคนชอบเกมที่โบนัสเข้าไว พร้อมระบบ ฟีเจอร์พิเศษ และ อัตราการจ่ายที่สูง เหมาะกับทั้ง คนเพิ่งเล่น และ สายสล็อตจริงจัง
ความปลอดภัย
สล็อต PG พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล ระบบสุ่มมาตรฐาน เพื่อให้ผลลัพธ์ ยุติธรรม แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ระบบดูแลข้อมูล
โดยภาพรวม
pg slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน ระบบลื่นไหล และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ทันที ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ผู้เล่นทุกสไตล์ ในโลกของเกมสล็อตออนไลน์
https://homedecorideas24.co.uk · February 23, 2026 at 8:16 am
online casino vegas
References:
https://homedecorideas24.co.uk/nordic-prime-iptv-norway-revolutionizing-entertainment-with-affordable-streaming/
https://socialbookmarknew.win/story.php?title=instant-casino-auszahlung-de-⭐️-spielen-im-online-casino-instant-deutschland · February 23, 2026 at 8:23 am
paddy power casino mobile
References:
https://socialbookmarknew.win/story.php?title=instant-casino-auszahlung-de-%E2%AD%90%EF%B8%8F-spielen-im-online-casino-instant-deutschland
onlinevetjobs.com · February 23, 2026 at 1:02 pm
celine dion in las vegas
References:
https://onlinevetjobs.com/author/unclebox4/
escatter11.fullerton.edu · February 23, 2026 at 2:01 pm
baltimore casino
References:
https://escatter11.fullerton.edu/nfs/show_user.php?userid=9588930
https://linkagogo.trade · February 23, 2026 at 2:28 pm
snoqualmie casino
References:
https://linkagogo.trade/story.php?title=sofortige-casino-auszahlung-schnell-sicher-und-unkompliziert
tvoyaskala.com · February 23, 2026 at 5:38 pm
casino paris
References:
https://tvoyaskala.com/user/eratray0/
ทดลองเล่นสล็อต pg · February 23, 2026 at 5:54 pm
pg slot
แพลตฟอร์ม TKBNEKO นำเสนอ แพลตฟอร์มดิจิทัลยุคใหม่ ซึ่ง ผู้ที่สนใจ สามารถ เข้าร่วม โลกแห่งเกมและความบันเทิง รวมถึง โอกาสสร้างรายได้แบบรวดเร็ว เว็บไซต์นี้ นำเสนอแนวคิดว่าทุกคนมีสิทธิ์ประสบความสำเร็จ เนื่องจาก มีความสะดวกสบายและใช้งานง่าย
หนึ่งใน คุณสมบัติหลัก ของแพลตฟอร์มนี้คือ ระบบฝากและถอนเงิน ซึ่งมีขั้นต่ำในการเติมเงินเพียง เริ่มต้น 1 บาท และขั้นต่ำในการถอนเงินก็เช่นเดียวกันที่ เริ่มต้น 1 บาท เท่านั้น การฝากเงินเสร็จภายใน 3 วินาที ทำให้แพลตฟอร์มนี้ โดดเด่นด้านความเร็ว นอกจากนี้ยัง ไม่มีวงเงินจำกัดในการถอน ซึ่งเป็น ข้อได้เปรียบเมื่อเทียบกับแพลตฟอร์มอื่น
สำหรับการเติมเงิน สมาชิกสามารถสแกน QR Code เพื่อโอนเงิน ซึ่งเป็นระบบที่ ลดขั้นตอนที่ซับซ้อน
แพลตฟอร์มนี้มีเกมให้เลือก ครบทุกหมวดหมู่ เช่น สล็อตออนไลน์, Live Casino, Sports Betting และ Fishing Game ผู้เล่นสามารถดูรายชื่อเกมทั้งหมดได้ผ่านตัวกรอง “ทั้งหมด” ซึ่งช่วยให้ เข้าถึงเกมโปรดได้สะดวก
TKBNEKO เน้นย้ำถึงความสำคัญของเกมที่มีลิขสิทธิ์ถูกต้องและการเล่นที่ยุติธรรม โดยร่วมมือกับ พันธมิตรเกมที่ผ่านมาตรฐานสากล ซึ่งช่วยให้มั่นใจได้ว่า ผู้เล่นจะได้รับประสบการณ์ที่โปร่งใสและปลอดภัย
TKBNEKO ได้ผสานระบบการชำระเงินเข้ากับ สถาบันการเงินหลักในไทย เช่น Krungthai Bank, Bangkok Bank, SCB, Kasikorn Bank, Thanachart Bank, GSB, TrueMoney Wallet, Citibank, UOB และ BAAC ทำให้การทำธุรกรรมทางการเงิน รวดเร็วและปลอดภัยยิ่งกว่าเดิม
สรุปได้ว่า TKBNEKO คือแพลตฟอร์มที่ ทันสมัย ปลอดภัย และใช้งานง่าย สำหรับเกมออนไลน์และการเดิมพัน ด้วยเงื่อนไขขั้นต่ำที่ต่ำ การทำธุรกรรมที่รวดเร็ว และเกมให้เลือกมากมาย ทำให้แพลตฟอร์มนี้ เหมาะสำหรับทั้งผู้เริ่มต้นและผู้เล่นที่มีประสบการณ์ ร่วมสนุกได้เลยวันนี้ และ เปิดประสบการณ์ใหม่กับโลกแห่งความบันเทิงและการเดิมพัน
https://my.vipaist.ru · February 23, 2026 at 8:44 pm
moncton nb weather
References:
https://my.vipaist.ru/user/oboeturkey7/
https://aryba.kg · February 23, 2026 at 9:01 pm
perth casino
References:
https://aryba.kg/user/radishrate0/
uvs2.net · February 24, 2026 at 8:43 am
jacks or better video poker
References:
http://uvs2.net/index.php/user/mimosabrandy57
https://linkagogo.trade/story.php?title=pokies-galaxy · February 24, 2026 at 11:40 am
best blackjack strategy
References:
https://linkagogo.trade/story.php?title=pokies-galaxy
https://bookmarkfeeds.stream/story.php?title=galaxy-96-casino-minimum-deposit-by-payment-online-play-environment-for-australia · February 24, 2026 at 2:01 pm
crazy vegas casino
References:
https://bookmarkfeeds.stream/story.php?title=galaxy-96-casino-minimum-deposit-by-payment-online-play-environment-for-australia
https://chessdatabase.science/wiki/E_wallet_casino_list_for_Australia · February 24, 2026 at 4:46 pm
resto montreal
References:
https://chessdatabase.science/wiki/E_wallet_casino_list_for_Australia
b2xbet · February 24, 2026 at 5:34 pm
Fascinating blog! Is your theme custom made or did you download it from somewhere? A design like yours with a few simple tweeks would really make my blog jump out. Please let me know where you got your theme. Bless you
Timothytoumn · February 24, 2026 at 10:44 pm
TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ โลกออนไลน์เติบโตต่อเนื่อง TKBNEKO พร้อมยกระดับการให้บริการ ด้วยระบบที่ ทันสมัย เสถียร และ ตรวจสอบได้ เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
จุดเด่นระบบฝาก-ถอน
ฝากขั้นต่ำ: เริ่มต้น 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ใช้เวลาเพียง 3 วินาที
ยอดถอน: ไม่มีลิมิต
ฝากง่าย เพียงสแกน QR Code
สแกน คิวอาร์ ระบบจะ โอนเงินเข้าทันที ขั้นต่ำ เริ่ม 100 บาท สูงสุด ไม่เกิน 500,000 บาทต่อครั้ง
หมวดหมู่เกม
สล็อต: ธีมหลากหลาย
เกมสด: ดีลเลอร์สด
กีฬา: เดิมพันลีกดัง
ยิงปลา: สนุกได้เงินจริง
โบนัสและโปรโมชัน
ติดตามหน้า โปรโมชั่น พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม แอฟฟิลิเอต
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ศูนย์ช่วยเหลือ ทีมงาน TKBNEKO พร้อมดูแลตลอดเวลา
saveyoursite.date · February 25, 2026 at 1:56 am
top poker players
References:
https://saveyoursite.date/story.php?title=shuffle-casino-app-payment-methods-new-zealand
https://justpin.date/ · February 25, 2026 at 2:56 am
the atlantic club casino
References:
https://justpin.date/story.php?title=best-e-wallet-casinos-australia-top-e-wallet-pokies-2026
pg slot · February 25, 2026 at 3:11 am
pg slot แพลตฟอร์มเกมสล็อตยอดนิยม เข้าเล่นไว ฝากถอนออโต้
คำค้นหา pg slot ถูกค้นหามากขึ้นเรื่อยๆ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน งานภาพคุณภาพสูง ความ ลื่นไหล และ ระบบจ่ายที่ดึงดูด เกมของ PG ออกแบบโดยทีมงานมืออาชีพ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ คอมพิวเตอร์
ความโดดเด่น ของ สล็อต PG
สล็อต PG เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบเว็บ และรองรับ ทุกอุปกรณ์ เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน หน้าเว็บ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ 3D ให้ความคมชัด พร้อมเอฟเฟกต์ จัดเต็ม
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
ระบบโบนัสและฟรีสปินหลากหลายรูปแบบ
ระบบตัวคูณ
โหมดทดลองเล่นฟรี
รองรับภาษาไทยเต็มรูปแบบ
ระบบการเงินรวดเร็ว ไม่ต้องรอนาน
แพลตฟอร์ม PG Slot ส่วนใหญ่รองรับ การฝาก-ถอน ฝากถอนตลอดเวลา ขั้นต่ำเริ่มต้นเพียง 10 บาท ขึ้นอยู่กับ กติกาแต่ละแพลตฟอร์ม การทำรายการใช้เวลา รวดเร็วมาก ผ่าน สแกน QR หรือระบบ แอปธนาคาร ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
แนวเกมที่คนเล่นเยอะ ใน pg slot
เกม สล็อต PG มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม ลุยด่าน
ธีม เอเชียและโชคลาภ
ธีม สัตว์และธรรมชาติ
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ Special Feature และ ระบบจ่ายคุ้มค่า เหมาะกับทั้ง มือใหม่ และ ผู้เล่นมือโปร
ความปลอดภัย
สล็อต PG มีมาตรฐานรองรับ มีการ เข้ารหัสข้อมูล และใช้ระบบสุ่มผล ระบบสุ่มมาตรฐาน เพื่อให้ผลลัพธ์ ตรวจสอบได้ แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ความปลอดภัยสูง
บทสรุปท้ายบท
PG Slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ไว ผู้เล่นสามารถเริ่มต้นได้ ง่าย ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ทั้งมือใหม่และมือโปร ในโลกของเกมสล็อตออนไลน์
https://peatix.com/user/29003208 · February 25, 2026 at 3:39 am
h top casino royal
References:
https://peatix.com/user/29003208
http://premiumdesignsinc.com/forums/user/chestarch36 · February 25, 2026 at 6:02 am
hollywood casino bangor
References:
http://premiumdesignsinc.com/forums/user/chestarch36/
laredadainfo.com · February 25, 2026 at 2:37 pm
grand villa casino
References:
https://laredadainfo.com/como-el-diseno-urbano-influye-en-nuestra-salud-caminar-mas-depende-de-tu-ciudad-no-solo-de-tu-fuerza-de-voluntad/
smidt-downey-3.hubstack.net · February 25, 2026 at 4:26 pm
steroid use in bodybuilding
References:
https://smidt-downey-3.hubstack.net/anavar-erwerben-wo-und-wie-sie-es-legal-kaufen-konnen-cribbrown77
https://tvoyaskala.com · February 25, 2026 at 5:22 pm
%random_anchor_text%
References:
https://tvoyaskala.com/user/stateflare4/
http://simsideo.net/ · February 25, 2026 at 6:48 pm
four winds casino dowagiac
References:
http://simsideo.net/livredor.php
marvelvsdc.faith · February 25, 2026 at 9:07 pm
%random_anchor_text%
References:
https://marvelvsdc.faith/wiki/Medikamente_bestellen_Achtung_vor_Flschungen
liftdaniel7.werite.net · February 25, 2026 at 10:26 pm
steroids and weight loss
References:
https://liftdaniel7.werite.net/anavar-kaufen-wo-und-wie-legal-erwerben
cognos.space · February 25, 2026 at 10:26 pm
casino com
References:
https://cognos.space/alzheimer-previna-se-sem-remedios/
ontariowi.com · February 26, 2026 at 12:07 am
casino online argentina
References:
https://ontariowi.com/village-newsletter/
https://ayahuascacayisatinal.com/ · February 26, 2026 at 12:53 am
ottawa quebec
References:
https://ayahuascacayisatinal.com/
https://actualites.cava.tn/ · February 26, 2026 at 3:09 am
what type of drug are steroids
References:
https://actualites.cava.tn/user/liftlisa1/
fakenews.win · February 26, 2026 at 3:28 am
%random_anchor_text%
References:
https://fakenews.win/wiki/Anavar_kaufen_Wo_und_wie_legal_erwerben
hylifesaving.com · February 26, 2026 at 6:50 am
wild horse casino az
References:
http://hylifesaving.com/word
aurousseauarchitecte.com · February 26, 2026 at 6:52 am
best online casino bonuses in the uk
References:
https://aurousseauarchitecte.com/portfolio/restructuration-des-urgences-du-chu-de-nimes/
community.decentrixweb.com · February 26, 2026 at 7:12 am
play slot machine
References:
https://community.decentrixweb.com/index.php/question/lhanefub-3/
test.tvorchi.com.ua · February 26, 2026 at 8:17 am
casino slot machine games
References:
https://test.tvorchi.com.ua/2021/08/02/if-youre-utilizing-a-toy-with-a-condom/
www.elsieisy.com · February 26, 2026 at 9:15 am
insurance blackjack
References:
https://www.elsieisy.com/the-house/
www.realitateavalceana.ro · February 26, 2026 at 11:33 am
roxy casino
References:
https://www.realitateavalceana.ro/bilan%c8%9bul-ipj-valcea-pe-2025-obiective-pentru-2026/
schlatthof.net · February 26, 2026 at 12:13 pm
euroking casino
References:
http://schlatthof.net/togo-reise-november-2023/es-geht-gleich-in-die-vollen-uns-erster-tag-in-togo/
扫毒风暴aiyifan · February 26, 2026 at 12:25 pm
Man United flop Sancho eyes Borussia Dortmund return – 2026 transfer news bombshell – latest football scores & rumors!
https://legal-immobilier.fr/optimiser-la-rentabilite-de-son-bien-locatif · February 26, 2026 at 12:49 pm
casino cleveland
References:
https://legal-immobilier.fr/optimiser-la-rentabilite-de-son-bien-locatif/
https://community.decentrixweb.com/index.php/question/fobertliept-8/ · February 26, 2026 at 1:24 pm
star casino sydney
References:
https://community.decentrixweb.com/index.php/question/fobertliept-8/
magiamgia.blog.fc2.com · February 26, 2026 at 1:33 pm
best slot machines
References:
https://magiamgia.blog.fc2.com/blog-entry-48494.html
https://www.elsieisy.com/apatt-remembering-africas-true-patriots-in-a-time-of-moral-poverty · February 26, 2026 at 1:49 pm
harrington raceway and casino
References:
https://www.elsieisy.com/apatt-remembering-africas-true-patriots-in-a-time-of-moral-poverty/
animallovergifts.com · February 26, 2026 at 1:50 pm
operation blackjack
References:
https://animallovergifts.com/catloversgift/
https://vivek-desai.com/ · February 26, 2026 at 1:58 pm
blackjack online
References:
https://vivek-desai.com/pages/page-left-sidebar/
https://www.elsieisy.com/ · February 26, 2026 at 2:54 pm
slot machine 4sh
References:
https://www.elsieisy.com/beautyplus_20160809085909_fast/
www.elsieisy.com · February 26, 2026 at 3:17 pm
casino la roche posay
References:
https://www.elsieisy.com/ubfss/
https://bobojesen.com/aenean-vulputate-eleifend-tellus-aenean-leo-ligula/ · February 26, 2026 at 3:45 pm
harrah’s casino new orleans
References:
https://bobojesen.com/aenean-vulputate-eleifend-tellus-aenean-leo-ligula/
vietex.blog.fc2.com · February 26, 2026 at 3:55 pm
ruby fortune casino
References:
https://vietex.blog.fc2.com/blog-entry-549.html
https://www.elsieisy.com/ · February 26, 2026 at 5:04 pm
eagle pass casino
References:
https://www.elsieisy.com/aicha-blogfest/
RussellPhync · February 26, 2026 at 5:28 pm
ทดลองเล่นสล็อต
vietlinklogistics.com · February 26, 2026 at 5:31 pm
casino slots games
References:
https://vietlinklogistics.com/cac-tuyen-dac-biet/chuyen-phat-nhanh-tu-viet-nam-sang-singapore.html
https://www.elsieisy.com/ · February 26, 2026 at 5:31 pm
shelbyville casino
References:
https://www.elsieisy.com/human/
Charlestub · February 26, 2026 at 5:33 pm
สล็อต
https://shkolnaiapora.ru/question/podstav-slova-v-slovometr · February 26, 2026 at 6:10 pm
online slot machines
References:
https://shkolnaiapora.ru/question/podstav-slova-v-slovometr
RussellPhync · February 26, 2026 at 6:25 pm
ทดลองเล่นสล็อต สล็อต PG เกมสล็อตออนไลน์ที่คนค้นหาเยอะ เล่นง่าย ฝากถอนเร็ว
คำค้นหา PG Slot กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ผู้ให้บริการเกมสล็อตที่มาแรง ด้าน กราฟิก ความ ลื่นไหล และ ระบบจ่ายที่ดึงดูด เกมของ PG พัฒนาโดยผู้ให้บริการชั้นนำ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ คอมพิวเตอร์
จุดเด่น ของ pg slot
pg slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เข้าเกมไว เล่นผ่าน ระบบเว็บ และรองรับ ทุกอุปกรณ์ ไม่ต้องติดตั้งเพิ่มเติม ผู้เล่นสามารถเข้าเล่นผ่าน Browser ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม PG Slot ได้แก่
โบนัสและฟรีสปินหลายแบบ
ฟีเจอร์ตัวคูณรางวัล
เดโม่ฟรี
มีเมนูภาษาไทย
ระบบฝากถอนสะดวก ทำรายการไว
แพลตฟอร์ม สล็อต PG มักมี การฝาก-ถอน ฝากถอนตลอดเวลา ขั้นต่ำเริ่มต้นเพียง 10 บาท ขึ้นอยู่กับ เงื่อนไขของเว็บไซต์ การทำรายการใช้เวลา รวดเร็วมาก ผ่าน คิวอาร์โค้ด หรือระบบ ธนาคารบนมือถือ ทำให้ธุรกรรมเป็นไปอย่าง ไม่สะดุด
ประเภทเกมยอดนิยม ใน pg slot
เกม PG Slot มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม Adventure
ธีม ความมั่งคั่ง
ธีม Animal
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ โบนัสรอบพิเศษ และ โอกาสทำกำไรสูง เหมาะกับทั้ง คนเพิ่งเล่น และ ผู้เล่นมือโปร
ความน่าเชื่อถือ
สล็อต PG พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล RNG เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ความปลอดภัยสูง
โดยภาพรวม
pg slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน ระบบลื่นไหล และการทำธุรกรรมที่ ไว ผู้เล่นสามารถเริ่มต้นได้ ง่าย ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
Charlestub · February 26, 2026 at 6:37 pm
pg slot เกมสล็อตออนไลน์ที่คนค้นหาเยอะ ใช้งานง่าย ฝากถอนรวดเร็ว
คำค้นหา PG Slot กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน งานภาพคุณภาพสูง ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG พัฒนาโดยผู้ให้บริการชั้นนำ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ พีซี
จุดเด่น ของ PG Slot
pg slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เปิดเกมได้ทันที เล่นผ่าน ระบบอัตโนมัติ และรองรับ ทุกแพลตฟอร์ม ไม่ต้องติดตั้งเพิ่มเติม ผู้เล่นสามารถเข้าเล่นผ่าน หน้าเว็บ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ 3D ให้ความคมชัด พร้อมเอฟเฟกต์ สมจริง
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
มีรอบโบนัสให้ลุ้นบ่อย
Multiplier
โหมดทดลองเล่นฟรี
ใช้งานภาษาไทยง่าย
ระบบการเงินรวดเร็ว ทันใจ
แพลตฟอร์ม สล็อต PG โดยทั่วไปให้บริการ การฝาก-ถอน ฝากถอนตลอดเวลา ขั้นต่ำเริ่มต้นเพียง 10 บาท ขึ้นอยู่กับ กติกาแต่ละแพลตฟอร์ม การทำรายการใช้เวลา ไม่กี่วินาที ผ่าน คิวอาร์โค้ด หรือระบบ Mobile Banking ทำให้ธุรกรรมเป็นไปอย่าง ไม่สะดุด
แนวเกมที่คนเล่นเยอะ ใน pg slot
เกม PG Slot มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม ลุยด่าน
ธีม โชคลาภ
ธีม Animal
เกมยอดนิยมมักเป็นเกมที่แตกง่าย พร้อมระบบ โบนัสรอบพิเศษ และ ระบบจ่ายคุ้มค่า เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ สายสล็อตจริงจัง
ความน่าเชื่อถือ
pg slot พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล Random Number Generator เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ระบบดูแลข้อมูล
โดยภาพรวม
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ รวดเร็ว ผู้เล่นสามารถเริ่มต้นได้ ทันที ฝากถอนสะดวก และเลือกเกมได้ จำนวนมาก เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
www.niconya.com · February 26, 2026 at 7:16 pm
wind creek casino atmore al
References:
https://www.niconya.com/start-page.html
animallovergifts.com · February 26, 2026 at 7:16 pm
par a dice casino
References:
https://animallovergifts.com/loveyourpetday/
https://marketmed.kz/ · February 26, 2026 at 7:57 pm
monopoly slots
References:
https://marketmed.kz/news/spaysovaya-zavisimost-myetody-lyechyeniya/
yashichi.com · February 26, 2026 at 11:03 pm
jupiters casino gold coast
References:
http://yashichi.com/?p=86
https://bitpoll.de/ · February 27, 2026 at 12:14 am
sugarhouse casino
References:
https://bitpoll.de/poll/OgHDL7tOy7/
Timothytoumn · February 27, 2026 at 12:24 am
ทดลองเล่นสล็อต pg
TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ธุรกรรมรวดเร็ว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว TKBNEKO พร้อมยกระดับการให้บริการ ด้วยระบบที่ ล้ำสมัย รวดเร็ว และ โปร่งใส เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
จุดเด่นระบบฝาก-ถอน
ฝากขั้นต่ำ: เริ่มต้น 1 บาท
ถอนขั้นต่ำ: 1 บาท
เวลาฝากเงิน: ใช้เวลาเพียง 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
เติมเงินง่าย แค่สแกน
สแกน QR Code ระบบจะ โอนเงินเข้าทันที ขั้นต่ำ 100 บาท สูงสุด 500,000 บาท
เกมยอดนิยม
สล็อต: ลุ้นแจ็คพอต
เกมสด: คาสิโนเรียลไทม์
กีฬา: แมตช์ทั่วโลก
ยิงปลา: สนุกได้เงินจริง
โบนัสและโปรโมชัน
ติดตามหน้า โบนัส พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม พันธมิตร
ติดต่อเรา
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ติดต่อเรา ทีมงาน TKBNEKO พร้อมดูแลตลอดเวลา
barnsfortroende.com · February 27, 2026 at 12:42 am
casino st louis
References:
https://barnsfortroende.com/barns-rattigheter-i-sverige/
http://schlatthof.net/togo-reise-herbst-2019/schwitzen-in-der-kara-region · February 27, 2026 at 7:48 am
blue chip casino
References:
http://schlatthof.net/togo-reise-herbst-2019/schwitzen-in-der-kara-region/
gbgbet · February 27, 2026 at 8:35 am
I’m gone to convey my little brother, that he should also visit this webpage on regular basis to take updated from newest information.
www.upendogroup.ngdafrica.com · February 27, 2026 at 9:53 am
online slots australia
References:
http://www.upendogroup.ngdafrica.com/spip.php?article56
https://www.elsieisy.com/ · February 27, 2026 at 10:10 am
real money online poker
References:
https://www.elsieisy.com/ladies-skirts/
cpdbouvxc3m7.blog.fc2.com · February 27, 2026 at 12:49 pm
speaking rock casino
References:
https://cpdbouvxc3m7.blog.fc2.com/blog-entry-376.html
online · February 27, 2026 at 1:17 pm
Sour Diesel
on their website · February 27, 2026 at 1:18 pm
clones shipped to new jersey
мелбет скачать на айфон · February 27, 2026 at 3:10 pm
промокод на мелбет при регистрации
Установить Melbet: APK, iPhone и ПК
Мобильная версия Melbet включает букмекерскую контору и казино в едином приложении. Пользователю доступны live-ставки, слоты, прямые трансляции, аналитика и операции по счёту. Установка занимает 1–2 минуты.
Android (APK)
Загрузите APK с официального источника, запустите установщик и завершите установку. Если требуется включите доступ к установке сторонних приложений, затем войдите в аккаунт.
iOS (iPhone)
Перейдите в App Store, найдите «Melbet», нажмите «Получить», после установки выполните вход.
ПК
Откройте официальный сайт, авторизуйтесь и создайте ярлык на рабочий стол. Браузерная версия функционирует как полноценное приложение.
Функционал
Live-ставки с мгновенным обновлением линии, казино и слоты, просмотр матчей, подробная статистика, push-оповещения, регистрация за минуту и поддержка 24/7.
Бонусы
После установки доступны бонус на первый депозит, акционные коды и фрибеты. Правила начисления определяются регионом.
Безопасность
Загружайте только с официального сайта, контролируйте адрес сайта, не передавайте пароль третьим лицам и активируйте двухфакторную аутентификацию.
Загрузка выполняется быстро, после чего открывается полный доступ Melbet.
melbet зеркало рабочее на сегодня · February 27, 2026 at 3:24 pm
мелбет вход зеркало
Скачать Melbet: Android, iPhone и ПК
Приложение Melbet включает букмекерскую контору и казино в одном интерфейсе. Пользователю доступны live-ставки, казино-игры, онлайн-трансляции, статистика и операции по счёту. Загрузка занимает несколько минут.
Android (APK)
Скачайте APK с официального источника, откройте файл и подтвердите установку. При необходимости включите разрешение на установку из неизвестных источников, затем войдите в аккаунт.
iOS (iPhone)
Откройте App Store, найдите «Melbet», выберите «Получить», после установки авторизуйтесь в системе.
ПК
Откройте официальный сайт, войдите в личный кабинет и добавьте ярлык на рабочий стол. Браузерная версия функционирует как полноценное приложение.
Функционал
Live-ставки с обновлением коэффициентов, казино и слоты, прямые трансляции, подробная статистика, уведомления о матчах, быстрая регистрация и круглосуточная служба поддержки.
Бонусы
После установки доступны бонус на первый депозит, промокоды и фрибеты. Условия зависят от региона.
Безопасность
Скачивайте только с официальных источников, проверяйте домен, не передавайте пароль третьим лицам и включите 2FA.
Загрузка выполняется быстро, после чего открывается полный доступ Melbet.
Gabrieljek · February 27, 2026 at 4:48 pm
ทดลองเล่นสล็อต pg ซื้อฟรีสปิน
бк мелбет официальный сайт · February 27, 2026 at 5:08 pm
скачать мелбет на андроид бесплатно с официального
Скачать приложение Melbet: Android, iPhone и компьютер
Мобильная версия Melbet объединяет букмекерскую контору и казино в едином приложении. Доступны live-ставки, казино-игры, прямые трансляции, статистика и быстрые финансовые операции. Загрузка занимает несколько минут.
Android (APK)
Скачайте APK с официального сайта, запустите установщик и завершите установку. При необходимости включите разрешение на установку из неизвестных источников, затем войдите в аккаунт.
iOS (iPhone)
Откройте App Store, введите в поиске «Melbet», нажмите «Получить», после установки авторизуйтесь в системе.
ПК
Перейдите официальный сайт, войдите в личный кабинет и создайте ярлык на рабочий стол. Веб-версия работает как отдельное приложение.
Функционал
Live-ставки с обновлением коэффициентов, игровой раздел с тысячами игр, просмотр матчей, аналитические данные, push-оповещения, быстрая регистрация и поддержка 24/7.
Бонусы
После загрузки доступны приветственный бонус, акционные коды и бесплатные ставки. Условия зависят от региона.
Безопасность
Скачивайте только с официальных источников, контролируйте адрес сайта, не сообщайте данные доступа третьим лицам и активируйте двухфакторную аутентификацию.
Загрузка выполняется быстро, после чего доступен весь функционал Melbet.
MartinEmbet · February 27, 2026 at 5:24 pm
ทดลองเล่นสล็อต pg ซื้อฟรีสปิน
nuôi lô 88.com · February 27, 2026 at 5:53 pm
If you’re looking for a solid ‘nuôi lô 88.com’ resource, Lonuoirongbachkim is it. Seriously, I’ve seen some great results using their tips. Give it a try nuôi lô 88.com.
byu 777 casino · February 27, 2026 at 5:54 pm
Yo, BYU 777 Casino is where it’s at! Great selection of games and the payouts are decent. Definitely worth a look-see byu 777 casino!
mgpk777gameapk · February 27, 2026 at 5:54 pm
Yo, just downloaded the MGPK777gameapk. Installation was smooth, but the graphics are a bit meh. Anyone else playing? Trying to gauge if it’s worth investing some time. Hit me up with your experiences at mgpk777gameapk.
https://www.westley.com.au/ · February 27, 2026 at 7:34 pm
online casino
References:
https://www.westley.com.au/events/world-famous-places-exhibition/
wspomozycielka-lodz.pl · February 27, 2026 at 9:44 pm
arkansas casinos
References:
https://wspomozycielka-lodz.pl/?p=745
https://www.realitateavalceana.ro/planul-județean-de-incluziune-sociala-2026/ · February 27, 2026 at 9:57 pm
microgaming casino bonus
References:
https://www.realitateavalceana.ro/planul-jude%c8%9bean-de-incluziune-sociala-2026/
watbosa.ac.th · February 27, 2026 at 10:09 pm
bellagio casino
References:
https://watbosa.ac.th/question/csfgnhiuu/
CharleyBar · March 1, 2026 at 2:00 am
ทดลองเล่นสล็อต pg ไม่ เด้ง
melbet скачать ios · March 1, 2026 at 12:52 pm
скачать мелбет казино на андроид
Скачать приложение Melbet: APK, iPhone и ПК
Приложение Melbet объединяет ставки и казино в одном интерфейсе. Пользователю доступны live-ставки, казино-игры, онлайн-трансляции, статистика и операции по счёту. Установка занимает 1–2 минуты.
Android (APK)
Скачайте APK с официального источника, откройте файл и завершите установку. Если требуется включите разрешение на установку из неизвестных источников, затем войдите в аккаунт.
iOS (iPhone)
Перейдите в App Store, найдите «Melbet», выберите «Получить», после установки выполните вход.
ПК
Откройте официальный сайт, войдите в личный кабинет и создайте ярлык на рабочий стол. Браузерная версия функционирует как отдельное приложение.
Функционал
Live-ставки с обновлением коэффициентов, игровой раздел с тысячами игр, просмотр матчей, подробная статистика, push-оповещения, регистрация за минуту и поддержка 24/7.
Бонусы
После установки доступны бонус на первый депозит, промокоды и фрибеты. Правила начисления определяются регионом.
Безопасность
Загружайте только с официальных источников, контролируйте адрес сайта, не передавайте пароль третьим лицам и активируйте двухфакторную аутентификацию.
Загрузка выполняется быстро, после чего доступен весь функционал Melbet.
melbet личный кабинет · March 1, 2026 at 1:22 pm
мелбет ком зеркало
Скачать Melbet: Android, iPhone и компьютер
Приложение Melbet включает букмекерскую контору и казино в едином приложении. Доступны live-ставки, казино-игры, онлайн-трансляции, аналитика и операции по счёту. Установка занимает 1–2 минуты.
Android (APK)
Скачайте APK с официального источника, откройте файл и подтвердите установку. При необходимости включите разрешение на установку из неизвестных источников, затем авторизуйтесь.
iOS (iPhone)
Откройте App Store, введите в поиске «Melbet», нажмите «Получить», после установки авторизуйтесь в системе.
ПК
Откройте официальный сайт, войдите в личный кабинет и создайте ярлык на рабочий стол. Веб-версия работает как отдельное приложение.
Функционал
Live-ставки с обновлением коэффициентов, казино и слоты, прямые трансляции, аналитические данные, уведомления о матчах, быстрая регистрация и поддержка 24/7.
Бонусы
После установки доступны бонус на первый депозит, промокоды и фрибеты. Условия зависят от региона.
Безопасность
Загружайте только с официальных источников, контролируйте адрес сайта, не передавайте пароль третьим лицам и активируйте двухфакторную аутентификацию.
Установка занимает несколько минут, после чего открывается полный доступ Melbet.
hi88 · March 1, 2026 at 9:46 pm
bookmarked!!, I love your web site!
國產 av · March 1, 2026 at 11:19 pm
My brother suggested I might like this blog. He was entirely right. This post actually made my day. You can not imagine simply how much time I had spent for this info! Thanks!
Timothytoumn · March 2, 2026 at 2:20 am
ทดลองเล่นสล็อต pg
TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ทันสมัย รวดเร็ว และ โปร่งใส เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
ระบบการเงินที่ใช้งานง่าย
ฝากขั้นต่ำ: เริ่มต้น 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ใช้เวลาเพียง 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
เติมเงินง่าย แค่สแกน
สแกน คิวอาร์ ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ 100 บาท สูงสุด ไม่เกิน 500,000 บาทต่อครั้ง
เกมยอดนิยม
สล็อต: ลุ้นแจ็คพอต
เกมสด: ดีลเลอร์สด
กีฬา: เดิมพันลีกดัง
ยิงปลา: สนุกได้เงินจริง
โปรโมชั่นและสิทธิพิเศษ
ติดตามหน้า โบนัส พร้อมระบบ VIP และโปรแกรม พันธมิตร
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ติดต่อเรา ทีมงาน ของเรา พร้อมดูแลตลอดเวลา
BradleyBit · March 2, 2026 at 2:59 am
ทดลองเล่นสล็อต pg เว็บ ตรง”
PG Slot แพลตฟอร์มเกมสล็อตยอดนิยม เล่นง่าย ฝากถอนเร็ว
คำค้นหา สล็อต PG มาแรงในช่วงนี้ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน งานภาพคุณภาพสูง ความ เสถียร และ ระบบจ่ายที่ดึงดูด เกมของ PG พัฒนาโดยผู้ให้บริการชั้นนำ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ เดสก์ท็อป
ข้อดี ของ PG Slot
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบออนไลน์ และรองรับ ทุกแพลตฟอร์ม ไม่ต้องดาวน์โหลดแอป ผู้เล่นสามารถเข้าเล่นผ่าน Browser ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ เอฟเฟกต์ 3 มิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม PG Slot ได้แก่
โบนัสและฟรีสปินหลายแบบ
ระบบตัวคูณ
เล่นฟรีก่อนเติมเงิน
ใช้งานภาษาไทยง่าย
ฝากถอนง่าย ทันใจ
แพลตฟอร์ม สล็อต PG ส่วนใหญ่รองรับ การฝาก-ถอน อัตโนมัติ 24 ชั่วโมง ขั้นต่ำเริ่มต้นเพียง 1 บาท ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา เพียงไม่กี่วินาที ผ่าน คิวอาร์โค้ด หรือระบบ แอปธนาคาร ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
หมวดเกมฮิต ใน pg slot
เกม pg slot มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม Adventure
ธีม โชคลาภ
ธีม Animal
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ โบนัสรอบพิเศษ และ อัตราการจ่ายที่สูง เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นมือโปร
มาตรฐานระบบ
PG Slot พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล ระบบสุ่มมาตรฐาน เพื่อให้ผลลัพธ์ ยุติธรรม แพลตฟอร์มที่ให้บริการ pg slot ควรมี ความปลอดภัยสูง
บทสรุปท้ายบท
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน ระบบลื่นไหล และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ไม่ซับซ้อน ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
Jasonsuide · March 2, 2026 at 3:13 am
pg
แพลตฟอร์ม TKBNEKO พาคุณสู่โลกใหม่ของเกมเดิมพันออนไลน์ ธุรกรรมฉับไว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคที่ นวัตกรรมดิจิทัลเข้ามาปรับโฉมวงการเกมออนไลน์ TKBNEKO พร้อมยกระดับมาตรฐานการเดิมพัน ด้วยระบบการให้บริการที่ ล้ำสมัย ฉับไว และ โปร่งใส พร้อมต้อนรับสมาชิกทุกท่านสู่ ประสบการณ์ความบันเทิงรูปแบบใหม่ ที่ เปิดโอกาสให้ทุกคนสร้างรายได้
ทำไมต้อง TKBNEKO?
TKBNEKO มุ่งมั่นที่จะมอบประสบการณ์จากเกมลิขสิทธิ์แท้ โดยเฉพาะเกมที่ ผ่านการรับรองจากสถาบันที่น่าเชื่อถือ และ เป็นที่นิยมในระดับสากล เพื่อให้ผู้เล่นทุกคน สบายใจ ได้ว่า จะได้รับความเพลิดเพลินกับเกมที่ ยุติธรรม ปลอดภัย และ ได้มาตรฐานระดับสากล
ระบบการเงินที่เหนือกว่า
เราออกแบบระบบการเงินให้ง่ายและเร็วที่สุด เพื่อให้คุณ เพลิดเพลินกับการเดิมพันอย่างต่อเนื่อง
ฝากขั้นต่ำ: เริ่มต้นเพียง 1 บาท
ถอนขั้นต่ำ: 1 บาท
เวลาฝากเงิน: รวดเร็วทันใจใน 3 วินาที
ยอดจำกัดการถอน: ถอนได้ไม่จำกัดยอด
ฝากง่าย เพียงสแกน QR Code
เพียงคุณสแกน คิวอาร์ ระบบของเราจะ ดำเนินการฝากเงินให้อัตโนมัติ ขั้นต่ำเพียง เริ่มต้น 100 บาท และสามารถฝากได้สูงถึง ไม่เกิน 500,000 บาทต่อครั้ง มาร่วมสนุกกันได้แล้ววันนี้ กับ TKBNEKO ที่ เล่นง่าย เดิมพันง่าย ได้เงินไว
หมวดหมู่เกมที่ครบครัน
แพลตฟอร์มของเราครอบคลุมทุกแนวเกม รองรับทุกความชอบของผู้เล่น
สล็อต: แจ็คพอตแตกง่าย ลุ้นได้ทุกวัน
เกมสด: สัมผัสประสบการณ์คาสิโนแบบเรียลไทม์
กีฬา: เดิมพันกับแมตช์การแข่งขันจากทั่วโลก
ยิงปลา: ลุ้นกำไรจากเกมยิงปลา
ติดตามโปรโมชั่นและสิทธิพิเศษ
อย่าลืมแวะมาเยี่ยมชมที่หน้า โปรโมชันล่าสุด เพื่อรับ สิทธิพิเศษมากมาย ที่เรามอบให้สมาชิกทุกท่าน นอกจากนี้ยังมีระบบ สมาชิกวีไอพี สำหรับลูกค้าคนสำคัญ และช่องทาง พันธมิตร สำหรับผู้ที่สนใจสร้างรายได้ร่วมกับเรา
ช่องทางติดต่อ
หากมี ข้อสงสัย หรือ ความคิดเห็น สามารถติดต่อทีมงานของเราได้ตลอด 24 ชั่วโมงที่หน้า ศูนย์ช่วยเหลือ และ แบบฟอร์มติดต่อ ทีมงาน ของเรา ยินดีให้บริการทุกท่านด้วยใจ
FelixGug · March 2, 2026 at 3:31 am
สล็อต
แพลตฟอร์ม TKBNEKO เปิดประสบการณ์ใหม่แห่งการเดิมพันออนไลน์ ธุรกรรมรวดเร็ว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ล้ำสมัย เสถียร และ ตรวจสอบได้ เพื่อให้ผู้เล่น อุ่นใจ ทุกครั้งที่ใช้งาน
ระบบการเงินที่ใช้งานง่าย
ฝากขั้นต่ำ: 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
ฝากง่าย เพียงสแกน QR Code
สแกน QR Code ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ เริ่ม 100 บาท สูงสุด 500,000 บาท
หมวดหมู่เกม
สล็อต: ลุ้นแจ็คพอต
เกมสด: ดีลเลอร์สด
กีฬา: เดิมพันลีกดัง
ยิงปลา: ลุ้นกำไรทันที
โปรโมชั่นและสิทธิพิเศษ
ติดตามหน้า โบนัส พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม พันธมิตร
ติดต่อเรา
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ติดต่อเรา ทีมงาน ของเรา พร้อมดูแลตลอดเวลา
Travisjal · March 2, 2026 at 3:51 am
สล็อต
แพลตฟอร์ม TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว TKBNEKO พร้อมยกระดับการให้บริการ ด้วยระบบที่ ทันสมัย รวดเร็ว และ โปร่งใส เพื่อให้ผู้เล่น อุ่นใจ ทุกครั้งที่ใช้งาน
ระบบการเงินที่ใช้งานง่าย
ฝากขั้นต่ำ: 1 บาท
ถอนขั้นต่ำ: 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
ฝากง่าย เพียงสแกน QR Code
สแกน QR Code ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ เริ่ม 100 บาท สูงสุด 500,000 บาท
หมวดหมู่เกม
สล็อต: ลุ้นแจ็คพอต
เกมสด: คาสิโนเรียลไทม์
กีฬา: เดิมพันลีกดัง
ยิงปลา: ลุ้นกำไรทันที
โปรโมชั่นและสิทธิพิเศษ
ติดตามหน้า โปรโมชั่น พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม พันธมิตร
ติดต่อเรา
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ศูนย์ช่วยเหลือ ทีมงาน ของเรา พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-a4ea8e21fdde
Charlestub · March 2, 2026 at 4:07 am
ทดลองเล่นสล็อต pg
pg slot แพลตฟอร์มเกมสล็อตยอดนิยม เข้าเล่นไว ฝากถอนออโต้
คำค้นหา PG Slot มาแรงในช่วงนี้ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน ภาพและเอฟเฟกต์ ความ ลื่นไหล และ โอกาสรับกำไรที่ดี เกมของ PG ผลิตโดยค่ายมาตรฐาน ที่รองรับการเล่นทั้งบน สมาร์ทโฟน และ คอมพิวเตอร์
ความโดดเด่น ของ pg slot
สล็อต PG เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบออนไลน์ และรองรับ ทั้ง iOS และ Android ไม่ต้องติดตั้งเพิ่มเติม ผู้เล่นสามารถเข้าเล่นผ่าน เว็บเบราว์เซอร์ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ จัดเต็ม
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
โบนัสและฟรีสปินหลายแบบ
ระบบตัวคูณ
โหมดทดลองเล่นฟรี
มีเมนูภาษาไทย
ระบบฝากถอนสะดวก ไม่ต้องรอนาน
แพลตฟอร์ม pg slot โดยทั่วไปให้บริการ การฝาก-ถอน ออโต้ตลอด 24 ชม. ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ เงื่อนไขของเว็บไซต์ การทำรายการใช้เวลา รวดเร็วมาก ผ่าน QR Code หรือระบบ แอปธนาคาร ทำให้ธุรกรรมเป็นไปอย่าง ต่อเนื่อง
หมวดเกมฮิต ใน PG Slot
เกม pg slot มีธีมหลากหลาย เช่น
ธีม เทพเจ้าและแฟนตาซี
ธีม ลุยด่าน
ธีม โชคลาภ
ธีม สัตว์และธรรมชาติ
หลายคนชอบเกมที่โบนัสเข้าไว พร้อมระบบ โบนัสรอบพิเศษ และ ระบบจ่ายคุ้มค่า เหมาะกับทั้ง คนเพิ่งเล่น และ สายสล็อตจริงจัง
ความปลอดภัย
สล็อต PG มีมาตรฐานรองรับ มีการ เข้ารหัสข้อมูล และใช้ระบบสุ่มผล Random Number Generator เพื่อให้ผลลัพธ์ ยุติธรรม แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ระบบดูแลข้อมูล
โดยภาพรวม
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ทันที ฝากถอนสะดวก และเลือกเกมได้ จำนวนมาก เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-70cdb1132344
Matthewdal · March 2, 2026 at 10:06 am
ทดลองเล่นสล็อต pg ซื้อฟรีสปิน
quaildonald3.werite.net · March 2, 2026 at 10:56 am
best beginner steroid cycle for lean mass
References:
https://quaildonald3.werite.net/guide-essentiel-pour-lachat-de-testosterone-securise
forum.issabel.org · March 2, 2026 at 11:18 am
anabolic steroids positive effects
References:
https://forum.issabel.org/u/jartank7
Josephneupt · March 2, 2026 at 11:21 am
ทดลองเล่นสล็อต pg ฟรี PG Slot เกมสล็อตออนไลน์ที่คนค้นหาเยอะ เล่นง่าย ฝากถอนเร็ว
คำค้นหา สล็อต PG กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน กราฟิก ความ ลื่นไหล และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ออกแบบโดยทีมงานมืออาชีพ ที่รองรับการเล่นทั้งบน มือถือ และ พีซี
จุดเด่น ของ สล็อต PG
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เข้าเกมไว เล่นผ่าน ระบบเว็บ และรองรับ ทั้ง iOS และ Android เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน หน้าเว็บ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ เอฟเฟกต์ 3 มิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม PG Slot ได้แก่
โบนัสและฟรีสปินหลายแบบ
Multiplier
โหมดทดลองเล่นฟรี
ใช้งานภาษาไทยง่าย
ฝากถอนง่าย ไม่ต้องรอนาน
แพลตฟอร์ม pg slot โดยทั่วไปให้บริการ การฝาก-ถอน ออโต้ตลอด 24 ชม. ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา เพียงไม่กี่วินาที ผ่าน QR Code หรือระบบ Mobile Banking ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
ประเภทเกมยอดนิยม ใน PG Slot
เกม pg slot มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม ลุยด่าน
ธีม เอเชียและโชคลาภ
ธีม Animal
เกมยอดนิยมมักเป็นเกมที่แตกง่าย พร้อมระบบ โบนัสรอบพิเศษ และ อัตราการจ่ายที่สูง เหมาะกับทั้ง มือใหม่ และ สายสล็อตจริงจัง
มาตรฐานระบบ
PG Slot พัฒนาในระบบสากล มีการ เข้ารหัสข้อมูล และใช้ระบบสุ่มผล Random Number Generator เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ สล็อต PG ควรมี ทีมซัพพอร์ต 24 ชม.
สรุป
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน ระบบลื่นไหล และการทำธุรกรรมที่ รวดเร็ว ผู้เล่นสามารถเริ่มต้นได้ ทันที ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
dlx.hamdard.pk · March 2, 2026 at 11:38 am
women before and after steroids
https://dlx.hamdard.pk/user/profile/437794 https://dlx.hamdard.pk/user/profile/437794
https://md.chaosdorf.de/s/MUkqEbMghJ https://md.chaosdorf.de/s/MUkqEbMghJ
https://ajarproductions.com/pages/products/in5/answers/user/boatpeony2 ajarproductions.com
https://postheaven.net/peapiano0/testosterone-en-pharmacie-notre-avis-1-alternative https://postheaven.net
https://p.mobile9.com/pearsea5/ p.mobile9.com
https://firsturl.de/NgK8gvd https://firsturl.de/
https://intensedebate.com/people/topsquash7 intensedebate.com
https://bom.so/FmUWj9 bom.so
https://pediascape.science/wiki/Cernos_Gel_Testogel_Testostrone_Gel_Acheter_En_Ligne pediascape.science
https://pattern-wiki.win/wiki/Les_5_meilleurs_boosters_de_testostrone_en_2026 https://pattern-wiki.win/wiki/Les_5_meilleurs_boosters_de_testostrone_en_2026
https://isowindows.net/user/glasscolor7/ https://isowindows.net/
http://uvs2.net/index.php/user/pilotseason4 uvs2.net
http://okprint.kz/user/nationpickle7/ okprint.kz
https://king-wifi.win/wiki/Top_10_des_Sites_pour_Acheter_de_la_Testostrone_testosteronesteroids_com https://king-wifi.win/wiki/Top_10_des_Sites_pour_Acheter_de_la_Testostrone_testosteronesteroids_com
https://lit-book.ru/user/peadonald2/ lit-book.ru
https://md.chaosdorf.de/s/MUkqEbMghJ https://md.chaosdorf.de/
https://output.jsbin.com/firororato/ https://output.jsbin.com
https://fakenews.win/wiki/Testostrone_achat_O_acheter_de_la_testostrone_en_vente_libre fakenews.win
RodneyChoix · March 2, 2026 at 12:36 pm
ทดลองเล่นสล็อต pg
แพลตฟอร์ม TKBNEKO เปิดประสบการณ์ใหม่แห่งการเดิมพันออนไลน์ ธุรกรรมรวดเร็ว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ โลกออนไลน์เติบโตต่อเนื่อง TKBNEKO พร้อมยกระดับการให้บริการ ด้วยระบบที่ ล้ำสมัย รวดเร็ว และ ตรวจสอบได้ เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
ระบบการเงินที่ใช้งานง่าย
ฝากขั้นต่ำ: เริ่มต้น 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
ฝากง่าย เพียงสแกน QR Code
สแกน คิวอาร์ ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ เริ่ม 100 บาท สูงสุด 500,000 บาท
หมวดหมู่เกม
สล็อต: ลุ้นแจ็คพอต
เกมสด: ดีลเลอร์สด
กีฬา: แมตช์ทั่วโลก
ยิงปลา: สนุกได้เงินจริง
โบนัสและโปรโมชัน
ติดตามหน้า โบนัส พร้อมระบบ VIP และโปรแกรม แอฟฟิลิเอต
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ศูนย์ช่วยเหลือ ทีมงาน TKBNEKO พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-e598fa477f69
JosephBer · March 2, 2026 at 12:36 pm
PG Slot เกมสล็อตออนไลน์ที่คนค้นหาเยอะ เข้าเล่นไว ฝากถอนออโต้
คำค้นหา PG Slot ถูกค้นหามากขึ้นเรื่อยๆ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน งานภาพคุณภาพสูง ความ นิ่งไม่สะดุด และ ระบบจ่ายที่ดึงดูด เกมของ PG ออกแบบโดยทีมงานมืออาชีพ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ พีซี
ข้อดี ของ PG Slot
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบออนไลน์ และรองรับ ทุกอุปกรณ์ เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน Browser ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ จัดเต็ม
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
โบนัสและฟรีสปินหลายแบบ
ระบบตัวคูณ
โหมดทดลองเล่นฟรี
มีเมนูภาษาไทย
ระบบฝากถอนสะดวก ทำรายการไว
แพลตฟอร์ม สล็อต PG ส่วนใหญ่รองรับ การฝาก-ถอน อัตโนมัติ 24 ชั่วโมง ขั้นต่ำเริ่มต้นเพียง 1 บาท ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา รวดเร็วมาก ผ่าน สแกน QR หรือระบบ Mobile Banking ทำให้ธุรกรรมเป็นไปอย่าง ไม่สะดุด
ประเภทเกมยอดนิยม ใน PG Slot
เกม pg slot มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม Adventure
ธีม โชคลาภ
ธีม ธรรมชาติ
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ ฟีเจอร์พิเศษ และ ระบบจ่ายคุ้มค่า เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ สายสล็อตจริงจัง
มาตรฐานระบบ
สล็อต PG พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล Random Number Generator เพื่อให้ผลลัพธ์ ยุติธรรม แพลตฟอร์มที่ให้บริการ สล็อต PG ควรมี ระบบดูแลข้อมูล
โดยภาพรวม
PG Slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ง่าย ฝากถอนสะดวก และเลือกเกมได้ จำนวนมาก เหมาะสำหรับ ผู้เล่นทุกสไตล์ ในโลกของเกมสล็อตออนไลน์
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-70cdb1132344
karayaz.ru · March 2, 2026 at 12:37 pm
strongest muscle building supplement
http://ezproxy.cityu.edu.hk/login?url=https://byizea.fr/js/pgs/?acheter_de_la_testosterone_2.html http://ezproxy.cityu.edu.hk
http://okprint.kz/user/nationpickle7/ okprint.kz
https://writeablog.net/boatcolor6/activtesto-gelules-prix-effet-avis-pharmacie-esquirol-r writeablog.net
https://shapiro-stage-3.hubstack.net/top-10-des-sites-pour-acheter-de-la-testosterone-testosterone-steroids-com shapiro-stage-3.hubstack.net
http://stroyrem-master.ru/user/clubsquare7/ http://stroyrem-master.ru/user/clubsquare7
http://premiumdesignsinc.com/forums/user/lilacsleet1/ http://premiumdesignsinc.com
https://poiskpredkov.by/members/hotbrass5/activity/720878/ https://poiskpredkov.by
https://yogicentral.science/wiki/Top_10_des_Sites_pour_Acheter_de_la_Testostrone_testosteronesteroids_com yogicentral.science
http://techou.jp/index.php?clubidea1 techou.jp
https://forum.issabel.org/u/jartank7 https://forum.issabel.org
https://algowiki.win/wiki/Post:Meilleur_booster_de_testostrone_Le_vrai_classement_du_pharmacien algowiki.win
https://www.giveawayoftheday.com/forums/profile/1668756 https://www.giveawayoftheday.com/
https://schwanger.mamaundbaby.com/user/kevinpiano4 schwanger.mamaundbaby.com
http://jobboard.piasd.org/author/dogbrass9/ jobboard.piasd.org
https://dlx.hamdard.pk/user/profile/437794 https://dlx.hamdard.pk/user/profile/437794
https://hedge.fachschaft.informatik.uni-kl.de/s/gpnoayAir https://hedge.fachschaft.informatik.uni-kl.de/s/gpnoayAir
https://www.blurb.com/user/peasleet8 http://www.blurb.com
https://www.youtube.com/redirect?q=https://byizea.fr/js/pgs/?acheter_de_la_testosterone_2.html https://www.youtube.com
References:
http://karayaz.ru/user/selectseason5/
www.garagesale.es · March 2, 2026 at 1:19 pm
10 times 100
https://opensourcebridge.science/wiki/ANDROTARDYL_250_mg_1_ml_prix_notice_effets_secondaires_posologie_solution_injectable_intramusculaire opensourcebridge.science
https://zenwriting.net/kevinrouter2/testosterone-medicament-pharmacie-risques-pourquoi https://zenwriting.net/kevinrouter2/testosterone-medicament-pharmacie-risques-pourquoi
http://digitaltibetan.win/index.php?title=Post:Viagra_sans_ordonnance_les_meilleures_alternatives_lgales_acheter&action=submit digitaltibetan.win
https://www.divephotoguide.com/user/selectlocket5 https://www.divephotoguide.com
https://rentry.co/fh3g3ryh https://rentry.co/
https://alushta-shirak.ru/user/lilacbit1/ alushta-shirak.ru
https://graph.org/Acheter-Sustanon-250-Injection-03-02 https://graph.org
https://classifieds.ocala-news.com/author/gardenbit0 classifieds.ocala-news.com
http://amur.1gb.ua/user/pearpeony5/ amur.1gb.ua
https://urlscan.io/result/019cadac-a902-755b-9fba-dadd8bb14ab3/ https://urlscan.io/result/019cadac-a902-755b-9fba-dadd8bb14ab3
http://digitaltibetan.win/index.php?title=Post:Viagra_sans_ordonnance_les_meilleures_alternatives_lgales_acheter&action=submit http://digitaltibetan.win/
https://diego-maradona.com.az/user/handsea0/ diego-maradona.com.az
https://medibang.com/author/27868048/ https://medibang.com/
https://medibang.com/author/27868048/ medibang.com
https://web.ggather.com/museumtank7/ https://web.ggather.com/museumtank7/
https://www.divephotoguide.com/user/selectlocket5 http://www.divephotoguide.com
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=clefdonald6 eskisehiruroloji.com
https://hedge.fachschaft.informatik.uni-kl.de/s/gpnoayAir https://hedge.fachschaft.informatik.uni-kl.de/s/gpnoayAir
References:
https://www.garagesale.es/author/topseason5/
chessdatabase.science · March 2, 2026 at 2:15 pm
making anabolic steroids
https://hack.allmende.io/s/Q6Qut8x94 hack.allmende.io
https://md.chaosdorf.de/s/MUkqEbMghJ md.chaosdorf.de
https://thybo-flores.thoughtlanes.net/t-c3-a9moignage-apport-de-testost-c3-a9rone-troubles-de-l-c3-a9rection-club-doctissimo-fr https://thybo-flores.thoughtlanes.net/
https://school-of-safety-russia.ru/user/boatsea6/ school-of-safety-russia.ru
https://www.giveawayoftheday.com/forums/profile/1668756 https://www.giveawayoftheday.com/
https://algowiki.win/wiki/Post:Meilleur_booster_de_testostrone_Le_vrai_classement_du_pharmacien algowiki.win
http://tropicana.maxlv.ru/user/clubfrog0/ http://tropicana.maxlv.ru
http://jobboard.piasd.org/author/dogbrass9/ jobboard.piasd.org
https://web.ggather.com/museumtank7/ https://web.ggather.com
https://www.giveawayoftheday.com/forums/profile/1668756 https://www.giveawayoftheday.com/forums/profile/1668756
https://atavi.com/share/xq4oxdzstbfi atavi.com
https://onlinevetjobs.com/author/topcoil4/ https://onlinevetjobs.com/
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=clefdonald6 eskisehiruroloji.com
https://doc.adminforge.de/s/ap_2RFkJnO doc.adminforge.de
https://500px.com/p/thiesenwlfchaney https://500px.com
https://medibang.com/author/27868048/ medibang.com
https://doodleordie.com/profile/selectrouter5 https://doodleordie.com
http://bioimagingcore.be/q2a/user/clefarrow5 http://bioimagingcore.be/
References:
https://chessdatabase.science/wiki/Testostrone_mdicament_pharmacie_risques_pourquoi
egamersbox.com · March 2, 2026 at 3:29 pm
is there a natural steroid
https://doodleordie.com/profile/selectrouter5 doodleordie.com
https://p.mobile9.com/pearsea5/ https://p.mobile9.com/pearsea5
https://peatix.com/user/29015226 https://peatix.com/
https://www.blurb.com/user/peasleet8 http://www.blurb.com
http://amur.1gb.ua/user/pearpeony5/ amur.1gb.ua
https://audiobook.net.pl/user/toptank1/ https://audiobook.net.pl/user/toptank1
https://thybo-flores.thoughtlanes.net/t-c3-a9moignage-apport-de-testost-c3-a9rone-troubles-de-l-c3-a9rection-club-doctissimo-fr thybo-flores.thoughtlanes.net
http://amur.1gb.ua/user/pearpeony5/ amur.1gb.ua
https://doodleordie.com/profile/selectrouter5 https://doodleordie.com/
https://www.investagrams.com/Profile/shapir3569383 http://www.investagrams.com
https://ajarproductions.com/pages/products/in5/answers/user/boatpeony2 https://ajarproductions.com/
https://wikimapia.org/external_link?url=https://byizea.fr/js/pgs/?acheter_de_la_testosterone_2.html https://wikimapia.org
https://egamersbox.com/cool/index.php?page=user&action=pub_profile&id=331094 https://egamersbox.com/cool/index.php?page=user&action=pub_profile&id=331094
https://alushta-shirak.ru/user/lilacbit1/ https://alushta-shirak.ru/user/lilacbit1
https://notes.io/escae notes.io
https://md.swk-web.com/s/hUzPET6Z2 https://md.swk-web.com/s/hUzPET6Z2
https://clinfowiki.win/wiki/Post:Douleur_une_nouvelle_tude_dsigne_la_testostrone_comme_un_antidouleur clinfowiki.win
https://kanban.xsitepool.tu-freiberg.de/s/Bke0S5aMK-l kanban.xsitepool.tu-freiberg.de
國產 av · March 2, 2026 at 4:11 pm
Excellent, what a weblog it is! This webpage presents helpful information to us, keep it up.
https://www.mixcloud.com/pearrouter4 · March 2, 2026 at 4:37 pm
anabolic steroids review
https://algowiki.win/wiki/Post:Meilleur_booster_de_testostrone_Le_vrai_classement_du_pharmacien algowiki.win
https://mapleprimes.com/users/dogbobcat8 mapleprimes.com
https://schoolido.lu/user/selectbow4/ https://schoolido.lu/user/selectbow4
https://peatix.com/user/29015226 peatix.com
https://opensourcebridge.science/wiki/ANDROTARDYL_250_mg_1_ml_prix_notice_effets_secondaires_posologie_solution_injectable_intramusculaire https://opensourcebridge.science/
https://moparwiki.win/wiki/Post:TESTAVAN_gel_23_mg_fl_dos_85_5_g_Commander_en_ligne https://moparwiki.win/wiki/Post:TESTAVAN_gel_23_mg_fl_dos_85_5_g_Commander_en_ligne
https://cox-flores-2.mdwrite.net/testosterone-achat-ou-acheter-de-la-testosterone-en-vente-libre cox-flores-2.mdwrite.net
https://king-wifi.win/wiki/Top_10_des_Sites_pour_Acheter_de_la_Testostrone_testosteronesteroids_com king-wifi.win
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1866059 gaiaathome.eu
https://quaildonald3.werite.net/guide-essentiel-pour-lachat-de-testosterone-securise https://quaildonald3.werite.net
https://sportpoisktv.ru/author/clefscent8/ https://sportpoisktv.ru/
https://fkwiki.win/wiki/Post:Acheter_Testosterone_en_ligne_meilleur_prix fkwiki.win
http://digitaltibetan.win/index.php?title=Post:Viagra_sans_ordonnance_les_meilleures_alternatives_lgales_acheter&action=submit digitaltibetan.win
https://pad.stuve.uni-ulm.de/s/x5pi3nlkPM pad.stuve.uni-ulm.de
https://mapleprimes.com/users/dogbobcat8 mapleprimes.com
https://md.swk-web.com/s/hUzPET6Z2 md.swk-web.com
https://algowiki.win/wiki/Post:Meilleur_booster_de_testostrone_Le_vrai_classement_du_pharmacien https://algowiki.win/
http://lida-stan.by/user/polandsoda4/ http://lida-stan.by/user/polandsoda4
References:
https://www.mixcloud.com/pearrouter4/
https://dreevoo.com · March 2, 2026 at 6:47 pm
effects steroids have on the body
http://uvs2.net/index.php/user/galloncamera1 http://uvs2.net/index.php/user/galloncamera1
https://schoolido.lu/user/sphynxsalary8/ https://schoolido.lu
http://karayaz.ru/user/sphynxarcher5/ http://karayaz.ru/
https://isowindows.net/user/hatnose3/ isowindows.net
https://pads.jeito.nl/s/raJxkQg_gd https://pads.jeito.nl
https://erickson-lam.mdwrite.net/buy-clenbuterol-the-best-steroid-source-online erickson-lam.mdwrite.net
https://mozillabd.science/wiki/Buy_Clenbuterol_Injection_200g_Genesis_for_42_00_legally_with_UK_delivery_online mozillabd.science
https://postheaven.net/shoearcher0/clenbuterol-for-sale-buy-clenbuterol-online-in-the-usa https://postheaven.net/shoearcher0/clenbuterol-for-sale-buy-clenbuterol-online-in-the-usa
http://celebratebro.in/birthdays-in-bangalore/index.php?qa=user&qa_1=sphynxaries1 http://celebratebro.in/birthdays-in-bangalore/index.php?qa=user&qa_1=sphynxaries1
https://audiobook.net.pl/user/foxgrade7/ https://audiobook.net.pl
https://wikimapia.org/external_link?url=https://thehollywoodtrainerclub.com/static/pgs/?buy_clenbuterol_4.html https://wikimapia.org
https://raindrop.io/wishnose1/pollockbarker3601-67636133 raindrop.io
https://rentry.co/zksvagwa rentry.co
https://web.ggather.com/edgestage6/ web.ggather.com
http://okprint.kz/user/fireddrain6/ http://okprint.kz/
https://lovewiki.faith/wiki/Clenbuterol_for_Weight_Loss_Does_It_Work https://lovewiki.faith/wiki/Clenbuterol_for_Weight_Loss_Does_It_Work
https://blogfreely.net/sudancarp3/clenbuterol-suppliers-usa blogfreely.net
https://cattletrailers.com.au/author/summerjeff4/ https://cattletrailers.com.au
References:
https://dreevoo.com/profile.php?pid=1186201
www.divephotoguide.com · March 2, 2026 at 7:45 pm
androgenic steroid
https://moparwiki.win/wiki/Post:Buy_Clenbuterol_at_a_Low_Price_from_a_Direct_Supplier_Arizona_US https://moparwiki.win
https://atavi.com/share/xq4thkz8dqh atavi.com
https://output.jsbin.com/rehadawasi/ output.jsbin.com
https://dokuwiki.stream/wiki/Clenbuterol_tablet_for_Sale_10mcg_100_tabs_Geno_Pharma_US_CA dokuwiki.stream
https://raindrop.io/wishnose1/pollockbarker3601-67636133 raindrop.io
https://bandori.party/user/507882/gallonrate9/ bandori.party
https://morphomics.science/wiki/Clenbuterol_40mcg_Cut_Fat_Quickly morphomics.science
https://500px.com/p/pittsrcaagger 500px.com
https://diego-maradona.com.az/user/mooncarp6/ https://diego-maradona.com.az/
https://dreevoo.com/profile.php?pid=1186201 dreevoo.com
http://volleypedia.org/index.php?qa=user&qa_1=rolldance3 volleypedia.org
https://elearnportal.science/wiki/Buy_Clenbuterol elearnportal.science
https://hedgedoc.eclair.ec-lyon.fr/s/QOQtvH6Po hedgedoc.eclair.ec-lyon.fr
http://kriminal-ohlyad.com.ua/user/wayyew2/ kriminal-ohlyad.com.ua
https://notes.io/escK9 notes.io
https://hedgedoc.eclair.ec-lyon.fr/s/QOQtvH6Po hedgedoc.eclair.ec-lyon.fr
https://to-portal.com/firedwoman6 to-portal.com
https://squareblogs.net/chestson6/clenbuterol-hydrochloride-genesis squareblogs.net
References:
https://www.divephotoguide.com/user/shoezebra4
levesque-gylling-2.thoughtlanes.net · March 2, 2026 at 8:13 pm
anabolic mass gainer side effects
References:
https://levesque-gylling-2.thoughtlanes.net/risks-and-safety-of-clenbuterol-for-bodybuilding
waywoman3.bravejournal.net · March 2, 2026 at 8:47 pm
winstrol for men
References:
https://waywoman3.bravejournal.net/buy-clenbuterol-usa-legal-clenbuterol-for-sale-online
premiumdesignsinc.com · March 2, 2026 at 9:29 pm
anabol 10
https://oiaedu.com/forums/users/moonbomber8/ https://oiaedu.com
https://mmcon.sakura.ne.jp:443/mmwiki/index.php?shoestage1 mmcon.sakura.ne.jp
https://digitaltibetan.win/wiki/Post:Buy_Clenbuterol_Generic_Online digitaltibetan.win
http://volleypedia.org/index.php?qa=user&qa_1=rolldance3 volleypedia.org
https://mozillabd.science/wiki/Buy_Clenbuterol_Injection_200g_Genesis_for_42_00_legally_with_UK_delivery_online https://mozillabd.science/
https://lit-book.ru/user/chestson4/ https://lit-book.ru/user/chestson4/
https://ccsakura.jp:443/index.php?wayjeff3 ccsakura.jp
https://skitterphoto.com/photographers/2379580/rodriguez-wynn skitterphoto.com
https://funsilo.date/wiki/Clenbuterol_Clen_An_Overview https://funsilo.date/wiki/Clenbuterol_Clen_An_Overview
https://hedgedoc.info.uqam.ca/s/XPN_72H4i hedgedoc.info.uqam.ca
https://bandori.party/user/507882/gallonrate9/ https://bandori.party/
https://aguirre-chappell.hubstack.net/crazy-bulk-clenbuterol-amazon-where-to-buy-amazon-or-official https://aguirre-chappell.hubstack.net
https://humanlove.stream/wiki/Where_To_Buy_Clenbuterol_Online_Safe_Websites https://humanlove.stream/
https://500px.com/p/pittsrcaagger 500px.com
https://peters-yde.technetbloggers.de/what-is-clenbuterol peters-yde.technetbloggers.de
http://karayaz.ru/user/sphynxarcher5/ http://karayaz.ru/user/sphynxarcher5/
https://pad.stuve.de/s/9ZEP1ZN9H pad.stuve.de
https://isowindows.net/user/hatnose3/ isowindows.net
References:
http://premiumdesignsinc.com/forums/user/spleenarcher5/
ezproxy.cityu.edu.hk · March 2, 2026 at 10:55 pm
pics of bodybuilders on steroids
https://oiaedu.com/forums/users/moonbomber8/ https://oiaedu.com/forums/users/moonbomber8
https://humanlove.stream/wiki/Where_To_Buy_Clenbuterol_Online_Safe_Websites https://humanlove.stream
https://oiaedu.com/forums/users/moonbomber8/ oiaedu.com
https://erickson-lam.mdwrite.net/buy-clenbuterol-the-best-steroid-source-online erickson-lam.mdwrite.net
http://celebratebro.in/birthdays-in-bangalore/index.php?qa=user&qa_1=sphynxaries1 celebratebro.in
http://jobboard.piasd.org/author/teafamily7/ http://jobboard.piasd.org/author/teafamily7
http://okprint.kz/user/fireddrain6/ http://okprint.kz/user/fireddrain6
https://wikimapia.org/external_link?url=https://thehollywoodtrainerclub.com/static/pgs/?buy_clenbuterol_4.html wikimapia.org
https://www.garagesale.es/author/lizardrate2/ http://www.garagesale.es
https://oiaedu.com/forums/users/moonbomber8/ oiaedu.com
https://bandori.party/user/507882/gallonrate9/ bandori.party
https://atavi.com/share/xq4thkz8dqh https://atavi.com/share/xq4thkz8dqh
https://500px.com/p/pittsrcaagger 500px.com
https://ellington-castaneda.federatedjournals.com/top-weight-loss-medications ellington-castaneda.federatedjournals.com
https://funsilo.date/wiki/Clenbuterol_Clen_An_Overview https://funsilo.date/wiki/Clenbuterol_Clen_An_Overview
http://karayaz.ru/user/sphynxarcher5/ karayaz.ru
http://okprint.kz/user/fireddrain6/ okprint.kz
http://kriminal-ohlyad.com.ua/user/wayyew2/ kriminal-ohlyad.com.ua
References:
http://ezproxy.cityu.edu.hk/login?url=https://thehollywoodtrainerclub.com/static/pgs/?buy_clenbuterol_4.html
https://sfenglishlessons.com · March 2, 2026 at 11:28 pm
new bodybuilding drug
https://pad.geolab.space/s/sw5nujXLP pad.geolab.space
https://www.udrpsearch.com/user/moononion4 http://www.udrpsearch.com
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=edgeson7 eskisehiruroloji.com
https://moparwiki.win/wiki/Post:Buy_Clenbuterol_at_a_Low_Price_from_a_Direct_Supplier_Arizona_US moparwiki.win
http://volleypedia.org/index.php?qa=user&qa_1=rolldance3 volleypedia.org
https://md.chaosdorf.de/s/nSSENdwlTZ md.chaosdorf.de
https://ccsakura.jp:443/index.php?wayjeff3 ccsakura.jp
https://alushta-shirak.ru/user/chestdance0/ alushta-shirak.ru
https://nhadat24.org/author/sphynxonion0 https://nhadat24.org/author/sphynxonion0
https://pads.jeito.nl/s/raJxkQg_gd pads.jeito.nl
https://pads.zapf.in/s/ytHh9jJvg6 pads.zapf.in
https://mapleprimes.com/users/spleenfamily5 https://mapleprimes.com
https://dokuwiki.stream/wiki/Clenbuterol_tablet_for_Sale_10mcg_100_tabs_Geno_Pharma_US_CA dokuwiki.stream
https://trade-britanica.trade/wiki/Clenbuterol_suppliers_USA https://trade-britanica.trade/
https://firsturl.de/gf5yY4c https://firsturl.de/
https://notes.io/escK9 https://notes.io/escK9
http://uvs2.net/index.php/user/galloncamera1 http://uvs2.net/
https://pattern-wiki.win/wiki/Clenbuterol_Clen_An_Overview pattern-wiki.win
References:
https://sfenglishlessons.com/members/shoewaiter4/activity/582390/
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1866094 · March 3, 2026 at 1:43 am
how much are steroids
References:
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1866094
matkafasi.com · March 3, 2026 at 2:16 am
steroids for working out
References:
https://matkafasi.com/user/wishforce4
ajarproductions.com · March 3, 2026 at 7:50 am
steroids for bodybuilding side effects
References:
https://ajarproductions.com/pages/products/in5/answers/user/quillgrade1
Jasonsuide · March 4, 2026 at 12:41 am
pg
แพลตฟอร์ม TKBNEKO พาคุณสู่โลกใหม่ของเกมเดิมพันออนไลน์ ระบบการเงินรวดเร็ว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคที่ เทคโนโลยีเปลี่ยนวิถีการเดิมพันออนไลน์ไปอย่างสิ้นเชิง TKBNEKO เข้ามาสร้างมาตรฐานใหม่ให้กับวงการ ด้วยระบบการให้บริการที่ ทันสมัย รวดเร็ว และ โปร่งใส พร้อมต้อนรับสมาชิกทุกท่านสู่ โลกแห่งเกมที่เหนือกว่าเดิม ที่ ตอบโจทย์ทั้งมือใหม่และมืออาชีพ
เหตุผลที่ควรเลือก TKBNEKO
TKBNEKO มุ่งมั่นที่จะมอบประสบการณ์จากเกมลิขสิทธิ์แท้ โดยเฉพาะเกมที่ ได้รับการตรวจสอบจากองค์กรสากล และ ได้รับการยอมรับมากที่สุดในอุตสาหกรรม เพื่อให้ผู้เล่นทุกคน สบายใจ ได้ว่า จะได้รับความเพลิดเพลินกับเกมที่ โปร่งใส ปลอดภัย และ มีคุณภาพสูง
จุดเด่นของระบบฝาก-ถอน
เราออกแบบระบบการเงินให้ง่ายและเร็วที่สุด เพื่อให้คุณ เพลิดเพลินกับการเดิมพันอย่างต่อเนื่อง
ฝากขั้นต่ำ: เพียง 1 บาท
ถอนขั้นต่ำ: เพียง 1 บาท
เวลาฝากเงิน: ใช้เวลาเพียง 3 วินาที
ยอดจำกัดการถอน: ไม่มียอดจำกัดต่อวัน
ฝากง่าย เพียงสแกน QR Code
เพียงคุณสแกน QR Code ระบบของเราจะ โอนเงินเข้าระบบทันที ขั้นต่ำเพียง 100 บาท และสามารถฝากได้สูงถึง ไม่เกิน 500,000 บาทต่อครั้ง เริ่มต้นได้ทันที กับ TKBNEKO ที่ ใช้งานง่าย ทำกำไรได้รวดเร็ว
หมวดหมู่เกมที่ครบครัน
แพลตฟอร์มของเราครอบคลุมทุกแนวเกม รองรับทุกความชอบของผู้เล่น
สล็อต: ธีมมากมาย พร้อมลุ้นรางวัลใหญ่
เกมสด: เล่นสดเหมือนอยู่ในคาสิโนจริง
กีฬา: เดิมพันกับแมตช์การแข่งขันจากทั่วโลก
ยิงปลา: ลุ้นกำไรจากเกมยิงปลา
อัปเดตโปรโมชันล่าสุด
อย่าลืมแวะมาเยี่ยมชมที่หน้า โปรโมชั่น เพื่อรับ สิทธิพิเศษมากมาย ที่เรามอบให้สมาชิกทุกท่าน นอกจากนี้ยังมีระบบ สมาชิกวีไอพี สำหรับลูกค้าคนสำคัญ และช่องทาง แอฟฟิลิเอต สำหรับผู้ที่สนใจสร้างรายได้ร่วมกับเรา
ช่องทางติดต่อ
หากมี คำถาม หรือ ข้อเสนอแนะ สามารถติดต่อทีมงานของเราได้ตลอด 24 ชั่วโมงที่หน้า ฝ่ายสนับสนุน และ แบบฟอร์มติดต่อ ทีมงาน ของเรา ยินดีให้บริการทุกท่านด้วยใจ
av 女優 · March 4, 2026 at 1:53 am
Thanks in support of sharing such a pleasant opinion, piece of writing is good, thats why i have read it completely
BradleyBit · March 4, 2026 at 4:12 am
ทดลองเล่นสล็อต pg เว็บ ตรง”
pg slot แพลตฟอร์มเกมสล็อตยอดนิยม เข้าเล่นไว ฝากถอนออโต้
คำค้นหา สล็อต PG ถูกค้นหามากขึ้นเรื่อยๆ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน ภาพและเอฟเฟกต์ ความ ลื่นไหล และ โอกาสรับกำไรที่ดี เกมของ PG พัฒนาโดยผู้ให้บริการชั้นนำ ที่รองรับการเล่นทั้งบน มือถือ และ เดสก์ท็อป
ข้อดี ของ สล็อต PG
pg slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เข้าเกมไว เล่นผ่าน ระบบเว็บ และรองรับ ทุกแพลตฟอร์ม เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน เว็บเบราว์เซอร์ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ เอฟเฟกต์ 3 มิติ ให้ความคมชัด พร้อมเอฟเฟกต์ จัดเต็ม
คุณสมบัติหลักของเกม pg slot ได้แก่
มีรอบโบนัสให้ลุ้นบ่อย
ระบบตัวคูณ
เล่นฟรีก่อนเติมเงิน
รองรับภาษาไทยเต็มรูปแบบ
ระบบฝากถอนสะดวก ทำรายการไว
แพลตฟอร์ม pg slot ส่วนใหญ่รองรับ การฝาก-ถอน ออโต้ตลอด 24 ชม. ขั้นต่ำเริ่มต้นเพียง 10 บาท ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา เพียงไม่กี่วินาที ผ่าน QR Code หรือระบบ Mobile Banking ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
ประเภทเกมยอดนิยม ใน pg slot
เกม สล็อต PG มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม ลุยด่าน
ธีม โชคลาภ
ธีม Animal
หลายคนชอบเกมที่โบนัสเข้าไว พร้อมระบบ Special Feature และ ระบบจ่ายคุ้มค่า เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นมือโปร
มาตรฐานระบบ
สล็อต PG พัฒนาในระบบสากล มีการ เข้ารหัสข้อมูล และใช้ระบบสุ่มผล RNG เพื่อให้ผลลัพธ์ ตรวจสอบได้ แพลตฟอร์มที่ให้บริการ สล็อต PG ควรมี ความปลอดภัยสูง
โดยภาพรวม
pg slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ไว ผู้เล่นสามารถเริ่มต้นได้ ไม่ซับซ้อน ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ผู้เล่นทุกสไตล์ ในโลกของเกมสล็อตออนไลน์
RodneyChoix · March 4, 2026 at 4:12 am
ทดลองเล่นสล็อต pg
แพลตฟอร์ม TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ทันสมัย รวดเร็ว และ ตรวจสอบได้ เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
ระบบการเงินที่ใช้งานง่าย
ฝากขั้นต่ำ: 1 บาท
ถอนขั้นต่ำ: 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่มีลิมิต
เติมเงินง่าย แค่สแกน
สแกน คิวอาร์ ระบบจะ โอนเงินเข้าทันที ขั้นต่ำ เริ่ม 100 บาท สูงสุด 500,000 บาท
เกมยอดนิยม
สล็อต: ลุ้นแจ็คพอต
เกมสด: ดีลเลอร์สด
กีฬา: แมตช์ทั่วโลก
ยิงปลา: สนุกได้เงินจริง
โบนัสและโปรโมชัน
ติดตามหน้า โปรโมชั่น พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม พันธมิตร
ติดต่อเรา
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ติดต่อเรา ทีมงาน TKBNEKO พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-e598fa477f69
winpot · March 4, 2026 at 8:05 pm
Hello superb website! Does running a blog such as this require a large amount of work? I’ve absolutely no understanding of coding however I had been hoping to start my own blog in the near future. Anyway, should you have any recommendations or techniques for new blog owners please share. I understand this is off topic however I simply wanted to ask. Kudos!
Jacobdaw · March 4, 2026 at 10:08 pm
Надежные специалисты предлагают базы хрумера купить, чтобы упростить процесс работы.
FelixGug · March 5, 2026 at 2:10 am
สล็อต
TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว TKBNEKO พร้อมยกระดับการให้บริการ ด้วยระบบที่ ทันสมัย เสถียร และ ตรวจสอบได้ เพื่อให้ผู้เล่น อุ่นใจ ทุกครั้งที่ใช้งาน
จุดเด่นระบบฝาก-ถอน
ฝากขั้นต่ำ: เริ่มต้น 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ใช้เวลาเพียง 3 วินาที
ยอดถอน: ไม่มีลิมิต
ฝากง่าย เพียงสแกน QR Code
สแกน คิวอาร์ ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ เริ่ม 100 บาท สูงสุด 500,000 บาท
หมวดหมู่เกม
สล็อต: ลุ้นแจ็คพอต
เกมสด: คาสิโนเรียลไทม์
กีฬา: เดิมพันลีกดัง
ยิงปลา: สนุกได้เงินจริง
โบนัสและโปรโมชัน
ติดตามหน้า โปรโมชั่น พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม พันธมิตร
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ติดต่อเรา ทีมงาน ของเรา พร้อมดูแลตลอดเวลา
Travisjal · March 5, 2026 at 2:12 am
สล็อต
TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ทันสมัย รวดเร็ว และ ตรวจสอบได้ เพื่อให้ผู้เล่น อุ่นใจ ทุกครั้งที่ใช้งาน
ระบบการเงินที่ใช้งานง่าย
ฝากขั้นต่ำ: 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
เติมเงินง่าย แค่สแกน
สแกน คิวอาร์ ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ 100 บาท สูงสุด ไม่เกิน 500,000 บาทต่อครั้ง
เกมยอดนิยม
สล็อต: ธีมหลากหลาย
เกมสด: คาสิโนเรียลไทม์
กีฬา: แมตช์ทั่วโลก
ยิงปลา: ลุ้นกำไรทันที
โปรโมชั่นและสิทธิพิเศษ
ติดตามหน้า โบนัส พร้อมระบบ VIP และโปรแกรม แอฟฟิลิเอต
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ศูนย์ช่วยเหลือ ทีมงาน TKBNEKO พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-a4ea8e21fdde
注册以获取100 USDT · March 5, 2026 at 9:59 am
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
Jasonsuide · March 5, 2026 at 2:41 pm
TKBNEKO มอบมิติใหม่ของการเดิมพันออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน QR Code
ในยุคที่ เทคโนโลยีเปลี่ยนวิถีการเดิมพันออนไลน์ไปอย่างสิ้นเชิง TKBNEKO เข้ามาสร้างมาตรฐานใหม่ให้กับวงการ ด้วยระบบการให้บริการที่ ล้ำสมัย ฉับไว และ ตรวจสอบได้ พร้อมต้อนรับสมาชิกทุกท่านสู่ ประสบการณ์ความบันเทิงรูปแบบใหม่ ที่ ใครๆ ก็เป็นเถ้าแก่ได้
เพราะอะไรหลายคนจึงเลือก TKBNEKO
TKBNEKO มุ่งมั่นที่จะมอบประสบการณ์จากเกมลิขสิทธิ์แท้ โดยเฉพาะเกมที่ มีใบรับรองอย่างถูกต้อง และ เป็นที่นิยมในระดับสากล เพื่อให้ผู้เล่นทุกคน สบายใจ ได้ว่า จะได้รับความเพลิดเพลินกับเกมที่ ไม่มีการเอาเปรียบ มีระบบรักษาความปลอดภัยสูง และ ตอบโจทย์ผู้เล่นยุคใหม่
ระบบการเงินที่เหนือกว่า
เรามุ่งเน้นความสะดวกของผู้เล่น เพื่อให้คุณ เพลิดเพลินกับการเดิมพันอย่างต่อเนื่อง
ฝากขั้นต่ำ: เพียง 1 บาท
ถอนขั้นต่ำ: เพียง 1 บาท
เวลาฝากเงิน: รวดเร็วทันใจใน 3 วินาที
ยอดจำกัดการถอน: ไม่มีลิมิตการถอนรายวัน
เติมเงินง่ายด้วย QR Code
เพียงคุณสแกน QR Code ระบบของเราจะ โอนเงินเข้าระบบทันที ขั้นต่ำเพียง เริ่มต้น 100 บาท และสามารถฝากได้สูงถึง สูงสุด 500,000 บาท มาร่วมสนุกกันได้แล้ววันนี้ กับ TKBNEKO ที่ ตอบโจทย์การเดิมพันยุคใหม่
หมวดหมู่เกมที่ครบครัน
TKBNEKO รวมเกมสุดฮิตไว้ในที่เดียว รองรับทุกความชอบของผู้เล่น
สล็อต: ธีมมากมาย พร้อมลุ้นรางวัลใหญ่
เกมสด: ดีลเลอร์ถ่ายทอดสดตลอดเวลา
กีฬา: เดิมพันกับแมตช์การแข่งขันจากทั่วโลก
ยิงปลา: สนุกกับการยิงปลาแบบได้เงิน
อัปเดตโปรโมชันล่าสุด
อย่าลืมแวะมาเยี่ยมชมที่หน้า โปรโมชั่น เพื่อรับ สิทธิพิเศษมากมาย ที่เรามอบให้สมาชิกทุกท่าน นอกจากนี้ยังมีระบบ ลูกค้าระดับพรีเมียม สำหรับลูกค้าคนสำคัญ และช่องทาง พันธมิตร สำหรับผู้ที่สนใจสร้างรายได้ร่วมกับเรา
ติดต่อเรา
หากมี ปัญหา หรือ ข้อเสนอแนะ สามารถติดต่อทีมงานของเราได้ตลอด 24 ชั่วโมงที่หน้า ฝ่ายสนับสนุน และ ข้อเสนอแนะ ทีมงาน ของเรา ยินดีให้บริการทุกท่านด้วยใจ
RodneyChoix · March 5, 2026 at 5:14 pm
ทดลองเล่นสล็อต pg
TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ โลกออนไลน์เติบโตต่อเนื่อง เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ล้ำสมัย รวดเร็ว และ โปร่งใส เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
จุดเด่นระบบฝาก-ถอน
ฝากขั้นต่ำ: 1 บาท
ถอนขั้นต่ำ: 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
ฝากง่าย เพียงสแกน QR Code
สแกน QR Code ระบบจะ โอนเงินเข้าทันที ขั้นต่ำ 100 บาท สูงสุด ไม่เกิน 500,000 บาทต่อครั้ง
เกมยอดนิยม
สล็อต: ลุ้นแจ็คพอต
เกมสด: คาสิโนเรียลไทม์
กีฬา: แมตช์ทั่วโลก
ยิงปลา: ลุ้นกำไรทันที
โปรโมชั่นและสิทธิพิเศษ
ติดตามหน้า โปรโมชั่น พร้อมระบบ สมาชิกพรีเมียม และโปรแกรม พันธมิตร
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ศูนย์ช่วยเหลือ ทีมงาน ของเรา พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-e598fa477f69
winpot · March 5, 2026 at 5:15 pm
Having read this I believed it was really enlightening. I appreciate you taking the time and effort to put this information together. I once again find myself personally spending a significant amount of time both reading and leaving comments. But so what, it was still worth it!
JosephBer · March 5, 2026 at 8:42 pm
ทดลองเล่นสล็อต pg
PG Slot แพลตฟอร์มเกมสล็อตยอดนิยม เข้าเล่นไว ฝากถอนออโต้
คำค้นหา สล็อต PG มาแรงในช่วงนี้ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน งานภาพคุณภาพสูง ความ ลื่นไหล และ ระบบจ่ายที่ดึงดูด เกมของ PG ผลิตโดยค่ายมาตรฐาน ที่รองรับการเล่นทั้งบน มือถือ และ คอมพิวเตอร์
ข้อดี ของ pg slot
สล็อต PG เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบเว็บ และรองรับ ทุกแพลตฟอร์ม เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน เว็บเบราว์เซอร์ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ จัดเต็ม
คุณสมบัติหลักของเกม PG Slot ได้แก่
ระบบโบนัสและฟรีสปินหลากหลายรูปแบบ
ระบบตัวคูณ
เล่นฟรีก่อนเติมเงิน
ใช้งานภาษาไทยง่าย
ระบบฝากถอนสะดวก ไม่ต้องรอนาน
แพลตฟอร์ม PG Slot มักมี การฝาก-ถอน ฝากถอนตลอดเวลา ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา ไม่กี่วินาที ผ่าน สแกน QR หรือระบบ แอปธนาคาร ทำให้ธุรกรรมเป็นไปอย่าง ต่อเนื่อง
แนวเกมที่คนเล่นเยอะ ใน PG Slot
เกม PG Slot มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม Adventure
ธีม เอเชียและโชคลาภ
ธีม ธรรมชาติ
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ โบนัสรอบพิเศษ และ โอกาสทำกำไรสูง เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นที่มีประสบการณ์
ความน่าเชื่อถือ
สล็อต PG มีมาตรฐานรองรับ มีการ ปกป้องข้อมูลผู้เล่น และใช้ระบบสุ่มผล RNG เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ สล็อต PG ควรมี ความปลอดภัยสูง
บทสรุปท้ายบท
pg slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ไม่ซับซ้อน ฝากถอนสะดวก และเลือกเกมได้ จำนวนมาก เหมาะสำหรับ ผู้เล่นทุกสไตล์ ในโลกของเกมสล็อตออนไลน์
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-70cdb1132344
Josephneupt · March 5, 2026 at 8:43 pm
ทดลองเล่นสล็อต pg ฟรี PG Slot เกมสล็อตออนไลน์ที่คนค้นหาเยอะ เล่นง่าย ฝากถอนเร็ว
คำค้นหา pg slot กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ผู้ให้บริการเกมสล็อตที่มาแรง ด้าน ภาพและเอฟเฟกต์ ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ผลิตโดยค่ายมาตรฐาน ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ เดสก์ท็อป
ข้อดี ของ pg slot
สล็อต PG เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เข้าเกมไว เล่นผ่าน ระบบออนไลน์ และรองรับ ทุกอุปกรณ์ ไม่ต้องติดตั้งเพิ่มเติม ผู้เล่นสามารถเข้าเล่นผ่าน เว็บเบราว์เซอร์ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ 3D ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม PG Slot ได้แก่
ระบบโบนัสและฟรีสปินหลากหลายรูปแบบ
ระบบตัวคูณ
โหมดทดลองเล่นฟรี
รองรับภาษาไทยเต็มรูปแบบ
ระบบการเงินรวดเร็ว ไม่ต้องรอนาน
แพลตฟอร์ม สล็อต PG มักมี การฝาก-ถอน ฝากถอนตลอดเวลา ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา รวดเร็วมาก ผ่าน QR Code หรือระบบ ธนาคารบนมือถือ ทำให้ธุรกรรมเป็นไปอย่าง ไม่สะดุด
หมวดเกมฮิต ใน PG Slot
เกม สล็อต PG มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม ลุยด่าน
ธีม ความมั่งคั่ง
ธีม สัตว์และธรรมชาติ
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ Special Feature และ อัตราการจ่ายที่สูง เหมาะกับทั้ง มือใหม่ และ สายสล็อตจริงจัง
ความปลอดภัย
pg slot พัฒนาในระบบสากล มีการ ปกป้องข้อมูลผู้เล่น และใช้ระบบสุ่มผล Random Number Generator เพื่อให้ผลลัพธ์ ตรวจสอบได้ แพลตฟอร์มที่ให้บริการ สล็อต PG ควรมี ความปลอดภัยสูง
บทสรุปท้ายบท
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน โบนัสหลากหลาย และการทำธุรกรรมที่ รวดเร็ว ผู้เล่นสามารถเริ่มต้นได้ ไม่ซับซ้อน ฝากถอนสะดวก และเลือกเกมได้ จำนวนมาก เหมาะสำหรับ ผู้เล่นทุกสไตล์ ในโลกของเกมสล็อตออนไลน์
tuan88 · March 5, 2026 at 9:21 pm
tuan88
BradleyBit · March 6, 2026 at 4:47 am
PG Slot เกมสล็อตออนไลน์ที่คนค้นหาเยอะ เล่นง่าย ฝากถอนเร็ว
คำค้นหา PG Slot กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน ภาพและเอฟเฟกต์ ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ออกแบบโดยทีมงานมืออาชีพ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ พีซี
ความโดดเด่น ของ สล็อต PG
pg slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เข้าเกมไว เล่นผ่าน ระบบเว็บ และรองรับ ทั้ง iOS และ Android ไม่ต้องติดตั้งเพิ่มเติม ผู้เล่นสามารถเข้าเล่นผ่าน หน้าเว็บ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สมจริง
คุณสมบัติหลักของเกม pg slot ได้แก่
ระบบโบนัสและฟรีสปินหลากหลายรูปแบบ
ฟีเจอร์ตัวคูณรางวัล
เดโม่ฟรี
รองรับภาษาไทยเต็มรูปแบบ
ฝากถอนง่าย ทำรายการไว
แพลตฟอร์ม pg slot มักมี การฝาก-ถอน ออโต้ตลอด 24 ชม. ขั้นต่ำเริ่มต้นเพียง 10 บาท ขึ้นอยู่กับ กติกาแต่ละแพลตฟอร์ม การทำรายการใช้เวลา ไม่กี่วินาที ผ่าน คิวอาร์โค้ด หรือระบบ แอปธนาคาร ทำให้ธุรกรรมเป็นไปอย่าง ไม่สะดุด
ประเภทเกมยอดนิยม ใน pg slot
เกม PG Slot มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม Adventure
ธีม โชคลาภ
ธีม ธรรมชาติ
เกมยอดนิยมมักเป็นเกมที่แตกง่าย พร้อมระบบ โบนัสรอบพิเศษ และ อัตราการจ่ายที่สูง เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นที่มีประสบการณ์
มาตรฐานระบบ
PG Slot พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล ระบบสุ่มมาตรฐาน เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ทีมซัพพอร์ต 24 ชม.
สรุป
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ง่าย ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
Jasonsuide · March 7, 2026 at 3:21 am
TKBNEKO พาคุณสู่โลกใหม่ของเกมเดิมพันออนไลน์ ระบบการเงินรวดเร็ว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคที่ นวัตกรรมดิจิทัลเข้ามาปรับโฉมวงการเกมออนไลน์ TKBNEKO ขอเป็นส่วนหนึ่งในการปฏิวัติวงการเกม ด้วยระบบการให้บริการที่ อัปเดตตลอดเวลา รวดเร็ว และ โปร่งใส พร้อมต้อนรับสมาชิกทุกท่านสู่ โลกแห่งเกมที่เหนือกว่าเดิม ที่ ตอบโจทย์ทั้งมือใหม่และมืออาชีพ
ทำไมต้อง TKBNEKO?
แพลตฟอร์มของเรารวบรวมเกมที่ได้มาตรฐาน โดยเฉพาะเกมที่ ผ่านการรับรองจากสถาบันที่น่าเชื่อถือ และ เป็นที่นิยมในระดับสากล เพื่อให้ผู้เล่นทุกคน มั่นใจ ได้ว่า จะได้รับความเพลิดเพลินกับเกมที่ โปร่งใส ปลอดภัย และ มีคุณภาพสูง
จุดเด่นของระบบฝาก-ถอน
เรามุ่งเน้นความสะดวกของผู้เล่น เพื่อให้คุณ โฟกัสกับความสนุกได้อย่างเต็มที่
ฝากขั้นต่ำ: ขั้นต่ำแค่ 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: รวดเร็วทันใจใน 3 วินาที
ยอดจำกัดการถอน: ไม่มียอดจำกัดต่อวัน
ธุรกรรมสะดวก แค่สแกนคิวอาร์
เพียงคุณสแกน โค้ดคิวอาร์ ระบบของเราจะ ดำเนินการฝากเงินให้อัตโนมัติ ขั้นต่ำเพียง 100 บาท และสามารถฝากได้สูงถึง ไม่เกิน 500,000 บาทต่อครั้ง เริ่มต้นได้ทันที กับ แพลตฟอร์มของเรา ที่ ใช้งานง่าย ทำกำไรได้รวดเร็ว
คลังเกมคุณภาพ
แพลตฟอร์มของเราครอบคลุมทุกแนวเกม รองรับทุกความชอบของผู้เล่น
สล็อต: ธีมมากมาย พร้อมลุ้นรางวัลใหญ่
เกมสด: สัมผัสประสบการณ์คาสิโนแบบเรียลไทม์
กีฬา: เดิมพันกับแมตช์การแข่งขันจากทั่วโลก
ยิงปลา: สนุกกับการยิงปลาแบบได้เงิน
รับโบนัสและข้อเสนอสุดคุ้ม
อย่าลืมแวะมาเยี่ยมชมที่หน้า โปรโมชันล่าสุด เพื่อรับ ของรางวัลพิเศษ ที่เรามอบให้สมาชิกทุกท่าน นอกจากนี้ยังมีระบบ ลูกค้าระดับพรีเมียม สำหรับลูกค้าคนสำคัญ และช่องทาง พาร์ทเนอร์ สำหรับผู้ที่สนใจสร้างรายได้ร่วมกับเรา
ติดต่อเรา
หากมี ปัญหา หรือ ความคิดเห็น สามารถติดต่อทีมงานของเราได้ตลอด 24 ชั่วโมงที่หน้า ศูนย์ช่วยเหลือ และ แบบฟอร์มติดต่อ ทีมงาน TKBNEKO ยินดีให้บริการทุกท่านด้วยใจ
RodneyChoix · March 7, 2026 at 7:19 pm
ทดลองเล่นสล็อต pg
แพลตฟอร์ม TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ฝาก-ถอนไว ด้วยระบบสแกน คิวอาร์โค้ด
ในยุคดิจิทัลที่ โลกออนไลน์เติบโตต่อเนื่อง เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ทันสมัย เสถียร และ ตรวจสอบได้ เพื่อให้ผู้เล่น อุ่นใจ ทุกครั้งที่ใช้งาน
จุดเด่นระบบฝาก-ถอน
ฝากขั้นต่ำ: เริ่มต้น 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ภายใน 3 วินาที
ยอดถอน: ไม่มีลิมิต
เติมเงินง่าย แค่สแกน
สแกน คิวอาร์ ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ 100 บาท สูงสุด 500,000 บาท
หมวดหมู่เกม
สล็อต: ธีมหลากหลาย
เกมสด: คาสิโนเรียลไทม์
กีฬา: แมตช์ทั่วโลก
ยิงปลา: ลุ้นกำไรทันที
โบนัสและโปรโมชัน
ติดตามหน้า โบนัส พร้อมระบบ VIP และโปรแกรม แอฟฟิลิเอต
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ศูนย์ช่วยเหลือ ทีมงาน ของเรา พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-e598fa477f69
"oppna binance-konto · March 8, 2026 at 12:05 am
Your article helped me a lot, is there any more related content? Thanks! https://accounts.binance.info/ro/register?ref=HX1JLA6Z
BradleyBit · March 8, 2026 at 12:37 pm
PG Slot แพลตฟอร์มเกมสล็อตยอดนิยม เล่นง่าย ฝากถอนเร็ว
คำค้นหา สล็อต PG มาแรงในช่วงนี้ ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน งานภาพคุณภาพสูง ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ผลิตโดยค่ายมาตรฐาน ที่รองรับการเล่นทั้งบน มือถือ และ พีซี
ข้อดี ของ pg slot
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เปิดเกมได้ทันที เล่นผ่าน ระบบออนไลน์ และรองรับ ทุกอุปกรณ์ ไม่ต้องดาวน์โหลดแอป ผู้เล่นสามารถเข้าเล่นผ่าน เว็บเบราว์เซอร์ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ เอฟเฟกต์ 3 มิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
มีรอบโบนัสให้ลุ้นบ่อย
ฟีเจอร์ตัวคูณรางวัล
เล่นฟรีก่อนเติมเงิน
ใช้งานภาษาไทยง่าย
ระบบการเงินรวดเร็ว ไม่ต้องรอนาน
แพลตฟอร์ม PG Slot โดยทั่วไปให้บริการ การฝาก-ถอน ฝากถอนตลอดเวลา ขั้นต่ำเริ่มต้นเพียง 1 บาท ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา ไม่กี่วินาที ผ่าน QR Code หรือระบบ ธนาคารบนมือถือ ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
แนวเกมที่คนเล่นเยอะ ใน PG Slot
เกม pg slot มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม ลุยด่าน
ธีม โชคลาภ
ธีม Animal
เกมยอดนิยมมักเป็นเกมที่แตกง่าย พร้อมระบบ Special Feature และ โอกาสทำกำไรสูง เหมาะกับทั้ง คนเพิ่งเล่น และ สายสล็อตจริงจัง
ความปลอดภัย
pg slot พัฒนาในระบบสากล มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล RNG เพื่อให้ผลลัพธ์ ยุติธรรม แพลตฟอร์มที่ให้บริการ pg slot ควรมี ความปลอดภัยสูง
โดยภาพรวม
pg slot เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ไว ผู้เล่นสามารถเริ่มต้นได้ ทันที ฝากถอนสะดวก และเลือกเกมได้ หลากหลายแนว เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
Travisjal · March 8, 2026 at 12:45 pm
สล็อต
แพลตฟอร์ม TKBNEKO มอบมิติใหม่ของเกมออนไลน์ ธุรกรรมรวดเร็ว ด้วยระบบสแกน QR Code
ในยุคดิจิทัลที่ เทคโนโลยีพัฒนาอย่างรวดเร็ว เรามุ่งเน้นมาตรฐานใหม่ของการเดิมพัน ด้วยระบบที่ ล้ำสมัย รวดเร็ว และ โปร่งใส เพื่อให้ผู้เล่น มั่นใจ ทุกครั้งที่ใช้งาน
จุดเด่นระบบฝาก-ถอน
ฝากขั้นต่ำ: 1 บาท
ถอนขั้นต่ำ: ขั้นต่ำ 1 บาท
เวลาฝากเงิน: ใช้เวลาเพียง 3 วินาที
ยอดถอน: ไม่จำกัดต่อวัน
เติมเงินง่าย แค่สแกน
สแกน คิวอาร์ ระบบจะ ประมวลผลอัตโนมัติ ขั้นต่ำ 100 บาท สูงสุด 500,000 บาท
เกมยอดนิยม
สล็อต: ลุ้นแจ็คพอต
เกมสด: ดีลเลอร์สด
กีฬา: เดิมพันลีกดัง
ยิงปลา: ลุ้นกำไรทันที
โบนัสและโปรโมชัน
ติดตามหน้า โปรโมชั่น พร้อมระบบ VIP และโปรแกรม แอฟฟิลิเอต
ฝ่ายบริการลูกค้า
สอบถามข้อมูลได้ตลอด 24 ชั่วโมง ผ่านหน้า ติดต่อเรา ทีมงาน TKBNEKO พร้อมดูแลตลอดเวลา
https://medium.com/@ratypw/ทดลองเล่นสล็อต-a4ea8e21fdde
колие · March 8, 2026 at 12:55 pm
златни бижута
Charlestub · March 8, 2026 at 1:02 pm
ทดลองเล่นสล็อต pg
pg slot แพลตฟอร์มเกมสล็อตยอดนิยม เข้าเล่นไว ฝากถอนออโต้
คำค้นหา pg slot กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน ภาพและเอฟเฟกต์ ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG พัฒนาโดยผู้ให้บริการชั้นนำ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ พีซี
ความโดดเด่น ของ pg slot
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบออนไลน์ และรองรับ ทั้ง iOS และ Android ไม่ต้องดาวน์โหลดแอป ผู้เล่นสามารถเข้าเล่นผ่าน เว็บเบราว์เซอร์ ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
มีรอบโบนัสให้ลุ้นบ่อย
Multiplier
เดโม่ฟรี
รองรับภาษาไทยเต็มรูปแบบ
ระบบฝากถอนสะดวก ทันใจ
แพลตฟอร์ม pg slot ส่วนใหญ่รองรับ การฝาก-ถอน อัตโนมัติ 24 ชั่วโมง ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ ระบบของผู้ให้บริการ การทำรายการใช้เวลา เพียงไม่กี่วินาที ผ่าน คิวอาร์โค้ด หรือระบบ Mobile Banking ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
หมวดเกมฮิต ใน pg slot
เกม PG Slot มีธีมหลากหลาย เช่น
ธีม เทพเจ้า
ธีม ลุยด่าน
ธีม โชคลาภ
ธีม Animal
ผู้เล่นนิยมเกมที่มีรอบพิเศษบ่อย พร้อมระบบ โบนัสรอบพิเศษ และ อัตราการจ่ายที่สูง เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นที่มีประสบการณ์
ความน่าเชื่อถือ
สล็อต PG พัฒนาในระบบสากล มีการ ปกป้องข้อมูลผู้เล่น และใช้ระบบสุ่มผล RNG เพื่อให้ผลลัพธ์ ตรวจสอบได้ แพลตฟอร์มที่ให้บริการ PG Slot ควรมี ความปลอดภัยสูง
สรุป
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ รวดเร็ว ผู้เล่นสามารถเริ่มต้นได้ ง่าย ฝากถอนสะดวก และเลือกเกมได้ หลากหลายแนว เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
https://medium.com/@ratypw/ทดลองเล่นสล็อต-pg-70cdb1132344
binance · March 8, 2026 at 11:00 pm
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Pixapostasesportivas · March 9, 2026 at 3:19 am
Jogo do Tigrinho estratégia de sessão: 300 giros e stop – funciona?
BradleyBit · March 9, 2026 at 1:12 pm
pg slot แพลตฟอร์มเกมสล็อตยอดนิยม เล่นง่าย ฝากถอนเร็ว
คำค้นหา สล็อต PG กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น ค่ายเกมที่มีชื่อเสียง ด้าน ภาพและเอฟเฟกต์ ความ เสถียร และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ออกแบบโดยทีมงานมืออาชีพ ที่รองรับการเล่นทั้งบน มือถือ และ เดสก์ท็อป
ข้อดี ของ pg slot
สล็อต PG เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ เปิดเกมได้ทันที เล่นผ่าน ระบบอัตโนมัติ และรองรับ ทั้ง iOS และ Android ไม่ต้องติดตั้งเพิ่มเติม ผู้เล่นสามารถเข้าเล่นผ่าน Browser ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม สล็อต PG ได้แก่
มีรอบโบนัสให้ลุ้นบ่อย
ระบบตัวคูณ
เดโม่ฟรี
รองรับภาษาไทยเต็มรูปแบบ
ระบบฝากถอนสะดวก ไม่ต้องรอนาน
แพลตฟอร์ม สล็อต PG โดยทั่วไปให้บริการ การฝาก-ถอน ออโต้ตลอด 24 ชม. ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ เงื่อนไขของเว็บไซต์ การทำรายการใช้เวลา เพียงไม่กี่วินาที ผ่าน คิวอาร์โค้ด หรือระบบ แอปธนาคาร ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
แนวเกมที่คนเล่นเยอะ ใน pg slot
เกม สล็อต PG มีธีมหลากหลาย เช่น
ธีม เทพเจ้าและแฟนตาซี
ธีม ผจญภัย
ธีม โชคลาภ
ธีม ธรรมชาติ
หลายคนชอบเกมที่โบนัสเข้าไว พร้อมระบบ โบนัสรอบพิเศษ และ อัตราการจ่ายที่สูง เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นมือโปร
ความน่าเชื่อถือ
PG Slot ใช้ระบบที่ได้มาตรฐาน มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล ระบบสุ่มมาตรฐาน เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ pg slot ควรมี ความปลอดภัยสูง
บทสรุปท้ายบท
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน กราฟิกคุณภาพ และการทำธุรกรรมที่ ไว ผู้เล่นสามารถเริ่มต้นได้ ทันที ฝากถอนสะดวก และเลือกเกมได้ จำนวนมาก เหมาะสำหรับ ผู้เล่นทุกสไตล์ ในโลกของเกมสล็อตออนไลน์
Josephneupt · March 9, 2026 at 1:14 pm
ทดลองเล่นสล็อต pg ฟรี สล็อต PG เกมสล็อตออนไลน์ที่คนค้นหาเยอะ เข้าเล่นไว ฝากถอนออโต้
คำค้นหา สล็อต PG กำลังได้รับความนิยมอย่างต่อเนื่อง ในกลุ่มผู้เล่นเกมสล็อตออนไลน์ เพราะเป็น แบรนด์เกมที่โดดเด่น ด้าน กราฟิก ความ ลื่นไหล และ อัตราการจ่ายรางวัลที่น่าสนใจ เกมของ PG ออกแบบโดยทีมงานมืออาชีพ ที่รองรับการเล่นทั้งบน โทรศัพท์มือถือ และ คอมพิวเตอร์
จุดเด่น ของ pg slot
PG Slot เป็นเกมสล็อตออนไลน์ที่ออกแบบมาให้ โหลดเร็ว เล่นผ่าน ระบบออนไลน์ และรองรับ ทุกแพลตฟอร์ม เข้าเล่นผ่านเว็บได้เลย ผู้เล่นสามารถเข้าเล่นผ่าน Browser ได้ทันที ภาพและเสียงถูกพัฒนาในรูปแบบ สามมิติ ให้ความคมชัด พร้อมเอฟเฟกต์ สวยงาม
คุณสมบัติหลักของเกม pg slot ได้แก่
โบนัสและฟรีสปินหลายแบบ
ฟีเจอร์ตัวคูณรางวัล
โหมดทดลองเล่นฟรี
รองรับภาษาไทยเต็มรูปแบบ
ฝากถอนง่าย ทำรายการไว
แพลตฟอร์ม สล็อต PG มักมี การฝาก-ถอน ออโต้ตลอด 24 ชม. ขั้นต่ำเริ่มต้นเพียง หลักหน่วย ขึ้นอยู่กับ กติกาแต่ละแพลตฟอร์ม การทำรายการใช้เวลา รวดเร็วมาก ผ่าน คิวอาร์โค้ด หรือระบบ ธนาคารบนมือถือ ทำให้ธุรกรรมเป็นไปอย่าง ลื่นไหล
แนวเกมที่คนเล่นเยอะ ใน pg slot
เกม pg slot มีธีมหลากหลาย เช่น
ธีม แฟนตาซี
ธีม ผจญภัย
ธีม โชคลาภ
ธีม Animal
เกมยอดนิยมมักเป็นเกมที่แตกง่าย พร้อมระบบ Special Feature และ อัตราการจ่ายที่สูง เหมาะกับทั้ง ผู้เล่นเริ่มต้น และ ผู้เล่นมือโปร
ความปลอดภัย
PG Slot มีมาตรฐานรองรับ มีการ รักษาความปลอดภัย และใช้ระบบสุ่มผล RNG เพื่อให้ผลลัพธ์ โปร่งใส แพลตฟอร์มที่ให้บริการ pg slot ควรมี ระบบดูแลข้อมูล
สรุป
สล็อต PG เป็นตัวเลือกยอดนิยมสำหรับผู้ที่ต้องการเล่นสล็อตออนไลน์ ด้วยจุดเด่นด้าน โบนัสหลากหลาย และการทำธุรกรรมที่ ทันใจ ผู้เล่นสามารถเริ่มต้นได้ ไม่ซับซ้อน ฝากถอนสะดวก และเลือกเกมได้ ครบทุกหมวด เหมาะสำหรับ ทุกระดับประสบการณ์ ในโลกของเกมสล็อตออนไลน์
gbgbet · March 9, 2026 at 11:20 pm
Undeniably believe that which you said. Your favorite justification seemed to be on the internet the simplest thing to be aware of. I say to you, I certainly get annoyed while people think about worries that they plainly do not know about. You managed to hit the nail upon the top and defined out the whole thing without having side-effects , people can take a signal. Will probably be back to get more. Thanks
https://www.snoopygarden.com/ · March 10, 2026 at 7:44 am
References:
Casino online sicuri
References:
https://www.snoopygarden.com/sn_event/?bmode=view&idx=162746114
http://healthysociety.kr/ · March 10, 2026 at 9:56 am
References:
Cherokee casino west siloam
References:
http://healthysociety.kr/24/?bmode=view&idx=4618149
www.toycarland.com · March 10, 2026 at 11:22 am
References:
Hollywood casino joliet
References:
http://www.toycarland.com/blog.php?aidx=122259
rufus download · March 10, 2026 at 11:57 am
rufus Rufus is known as a small, no-cost, open-source utility built to create bootable USB drives. It allows you to prepare a USB flash drive that can set up an operating system, run diagnostic tools, or boot into a recovery environment. The program does not require installation and can be launched as soon as it is downloaded.
The main function of Rufus is to create bootable USB media from ISO images quickly and reliably. This allows users to install or run operating systems directly from a USB flash drive without the need for DVDs. The tool supports a broad selection of operating systems and service utilities, which makes the program useful for both regular users and system administrators.
Rufus runs on computers with Microsoft Windows, starting from Windows 7. Both 32-bit and 64-bit versions are supported, and there is also a version available for ARM64 architecture.
The software lets users create bootable USB drives from many different ISO images. It can be used to prepare a USB drive for installing Windows 11, Windows 10, Windows 8.1, or Windows 7, as well as various Linux distributions. Rufus also works with DOS systems and other recovery or maintenance tools commonly used for troubleshooting computers.
One of the included features of Rufus is the ability to download official Windows ISO images directly from Microsoft servers. This allows users to obtain original installation images for Windows 8.1, Windows 10, and Windows 11 without searching for them on third-party websites.
In addition to creating bootable drives, Rufus can format USB devices. It supports several file systems including FAT32, NTFS, exFAT, UDF, and ReFS. This flexibility allows the USB drive to be prepared for different use cases and compatibility requirements.
Rufus supports both legacy BIOS systems and modern UEFI environments. Because of this, bootable drives created with Rufus can work on older computers as well as newer systems that use UEFI and Secure Boot.
Another feature included in Rufus is Windows To Go support. This option allows users to run a full Windows environment directly from a USB drive. It can be useful for testing systems, performing maintenance, or working on multiple computers without installing Windows on the internal drive.
Rufus also provides the option to bypass certain Windows 11 installation requirements. When creating an installation USB, the program can disable checks for TPM 2.0, Secure Boot, and minimum RAM requirements. This makes it possible to install Windows 11 on computers that would otherwise not meet the official hardware requirements.
One of the reasons Rufus has become popular is its speed and simplicity. The program is extremely small, about 1.9 MB in size, and runs as a portable application without installation. It is distributed under the GPL v3 open-source license, supports more than 70 languages, and contains no advertisements, bundled software, or tracking components.
Rufus works with a large number of ISO images. These include multiple versions of Windows, Windows Server editions, FreeDOS, and various system tools such as GParted, Hiren’s Boot CD, Parted Magic, and Clonezilla. Because of this wide compatibility, the program can be used not only for installing operating systems but also for disk management, data recovery, and system maintenance tasks.
To use Rufus, a computer running Windows 7 or later and a USB flash drive are required. The program does not need to be installed. Users simply download the executable file, run it, select the ISO image they want to use, and create a bootable USB drive. Due to its simplicity, speed, and reliability, Rufus remains one of the most widely used tools for creating bootable USB drives.
melbet казино · March 10, 2026 at 12:13 pm
melbet bonus code
Скачать Melbet: APK, iPhone и компьютер
Приложение Melbet объединяет ставки и казино в едином приложении. Пользователю доступны live-ставки, слоты, прямые трансляции, статистика и быстрые финансовые операции. Загрузка занимает несколько минут.
Android (APK)
Загрузите APK с официального сайта, откройте файл и завершите установку. При необходимости включите доступ к установке сторонних приложений, затем авторизуйтесь.
iOS (iPhone)
Откройте App Store, введите в поиске «Melbet», выберите «Получить», после установки авторизуйтесь в системе.
ПК
Откройте официальный сайт, авторизуйтесь и создайте ярлык на рабочий стол. Веб-версия работает как отдельное приложение.
Функционал
Live-ставки с мгновенным обновлением линии, казино и слоты, прямые трансляции, аналитические данные, push-оповещения, быстрая регистрация и круглосуточная служба поддержки.
Бонусы
После загрузки доступны приветственный бонус, акционные коды и фрибеты. Правила начисления определяются регионом.
Безопасность
Скачивайте только с официальных источников, проверяйте домен, не сообщайте данные доступа третьим лицам и активируйте двухфакторную аутентификацию.
Установка занимает несколько минут, после чего доступен весь функционал Melbet.
melbet на айфон · March 10, 2026 at 12:15 pm
скачать мелбет казино на андроид
Скачать Melbet: APK, iPhone и ПК
Мобильная версия Melbet объединяет ставки и казино в одном интерфейсе. Доступны live-ставки, казино-игры, прямые трансляции, аналитика и операции по счёту. Установка занимает несколько минут.
Android (APK)
Скачайте APK с официального источника, запустите установщик и подтвердите установку. При необходимости включите разрешение на установку из неизвестных источников, затем авторизуйтесь.
iOS (iPhone)
Перейдите в App Store, найдите «Melbet», выберите «Получить», после установки выполните вход.
ПК
Перейдите официальный сайт, войдите в личный кабинет и добавьте ярлык на рабочий стол. Веб-версия работает как полноценное приложение.
Функционал
Live-ставки с мгновенным обновлением линии, казино и слоты, просмотр матчей, подробная статистика, уведомления о матчах, регистрация за минуту и круглосуточная служба поддержки.
Бонусы
После установки доступны бонус на первый депозит, акционные коды и фрибеты. Правила начисления определяются регионом.
Безопасность
Загружайте только с официальных источников, контролируйте адрес сайта, не сообщайте данные доступа третьим лицам и включите 2FA.
Установка занимает несколько минут, после чего открывается полный доступ Melbet.
neetpeople.kr · March 10, 2026 at 12:16 pm
References:
Hollywood casino mississippi
References:
https://neetpeople.kr/event/?bmode=view&idx=8781989
xn88 · March 11, 2026 at 6:24 am
Một trong những yếu tố quan trọng mà người chơi quan tâm khi tham gia cá cược trực tuyến chính là độ an toàn bảo mật. xn88 Tại đây, nhà cái luôn cam kết đảm bảo quyền riêng tư và an ninh tuyệt đối cho tất cả người dùng. TONY03-11O
phcash · March 12, 2026 at 9:05 am
I am in fact happy to read this web site posts which contains lots of helpful facts, thanks for providing these kinds of statistics.
скачать бк мелбет на айфон · March 12, 2026 at 4:37 pm
скачать мелбет на телефон
Скачать Melbet: APK, iOS и ПК
Приложение Melbet включает ставки и казино в одном интерфейсе. Пользователю доступны live-ставки, слоты, прямые трансляции, статистика и операции по счёту. Установка занимает 1–2 минуты.
Android (APK)
Загрузите APK с официального источника, запустите установщик и подтвердите установку. Если требуется включите доступ к установке сторонних приложений, затем авторизуйтесь.
iOS (iPhone)
Перейдите в App Store, введите в поиске «Melbet», выберите «Получить», после установки авторизуйтесь в системе.
ПК
Перейдите официальный сайт, войдите в личный кабинет и добавьте ярлык на рабочий стол. Браузерная версия функционирует как отдельное приложение.
Функционал
Live-ставки с мгновенным обновлением линии, игровой раздел с тысячами игр, прямые трансляции, аналитические данные, уведомления о матчах, быстрая регистрация и поддержка 24/7.
Бонусы
После загрузки доступны бонус на первый депозит, акционные коды и фрибеты. Условия зависят от региона.
Безопасность
Загружайте только с официальных источников, контролируйте адрес сайта, не сообщайте данные доступа третьим лицам и включите 2FA.
Установка занимает несколько минут, после чего доступен весь функционал Melbet.
nerve calm · March 12, 2026 at 10:54 pm
**nerve calm**
NerveCalm is a high-quality nutritional supplement crafted to promote nerve wellness, ease chronic discomfort, and boost everyday vitality.
allwin · March 13, 2026 at 7:35 am
I always used to study article in news papers but now as I am a user of internet therefore from now I am using net for content, thanks to web.
okebet · March 13, 2026 at 9:41 am
Since the admin of this web site is working, no hesitation very rapidly it will be famous, due to its quality contents.
Garrygig · March 13, 2026 at 10:27 pm
вулкан вегас зеркало
https://t.me/s/realvulcanvegas
Robertnex · March 14, 2026 at 11:14 am
Автозайм
Займ под залог ПТС в Самаре — представляет собой возможность взять средства под машину без необходимости продавать машины и без долгих банковских процедур. Основная характеристика такого займа — транспорт остаётся у владельца у собственника, а в залог передаётся только ПТС. Это позволяет использовать автомобилем, пока действует договор займа.
Выдача денег происходит в день обращения. Заявка рассматривается около 15 мин, после чего выносится ответ по сумме займа и условиям оформления. Сумма финансирования может составлять до уровня 5 000 000 ?, а процентная ставка начинается с уровня 2% в месяц. Период кредитования обычно составляет до 60 мес., по этой причине клиент выбирает удобный план платежей.
Система оформления заявки доступна через интернет. Клиент оставляет форму, вносит информацию об авто и желаемую сумму. После проверки документов приходит предварительное решение. Чаще всего средства выдаются в день оформления, когда оформляется договор займа.
Для расчёта параметров применяется калькулятор займа. К примеру, при сумме 300 000 ? на период 12 месяцев платёж в месяц составит примерно 33 057 ?. Итоговая сумма переплаты по такому займу составит примерно 96 684 ?. Конечные параметры могут изменяться в зависимости стоимости автомобиля и установленного срока займа.
На сайтах автозаймов нередко показывается онлайн-лента заявок. Этот блок демонстрирует активность системы и примеры обработанных заявок из разных городов. Например, заявки на суммы 1 840 000 ? из Тулы, 1 890 000 ? город Москва или 1 470 000 ? город Челябинск получают статус «Одобрено». Некоторые обращений находятся в стадии проверки — например такие суммы, 290 000 ? город Сочи или 720 000 ? из Екатеринбурга. Подобные разделы отображают текущую активность платформы и число заявок сегодня и в текущем месяце.
Автозайм под залог ПТС подходит тем, кому требуется оперативно получить значительную сумму без продажи автомобиля. Основные параметры таких займов — ставка начиная от 2% в месяц, одобрение около 15 минут, размер займа до 5 000 000 ? и возможность оформить заявку через интернет. После отправки формы клиент может дождаться решения, связаться через мессенджер или связаться с менеджером для уточнения деталей оформления.
https://samara.carzaem.ru/
top646 · March 14, 2026 at 7:30 pm
Link exchange is nothing else except it is simply placing the other person’s webpage link on your page at proper place and other person will also do similar in support of you.
80wim · March 14, 2026 at 8:22 pm
Alright, giving 80wim a whirl. Interface is pretty clean and easy to use. Nothing too flashy, but it gets the job done. They seem to have alright odds. Give it a look: 80wim.
81betcc · March 14, 2026 at 8:22 pm
Thinking about trying 81betcc. I saw some decent reviews. Gotta see what the fuss is about. Might give it a go and drop some dough there. check them out by yourself: 81betcc.
868vip1 · March 14, 2026 at 8:23 pm
Yo, checking out 868vip1. The site looks legit, and they have a decent selection of games. I haven’t won big yet, but I also haven’t been burned. Worth a look if you’re seeking a new place to try your luck: 868vip1.
Robertnex · March 17, 2026 at 12:02 am
https://hype4free.com/index.php?page=user&action=pub_profile&id=14332&item_type=active&per_page=16
davidson-watkins-3.technetbloggers.de · March 17, 2026 at 3:28 pm
yakama legends casino
https://pad.stuve.uni-ulm.de/s/C5y61AMseZ pad.stuve.uni-ulm.de
https://case.edu/cgi-bin/newsline.pl?URL=https://tvoyaskala.com/user/desireguitar3/ https://case.edu/cgi-bin/newsline.pl?URL=https://tvoyaskala.com/user/desireguitar3/
https://raindrop.io/liquidmap3/chobrandt0009-68527557 https://raindrop.io/liquidmap3/chobrandt0009-68527557
https://sisterinch8.werite.net/big4-gold-coast-caravan-park-book-direct-and-save-with-big4 https://sisterinch8.werite.net
https://postheaven.net/bitesleep0/tips-and-strategies-for-betting-on-virtual-sports-winner-odds postheaven.net
https://isowindows.net/user/mindtest4/ https://isowindows.net/user/mindtest4/
https://to-portal.com/beetsleep3 to-portal.com
https://www.bidbarg.com/legal/user/playsoil6 https://www.bidbarg.com/
https://matkafasi.com/user/peanutcanada6 matkafasi.com
https://rentry.co/b9m76x2m https://rentry.co/b9m76x2m
http://qa.doujiju.com/index.php?qa=user&qa_1=sisterstew4 qa.doujiju.com
https://doc.adminforge.de/s/ZPfSHsC6Oe doc.adminforge.de
https://classifieds.ocala-news.com/author/mindcanada9 classifieds.ocala-news.com
https://hackmd.okfn.de/s/B1bxNLUcWe hackmd.okfn.de
https://hackmd.okfn.de/s/rJ_MZbIcZl hackmd.okfn.de
https://notes.bmcs.one/s/JPpX4zP0M https://notes.bmcs.one/s/JPpX4zP0M
https://baker-padilla.mdwrite.net/hotels-with-free-wi-fi-in-new-york baker-padilla.mdwrite.net
https://doc.adminforge.de/s/6dMjqZgFre https://doc.adminforge.de
References:
https://bookcycle5.werite.net/grayscale-launches-avalanche-staking-etf-for-avax-exposure
meier-meyer-3.federatedjournals.com · March 17, 2026 at 4:14 pm
References:
Emerald queen casino tacoma
References:
https://500px.com/p/keatingxqpchristie
казино х регистрация · March 17, 2026 at 4:41 pm
casino x полная версия
techou.jp · March 17, 2026 at 4:46 pm
References:
Orleans casino
References:
https://justbookmark.win/story.php?title=why-casino-operators-are-switching-to-third-party-software-distributors
urlscan.io · March 17, 2026 at 4:55 pm
gaming casino
https://peatix.com/user/29179090 https://peatix.com
https://diego-maradona.org/user/selfsnail1/ https://diego-maradona.org/user/selfsnail1
https://platform.joinus4health.eu/forums/users/tiestew4/ platform.joinus4health.eu
https://actualites.cava.tn/user/peanutlayer3/ actualites.cava.tn
https://www.demilked.com/author/tulipboat9/ http://www.demilked.com
https://ccsakura.jp:443/index.php?eventmap3 https://ccsakura.jp/
https://www.folkd.com/submit/schoolido.lu/user/lisaguitar1// https://www.folkd.com/submit/schoolido.lu/user/lisaguitar1
https://audiobook.net.pl/user/mindlocust6/ https://audiobook.net.pl/user/mindlocust6
https://ryu-ga-index.com:443/index.php?huynhpark919528 ryu-ga-index.com
https://squareblogs.net/conefaucet2/client-challenge squareblogs.net
http://ezproxy.cityu.edu.hk/login?url=https://www.udrpsearch.com/user/unitaugust2 http://ezproxy.cityu.edu.hk/
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1890740 gaiaathome.eu
https://bookmarkzones.trade/story.php?title=online-gambling-experience-with-real-rewards https://bookmarkzones.trade/story.php?title=online-gambling-experience-with-real-rewards
https://p.mobile9.com/goalsoil2/ p.mobile9.com
https://www.adpost4u.com/user/profile/4358349 http://www.adpost4u.com
https://raun-cardenas.mdwrite.net/craps-payout-chart-and-odds-guide-learn-to-calculate-your-winnings https://raun-cardenas.mdwrite.net
https://www.udrpsearch.com/user/blocklayer7 udrpsearch.com
https://urlscan.io/result/019cfb57-d5fc-735e-ad95-ed7f9f47fffa/ https://urlscan.io/result/019cfa34-51a1-7425-9c97-5e8f48981b36/
linkvault.win · March 17, 2026 at 5:07 pm
casino charlevoix
https://firsturl.de/xd55NU6 firsturl.de
https://tvoyaskala.com/user/conesteel3/ tvoyaskala.com
https://poole-lindegaard.technetbloggers.de/king-johnnie-casino-premium-online-gaming-australia-2026 poole-lindegaard.technetbloggers.de
https://pads.jeito.nl/s/jQi5bK1xi_ pads.jeito.nl
https://fravito.fr/user/profile/2215233 fravito.fr
https://gratisafhalen.be/author/beetcomic0/ gratisafhalen.be
https://numberfields.asu.edu/NumberFields/show_user.php?userid=6581808 numberfields.asu.edu
https://www.investagrams.com/Profile/sharpe3697079 http://www.investagrams.com
https://www.garagesale.es/author/stepbridge6/ https://www.garagesale.es/author/stepbridge6/
https://sundaynews.info/user/selfsushi1/ https://sundaynews.info/user/selfsushi1/
https://diego-maradona.com.az/user/liquidtest3/ https://diego-maradona.com.az/user/liquidtest3
https://to-portal.com/pumaboat6 to-portal.com
https://baby-newlife.ru/user/profile/500511 baby-newlife.ru
https://ccsakura.jp:443/index.php?sheepbun5 ccsakura.jp
https://hackmd.okfn.de/s/rJSlKbLqZg https://hackmd.okfn.de
https://saveyoursite.date/story.php?title=top-blackjack-strategy-for-2026-how-to-play-tips-to-win saveyoursite.date
https://mapleprimes.com/users/pumasteel8 https://mapleprimes.com/users/pumasteel8
https://graph.org/Real-Money-Wins-Online-Guaranteed-03-17 graph.org
References:
https://writeablog.net/selfash0/download-the-apk-from-uptodown
вулкан вегас официальный · March 17, 2026 at 5:29 pm
вулкан вегас зеркало
https://travelersqa.com · March 17, 2026 at 5:33 pm
gowild casino
https://test.najaed.com/user/eventboard9 test.najaed.com
https://pad.stuve.de/s/BM035ZFE4 pad.stuve.de
https://500px.com/p/baybtxfield https://500px.com/p/baybtxfield
https://www.bandsworksconcerts.info:443/index.php?playinch2 http://www.bandsworksconcerts.info
https://coolpot.stream/story.php?title=best-online-casino-payouts-australia-2026-top-sites-2026 https://coolpot.stream/story.php?title=best-online-casino-payouts-australia-2026-top-sites-2026
https://pad.stuve.uni-ulm.de/s/o_lNbDkeh pad.stuve.uni-ulm.de
https://notes.medien.rwth-aachen.de/-yhz8hdaTai46rFGQH3ILw/ https://notes.medien.rwth-aachen.de/-yhz8hdaTai46rFGQH3ILw/
https://trade-britanica.trade/wiki/Casinos_dont_have_a_get_out_of_jail_card_It_is_a_never_go_in_the_first_place https://trade-britanica.trade/wiki/Casinos_dont_have_a_get_out_of_jail_card_It_is_a_never_go_in_the_first_place
https://may22.ru/user/mindsleep3/ may22.ru
https://pad.geolab.space/s/Uk70zQsH9 pad.geolab.space
https://md.un-hack-bar.de/s/ZTSbTv6udH md.un-hack-bar.de
https://500px.com/p/hougaardkxdcarpenter 500px.com
https://poole-leon-3.technetbloggers.de/fast-payout-online-casino-australia-2026-top-5-instant-withdrawal-casino-sites-reviewed-1773742357 https://poole-leon-3.technetbloggers.de
https://ccsakura.jp:443/index.php?sheepmap8 ccsakura.jp
https://isowindows.net/user/sisterfaucet6/ isowindows.net
https://hedgedoc.info.uqam.ca/s/dx0ZlsQmW hedgedoc.info.uqam.ca
http://ask.mallaky.com/?qa=user/scarfsushi7 http://ask.mallaky.com/?qa=user/scarfsushi7
https://dreevoo.com/profile.php?pid=1324461 dreevoo.com
References:
https://peatix.com/user/29184579
hack.allmende.io · March 17, 2026 at 6:01 pm
rosemont casino
https://molchanovonews.ru/user/archperson0/ molchanovonews.ru
https://securityheaders.com/?q=https://www.folkd.com/submit/www.tikosatis.com/index.php?page=user&action=pub_profile&id=607270/ https://securityheaders.com/?q=https://www.folkd.com/submit/www.tikosatis.com/index.php?page=user&action=pub_profile&id=607270/
http://madk-auto.ru/user/sisterbone4/ madk-auto.ru
https://oiaedu.com/forums/users/mindcycle4/ oiaedu.com
https://platform.joinus4health.eu/forums/users/steporgan4/ platform.joinus4health.eu
https://prpack.ru/user/stepash8/ prpack.ru
https://to-portal.com/pumaboat6 https://to-portal.com/pumaboat6
https://bookmarkzones.trade/story.php?title=top-online-casino-ireland-best-of-2026-reviews-read-customer-service-reviews-of-irelandonline-casino https://bookmarkzones.trade/
https://fravito.fr/user/profile/2215114 fravito.fr
https://www.blurb.com/user/sheepperson0 http://www.blurb.com
https://is.gd/W2NYcU is.gd
https://a-taxi.com.ua/user/nicinch3/ a-taxi.com.ua
https://gratisafhalen.be/author/pilotash2/ gratisafhalen.be
https://is.gd/HfzhJE is.gd
https://justbookmark.win/story.php?title=gambling-laws-and-regulations-report-2026-finland https://justbookmark.win/
http://ask.mallaky.com/?qa=user/bitelayer7 ask.mallaky.com
https://ccsakura.jp:443/index.php?pilotorgan1 ccsakura.jp
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://officecold7.bravejournal.net/australian-online-gambling-trends-2025-outlook-for-au bbs.pku.edu.cn
References:
https://nhadat24.org/author/clausstew1
bookmark4you.win · March 17, 2026 at 7:33 pm
holland casino vacatures
https://pads.zapf.in/s/PdfcnFeaRL pads.zapf.in
https://www.garagesale.es/author/latheselect5/ https://www.garagesale.es/author/latheselect5
https://www.credly.com/users/steplayer4 http://www.credly.com
https://www.marocbikhir.com/user/profile/614023 http://www.marocbikhir.com
https://prpack.ru/user/beettest5/ prpack.ru
https://bundgaard-serup-2.technetbloggers.de/best-betting-sites-in-the-uk-2026-tested-ranked-and-expert-reviewed bundgaard-serup-2.technetbloggers.de
https://raindrop.io/archsnail8/coxboisen2756-68541275 raindrop.io
https://raindrop.io/tieselect8/karlssonalbrektsen5001-68541817 raindrop.io
https://squareblogs.net/selfboard4/top-10-online-roulette-casinos-2026-real-money-games squareblogs.net
https://www.blurb.com/user/bitestew2 http://www.blurb.com
https://classifieds.ocala-news.com/author/beettest7 classifieds.ocala-news.com
https://a-taxi.com.ua/user/tiecycle1/ https://a-taxi.com.ua
https://forum.issabel.org/u/beetcanada7 forum.issabel.org
https://xypid.win/story.php?title=luxury-hotel-in-las-vegas https://xypid.win/story.php?title=luxury-hotel-in-las-vegas
https://www.garagesale.es/author/bitekite6/ http://www.garagesale.es
https://citytoads.com/user/profile/77822 citytoads.com
https://notes.bmcs.one/s/R65J5qI4J notes.bmcs.one
https://matkafasi.com/user/latheboard4 matkafasi.com
References:
https://poole-boesen-2.blogbright.net/best-casino-payment-methods-in-canada-2026
https://test.najaed.com/user/cousinash3 · March 17, 2026 at 7:42 pm
References:
Lumiere casino
References:
https://pad.karuka.tech/s/cVPBAnB-s
https://writeablog.net/goalbone1/best-instant-withdrawal-crypto-casinos-and-fastest-payouts · March 17, 2026 at 10:09 pm
treasure island casino minnesota
https://www.tvbattle.com/index.php?page=user&action=pub_profile&id=277163 https://www.tvbattle.com/index.php?page=user&action=pub_profile&id=277163
https://a-taxi.com.ua/user/yokepastry0/ https://a-taxi.com.ua/user/yokepastry0
http://gojourney.xsrv.jp/index.php?selfleo6 gojourney.xsrv.jp
https://itkvariat.com/user/peanutsushi9/ https://itkvariat.com/
https://bandori.party/user/626654/tiebone2/ bandori.party
https://www.marocbikhir.com/user/profile/613454 http://www.marocbikhir.com
https://lykkegaard-adair-3.blogbright.net/crypto-casino-deposit-methods-explained-best-coins-wallets-and-how-to-withdraw-anonymously-2026 lykkegaard-adair-3.blogbright.net
https://www.tvbattle.com/index.php?page=user&action=pub_profile&id=276613 https://www.tvbattle.com/index.php?page=user&action=pub_profile&id=276613
https://fkwiki.win/wiki/Post:Top_15_Instant_Withdrawal_Crypto_Casinos_of_2025_Fastest_Payout_Casinos fkwiki.win
https://travelersqa.com/user/pumasushi1 travelersqa.com
https://blogfreely.net/cousincomic7/king-johnnie-casino-games-collection-2026-get-ready-to-win https://blogfreely.net/cousincomic7/king-johnnie-casino-games-collection-2026-get-ready-to-win
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://pad.geolab.space/s/fKLceTkt5 bbs.pku.edu.cn
https://www.question2answer.org/qa/user/sisterleo9 http://www.question2answer.org
https://ondashboard.win/story.php?title=what-are-the-limits-for-online-blackjack ondashboard.win
https://numberfields.asu.edu/NumberFields/show_user.php?userid=6582221 numberfields.asu.edu
https://bookmarkfeeds.stream/story.php?title=aussie-play-bonuses-different-bonus-and-promo-combinations-9 https://bookmarkfeeds.stream/
https://diego-maradona-ar.org/user/bookperson8/ https://diego-maradona-ar.org/
https://test.najaed.com/user/stepsleep5 test.najaed.com
References:
http://uvs2.net/index.php/user/bookleo0
https://sub.elfejewelry.com · March 17, 2026 at 10:14 pm
amsterdam casino
https://www.demilked.com/author/yokecanada8/ http://www.demilked.com
https://dreevoo.com/profile.php?pid=1323154 https://dreevoo.com/
https://notes.io/ecqYp notes.io
https://www.divephotoguide.com/user/selfboat4 http://www.divephotoguide.com
https://able2know.org/user/coneboard6/ able2know.org
https://www.udrpsearch.com/user/tuliptest8 http://www.udrpsearch.com
https://analnoe.com/user/nicinch8/ analnoe.com
https://saveyoursite.date/story.php?title=oscars-2026-the-complete-list-of-winners-losers saveyoursite.date
https://wikimapia.org/external_link?url=https://codimd.communecter.org/kV6TRPFSRVmCNQ7nqG8rFw/ wikimapia.org
https://drejer-boswell-2.mdwrite.net/play-21-700-free-online-casino-games-no-download drejer-boswell-2.mdwrite.net
http://dudoser.com/user/bookbone8/ dudoser.com
https://hedgedoc.eclair.ec-lyon.fr/s/pw2782x2o hedgedoc.eclair.ec-lyon.fr
https://gaiaathome.eu/gaiaathome/show_user.php?userid=1890557 https://gaiaathome.eu/
https://bandori.party/user/628155/peanuttest5/ https://bandori.party
https://numberfields.asu.edu/NumberFields/show_user.php?userid=6582737 https://numberfields.asu.edu/
https://md.swk-web.com/s/savE2SaE6 md.swk-web.com
https://hackmd.okfn.de/s/S1T7auL9be https://hackmd.okfn.de
https://pad.geolab.space/s/lRMy5-aqB https://pad.geolab.space
References:
https://skitterphoto.com/photographers/2476766/truelsen-adair
https://invastu.kz · March 17, 2026 at 10:30 pm
atlantis casino
https://codimd.communecter.org/LnZlcfo8TLmpEeDrgdoe0g/ https://codimd.communecter.org/
https://invastu.kz/user/coneorgan6//user/pilottest0/ invastu.kz
https://md.swk-web.com/s/VLM1Hvr0B md.swk-web.com
https://drejer-mcgarry.thoughtlanes.net/where-to-find-the-glitziest-casinos-in-north-america https://drejer-mcgarry.thoughtlanes.net/where-to-find-the-glitziest-casinos-in-north-america
https://notes.io/eceZd https://notes.io/eceZd
https://ccsakura.jp:443/index.php?bitestew7 https://ccsakura.jp:443/index.php?bitestew7
https://numberfields.asu.edu/NumberFields/show_user.php?userid=6582737 numberfields.asu.edu
https://hedgedoc.eclair.ec-lyon.fr/s/CWCxY-AIY hedgedoc.eclair.ec-lyon.fr
https://may22.ru/user/archinch2/ https://may22.ru/
http://uchkombinat.com.ua/user/tulipinch6/ http://uchkombinat.com.ua/user/tulipinch6
https://gpsites.win/story.php?title=information-about-oshi-casino https://gpsites.win/story.php?title=information-about-oshi-casino
https://www.divephotoguide.com/user/selfboat4 http://www.divephotoguide.com
https://pad.geolab.space/s/SDBlWsnMO https://pad.geolab.space
https://servodriven.com/forums/users/crabperson0/ servodriven.com
https://pads.jeito.nl/s/5QU0AOIlaI pads.jeito.nl
https://invastu.kz/user/liquidcycle3/ invastu.kz
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://onlinevetjobs.com/author/pipegeese1/ https://bbs.pku.edu.cn/
https://raindrop.io/biteperson3/grossmanrush8799-68526156 https://raindrop.io/biteperson3/grossmanrush8799-68526156
atavi.com · March 17, 2026 at 10:39 pm
casino auto sales
https://invastu.kz/user/pilottest0/ invastu.kz
https://www.demilked.com/author/clausselect9/ https://www.demilked.com/
https://aryba.kg/user/booklayer0/ aryba.kg
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://lit-book.ru/user/peenlift6/ https://bbs.pku.edu.cn
https://dehn-adair-2.thoughtlanes.net/the-best-online-casino-in-australia-2025 dehn-adair-2.thoughtlanes.net
http://volleypedia.org/index.php?qa=user&qa_1=archbun7 http://volleypedia.org/
https://blogfreely.net/booksnail0/crypto-sports-betting-in-canada-top-web3-sportsbooks-for-live-markets https://blogfreely.net/
https://yatirimciyiz.net/user/sheeppurple6 yatirimciyiz.net
https://medibang.com/author/27978326/ medibang.com
https://zenwriting.net/tiesteel9/the-best-mobile-online-casinos-in-australia-for-2026 zenwriting.net
https://www.youtube.com/redirect?q=https://blender.community/melchiorsenjessen/ http://www.youtube.com
http://jobs.emiogp.com/author/steplayer0/ http://jobs.emiogp.com/
https://pad.geolab.space/s/SDBlWsnMO pad.geolab.space
https://www.udrpsearch.com/user/eventinch8 https://www.udrpsearch.com/
https://skitterphoto.com/photographers/2476766/truelsen-adair https://skitterphoto.com/photographers/2476766/truelsen-adair
https://poole-rojas-2.thoughtlanes.net/cricket-betting-tips https://poole-rojas-2.thoughtlanes.net/cricket-betting-tips
http://ezproxy.cityu.edu.hk/login?url=https://numberfields.asu.edu/NumberFields/show_user.php?userid=6580041 ezproxy.cityu.edu.hk
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://officecold7.bravejournal.net/australian-online-gambling-trends-2025-outlook-for-au https://bbs.pku.edu.cn/v2/jump-to.php?url=https://officecold7.bravejournal.net/australian-online-gambling-trends-2025-outlook-for-au
References:
https://keating-kruse-4.federatedjournals.com/the-pokies-australia-231-real-money-casino-with-human-support
www.giveawayoftheday.com · March 17, 2026 at 11:11 pm
game twist casino
https://md.chaosdorf.de/s/mo2R5F0RWt md.chaosdorf.de
https://rees-hyldgaard.federatedjournals.com/crypto-casino-licensing-guide-legal-blockchain-gambling rees-hyldgaard.federatedjournals.com
https://lit-book.ru/user/goalsleep0/ lit-book.ru
https://nhadat24.org/author/sisterorgan6 nhadat24.org
https://lykkegaard-adair-3.blogbright.net/crypto-casino-deposit-methods-explained-best-coins-wallets-and-how-to-withdraw-anonymously-2026 https://lykkegaard-adair-3.blogbright.net
https://invastu.kz/user/pumabun2/ https://invastu.kz/
https://www.credly.com/users/tiemap9 https://www.credly.com
https://www.udrpsearch.com/user/tuliptest8 https://www.udrpsearch.com/user/tuliptest8
https://schoolido.lu/user/liquidbridge7/ schoolido.lu
https://may22.ru/user/mindsleep3/ may22.ru
https://rentry.co/sfpqnai3 rentry.co
https://doc.adminforge.de/s/wF9GTstg9e https://doc.adminforge.de/s/wF9GTstg9e
https://https://www.giveawayoftheday.com/forums/profile/1724955/forums/profile/1724955 https://www.giveawayoftheday.com/
https://atavi.com/share/xqyg9xz1ushwy https://atavi.com/share/xqyg9xz1ushwy
http://ezproxy.cityu.edu.hk/login?url=https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=croplift8 ezproxy.cityu.edu.hk
https://pad.karuka.tech/s/T4PvFgUsX pad.karuka.tech
https://schneider-morales-3.hubstack.net/online-casino-customer-support-what-are-my-options schneider-morales-3.hubstack.net
http://dudoser.com/user/bookbone8/ dudoser.com
aryba.kg · March 17, 2026 at 11:19 pm
slot machine apk
https://vacuum24.ru/user/profile/559959 vacuum24.ru
https://hedgedoc.info.uqam.ca/s/FyW3m_VNo https://hedgedoc.info.uqam.ca/
https://a-taxi.com.ua/user/nicinch3/ a-taxi.com.ua
https://ryu-ga-index.com:443/index.php?beringbean926389 ryu-ga-index.com
https://to-portal.com/tulipcanada6 https://to-portal.com/tulipcanada6
https://lovebookmark.win/story.php?title=how-to-start-playing-at-golden-crown-casino-beginner-guide https://lovebookmark.win
https://www.24propertyinspain.com/user/profile/1402217 https://www.24propertyinspain.com/user/profile/1402217
https://baby-newlife.ru/user/profile/500488 https://baby-newlife.ru/user/profile/500488
https://medibang.com/author/27975852/ https://medibang.com/author/27975852
https://p.mobile9.com/lettersnail6/ p.mobile9.com
https://zenwriting.net/letterbone6/bellagio-rewards-guide-free-rooms-food-and-drink-las-vegas https://zenwriting.net/letterbone6/bellagio-rewards-guide-free-rooms-food-and-drink-las-vegas
https://truelsen-hyldgaard-2.mdwrite.net/las-vegas-casinos-offer-canada-friendly-money-savings https://truelsen-hyldgaard-2.mdwrite.net/las-vegas-casinos-offer-canada-friendly-money-savings
https://pad.geolab.space/s/_BbdpgCsB pad.geolab.space
https://graph.org/Best-Payout-Online-Casinos-in-Australia-2026-Highest-Payouts-03-17 https://graph.org/
https://prosmart.by/user/bookbone8/ https://prosmart.by/user/bookbone8
https://forum.issabel.org/u/letterperson8 forum.issabel.org
https://sub.elfejewelry.com:443/index.php?vaughangeisler228313 https://sub.elfejewelry.com
https://davidson-shore-2.blogbright.net/best-payid-casinos-in-australia-2026-real-money-payid-pokies https://davidson-shore-2.blogbright.net/best-payid-casinos-in-australia-2026-real-money-payid-pokies
References:
https://diego-maradona-ar.org/user/bookcomic5/
urlscan.io · March 18, 2026 at 1:24 am
References:
Isle of capri florida
References:
https://bandori.party/user/628537/yokesleep2/
www.youtube.com · March 18, 2026 at 2:46 am
online casino vegas
http://ask.mallaky.com/?qa=user/scarfsushi7 ask.mallaky.com
https://notes.bmcs.one/s/R65J5qI4J notes.bmcs.one
https://bundgaard-mahoney.hubstack.net/how-australians-became-the-worlds-biggest-gamblers-gambling https://bundgaard-mahoney.hubstack.net
https://blogfreely.net/claussnail3/bk9-casino-review-a-premier-online-casino-experience-for-australian-players blogfreely.net
https://yatirimciyiz.net/user/yokefaucet8 https://yatirimciyiz.net/
https://ccsakura.jp:443/index.php?sheepselect9 https://ccsakura.jp
https://bandori.party/user/629282/cousinbone2/ bandori.party
https://matkafasi.com/user/latheboard4 matkafasi.com
https://telegra.ph/Analytics-Insight-Latest-AI-Crypto-Tech-News–Analysis-03-17 https://telegra.ph/Analytics-Insight-Latest-AI-Crypto-Tech-News–Analysis-03-17
https://dehn-adair-2.thoughtlanes.net/the-best-online-casino-in-australia-2025 dehn-adair-2.thoughtlanes.net
https://doodleordie.com/profile/archleo3 doodleordie.com
https://cattletrailers.com.au/author/bitestew9/ https://cattletrailers.com.au
https://500px.com/p/levinkfzhovgaard 500px.com
https://prpack.ru/user/stepash8/ https://prpack.ru/user/stepash8
https://www.blurb.com/user/tuliplayer4 http://www.blurb.com
https://notes.bmcs.one/s/gE0inZ_rK https://notes.bmcs.one
https://graph.org/King-Billy-Casino-Sign-Up-Guide–Bonus-03-17 graph.org
https://forum.issabel.org/u/tiemap7 forum.issabel.org
References:
https://forum.issabel.org/u/beetcanada7
raindrop.io · March 18, 2026 at 8:25 am
seminole casino brighton
https://xypid.win/story.php?title=sign-up-now-5 https://xypid.win/
https://medibang.com/author/27977420/ medibang.com
https://www.demilked.com/author/tulipboard8/ http://www.demilked.com
https://hedgedoc.info.uqam.ca/s/NzDRP5OcD https://hedgedoc.info.uqam.ca/
https://pikidi.com/seller/profile/bookcycle6 https://pikidi.com/seller/profile/bookcycle6
https://bandori.party/user/626626/playboard1/ https://bandori.party/user/626626/playboard1/
https://postheaven.net/selfperson5/best-instant-payout-crypto-casinos-top-15-picks-for-2026 https://postheaven.net/selfperson5/best-instant-payout-crypto-casinos-top-15-picks-for-2026
https://www.bandsworksconcerts.info:443/index.php?playlayer9 https://www.bandsworksconcerts.info:443/index.php?playlayer9
https://ecuadorenventa.net/author/goalorgan2/ https://ecuadorenventa.net/
https://yatirimciyiz.net/user/pilottest3 yatirimciyiz.net
https://www.udrpsearch.com/user/liquidpurple5 https://www.udrpsearch.com
https://www.investagrams.com/Profile/lykkeg3697767 https://www.investagrams.com
https://pad.geolab.space/s/I9AiClvXI pad.geolab.space
https://md.swk-web.com/s/2m6QsJU73 md.swk-web.com
https://bandori.party/user/629282/cousinbone2/ bandori.party
https://case.edu/cgi-bin/newsline.pl?URL=https://oiaedu.com/forums/users/desirehot2/ case.edu
https://g.clicgo.ru/user/liquidcycle5/ g.clicgo.ru
http://ezproxy.cityu.edu.hk/login?url=https://gaiaathome.eu/gaiaathome/show_user.php?userid=1888509 ezproxy.cityu.edu.hk
References:
https://ccsakura.jp:443/index.php?booksnail0
раменбет скачать · March 19, 2026 at 6:38 pm
раменбет играть онлайн
git.limework.net · March 20, 2026 at 5:09 pm
best anabolic supplement for mass
https://git.clickforadventure.co/scarlett943917 git.clickforadventure.co
http://139.59.100.212:3001/marlene58e6042 139.59.100.212
https://git.ultra.pub/juniorcalderon git.ultra.pub
http://www.shqkxh.org:3000/shaynaglynde33 http://www.shqkxh.org:3000/shaynaglynde33
http://62.173.140.174:10480/margaritoprimr http://62.173.140.174
http://pasarinko.zeroweb.kr/bbs/board.php?bo_table=notice&wr_id=9511965 http://pasarinko.zeroweb.kr/
https://www.herzog-it.de/isabellemackin http://www.herzog-it.de
http://120.26.116.243:3000/alenanina70838 120.26.116.243
https://gitea.kdlsvps.top/simaomq3718094 gitea.kdlsvps.top
http://192.238.205.92:3000/romainesmither 192.238.205.92
https://gitoria.ru/michalewiggins gitoria.ru
http://62.234.222.247:3000/elishazerangue 62.234.222.247
http://38.76.202.113:3000/jimmiesalting http://38.76.202.113:3000/jimmiesalting
http://180.163.77.12:3000/mairap41547834 180.163.77.12
https://txuki.duckdns.org/rickygreenwald txuki.duckdns.org
http://61.178.84.89:8998/louiegallant80 http://61.178.84.89:8998/louiegallant80
https://unpourcent.online/@carlota4075913 https://unpourcent.online/@carlota4075913
http://116.236.50.103:8789/kerryjarnigan8 116.236.50.103
References:
http://gang-yeon.com/bbs/board.php?bo_table=faq&wr_id=475719
http://182.92.251.55/ · March 20, 2026 at 5:40 pm
bodybuilding supplements that work like steroids
http://8.134.11.35:3000/buerosetta5784 8.134.11.35
http://124.221.208.175:53000/haigilroy11938 124.221.208.175
http://8.134.11.35:3000/buerosetta5784 8.134.11.35
http://124.221.208.175:53000/vidabowie81836 http://124.221.208.175
https://code.dsconce.space/tomokoarias401 https://code.dsconce.space
https://git.auth.com.br/lesliestoll03 git.auth.com.br
http://39.171.252.63:3000/roslyncota8550 39.171.252.63
http://221.226.114.142:13000/mohammaddrigge http://221.226.114.142/
https://wazifafood.com/employer/anadrol-vs-dianabol-bulking-steroids-compared/ wazifafood.com
http://ydds.cloud:3000/zanetuggle5985 http://ydds.cloud:3000/zanetuggle5985
https://forge.paperland.sg/pearlineconnib https://forge.paperland.sg/
https://csmsound.exagopartners.com/concetta03k742 csmsound.exagopartners.com
http://43.138.83.20:3000/shantaemarch44 http://43.138.83.20:3000/shantaemarch44
http://218.78.131.42:10030/latonyadelance 218.78.131.42
https://git.sophiagwen.au/ffxesteban747 https://git.sophiagwen.au
http://112.124.59.113:3000/marcelmaclean 112.124.59.113
http://8.129.11.230:7002/lannymailey975 8.129.11.230
https://git.apr.moscow/columbuspring https://git.apr.moscow/columbuspring
References:
https://jobs.maanas.in/institution/unlocking-muscle-gains-the-dbol-cycle-guide/
http://111.229.35.227:3000/kirkclements10 · March 20, 2026 at 5:42 pm
References:
Re-built mass side effects
References:
https://music.batalp.com/angiebehrends
https://git.slegeir.com · March 20, 2026 at 6:44 pm
common oral steroids
http://120.76.251.151:3000/elizabethcolor 120.76.251.151
https://www.postajob.co.uk/employer/dianabol-d-bol-methandrostenolone-benefits-uses-side-effects/ http://www.postajob.co.uk
https://web.datestreama.com/@thaddeusmoulde https://web.datestreama.com/@thaddeusmoulde
http://41.59.86.39:3000/adellzhang950 41.59.86.39
http://labai.polinema.ac.id:3000/larueconcepcio labai.polinema.ac.id
http://repo.magicbane.com/seymourbilodea repo.magicbane.com
http://nenadmihajlovic.net/forum/index.php?topic=1382181.0 nenadmihajlovic.net
http://shqkxh.org:3000/gabriellanjr00 shqkxh.org
http://47.100.208.160:51300/mattwatriama05 47.100.208.160
https://121.43.209.3:9443/adolphmcfarlan 121.43.209.3
https://platform.giftedsoulsent.com/ionashang2866 https://platform.giftedsoulsent.com/ionashang2866
http://106.55.61.128:3000/henryscarberry http://106.55.61.128/
https://git2.ujin.tech/phillippxna72 git2.ujin.tech
http://awg.bplaced.net/smf/index.php?action=profile;u=82592 http://awg.bplaced.net/
http://8.155.160.224:3000/melaniericci72 8.155.160.224
https://gitea.jobiglo.com/miaunaipon6937 https://gitea.jobiglo.com
https://git.deadpoo.net/everettolsen74 https://git.deadpoo.net
https://towerclimbers.work/employer/legal-raw-steroids-for-research-only/ towerclimbers.work
References:
http://58.213.60.6:19000/dorrisfree5258
https://career-hunters.com · March 20, 2026 at 7:19 pm
hardening agent bodybuilding
http://114.203.209.83:3000/milliefrisby2 http://114.203.209.83:3000/milliefrisby2
https://emphira.app/@kieram2977233 emphira.app
http://211.149.155.157:3000/donnastoneman 211.149.155.157
http://47.113.149.107:10110/evebetancourt9 http://47.113.149.107:10110/evebetancourt9
http://114.132.234.216:3000/olliefrancois 114.132.234.216
http://120.26.116.243:3000/mattlovelace63 http://120.26.116.243:3000/mattlovelace63
https://185.157.13.217/terrieedments https://185.157.13.217/
http://182.92.251.55:3000/ewrtrinidad59 182.92.251.55
http://tfjiang.cn:32773/shanondeschamp tfjiang.cn
https://git.dotb.cloud/brittnyktm643 git.dotb.cloud
http://38.47.180.165:3000/gildapzr180869 http://38.47.180.165:3000/gildapzr180869
https://conexaempregos.com.br/companies/what-is-the-legality-of-steroids-in-thailand-2026-laws-and-regulations/ https://conexaempregos.com.br/companies/what-is-the-legality-of-steroids-in-thailand-2026-laws-and-regulations
https://zudate.com/@shirleymcculle zudate.com
http://47.100.95.58:3000/sheltonclapp51 47.100.95.58
http://115.159.194.75:4000/kamangel146473 http://115.159.194.75/
http://global.gwangju.ac.kr/bbs/board.php?bo_table=g0101&wr_id=2109133 http://global.gwangju.ac.kr/bbs/board.php?bo_table=g0101&wr_id=2109133
https://drarchina.com/demo/@hopehulsey8896?page=about https://drarchina.com/demo/@hopehulsey8896?page=about
http://120.25.164.109:3000/carrollchilds http://120.25.164.109:3000/carrollchilds
References:
http://55x.top:9300/tristaconnelly
divitube.com · March 20, 2026 at 7:21 pm
steroids like supplements
http://8.134.11.35:3000/buerosetta5784 8.134.11.35
https://oke.zone/profile.php?id=248161 oke.zone
https://tunelifystream.com/kimberlymichal tunelifystream.com
http://114.215.207.150:3000/mittiezvk11456 http://114.215.207.150:3000/mittiezvk11456
http://47.102.36.9:3000/ryanfihelly584 47.102.36.9
https://www.godhip.com/gregkilburn825 https://www.godhip.com/gregkilburn825
https://git.autotion.net/mitchelpie0361 git.autotion.net
https://git.sskuaixiu.com/kimberlyc64313 https://git.sskuaixiu.com/
http://musicstreaming.yonetsystems.com/hannahcollie1 musicstreaming.yonetsystems.com
http://101.42.28.156:3000/jgnleonel5635 http://101.42.28.156:3000/jgnleonel5635
http://58.221.216.202:3000/verlenestillma 58.221.216.202
https://koonis.net/mitchells05215 https://koonis.net/
https://towerclimbers.work/employer/legal-raw-steroids-for-research-only/ towerclimbers.work
http://218.232.111.112:8300/hortensehowden 218.232.111.112
https://git.m.ctf.arrobe.fr/claribelswadli git.m.ctf.arrobe.fr
https://drarchina.com/demo/@hopehulsey8896?page=about https://drarchina.com/demo/@hopehulsey8896?page=about
http://47.113.103.172:3000/mose53i9142003 http://47.113.103.172:3000/mose53i9142003
https://soundrecords.zamworg.com/mukjohanna6276 soundrecords.zamworg.com
References:
https://meeting2up.it/@tressaedwards
merchantale.com · March 20, 2026 at 8:29 pm
References:
Steroids to lose weight and gain muscle
References:
http://git.yanei-iot.com:600/annmariehilton/2688jobs.khtp.com.my/wiki/Test-and-Dbol-Cycle-Dosage-for-Rapid-Muscle-and-Strength-Gains
http://43.156.250.29 · March 20, 2026 at 10:49 pm
References:
Winstrol anabolic
References:
http://182.92.251.55:3000/kylebeer111664
amore.is · March 20, 2026 at 11:06 pm
References:
Super trenbolone
References:
http://111.230.9.98:3000/lucasdoerr7780
http://103.119.85.197/ · March 21, 2026 at 12:41 am
can you get big without steroids
https://www.singuratate.ro/@lynellmckibben singuratate.ro
https://www.nextlink.hk/@juanitafogle08 nextlink.hk
https://git.alexavr.ru/isidrobundey16 git.alexavr.ru
https://ott.saikatinfotech.com/@melvinbattarbe?page=about ott.saikatinfotech.com
http://182.92.251.55:3000/alvad122914538 182.92.251.55
http://repo.magicbane.com/seymourbilodea repo.magicbane.com
http://8.152.223.61:3000/sallieballinge http://8.152.223.61/
https://luvmatefreematrimony.com/@nicholaspalmer https://luvmatefreematrimony.com/
http://85.214.41.219:49153/gracielademaio 85.214.41.219
http://122.51.51.35:3000/brandonwatson8 122.51.51.35
https://git.entryrise.com/georgina10g631 https://git.entryrise.com/georgina10g631
http://provision-sa.co.za:3000/cerysbiaggini0 provision-sa.co.za
http://www.mikarsoft.com/geoffreymartel http://www.mikarsoft.com/
https://www.melnica-group.ru/charlie7979739 melnica-group.ru
https://qarisound.com/reaganfarringt https://qarisound.com/
http://47.100.212.83:3000/dorinebaines83 http://47.100.212.83/
https://yours-tube.com/@hubertoswalt50?page=about yours-tube.com
http://120.77.94.227:9999/alexandralarna 120.77.94.227
References:
http://8.153.108.90:3000/alishanickson
http://tian-you.top · March 21, 2026 at 1:29 am
human growth hormone steroids
https://gitea.micro-stack.org/katherinepersi gitea.micro-stack.org
https://git.successkaoyan.com/meridithmcrae7 git.successkaoyan.com
https://app.boliviaplay.com.bo/jacquiemeza39 https://app.boliviaplay.com.bo/jacquiemeza39
http://106.55.0.66:31807/merilonergan53 http://106.55.0.66:31807/merilonergan53
http://shqkxh.org:3000/madgebidwill7 shqkxh.org
http://38.47.180.165:3000/gildapzr180869 38.47.180.165
https://tea.neuron.my/vonnievanhorn8 tea.neuron.my
https://healedonly.com/@penneykneebone healedonly.com
http://8.129.11.230:7002/dorisgariepy32 8.129.11.230
https://desante.dev/reaganlopes538 https://desante.dev
http://103.248.30.24:3000/nanbreton55818 http://103.248.30.24
http://120.24.175.146:3000/cecilegwendole http://120.24.175.146:3000/cecilegwendole
https://jobsathealthcare.com/employer/dianabol-vs-tren-the-ultimate-showdown-of-anabolics-for-muscle-gains/ jobsathealthcare.com
http://43.153.171.246:3000/marion29558176 43.153.171.246
https://gitea.jobiglo.com/miaunaipon6937 gitea.jobiglo.com
https://adufoshi.com/corrinebardon8 adufoshi.com
https://aprileaton.net/merlebeauregar aprileaton.net
https://emphira.app/@kennethdkp2970 https://emphira.app/
References:
http://103.228.160.127:3100/jessiehanton04
registrera dig f"or binance · March 21, 2026 at 2:52 am
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
https://truworker.com/employer/danabol-balkan-pharmaceuticals-10mg-tab-60tab-int/ · March 21, 2026 at 5:29 am
will one cycle of testosterone hurt you
https://laviesound.com/derrickrennie laviesound.com
http://120.77.94.227:9999/cassandramccue http://120.77.94.227/
http://106.55.61.128:3000/henryscarberry http://106.55.61.128
https://zm.aosenhw.com/@linomatra0449 zm.aosenhw.com
http://47.92.23.195:8418/alejandrinagab 47.92.23.195
https://www.robots.rip/xiomarafrederi http://www.robots.rip
http://41.180.4.117:3000/shelleyzimmerm 41.180.4.117
http://47.100.95.58:3000/sheltonclapp51 http://47.100.95.58
http://60.205.246.14:3389/raeccg90135493 60.205.246.14
https://sportjobs.gr/employer/jumping-the-border-for-performance-enhacing-drugs-job-listings-employer-listings-employmentjobsapplicants-for-maui-countyhawaii/ https://sportjobs.gr/
https://emphira.app/@kennethdkp2970 https://emphira.app/@kennethdkp2970
https://web.datestreama.com/@kristinelapine web.datestreama.com
https://git.sskuaixiu.com/koryd512845287 https://git.sskuaixiu.com/
http://47.94.173.135:3000/aliza47i289003 47.94.173.135
https://git.sophiagwen.au/vaypolly795312 git.sophiagwen.au
http://119.23.72.7/gus47o15108416 119.23.72.7
https://desante.dev/candidaskalski desante.dev
https://jstalentssolution.com/employer/660/how-to-make-your-dianabol-cycle-a-success https://jstalentssolution.com/employer/660/how-to-make-your-dianabol-cycle-a-success
References:
http://47.94.173.135:3000/celiaarmijo827
ubet95 · March 21, 2026 at 6:14 pm
I loved as much as you’ll receive carried out right here. The sketch is tasteful, your authored subject matter stylish. nonetheless, you command get got an impatience over that you wish be delivering the following. unwell unquestionably come more formerly again as exactly the same nearly a lot often inside case you shield this hike.
правила игры в блэкджек · March 21, 2026 at 11:31 pm
правила игры в блэкджек
джой казино зеркало на сегодня · March 21, 2026 at 11:32 pm
джой казино официальный сайт
http://223.108.157.174:3000/seleneesparza · March 22, 2026 at 3:42 am
References:
Jay cutler steroid
References:
https://git.parat.swiss/osflorri729946/www.theangel.fr2021/wiki/Detection+Times+of+Steroids
https://www.ringfloriangeyer.de/ · March 22, 2026 at 11:49 am
References:
Vaping and bodybuilding
References:
https://www.nina-perl.com/HOME/index.php/;focus=STRATP_com_cm4all_wdn_Flatpress_39616974&path=&frame=STRATP_com_cm4all_wdn_Flatpress_39616974?x=entry:entry250921-212437%3Bcomments:1
https://www.st-toenis-erleben.de/ · March 22, 2026 at 1:19 pm
References:
The closest thing to steroids
References:
https://www.rbconsulting.info/MEDIEN-BLOG/BLOG/index.php/;focus=HSTPTP_com_cm4all_wdn_Flatpress_6899652&frame=HSTPTP_com_cm4all_wdn_Flatpress_6899652?x=entry:entry210302-234514;comments:1
esportenet · March 22, 2026 at 2:18 pm
Hey very nice web site!! Guy .. Beautiful .. Amazing .. I will bookmark your web site and take the feeds additionally? I am glad to seek out numerous helpful information here in the put up, we want develop extra techniques on this regard, thanks for sharing. . . . . .
www.djk-breitendiel.de · March 22, 2026 at 4:01 pm
References:
Best deca cycle
References:
https://www.ff-garlstorf.de/;focus=TKOMSI_com_cm4all_wdn_Flatpress_21838727&path=&frame=TKOMSI_com_cm4all_wdn_Flatpress_21838727?x=entry:entry240908-094448%3Bcomments:1
www.kraftplatz-weibel.ch · March 22, 2026 at 4:14 pm
References:
Best injectable steroid
References:
https://rheindoerfer.koeln/News/index.php/;focus=NCSITE_com_cm4all_wdn_Flatpress_229119&path=&frame=NCSITE_com_cm4all_wdn_Flatpress_229119?x=entry:entry251027-152001%3Bcomments:1
рулетка удачи · March 23, 2026 at 12:44 pm
колесо фортуны играть на деньги
Tür öffnen Worms · March 23, 2026 at 3:36 pm
Schlüsseldienst Worms
big win · March 23, 2026 at 5:54 pm
Have you ever considered creating an e-book or guest authoring on other sites? I have a blog based on the same subjects you discuss and would really like to have you share some stories/information. I know my visitors would value your work. If you’re even remotely interested, feel free to shoot me an e-mail.
demopgslots · March 24, 2026 at 3:44 am
Fenerbahce 0-3 Nottingham Forest 2026 Europa League play-off shock
goinbet · March 24, 2026 at 2:37 pm
Hi there friends, pleasant paragraph and fastidious urging commented at this place, I am actually enjoying by these.
moverbet · March 24, 2026 at 7:01 pm
I got this web site from my buddy who shared with me regarding this website and now this time I am visiting this website and reading very informative posts at this time.
pgsoftdemográtis · March 25, 2026 at 4:58 pm
Jogo do Tigrinho tá on fire em 2026! Quem já pegou x10 na cartinha misteriosa essa semana?
betx24 · March 25, 2026 at 11:52 pm
It’s appropriate time to make a few plans for the long run and it is time to be happy. I’ve learn this submit and if I may just I desire to recommend you few fascinating things or advice. Maybe you could write next articles regarding this article. I wish to learn more things approximately it!
demoslot · March 26, 2026 at 9:07 am
Cassino PG Soft com roleta diária: 80–250 giros grátis no Fortune Tiger toda noite
폰테크 · March 26, 2026 at 3:29 pm
폰테크
폰테크라는 방식은 자금이 급히 필요한 상황에서 많이 찾는 방식으로 소개됩니다. 최근에는 비대면 진행과 당일 입금, 미납요금 대납, 전국 상담 같은 항목이 함께 붙으면서 안내 문구도 늘어났습니다. 그렇다고 해서 검토할 때는 빠르다는 말보다 진행 구조를 먼저 봐야 합니다. 접수 방식, 진행 형태, 입금까지의 흐름을 먼저 확인하는 편이 낫습니다.
비대면 폰테크의 경우 방문 없이 상담부터 접수, 진행 안내까지 이어지는 구조가 많습니다. 서울, 경기, 인천 같은 수도권뿐 아니라 강원도, 충청도, 전라도, 경상도, 제주까지 전국 대응을 강조하는 곳도 많습니다. 이동 부담이 적다는 점은 장점이지만, 간단해 보일수록 조건은 더 세밀하게 봐야 합니다.
폰테크·가개통 안내 문구에서는 당일 진행, 당일 입금, 24시간 상담, 연중무휴 같은 문구가 자주 보입니다. 이런 문구보다 더 중요한 것은 진행 방식의 구체성입니다. 어떤 기종을 기준으로 상담하는지, 매입 조건이 어떻게 잡히는지, 비대면·방문·출장·대납 중 어떤 방식이 가능한지, 접수 후 입금은 언제 이뤄지는지까지 정리돼 있어야 합니다.
진행 흐름은 대체로 비슷합니다. 전화·문자·카카오톡으로 접수를 받고, 이후 기종과 조건에 맞춰 상담을 진행한 뒤, 방문, 출장, 비대면, 대납 중 방식을 고른 뒤, 기기 수령 뒤 바로 지급으로 이어지는 방식입니다. 순서는 짧아 보여도 실제 확인 항목은 적지 않습니다. 상담 단계에서 진행 가능 여부와 조건을 명확히 해야 이후 혼선이 적습니다.
전국 단위로 운영된다고 하는 곳들은 서울, 부산, 대구, 경기, 인천, 광주, 울산, 대전, 세종, 강원, 충북, 충남, 전북, 전남, 경북, 경남, 제주처럼 지역명을 촘촘히 배치합니다. 이런 방식은 지역 키워드 노출에 유리하고, 방문자에게 본인 지역도 포함된다는 느낌을 줍니다. 서울 폰테크, 경기 폰테크, 인천 가개통 같은 표현이 반복되는 이유도 여기에 있습니다.
상담 채널은 대체로 전화, 카카오톡, 신청 버튼 중심으로 구성됩니다. 보통 이런 채널 옆에는 신속 진행이나 1:1 상담 문구가 함께 배치됩니다. 실제로 봐야 할 것은 문구보다 운영 방식과 설명의 명확성입니다.
요약하면 핵심 포인트는 세 가지입니다. 현금이 급할 때 빠르게 검토할 수 있다는 점, 비대면과 전국 단위 상담이 가능하다는 점, 절차 흐름이 비교적 단순하다는 점입니다. 반대로 이용자 입장에서는 속도보다 조건, 절차, 지역 대응 범위, 상담 내용의 명확성을 먼저 봐야 합니다.
talon777 · March 27, 2026 at 4:51 am
An outstanding share! I’ve just forwarded this onto a co-worker who was doing a little research on this. And he actually bought me dinner simply because I stumbled upon it for him… lol. So allow me to reword this…. Thanks for the meal!! But yeah, thanks for spending some time to talk about this matter here on your website.
betcris · March 27, 2026 at 11:29 am
I am sure this piece of writing has touched all the internet visitors, its really really fastidious paragraph on building up new webpage.
폰테크 · March 27, 2026 at 6:39 pm
폰테크
폰테크라는 방식은 급하게 현금이 필요할 때 빠르게 검토되는 방식으로 거론됩니다. 최근에는 비대면 진행, 당일 입금, 미납요금 대납, 전국 상담 같은 요소가 함께 붙으면서 관련 안내도 더 많아졌습니다. 다만 실제로 알아볼 때는 빠르다는 말보다 진행 구조를 먼저 봐야 합니다. 어떤 절차로 접수되고 진행되고 입금되는지 보는 것이 우선입니다.
비대면 폰테크의 경우 방문 없이 상담, 접수, 진행 안내까지 상당 부분을 원격으로 처리하는 형태가 중심입니다. 서울·경기·인천 같은 수도권은 물론이고 강원도, 충청도, 전라도, 경상도, 제주까지 전국 대응을 강조하는 곳도 많습니다. 직접 움직이지 않아도 된다는 점은 편하지만, 절차가 단순해 보일수록 조건 확인은 더 정확해야 합니다.
이런 서비스 안내에서는 보통 당일 진행, 당일 입금, 24시간 상담, 365일 연중무휴 같은 표현이 반복됩니다. 하지만 핵심은 문구가 아니라 진행 내용의 구체성입니다. 상담 기준 기종, 매입 조건, 가능한 진행 방식, 접수 후 입금 시점까지 분명해야 합니다.
보통 진행 구조는 크게 다르지 않습니다. 전화·문자·카카오톡으로 접수를 받고, 조건과 기종을 확인한 다음, 원하는 거래 방식을 선택하고, 기기 수령 뒤 바로 지급으로 이어지는 방식입니다. 단계 수는 적어 보여도 실제로는 각 단계마다 확인할 내용이 다릅니다. 특히 처음 상담 단계에서 가능 조건을 분명히 해두는 것이 중요합니다.
전국 대응을 강조하는 업체들은 서울, 부산, 대구, 경기, 인천, 광주, 울산, 대전, 세종, 강원, 충북, 충남, 전북, 전남, 경북, 경남, 제주처럼 지역명을 촘촘히 배치합니다. 이런 방식은 지역 키워드 노출에 유리하고, 이용자에게 자기 지역도 가능하다는 인식을 줍니다. 이 때문에 지역명 조합 키워드가 반복적으로 쓰입니다.
상담 채널은 보통 대표전화, 카카오톡, 상담신청 버튼처럼 바로 연결되는 구조로 잡힙니다. 보통 이런 채널 옆에는 신속 진행이나 1:1 상담 문구가 함께 배치됩니다. 실제로 봐야 할 것은 문구보다 운영 방식과 설명의 명확성입니다.
결국 폰테크 소개에서 핵심은 세 가지입니다. 현금이 급할 때 빠르게 검토할 수 있다는 점, 비대면과 전국 단위 상담이 가능하다는 점, 절차 흐름이 비교적 단순하다는 점입니다. 이용자 기준에서는 빠르다는 말보다 조건과 절차를 먼저 보는 편이 맞습니다.
phwin · March 28, 2026 at 1:34 pm
bookmarked!!, I love your website!
winbra · March 29, 2026 at 7:50 am
We are a group of volunteers and opening a new scheme in our community. Your website offered us with valuable information to work on. You have done an impressive job and our entire community will be grateful to you.
폰테크 · March 29, 2026 at 12:18 pm
폰테크
폰테크는 자금이 급히 필요한 상황에서 자주 검토되는 수단으로 거론됩니다. 최근 들어 비대면 방식, 당일 입금, 미납요금 대납, 전국 상담 등이 함께 붙으면서 관련 안내도 더 많아졌습니다. 다만 실제로 알아볼 때는 속도보다 구조를 먼저 봐야 합니다. 어떤 절차로 접수되고 진행되고 입금되는지 보는 것이 우선입니다.
비대면 방식의 폰테크는 직접 방문하지 않고 상담과 접수, 진행 안내를 원격으로 처리하는 형태가 많습니다. 서울·경기·인천 같은 수도권은 물론이고 강원도, 충청도, 전라도, 경상도, 제주까지 전국 상담이 가능하다고 안내하는 경우가 많습니다. 직접 움직이지 않아도 된다는 점은 편하지만, 보기보다 단순해 보여도 조건 확인은 더 꼼꼼해야 합니다.
폰테크·가개통 안내 문구에서는 당일 진행, 당일 입금, 24시간 상담, 연중무휴 같은 문구가 자주 보입니다. 하지만 핵심은 문구가 아니라 진행 내용의 구체성입니다. 어떤 기종을 다루는지, 조건이 어떻게 정해지는지, 어떤 방식으로 진행 가능한지, 입금 시점이 언제인지까지 확인돼야 합니다.
보통 진행 구조는 크게 다르지 않습니다. 전화나 문자, 카카오톡으로 상담을 시작한 뒤, 조건과 기종을 확인한 다음, 방문, 출장, 비대면, 대납 중 방식을 고른 뒤, 기기 수령 뒤 바로 지급으로 이어지는 방식입니다. 겉으로는 단순해 보여도 단계마다 체크할 부분은 다릅니다. 특히 상담 단계에서 본인 상황에 맞는 진행 형태와 가능 조건을 분명히 해야 뒤에서 꼬이지 않습니다.
전국 서비스를 내세우는 곳들은 지역명을 세세하게 나열하는 경우가 많습니다. 이런 구성은 지역 검색에 강하고, 사용자에게 해당 지역에서도 진행 가능하다는 인상을 줍니다. 지역명과 서비스명을 붙인 표현이 반복되는 이유도 여기에 있습니다.
상담 채널은 대체로 전화, 카카오톡, 신청 버튼 중심으로 구성됩니다. 여기에 정식등록업체, 비대면 당일입금, 1:1 상담 같은 문구가 붙습니다. 다만 판단 기준은 광고 문구가 아니라 운영 정보와 절차 설명입니다.
결국 폰테크 소개에서 핵심은 세 가지입니다. 현금이 급할 때 빠르게 검토할 수 있다는 점, 비대면과 전국 단위 상담이 가능하다는 점, 절차 흐름이 비교적 단순하다는 점입니다. 반대로 실제 확인 포인트는 속도가 아니라 조건과 절차, 지역 대응 범위입니다.
폰테크 · March 30, 2026 at 1:19 pm
폰테크
폰테크는 보통 급하게 현금이 필요할 때 많이 찾는 방식으로 언급됩니다. 최근에는 비대면 진행과 당일 입금, 미납요금 대납, 전국 상담 같은 항목이 같이 노출되면서 안내 문구도 늘어났습니다. 다만 실제로 알아볼 때는 속도보다 절차를 먼저 확인해야 합니다. 접수 방식, 진행 형태, 입금까지의 흐름을 먼저 확인하는 편이 낫습니다.
비대면 폰테크는 방문 없이 상담, 접수, 진행 안내까지 상당 부분을 원격으로 처리하는 형태가 중심입니다. 서울, 경기, 인천 같은 수도권뿐 아니라 강원·충청·전라·경상·제주까지 전국 단위 상담을 내세우는 경우도 많습니다. 이동 부담이 적다는 점은 장점이지만, 보기보다 단순해 보여도 조건 확인은 더 꼼꼼해야 합니다.
이런 서비스 안내에서는 보통 당일 진행, 당일 입금, 24시간 상담, 365일 연중무휴 같은 표현이 반복됩니다. 중요한 것은 표현보다 실제 진행 방식입니다. 어떤 기종을 다루는지, 조건이 어떻게 정해지는지, 어떤 방식으로 진행 가능한지, 입금 시점이 언제인지까지 확인돼야 합니다.
보통 진행 구조는 크게 다르지 않습니다. 전화, 문자, 카카오톡으로 상담 신청을 받고, 이후 기종과 조건에 맞춰 상담을 진행한 뒤, 방문, 출장, 비대면, 대납 중 방식을 고른 뒤, 기기 수령 뒤 바로 지급으로 이어지는 방식입니다. 순서는 짧아 보여도 실제 확인 항목은 적지 않습니다. 특히 상담 단계에서 본인 상황에 맞는 진행 형태와 가능 조건을 분명히 해야 뒤에서 꼬이지 않습니다.
전국 단위로 운영된다고 하는 곳들은 서울, 부산, 대구, 경기, 인천, 광주, 울산, 대전, 세종, 강원, 충북, 충남, 전북, 전남, 경북, 경남, 제주처럼 지역명을 촘촘히 배치합니다. 이런 방식은 지역 키워드 노출에 유리하고, 이용자에게 자기 지역도 가능하다는 인식을 줍니다. 이 때문에 지역명 조합 키워드가 반복적으로 쓰입니다.
상담 채널은 보통 대표전화, 카카오톡, 상담신청 버튼처럼 바로 연결되는 구조로 잡힙니다. 그리고 여기에 정식등록업체, 당일입금, 1:1 상담 같은 표현이 더해집니다. 실제로 봐야 할 것은 문구보다 운영 방식과 설명의 명확성입니다.
요약하면 핵심 포인트는 세 가지입니다. 급전 상황에서 빠르게 진행할 수 있다는 점, 비대면과 전국 상담이 가능하다는 점, 상담 신청부터 지급까지 흐름이 단순하다는 점입니다. 반대로 이용자 입장에서는 속도보다 조건, 절차, 지역 대응 범위, 상담 내용의 명확성을 먼저 봐야 합니다.
wjevo · March 30, 2026 at 1:29 pm
I’m not sure why but this blog is loading very slow for me. Is anyone else having this issue or is it a problem on my end? I’ll check back later and see if the problem still exists.
Pk55 · March 31, 2026 at 4:56 am
That is a really good tip especially to those new to the blogosphere. Short but very accurate information… Appreciate your sharing this one. A must read article!
www.pulaplay.com · March 31, 2026 at 11:43 am
References:
Legal steroids 2019
References:
https://daterondetjolie.fr/@darrylmarcello
https://gitea.octifor.synology.me:60443/cornellbrunski · March 31, 2026 at 11:45 am
steroid body transformation
https://git.paulll.cc/todjarman48448 https://git.paulll.cc
https://gitea.adber.tech/carmelohorning gitea.adber.tech
https://gitea.ww3.tw/pedrochaplin85 gitea.ww3.tw
https://git.daoyoucloud.com/malissalondon/malissa2007/wiki/Clenbuterol-Wie-sicher-ist-es-wirklich%3F https://git.daoyoucloud.com/malissalondon/malissa2007/wiki/Clenbuterol-Wie-sicher-ist-es-wirklich?
https://mp3diary.com/demetriusduran mp3diary.com
http://124.236.46.74:9103/jorgqueen5109/gitlab.iplusus.com2020/wiki/Clenbuterol-Wirkung%2C-Anwendung%2C-Nebenwirkungen 124.236.46.74
https://botttechgroup.com/coreyangas8693 botttechgroup.com
https://play.talkdrove.cc.nf/@virginiaboucau?page=about play.talkdrove.cc.nf
https://mauicountyvirtualjobfair.com/employer/sind-clenbuterol-kuren-wirklich-sicher-zum-cutting/ mauicountyvirtualjobfair.com
http://43.138.83.20:3000/sherlynfalcone 43.138.83.20
http://47.107.168.59:3000/hiltonbowler99 47.107.168.59
https://git.lifetop.net/melbahartwell https://git.lifetop.net/melbahartwell
https://txuki.duckdns.org/ismaelbeals031 txuki.duckdns.org
http://82.26.157.11:3001/young57m199482 82.26.157.11
https://git.cyberuk.me/seleneshinn222 git.cyberuk.me
https://shop.apexo.in/@alvasaunders1?page=about https://shop.apexo.in/@alvasaunders1?page=about
https://xn--lpris-iua.nu/robcrook384121 https://lpris-iua.nu
https://qarisound.com/yiwblanca9017 qarisound.com
References:
http://xeroworld.team/hortensebaughm
http://59.110.47.157/ · March 31, 2026 at 12:10 pm
when misused
https://git.hgbenjamin.com/gwenponder046 https://git.hgbenjamin.com
https://srsbkn.eu.org/bernadettesidn srsbkn.eu.org
https://i10audio.com/alliechuter148 https://i10audio.com/alliechuter148
https://git.ihatemen.uk/rogerfetty5017 git.ihatemen.uk
https://nauticauruguay.com/rosariaramos59/iamtube.jp9983/wiki/Clenbuterol-40-mcg-50-tabs https://nauticauruguay.com
http://123.57.146.97:3000/helainekline97 http://123.57.146.97:3000/helainekline97
https://vigilanteapp.com/@krystalhaygood?page=about vigilanteapp.com
http://210.211.116.85:3000/bernadettebrog http://210.211.116.85:3000/bernadettebrog
https://mycrewdate.com/@torstengagai4 mycrewdate.com
https://silatdating.com/@edgar90497764 silatdating.com
https://gitea.scivigi.com/alexandria9241/git.anibilag.ru2998/wiki/Nebenwirkungen%3A-Clenbuterol-nicht-so-harmlos-wie-oft-gedacht gitea.scivigi.com
http://8.155.172.147:3001/keljohnette653 8.155.172.147
http://74.48.174.77:3000/antonyswu0815 74.48.174.77
http://139.196.103.114:18084/lindseysteel5/git.autotion.net6542/wiki/Clenbuterol-Dosierung http://139.196.103.114:18084/lindseysteel5/git.autotion.net6542/wiki/Clenbuterol-Dosierung
http://209.127.59.74:3000/brennastonor72 209.127.59.74
http://175.27.229.211:3000/coreyalfonso0/5191interior01.netpro.co.kr/wiki/Clenbuterol%3A-Erfahrungen%2C-Wirkung-%26-Alternativen-2026 http://175.27.229.211
https://gitee.planhomecloud.cn/peggy79k15609 https://gitee.planhomecloud.cn/peggy79k15609
https://git2.ne-it.net/alonzox2336759 git2.ne-it.net
References:
http://121.36.47.159:3000/eliflack901684/eli2020/wiki/Batteriespeicherl%C3%B6sungen-f%C3%BCr-Gewerbe
armenianmatch.com · March 31, 2026 at 12:18 pm
injectable steroid cycles
https://indianmixedwrestling.com/@ibokathleen994?page=about indianmixedwrestling.com
http://209.127.59.74:3000/brennastonor72 209.127.59.74
https://nauticauruguay.com/shelleyhodel8/shelley1980/wiki/Clenbuterol%3A-Wirkung%2C-Anwendungsgebiete-%26-Nebenwirkungen-%C2%BB-Krank-de https://nauticauruguay.com
https://gitea.amazingcoders.com/irenecurrent43/1803go-ro.eu/wiki/Clenbuterol%3A-Wirkung%2C-Nebenwirkungen-%26-Dosierung gitea.amazingcoders.com
https://www.beyoncetube.com/@sbiclaudio8263?page=about http://www.beyoncetube.com
http://122.116.190.233:3001/modestachauncy/modesta2018/wiki/Clenbuterol-Dosierung http://122.116.190.233:3001/modestachauncy/modesta2018/wiki/Clenbuterol-Dosierung
https://maru.bnkode.com/@arturoschmidt maru.bnkode.com
https://dating.hyesearch.com/@melainehowland dating.hyesearch.com
https://ltube.us/@lavinatedesco3?page=about ltube.us
https://git.sophiagwen.au/enriquemckenny git.sophiagwen.au
http://35.207.205.18:3000/imogenfrq59204/imogen1986/wiki/SPIROPENT-Tabletten-100-St–Bodfeld-Apotheke 35.207.205.18
http://106.55.174.214:3000/kentlessard578/543249.233.255.41/wiki/Clenbuterol-zum-Abnehmen http://106.55.174.214
https://tubevieu.com/@ofeliag5227054?page=about tubevieu.com
https://music.michaelmknight.com/hestergarvey6 music.michaelmknight.com
https://cloveebiz.com.ng/@pamngabidj6115?page=about https://cloveebiz.com.ng
https://www.shwemusic.com/kerriewhitting http://www.shwemusic.com
https://git.huwhy.cn/hollycruse0569 https://git.huwhy.cn
https://git.dotb.cloud/jefferytuckson https://git.dotb.cloud/jefferytuckson
References:
http://124.71.197.109:3000/richardfegan1
revenu.live · March 31, 2026 at 12:19 pm
how to get testosterone legally
https://git.ihatemen.uk/rogerfetty5017 git.ihatemen.uk
http://47.98.161.246:3000/aletheazhc8172/82.156.89.212001/wiki/Spiropent-Tabletten%3A-Dosierung%2C-Nebenwirkung-%26-Wirkung 47.98.161.246
https://git.cute.bet/antoineboykin/8595tayartaw.kyaikkhami.com/wiki/Erste+Schritte+mit+dem+Bodybuilding+mit+Clenbuterol-Steroid.- https://git.cute.bet/antoineboykin/8595tayartaw.kyaikkhami.com/wiki/Erste Schritte mit dem Bodybuilding mit Clenbuterol-Steroid.-
https://askmilton.tv/@merrillbedford?page=about askmilton.tv
https://meeting2up.it/@mariotillman8 meeting2up.it
http://106.55.61.128:3000/epifaniakersey 106.55.61.128
http://111.228.34.40:3000/asaallingham5 111.228.34.40
https://www.krakhead.dev/rudyplott1049/rudy2015/wiki/Medikamente-mit-dem-Bestandteil-Clenbuterol-hydrochlorid https://www.krakhead.dev
https://code.hpswk.com/robertobracegi/roberto2012/wiki/Vorher-Nachher-Ergebnisse-%26-die-richtige-Dosierun-Deus-.. https://code.hpswk.com/robertobracegi/roberto2012/wiki/Vorher-Nachher-Ergebnisse-&-die-richtige-Dosierun-Deus-..
https://git.tecno-group.mx/gabrielevanott git.tecno-group.mx
https://www.ttd.group/earnestinecara http://www.ttd.group
https://smallbusinessinternships.com/employer/aktuelles/ smallbusinessinternships.com
https://pod.tek.us/@njmwilbur6782?page=about pod.tek.us
http://139.196.96.28:13000/sylvia99s44080 http://139.196.96.28/
https://www.meetgr.com/@athenawinchest https://www.meetgr.com/@athenawinchest
https://git.clubeye.net/zenaidabagwell https://git.clubeye.net
http://106.15.235.242/nelsondelittle http://106.15.235.242/nelsondelittle
https://rsas.de/kandi32j087512 https://rsas.de/kandi32j087512
References:
https://romatube.com/@korycostello9?page=about
nrimatchmaking.com · March 31, 2026 at 12:19 pm
what is an anabolic hormone
https://volts.howto.co.ug/@nell65e4808810 volts.howto.co.ug
https://code.wemediacn.com/harrietlowes6 code.wemediacn.com
https://git.cute.bet/sandyx79479499 https://git.cute.bet/
https://dianyanai.com/franziskastrad https://dianyanai.com/
http://47.100.44.145:3000/veolanowell292 http://47.100.44.145:3000/veolanowell292
https://git.vsadygv.com/jeffrycarnes87 git.vsadygv.com
http://www.skwcf.top/fawn3593895877/git.silvertone.com.au1987/wiki/Clenbuterol-Dosierung http://www.skwcf.top
http://152.136.145.93:3000/rachelcota9049/gitea.nkal.me9704/wiki/Spiropent-Wirkung%2C-Nebenwirkungen%2C-Dosierung 152.136.145.93
https://www.workbay.online/profile/will1397759069 https://www.workbay.online/
http://36.133.248.69:3088/juditelfer5949 36.133.248.69
https://www.workerrenter.pro/profile/antjeclouse913 https://www.workerrenter.pro/
https://git.econutrix.com/estellarader42 git.econutrix.com
https://www.howeasynetwork.com/@gladiszavala4?page=about https://www.howeasynetwork.com/@gladiszavala4?page=about
https://loopplay.site/@pennicouncil1?page=about loopplay.site
http://41.59.86.39:3000/vanceschweizer/vance1988/wiki/Clenbuterol-Wirkung%2C-Nebenwirkungen%2C-Dosierung 41.59.86.39
https://wiibiplay.fun/@leticiatorode4?page=about wiibiplay.fun
https://www.chembans.com/@theresa57t3199 https://www.chembans.com
http://repo.atamiso.com/mitchellricci0/3048152/wiki/SPIROPENT+Tabletten+100+St+Preisvergleich%2C+PZN+1980325 http://repo.atamiso.com/
References:
http://47.99.119.173:13000/jessieenos1820/jessie1985/wiki/Ambroxol-%2B-Clenbuterol%3A-Nebenwirkung-%26-Wechselwirkung
https://camtalking.com · March 31, 2026 at 12:49 pm
buying online steroids
https://videowala.xyz//@rqwelizabet470?page=about https://videowala.xyz/
https://nrimatchmaking.com/@cierramulgrave nrimatchmaking.com
https://code.wemediacn.com/gracielalanham code.wemediacn.com
https://git.autotion.net/tonyharry7396 https://git.autotion.net/tonyharry7396
https://git.paulll.cc/kerih648727264/121.43.244.2095959/wiki/Clenbuterol%3A-Erfahrungen-%26-Nebenwirkungen https://git.paulll.cc
http://119.29.198.206:5630/jungdon7530070 119.29.198.206
http://musicstreaming.yonetsystems.com/alejandrinapro musicstreaming.yonetsystems.com
https://chubechube.com/@martinharringt?page=about chubechube.com
http://1.13.196.248:3000/theo80e8063158 http://1.13.196.248:3000/theo80e8063158
https://unitedmusicstreaming.com/janiehandley18 unitedmusicstreaming.com
https://meeting2up.it/@grettafortin19 meeting2up.it
https://hiwifi.denq.us:8418/juliannsmn8980 hiwifi.denq.us
https://loopplay.site/@pennicouncil1?page=about loopplay.site
https://nildigitalco.com/@susanneyrj6410?page=about nildigitalco.com
https://daftsex.lol/@jerefaith3585?page=about daftsex.lol
https://www.pulaplay.com/@kimberlynutter?page=about https://www.pulaplay.com/
https://vcs.cozydsp.space/maureen2179383/4263157.66.191.31/wiki/Spiropent-Tropfen-Wirkung%2C-Nebenwirkungen%2C-Dosierung vcs.cozydsp.space
https://git.lmbrs.org/terencejpw6062/41.59.86.392024/wiki/Clenbuterol%3A-Wirkung%2C-Anwendungsgebiete%2C-Nebenwirkungen git.lmbrs.org
References:
https://git.lifetop.net/lulapeterson18
http://49.233.255.41:3000/alfiedeshotel0 · March 31, 2026 at 12:54 pm
anabolic steroids athletes
https://git.gasshog.fr/danniellehalls/62.234.194.661993/wiki/Clenbuterol%3A-Verwendungen%2C-Nebenwirkungen-und-Risiken git.gasshog.fr
http://120.211.66.170:8418/tamarapack0056 120.211.66.170
https://git.silvertone.com.au/bjwabby4172081/git.cyberuk.me2021/wiki/Clenbuterol%3A-Erfahrungen%2C-Wirkung-%26-Alternativen-2026 https://git.silvertone.com.au
https://vidspace.store/@maci376682192?page=about vidspace.store
https://csmtube.exagopartners.com/@gitaquimby757?page=about csmtube.exagopartners.com
http://43.139.144.12:3000/samualgrills34 http://43.139.144.12:3000/samualgrills34
https://gitea.cfpoccitan.org/ariellecantero gitea.cfpoccitan.org
http://45.144.30.78:8083/ulrich63g08785 45.144.30.78
https://opensource.irext.net/theresamedland opensource.irext.net
https://www.godhip.com/dewittdonahoe http://www.godhip.com
https://adlr.cig22.com/randycpy554305 adlr.cig22.com
http://musicstreaming.yonetsystems.com/alejandrinapro http://musicstreaming.yonetsystems.com/
https://playxtream.com/@napoleon595739?page=about playxtream.com
https://nauticauruguay.com/seymourreese19 nauticauruguay.com
https://frp-mad.com:45237/christelbeale https://frp-mad.com/
https://git.vajdak.cz/karolinivy9521 git.vajdak.cz
https://traficut.com/@emorypak00998?page=about traficut.com
https://sithcom.de/hrxessie980421 https://sithcom.de/hrxessie980421
References:
https://git.binarycat.org/leslihuber0597
git.minecraftlegacy.com · March 31, 2026 at 1:03 pm
References:
Do steroids shrink your penis
References:
https://www.krakhead.dev/candelariaangl/www.mvacancy.com7221/wiki/Clenbuterol-Erfahrungen-%EF%B8%8F-Test-und-Bewertungen-2026
mailppto.top · March 31, 2026 at 1:21 pm
medical names for steroids
https://hipstrumentals.net/britneypurnell hipstrumentals.net
https://hipstrumentals.net/britneypurnell hipstrumentals.net
http://gitea.huangyanjie.com/ivallewellyn72 gitea.huangyanjie.com
http://dns.chenzhao.date:3000/heribertoatenc/giaovienvietnam.vn1983/wiki/Clenbuterol%3A-Wirkung%2C-Nebenwirkungen-und-sichere-Alternativen http://dns.chenzhao.date/
https://git.csi-kjsce.org/valentinaschna https://git.csi-kjsce.org/
http://1.95.192.200:59300/andreastell388 http://1.95.192.200
https://www.foreignspouse.com/@deneendunrossi https://www.foreignspouse.com/@deneendunrossi
http://101.126.150.202:3001/merissas191528 http://101.126.150.202:3001/merissas191528
http://8.134.11.35:3000/sadyedimarco38 http://8.134.11.35:3000/sadyedimarco38
http://101.35.227.2:3000/leorahaszler43/gitea.belanjaparts.com4960/wiki/Clenbuterol 101.35.227.2
https://dev.modelhub.org.cn/caitlingeogheg dev.modelhub.org.cn
https://date.etogetherness.com/@adrienekaberry https://date.etogetherness.com/@adrienekaberry
https://geniusactionblueprint.com/@shaylapalladin?page=about geniusactionblueprint.com
http://210.211.116.85:3000/antonioducan83 http://210.211.116.85:3000/antonioducan83
https://git.mauve.haus/willisiliffe3 git.mauve.haus
https://git.hgbenjamin.com/lynwood9369188 git.hgbenjamin.com
https://hero-cloud-stg-code.cnbita.com/winstongillies/winston1999/wiki/Clenbuterol-und-gezielter-Fettabbau hero-cloud-stg-code.cnbita.com
https://yourclipz.com/@linettearndell?page=about yourclipz.com
References:
http://39.96.211.118:3000/blythedickens9
goeed.com · March 31, 2026 at 1:40 pm
tren cutting cycle
http://106.15.235.242/katherine89729/7955863/wiki/Clenbuterol:-Fettkiller-oder-gef%C3%A4hrliches-Dopingmittel%3F http://106.15.235.242/katherine89729/7955863/wiki/Clenbuterol:-Fettkiller-oder-gefährliches-Dopingmittel?
https://hlumi.com/@millie44j1948?page=about https://hlumi.com/@millie44j1948?page=about
http://113.177.27.200:2033/simongritton4/www.ihomethink.com1991/wiki/Muskelaufbau-trotz-Di%C3%A4t%3F-Was-mit-Clenbuterol-tats%C3%A4chlich-m%C3%B6glich-ist 113.177.27.200
https://hearty.rip/hildakeith2240 hearty.rip
https://ttym.space/myrabolton713 ttym.space
https://zenithgrs.com/employer/clenovet-0025-mg-ml-fachinformation/ https://zenithgrs.com/employer/clenovet-0025-mg-ml-fachinformation/
http://code.sz-chaohui.cn/scotteusebio86 code.sz-chaohui.cn
https://ns2.asso-web.com/qtjangie38279 https://ns2.asso-web.com/qtjangie38279
https://git.suo0.com/gisellegalarza https://git.suo0.com
http://120.48.141.82:3000/jannaavent3384/gitea.nongnghiepso.com1984/wiki/Cera-Clen-Ceranfeldreiniger-200-ml 120.48.141.82
https://abadeez.com/@sybilpyle3017?page=about https://abadeez.com/@sybilpyle3017?page=about
https://git.mauve.haus/jameynagel9913 https://git.mauve.haus/
http://220.132.16.87:3000/callumsommer55 220.132.16.87
https://www.workerrenter.pro/profile/antoinel292002 http://www.workerrenter.pro
http://82.156.121.2:3000/shaunabennett 82.156.121.2
https://git.clickforadventure.co/venbarbra87444/code.tczkiot.com3546/wiki/Was-sind-die-besten-Steroide-f%C3%BCr-Gewichtsverlust%3F git.clickforadventure.co
https://git.binarycat.org/josephineswaff https://git.binarycat.org
https://tcodpractice.com/tod28j60291647 tcodpractice.com
References:
https://seychelleslove.com/@mauricemcbride
http://139.59.100.212 · March 31, 2026 at 3:40 pm
References:
Gain muscle fast pills
References:
https://reoflix.com/@benito78i2918?page=about
43.156.250.29 · March 31, 2026 at 3:44 pm
health risks of anabolic steroids
https://vcs.cozydsp.space/efrainhuitt60 vcs.cozydsp.space
https://git.flymiracle.com/alejandramcdon git.flymiracle.com
https://git.davisdre.com/georgianagroom git.davisdre.com
http://47.100.44.145:3000/kristopher1909/7941245/wiki/Muskelaufbau-trotz-Di%C3%A4t%3F-Was-mit-Clenbuterol-tats%C3%A4chlich-m%C3%B6glich-ist http://47.100.44.145
https://mycrewdate.com/@michalcrouch69 https://mycrewdate.com/@michalcrouch69
https://reputable.cc/profile/stephanmercado https://reputable.cc/
https://www.godhip.com/ewanpresler506 http://www.godhip.com
https://vcs.cozydsp.space/efrainhuitt60 https://vcs.cozydsp.space/
http://101.42.28.156:3000/jamistarr60492 101.42.28.156
https://bigotube.com/@dorothea482151?page=about bigotube.com
https://iesoundtrack.tv/@bobbyeacuna91?page=about https://iesoundtrack.tv
https://git.successkaoyan.com/galenharness97 git.successkaoyan.com
https://shamrick.us/vanitag046488 shamrick.us
https://gitea.nongnghiepso.com/sophiez6766358/8299daftsex.lol/wiki/%E1%90%85-Anwendungsgebiete%2C-Dosierung-und-Nebenwirkungen-von-Clenbuterol gitea.nongnghiepso.com
http://139.196.103.114:18084/leonorbeazley1 http://139.196.103.114/
https://shop.apexo.in/@fredericka4435?page=about shop.apexo.in
https://git.ewengadonnaud.xyz/josetteboulton/3050inmessage.site/wiki/Clenbutrol-Erfahrungen%3A-Selbsttest%2C-Ergebnisse-%26-Bewertung-2026 git.ewengadonnaud.xyz
http://47.109.137.67:9091/latoshamadewel 47.109.137.67
References:
https://git.stormrain.cn/lyndoncramsie
armenianmatch.com · March 31, 2026 at 3:45 pm
anabolic supplements side effects
https://7yue.net/howardb0797623 7yue.net
https://git.huwhy.cn/bernard8446030 https://git.huwhy.cn/
https://freshtube.net/@anh87u85013269?page=about freshtube.net
http://104.254.131.244:3000/wilmernewell62/6031kayesbamusic.com/wiki/Clenbuterol-Anwendung%2C-Wirkung%2C-Nebenwirkungen 104.254.131.244
http://118.178.172.49:3000/leonorekirsova 118.178.172.49
http://47.111.1.12:3000/ymwbeatrice11 47.111.1.12
https://git.paulll.cc/skyeclawson800/4862friztty.com/wiki/Kaufen-Steroid-Kur-Plans-Online https://git.paulll.cc/
https://git.refinementservices.com/hiramwebb89794 https://git.refinementservices.com/hiramwebb89794
https://git.stormrain.cn/timothybooth36 https://git.stormrain.cn/
https://gitea.my-intrudair.com/mercedeso3522/6446vlotube.com/wiki/Clenbuterol%3A-Wirkung%2C-Anwendungsgebiete%2C-Nebenwirkungen gitea.my-intrudair.com
http://121.43.244.209:30000/margheritamcco/2131649/wiki/Spiropent-TN-Drug-Information%2C-Uses%2C-Side-Effects%2C-Chemistry http://121.43.244.209/
https://viddertube.com/@elmaoreilly984?page=about https://viddertube.com/
https://jovita.com/clarita82c2182 https://jovita.com/clarita82c2182
http://27.223.88.102:33000/coy47152864673 27.223.88.102
http://www.skwcf.top/carynschroeder/chubechube.com1999/wiki/Clenbuterol-Anwendung%2C-Wirkung%2C-Nebenwirkungen http://www.skwcf.top
https://git.healthathome.com.np/donettebatts6 https://git.healthathome.com.np
https://gitea.amazingcoders.com/marlenelerma76 gitea.amazingcoders.com
https://zm.aosenhw.com/@hellen45513360 https://zm.aosenhw.com/
References:
https://git.fast-blast.uk/hassan32120021
tubevieu.com · March 31, 2026 at 4:29 pm
anabolic steroid bodybuilding
http://104.254.131.244:3000/jilldfr3938465/1061687/wiki/Spiropent-Clenbuterolhydrochlorid-online-kaufen-Preis-%26-Kosten-Everyone-org 104.254.131.244
http://120.77.94.227:9999/bernardkimber http://120.77.94.227/
https://hero-cloud-stg-code.cnbita.com/belindacorrie/6615236/wiki/Der-ultimative-Clenbuterol-Kur-Plan%3A-Dosierung%2C-Vorteile-und-Risiken hero-cloud-stg-code.cnbita.com
https://rlgit.pro/zelmadearing6/2862www.canadiannewcomerjobs.ca/wiki/Doping:-alle-Informationen-zu-Clenbuterol https://rlgit.pro/
http://zzdgitea.stnav.com/juanitagass75 http://zzdgitea.stnav.com
https://git.ruixininfo.com/timmygardiner8 git.ruixininfo.com
https://jobs.foodtechconnect.com/companies/einschleichen/ https://jobs.foodtechconnect.com/
http://111.230.243.127:3000/daltonsam06825 http://111.230.243.127:3000/daltonsam06825
http://47.98.161.246:3000/gladistowns945 47.98.161.246
https://playtube.live//@maddisonmullen?page=about playtube.live
https://theudtaullu.com/@kendalllorenz5?page=about https://theudtaullu.com/@kendalllorenz5?page=about
https://camtalking.com/@shalandai0671 https://camtalking.com/@shalandai0671
https://buzzafricanmusic.com/xvzchristian40 https://buzzafricanmusic.com/xvzchristian40
https://lookingforjob.co/profile/kirstengleason lookingforjob.co
https://rsas.de/ahmadvarney72 rsas.de
https://git.vsadygv.com/trentmahan7921 https://git.vsadygv.com/
https://www.pajob.ch/employer/spiropent-tabletten-anwendung/ http://www.pajob.ch
https://armenianmatch.com/@diannefetty13 armenianmatch.com
References:
http://139.196.103.114:18084/leonorbeazley1
www.mvacancy.com · March 31, 2026 at 4:58 pm
References:
Muscle stack gnc
References:
http://62.43.207.91:8889/keeshahinds992
8.155.172.147 · March 31, 2026 at 5:24 pm
weight gain steroids
http://1.95.192.200:59300/toddastley3218 1.95.192.200
http://59.80.22.43:30000/roxannakellawa 59.80.22.43
https://omegat.dmu-medical.de/jacquelynshack/2375033/wiki/Clenbuterol-einnehmen:-Risiken-und-Nebenwirkungen https://omegat.dmu-medical.de/jacquelynshack/2375033/wiki/Clenbuterol-einnehmen:-Risiken-und-Nebenwirkungen
https://gitea.ontoast.uk/iveyboyland04/2359735/wiki/Die-Auswirkungen-von-Clenbuterol-auf-die-Basale-Stoffwechselrate-Expertenwissen-zu-Sportpharma https://gitea.ontoast.uk/
https://x1.tvos.cygnux.cn/ineslangler13 https://x1.tvos.cygnux.cn/ineslangler13
https://dyipniflix.com/site/@vivienf7052760?page=about https://dyipniflix.com/site/@vivienf7052760?page=about
https://txuki.duckdns.org/christopergues txuki.duckdns.org
https://playtube.live//@maddisonmullen?page=about playtube.live
https://git.fs.cs.uni-frankfurt.de/francesschutt https://git.fs.cs.uni-frankfurt.de
http://101.35.227.2:3000/kareem09a2846/gitea.gimmin.com7892/wiki/SPIROPENT-100-St-PZN-01980325 101.35.227.2
https://choosy.cc/@harrisviles02 choosy.cc
https://uk4mag.co.uk/video/@myrnabowes540?page=about uk4mag.co.uk
https://git.ecorous.org/charlinetisdal git.ecorous.org
https://git.adambissen.me/esteladonohue git.adambissen.me
https://gt.clarifylife.net/orenlefevre77 gt.clarifylife.net
http://106.55.61.128:3000/barbratilton53 106.55.61.128
https://vw-git.senecasense.com/marilou203812 vw-git.senecasense.com
http://blv-rd.tech:3001/norinewallace1 blv-rd.tech
References:
https://yourclipz.com/@averypenton075?page=about
gitlab.iplusus.com · March 31, 2026 at 5:41 pm
sport steroids
https://lius.familyds.org:3000/ulrikegiffen63 lius.familyds.org
http://43.134.49.17:3000/kiarasledge286 http://43.134.49.17:3000/kiarasledge286
http://39.101.170.62:9080/maurine82l8907 http://39.101.170.62:9080/maurine82l8907
https://hearty.rip/hildakeith2240 https://hearty.rip/
https://suprastream.tv/@ivaworthy7951?page=about suprastream.tv
https://fresh-jobs.in/employer/wie-effektiv-ist-clenbuterol-zur-gewichtsreduktion/ fresh-jobs.in
https://www.monasticeye.com/@pansypremo5427?page=about http://www.monasticeye.com
https://camtalking.com/@leliafrancis3 https://camtalking.com/@leliafrancis3
https://www.ohovideo.com/@felicitasswadl?page=about http://www.ohovideo.com
http://47.101.59.106:8181/rebeccahiggin/rebecca2012/wiki/Die+Rolle+von+Clenbuterol+in+der+Keto-Di%C3%A4t%3A+Ein+Expertenblick+Trainingsoptimierung+durch+Sportpharma 47.101.59.106
https://archea.dev/ouidalazarev1 https://archea.dev
https://www.tracksmyvan.com/francescap3768 http://www.tracksmyvan.com
https://gitea.brmm.ovh/ashleyrigsby4 https://gitea.brmm.ovh/ashleyrigsby4
https://git.fast-blast.uk/hassan32120021 git.fast-blast.uk
https://gitea.ww3.tw/porfiriocarney gitea.ww3.tw
https://hellomusic.app/valeriehogg723 https://hellomusic.app/
http://60.205.162.59:3000/marcustrue9386 60.205.162.59
http://81.70.24.14:3000/gudruna5511591 81.70.24.14
References:
https://dreamplacesai.de/virgil4820262
iraqitube.com · March 31, 2026 at 6:31 pm
gnc products protein
https://armenianmatch.com/@wesleyets22015 armenianmatch.com
http://183.236.243.71:3693/wileycarslaw3/4947125.229.107.240/wiki/Spiropent-kaufen 183.236.243.71
http://spnewstv.com/@kandikcv024991?page=about spnewstv.com
https://xonnon.com/@greg65q7798865?page=about xonnon.com
http://1.95.120.11:3000/reda12y000549 1.95.120.11
http://115.190.13.94:3333/vilmalovely839 115.190.13.94
https://lookingforjob.co/profile/kirstengleason lookingforjob.co
http://112.74.106.216:3000/avarowland9928 http://112.74.106.216:3000/avarowland9928
http://207.180.227.11:3001/ezekielthalber 207.180.227.11
https://xn--lpris-iua.nu/rochellesocha0 https://lpris-iua.nu/rochellesocha0
https://mycrewdate.com/@rosettabeeton mycrewdate.com
https://git.clubeye.net/alphonsoschnei git.clubeye.net
https://rlgit.pro/zelmadearing6/2862www.canadiannewcomerjobs.ca/wiki/Doping:-alle-Informationen-zu-Clenbuterol https://rlgit.pro/zelmadearing6/2862www.canadiannewcomerjobs.ca/wiki/Doping:-alle-Informationen-zu-Clenbuterol
https://volts.howto.co.ug/@tracymichalski volts.howto.co.ug
http://1.95.192.200:59300/samanthamonten http://1.95.192.200:59300/samanthamonten
https://videowala.xyz//@allieplace904?page=about https://videowala.xyz//@allieplace904?page=about
https://mardplay.com/davidaukp57879 mardplay.com
http://47.98.183.226:3000/rudolffreeman1 47.98.183.226
References:
https://stream.aea3.net/@james20r96712?page=about
www.izen.live · March 31, 2026 at 6:48 pm
anabolic steroids short term effects
https://fanajobs.com/profile/delilahgodson7 https://fanajobs.com/
http://www.scserverddns.top:13000/ronniebaader57 http://www.scserverddns.top
https://sportsdungeon.com/@germanbatman07?page=about sportsdungeon.com
http://66.179.208.56:3001/chantelno89334 66.179.208.56
http://gitlab.dev.jtyjy.com/laceynph870074 http://gitlab.dev.jtyjy.com
https://theudtaullu.com/@kendalllorenz5?page=about https://theudtaullu.com
https://hearty.rip/ricardobate054 hearty.rip
https://demo.playtubescript.com/@tanjamudie5638?page=about demo.playtubescript.com
https://goondepot.com/@barrettbevill8?page=about goondepot.com
http://47.98.161.246:3000/stephaniateal5 http://47.98.161.246
https://code.wemediacn.com/alizakerferd10/1050git.econutrix.com/wiki/Clenbuterol-Lexikon-der-Chemie https://code.wemediacn.com/alizakerferd10/1050git.econutrix.com/wiki/Clenbuterol-Lexikon-der-Chemie
https://mycrewdate.com/@michalcrouch69 mycrewdate.com
https://videos.awaregift.com/@stepaniemontgo?page=about videos.awaregift.com
https://www.peter-bartke.de/islat93771552 https://www.peter-bartke.de
https://gitea.css-sistemas.com.br/nilamckeel1458 https://gitea.css-sistemas.com.br/
https://git.lucas-michel.fr/leticiasleath7/leticia1987/wiki/SPIROPENT-Tabletten-Beipackzettel git.lucas-michel.fr
https://suprastream.tv/@kerrikappel83?page=about https://suprastream.tv/@kerrikappel83?page=about
https://vigilanteapp.com/@alonzoostrande?page=about https://vigilanteapp.com/@alonzoostrande?page=about
References:
https://liverights.org//@jonelle37c7962?page=about
http://111.230.9.98:3000/tressahargis82 · March 31, 2026 at 7:02 pm
References:
I love steroids
References:
http://106.52.21.251:3000/berniemilford
gitea.diputadosalta.gob.ar · March 31, 2026 at 7:07 pm
what are anabolic steroids?
https://gitea.gimmin.com/liamsalisbury gitea.gimmin.com
https://gitea.biboer.cn/bellstanford7 gitea.biboer.cn
https://git.hanumanit.co.th/maximilianchas git.hanumanit.co.th
https://www.asiapay-safe.top/hxucory0136030 http://www.asiapay-safe.top
http://47.76.48.105:3000/jhomildred895 http://47.76.48.105
http://blv-rd.tech:3001/julietamealmak http://blv-rd.tech:3001/julietamealmak
http://209.127.59.74:3000/estelapaz65951 209.127.59.74
https://git.malls.iformall.com/venusfhd913890/6456409/wiki/Spiropent-Wirkung%2C-Nebenwirkungen%2C-Dosierung git.malls.iformall.com
https://music.wzsipku.cn/ashleighcaroth music.wzsipku.cn
https://git.econutrix.com/lucasmcmichael git.econutrix.com
https://qarisound.com/stephania34w5 https://qarisound.com/
https://www.superphage.org/changkeble6894 http://www.superphage.org
http://47.92.113.131:3000/modestofassbin 47.92.113.131
https://loopplay.site/@marielcatron9?page=about loopplay.site
https://git.saike.fun:9755/carleyfinniss4/carley2020/wiki/Spiropent-Gebrauchsinformation git.saike.fun
https://git.veraskolivna.net/adrieneslocum git.veraskolivna.net
https://mginger.org/@kendraandrew03 mginger.org
https://code.wemediacn.com/gracielalanham/graciela2009/wiki/This-Is-Everything-You-Need-to-Know-About-Clenbuterol code.wemediacn.com
References:
https://lookingforjob.co/profile/madeleinesnook
git.ccmhub.se · March 31, 2026 at 7:33 pm
what are steroids composed of
http://115.190.13.94:3333/vilmalovely839 115.190.13.94
https://li1420-231.members.linode.com/jordank633830/7726115.190.214.62/wiki/Leistungen li1420-231.members.linode.com
https://chinami.com/@barrett6309359?page=about chinami.com
https://koseongnam.com/vicenteabt9319 https://koseongnam.com/
http://62.234.201.16/chauscullin612 http://62.234.201.16/
https://funnyutube.com/@leesacalwell64?page=about https://funnyutube.com/@leesacalwell64?page=about
https://lius.familyds.org:3000/ulrikegiffen63 https://lius.familyds.org/
https://code.tczkiot.com/sdjlavina4798 https://code.tczkiot.com/sdjlavina4798
https://git.binarycat.org/josephineswaff git.binarycat.org
https://gitea.nongnghiepso.com/maddisonbetts https://gitea.nongnghiepso.com/maddisonbetts
https://liverights.org//@jonelle37c7962?page=about https://liverights.org//@jonelle37c7962?page=about
https://gitea.nongnghiepso.com/maddisonbetts https://gitea.nongnghiepso.com
https://playtube.live//@dorthycrampton?page=about playtube.live
https://www.pulaplay.com/@kathaleenmull?page=about http://www.pulaplay.com
https://gitea.wuyuank.com/titusbaskett03 gitea.wuyuank.com
https://movieru.jp/portfolio/@mickichartres?page=about https://movieru.jp/
https://parnian.app/daciadebavay82 https://parnian.app/daciadebavay82
http://106.52.242.177:3000/kristibromham1 http://106.52.242.177:3000/kristibromham1
References:
http://218.245.96.10/kermitnewkirk
frp-mad.com · March 31, 2026 at 7:40 pm
the understanding gender is permanent is called
https://smartastream.com/@latoyabrient05?page=about https://smartastream.com
https://www.tracksmyvan.com/francescap3768 https://www.tracksmyvan.com
https://x1.tvos.cygnux.cn/ineslangler13 x1.tvos.cygnux.cn
https://www.wealthtv.tz/@elaineriddick?page=about http://www.wealthtv.tz
https://datingmywish.com/@tysongqd515889 https://datingmywish.com/
http://spnewstv.com/@kandikcv024991?page=about spnewstv.com
http://47.105.124.101:3000/pennitompkins 47.105.124.101
https://git.gonethome.id/sibylgrace4406 https://git.gonethome.id/
https://gitea.cantrell.io/frederickahigg/blackvision.co.uk8268/wiki/Meine-Erfahrungen-mit-CBD-%C3%96l-ein-Wundermittel%3F gitea.cantrell.io
http://git.520hx.vip/belenhunley30/3822git.cute.bet/wiki/SPIROPENT-Tabletten-100-St–Bodfeld-Apotheke http://git.520hx.vip
https://www.peter-bartke.de/enriquetawrefo https://www.peter-bartke.de
https://www.shlakoblock.com/emildahl907111 http://www.shlakoblock.com
http://218.78.131.42:10030/jina3121361451 http://218.78.131.42:10030/jina3121361451
https://actsolution.iptime.org:3000/magnoliacorrie https://actsolution.iptime.org
http://183.204.60.122:10081/silaswoodd453 http://183.204.60.122
http://82.26.157.11:3001/jeanacottee437 http://82.26.157.11/
https://124.70.144.1/hannahrays3788 124.70.144.1
https://codes.tools.asitavsen.com/lucianabritton https://codes.tools.asitavsen.com/lucianabritton
References:
https://gitea.amazingcoders.com/kirbygascoigne/2930925/wiki/Clenbuterol-Spiropent
http://36.153.162.171:3000/alanatreacy02/alana1994/wiki/Bestimmung der idealen Clenbuterol-Dosierung Driada Medical Store Offizieller Premium-Wiederverkäufer Schneller und sicherer Versand.- · March 31, 2026 at 7:49 pm
whats androgen
https://demo.playtubescript.com/@tanjamudie5638?page=about demo.playtubescript.com
https://hipstrumentals.net/janisidaway50 https://hipstrumentals.net/
https://git.cute.bet/laurieburdge1 git.cute.bet
http://styleupnow.com/@stanleyhahn13?page=about styleupnow.com
https://www.krakhead.dev/clairefreeland/claire2023/wiki/SPIROPENT-Tabletten-PZN-01980325 http://www.krakhead.dev
https://git.e-drones.com/latiagurney707 git.e-drones.com
https://git.davisdre.com/karlntu1841837 git.davisdre.com
https://git.archieri.fr/melva16h550480 git.archieri.fr
https://stream.aea3.net/@james20r96712?page=about stream.aea3.net
https://maxtravelagencys.com/employer/ventipulmin-ad-us-vet/ maxtravelagencys.com
http://66.179.208.56:3001/chantelno89334 http://66.179.208.56
http://58.213.60.6:19000/sherrillpittma 58.213.60.6
https://www.propose.lk/@albawaller2071 http://www.propose.lk
http://101.35.227.2:3000/scottybagot974 http://101.35.227.2:3000/scottybagot974
http://43.156.250.29:3000/homercogburn9 43.156.250.29
http://106.55.61.128:3000/barbratilton53 106.55.61.128
https://gitea.pnkx.top:8/stefaniebethea https://gitea.pnkx.top:8/stefaniebethea
http://81.69.229.51:3000/rodger76d8379 http://81.69.229.51:3000/rodger76d8379
References:
http://43.143.142.38:7001/mplola16926991/7239477/wiki/Clenbuterol%3A-Wirkung%2C-Anwendungsgebiete%2C-Nebenwirkungen
qpxy.cn · March 31, 2026 at 7:54 pm
gnc bodybuilding
https://www.cryptonewss.com/@henrylocke4247?page=about https://www.cryptonewss.com/@henrylocke4247?page=about
http://120.77.94.227:9999/krystaleichhor 120.77.94.227
https://git.123doit.com/cherievalentin https://git.123doit.com/cherievalentin
https://funnyutube.com/@leesacalwell64?page=about funnyutube.com
https://iamtube.jp/@leshlu19626183?page=about iamtube.jp
http://121.43.244.209:30000/margheritamcco/2131649/wiki/Spiropent-TN-Drug-Information%2C-Uses%2C-Side-Effects%2C-Chemistry 121.43.244.209
https://git.davisdre.com/georgianagroom https://git.davisdre.com
https://chenxil.top/elenaziesemer2 https://chenxil.top
https://www.workerrenter.pro/profile/judithdalgety http://www.workerrenter.pro
http://101.42.28.156:3000/staciahembree http://101.42.28.156:3000/staciahembree
https://kidstv.freearnings.com/@hunteralbert94?page=about https://kidstv.freearnings.com/@hunteralbert94?page=about
https://tageeapp.com/@domingagrace10?page=about https://tageeapp.com/@domingagrace10?page=about
https://shop.apexo.in/@fredericka4435?page=about shop.apexo.in
https://www.superphage.org/bradyharker768/43.143.37.1407315/wiki/SPIROPENT http://www.superphage.org
https://www.jobexpertsindia.com/companies/clenbuterol-t3-abnehmkur/ https://www.jobexpertsindia.com/
http://8.141.82.163:20000/duanethibodeau 8.141.82.163
https://git.hubhoo.com/jeromecate1663/124.223.18.411984/wiki/Clenbuterol%3A-Wirkung%2C-Nebenwirkungen-%26-Dosierung git.hubhoo.com
https://gt.clarifylife.net/mitchellmoultr gt.clarifylife.net
References:
http://36.133.248.69:3088/juancandler57
117.102.231.130 · March 31, 2026 at 8:04 pm
effects of prolonged steroid use on the human body
https://gitree.me/rodgerlapine13 https://gitree.me/rodgerlapine13
http://111.230.243.127:3000/daltonsam06825 111.230.243.127
https://git.daoyoucloud.com/ernestinehercu/ernestine1983/wiki/Clenbuterol-kaufen%3A-Der-Ultimative-Leitfaden-F%C3%BCr-M%C3%A4nner-Und-Frauen git.daoyoucloud.com
https://git.meshel.cn/emildeberry483 https://git.meshel.cn/emildeberry483
https://smusic.sochey.com/tammystricklin https://smusic.sochey.com/tammystricklin
https://git.stormrain.cn/timothybooth36 git.stormrain.cn
https://tcodpractice.com/tod28j60291647 tcodpractice.com
http://175.178.150.62:3002/vitohartley691 175.178.150.62
https://reoflix.com/@christianemase?page=about reoflix.com
http://8.140.232.131:8100/delmarasbury98/delmar2008/wiki/Erste-Schritte-mit-dem-Bodybuilding-mit-Clenbuterol-Steroid 8.140.232.131
https://demo.indeksyazilim.com/pdnmilan063887 demo.indeksyazilim.com
https://7yue.net/roxiemein09678 https://7yue.net
https://dev.kiramtech.com/qymeffie725870 dev.kiramtech.com
http://120.48.141.82:3000/jannaavent3384/gitea.nongnghiepso.com1984/wiki/Cera-Clen-Ceranfeldreiniger-200-ml 120.48.141.82
https://www.bongmedia.tv/@moisesloftin72?page=about http://www.bongmedia.tv
https://www.italia24.tv/tube/@marilynjme9021?page=about http://www.italia24.tv
http://120.201.125.140:3000/kittycani72771/6443416/wiki/Clenbuterol-g%C3%BCnstig-online-bestellen-ohne-Rezept 120.201.125.140
http://47.92.113.131:3000/modestofassbin 47.92.113.131
References:
https://koonis.net/debbraharlow99
git.yanei-iot.com · March 31, 2026 at 8:42 pm
anabolic steroids are which of the following
http://74.48.174.77:3000/noemifender307 http://74.48.174.77:3000/noemifender307
https://git.deadpoo.net/adolph31r2991 git.deadpoo.net
https://liverights.org//@jonelle37c7962?page=about liverights.org
http://121.43.244.209:30000/charlenespoffo/1.95.221.1741984/wiki/Der-ultimative-Clenbuterol-Kur-Plan:-Dosierung%2C-Vorteile-und-Risiken http://121.43.244.209
https://hexopt.com/bridgettgunter https://hexopt.com/
https://chinami.com/@juanclayton40?page=about chinami.com
https://git.automathon.org/ankespaull378 git.automathon.org
https://git.init.cool/silviaflannery https://git.init.cool/
https://git.daoyoucloud.com/ingenunn465200 git.daoyoucloud.com
http://8.155.172.147:3001/wilmermortense http://8.155.172.147
https://gitea.kdlsvps.top/arlettethorne3 https://gitea.kdlsvps.top/arlettethorne3
https://git.gonethome.id/jonah95685607 https://git.gonethome.id/
https://soliliquio.com/@brunodartnell0?page=about https://soliliquio.com/
https://viewcast.altervista.org/@jeroldbrennan4?page=about https://viewcast.altervista.org/@jeroldbrennan4?page=about
http://47.115.223.229:8888/maudelongstree http://47.115.223.229
http://47.112.118.149:10082/camillaw118515 47.112.118.149
https://kition.mhl.tuc.gr/pasqualelavall kition.mhl.tuc.gr
https://git.suo0.com/gisellegalarza https://git.suo0.com/
References:
http://194.5.152.156:3000/beatrizrosenst
wangbeibei.xyz · March 31, 2026 at 9:40 pm
most common steroid
http://119.29.249.176:3000/bebedanielson 119.29.249.176
https://git.mwapp.com.br/delilahblaze18 git.mwapp.com.br
http://103.119.85.197:3000/valerialackey1/valeria1991/wiki/Clenbuterol-Wirkung-Fettkiller-oder-gef%C3%A4hrliches-Dopingmittel%3F 103.119.85.197
http://106.55.61.128:3000/barbratilton53 106.55.61.128
https://www.oddmate.com/@valenciagum712 http://www.oddmate.com
https://niqnok.com/leandromanzi32 niqnok.com
http://wangbeibei.xyz:6002/salvatoregowin http://wangbeibei.xyz:6002/salvatoregowin
http://111.228.34.40:3000/vitowooley933 http://111.228.34.40/
https://daftsex.lol/@fatimacarrier8?page=about daftsex.lol
https://hlumi.com/@carsonn0110042?page=about https://hlumi.com/
https://m.my-conf.ru/kaceykuk496658 m.my-conf.ru
https://git.e-drones.com/princessv15948 git.e-drones.com
http://101.37.147.115:3000/antwankyngdon4 http://101.37.147.115:3000/antwankyngdon4
https://www.tracksmyvan.com/francescap3768 https://www.tracksmyvan.com/francescap3768
https://silatdating.com/@myronrosson992 silatdating.com
https://reoflix.com/@euniceobb33614?page=about https://reoflix.com/@euniceobb33614?page=about
http://120.77.94.227:9999/bernardkimber 120.77.94.227
https://kition.mhl.tuc.gr/leeminnis15428 https://kition.mhl.tuc.gr/leeminnis15428
git.smart-tool.jp · March 31, 2026 at 10:05 pm
clenbuterol side effects hair loss
https://tageeapp.com/@dinoflannagan?page=about tageeapp.com
https://niqnok.com/leandromanzi32 niqnok.com
http://119.3.186.224:3000/georgetoussain 119.3.186.224
https://maru.bnkode.com/@thadzimmerman9 maru.bnkode.com
http://139.196.103.114:18084/autumnzgs03069/gitea.mynas-lechner.de1996/wiki/Clenbuterol-Kaufen 139.196.103.114
https://www.cryptonewss.com/@emory766685129?page=about https://www.cryptonewss.com/
https://www.kingspalace.net/maybellegettin/2802158/wiki/Clenbuterol-Wirkung-Effekte%2C-Thermogenese-Und-Fettabbau http://www.kingspalace.net
https://devops.rs2i.fr/julianeclubbe7 devops.rs2i.fr
http://dns.chenzhao.date:3000/pqigiselle9491/skiivie.com2022/wiki/Clenbuterol-im-Vergleich%3A-Alternativen%2C-Wirkung-und-Risiken dns.chenzhao.date
https://gitlab.iplusus.com/xiomaragrantha/xiomara1999/wiki/Spiropent%C2%AE-100-St-mit-dem-E-Rezept-kaufen gitlab.iplusus.com
https://nauticauruguay.com/laurenenolan9/git.stonks.group1986/wiki/SP-Clenbuterol-zu-verkaufen nauticauruguay.com
https://iesoundtrack.tv/@mikeruggieri7?page=about https://iesoundtrack.tv/@mikeruggieri7?page=about
https://thefusionflix.com/@jeramy51592979?page=about thefusionflix.com
https://git.binarycat.org/abduljacoby49/www.xngel.com2464/wiki/Ventipulmin-COPD-and-Bronchitis-Syrup-for-Horses https://git.binarycat.org/abduljacoby49/www.xngel.com2464/wiki/Ventipulmin-COPD-and-Bronchitis-Syrup-for-Horses
https://lasigal.com/vedaclough6750 lasigal.com
https://www.izen.live/chandabsz24769 izen.live
https://mycrewdate.com/@michalcrouch69 https://mycrewdate.com
http://1.95.7.169:3000/ivorywills7375 1.95.7.169
References:
https://musixx.smart-und-nett.de/richmighell796
phoebe.roshka.com · March 31, 2026 at 10:37 pm
steroid online shop
https://www.superphage.org/ernest91k2654/2542441/wiki/Clenbuterol-Anwendungsgebiete https://www.superphage.org
https://videyme.online/@brigittegku349?page=about videyme.online
http://repo.atamiso.com/homerdallas917 http://repo.atamiso.com/homerdallas917
https://twoheartsagency.com/@paulaalston28 twoheartsagency.com
https://goeed.com/@grazynacrooks?page=about goeed.com
https://git.fast-blast.uk/hassan32120021 https://git.fast-blast.uk/
http://www.scserverddns.top:13000/irene47s164599/162.215.134.1496767/wiki/Spiropent-Tabletten%3A-Dosierung%2C-Nebenwirkung-%26-Wirkung http://www.scserverddns.top:13000/irene47s164599/162.215.134.1496767/wiki/Spiropent-Tabletten:-Dosierung,-Nebenwirkung-&-Wirkung
http://git.dglyoo.com/wilford8474270/120.48.144.831996/wiki/Clenbuterol-einnehmen:-Risiken-und-Nebenwirkungen http://git.dglyoo.com/
https://www.hyzq123.com/@elbam189225114?page=about https://www.hyzq123.com/@elbam189225114?page=about
https://gitea.my-intrudair.com/lelacaudle7341/49.233.255.411981/wiki/Das-Tempo-macht%C2%B4s%3A-Medikamente-ein–und-ausschleichen https://gitea.my-intrudair.com/lelacaudle7341/49.233.255.411981/wiki/Das-Tempo-macht´s:-Medikamente-ein–und-ausschleichen
http://104.254.131.244:3000/raqueltroup884/4546fanlibo.i234.me/wiki/Spiropent+Tropfen+30+ml+mit+dem+E-Rezept+kaufen.- http://104.254.131.244:3000/raqueltroup884/4546fanlibo.i234.me/wiki/Spiropent Tropfen 30 ml mit dem E-Rezept kaufen.-
https://myafritube.com/@damianb796213?page=about https://myafritube.com
https://chenxil.top/monagresham34 chenxil.top
http://81.69.229.51:3000/wqjmickey4371 81.69.229.51
https://git.suo0.com/gisellegalarza git.suo0.com
https://www.quranpak.site/maxmadrigal544 https://www.quranpak.site
http://repo.atamiso.com/homerdallas917 repo.atamiso.com
http://www.skwcf.top/lashawnbisdee/9956191/wiki/Clenbutrol-Erfahrungen%3A-Selbsttest%2C-Ergebnisse-%26-Bewertung-2026 http://www.skwcf.top
References:
http://1.117.168.31:3002/margaretflemin
quickdate.arenascript.de · March 31, 2026 at 10:48 pm
References:
Corticosteroids have many muscle building effects
References:
http://8.138.249.120:3000/kristinastrope
http://61.178.84.89 · March 31, 2026 at 10:52 pm
prescription steroid names
http://221.226.114.142:13000/clintonsauls31 221.226.114.142
https://sportsdungeon.com/@germanbatman07?page=about https://sportsdungeon.com/@germanbatman07?page=about
http://47.104.60.158:7777/santopike99277 http://47.104.60.158/
https://www.cryptonewss.com/@emory766685129?page=about cryptonewss.com
https://hellomusic.app/russelhaydon8 https://hellomusic.app/russelhaydon8
https://tayartaw.kyaikkhami.com/carolynpina97 https://tayartaw.kyaikkhami.com/carolynpina97
https://iraqitube.com/@meredithsko332?page=about https://iraqitube.com/@meredithsko332?page=about
https://abadeez.com/@elizahemphill3?page=about abadeez.com
http://123.57.146.97:3000/alfredotunnecl http://123.57.146.97:3000/alfredotunnecl
https://www.itubee.com/@randolphsteinm?page=about http://www.itubee.com
https://www.ohovideo.com/@helenatruebrid?page=about https://www.ohovideo.com/@helenatruebrid?page=about
https://aladin.tube/@garnetreel3704?page=about https://aladin.tube/@garnetreel3704?page=about
https://git.hilmerarts.de/ionafornachon git.hilmerarts.de
http://gitlab.dev.jtyjy.com/laceynph870074 http://gitlab.dev.jtyjy.com
https://git.cute.bet/yongguerard782 git.cute.bet
http://120.77.94.227:9999/nevashillings/dev01.open-alt.com6742/wiki/Spiropent-Wirkung%2C-Nebenwirkungen%2C-Dosierung 120.77.94.227
https://www.jobexpertsindia.com/companies/clenbuterol-t3-abnehmkur/ https://www.jobexpertsindia.com
https://greenopps420.com/@hectori3610825?page=about greenopps420.com
References:
https://124.70.144.1/lucindakeiser
https://mmctube.com · March 31, 2026 at 10:58 pm
gnc supplement stacks
https://7yue.net/howardb0797623 7yue.net
https://quickdate.arenascript.de/@rosauraamaral0 quickdate.arenascript.de
http://121.43.244.209:30000/margheritamcco/2131649/wiki/Spiropent-TN-Drug-Information%2C-Uses%2C-Side-Effects%2C-Chemistry http://121.43.244.209/
https://koseongnam.com/vicenteabt9319 koseongnam.com
http://211.149.155.157:3000/angelorsd02051/111.170.153.1235473/wiki/Clenbuterol-Wikipedia 211.149.155.157
https://bigotube.com/@dorothea482151?page=about https://bigotube.com/@dorothea482151?page=about
https://twoheartsagency.com/@paulaalston28 twoheartsagency.com
http://47.109.137.67:9091/tinaahern53966 47.109.137.67
http://111.230.9.98:3000/scottyfauchery 111.230.9.98
https://datingmywish.com/@tysongqd515889 datingmywish.com
https://truthtube.video/@wesleyrosenhai?page=about truthtube.video
https://zenithgrs.com/employer/clenovet-0025-mg-ml-fachinformation/ zenithgrs.com
http://119.29.64.167:3000/bernardnal606 http://119.29.64.167/
http://47.94.55.54:3000/margaritowemys http://47.94.55.54:3000/margaritowemys
http://git.520hx.vip/belenhunley30/3822git.cute.bet/wiki/SPIROPENT-Tabletten-100-St–Bodfeld-Apotheke git.520hx.vip
https://git.ruixininfo.com/timmygardiner8 git.ruixininfo.com
https://gitea.cantrell.io/frederickahigg/blackvision.co.uk8268/wiki/Meine-Erfahrungen-mit-CBD-%C3%96l-ein-Wundermittel%3F https://gitea.cantrell.io/frederickahigg/blackvision.co.uk8268/wiki/Meine-Erfahrungen-mit-CBD-Öl-ein-Wundermittel?
http://dns.chenzhao.date:3000/pqigiselle9491/skiivie.com2022/wiki/Clenbuterol-im-Vergleich%3A-Alternativen%2C-Wirkung-und-Risiken http://dns.chenzhao.date/
References:
https://gitea.my-intrudair.com/rochellu058062/cyprusjobs.com.cy1984/wiki/Clenbuterol-Dosierung-Clen-f%C3%BCr-Bodybuilding
http://58.65.162.118:3000/clintonsnowden · March 31, 2026 at 11:02 pm
how long does winstrol take to work
http://dns.chenzhao.date:3000/pqigiselle9491/skiivie.com2022/wiki/Clenbuterol-im-Vergleich%3A-Alternativen%2C-Wirkung-und-Risiken dns.chenzhao.date
https://git.clubeye.net/igearnulfo192 git.clubeye.net
https://gitea.jsjymgroup.com/charlenewhitti/charlene2013/wiki/Spiropent-Tabletten-Anwendung gitea.jsjymgroup.com
http://117.72.61.28:5418/isabelladrew40 117.72.61.28
https://hexopt.com/bridgettgunter https://hexopt.com
https://iraqitube.com/@tyreezyz307410?page=about https://iraqitube.com/@tyreezyz307410?page=about
https://git.stormrain.cn/marianabanuelo https://git.stormrain.cn/
https://hunthub.com.au/@christopherbeh?page=about hunthub.com.au
https://spinvai.com/diegoziemba775 spinvai.com
http://43.143.142.38:7001/marylouabate52 43.143.142.38
https://124.70.144.1/lucindakeiser 124.70.144.1
https://www.ohovideo.com/@arnettestocks7?page=about http://www.ohovideo.com
https://superocho.org/@esperanzafoti5?page=about superocho.org
https://git.saidomar.fr/micaela80v9908 https://git.saidomar.fr/micaela80v9908
https://movie.nanuly.kr/@cazcharlene047?page=about movie.nanuly.kr
http://jinhon-info.com.tw:3000/sashaoman80664 jinhon-info.com.tw
https://videowala.xyz//@allieplace904?page=about https://videowala.xyz//@allieplace904?page=about
http://119.91.35.154:3000/peterdeneeve64 119.91.35.154
References:
https://demo.indeksyazilim.com/pdnmilan063887
https://git.genowisdom.cn · March 31, 2026 at 11:48 pm
best substance for muscle growth
https://clipbeans.com/@lynettescroggi?page=about clipbeans.com
http://git.520hx.vip/belenhunley30/3822git.cute.bet/wiki/SPIROPENT-Tabletten-100-St–Bodfeld-Apotheke http://git.520hx.vip/
https://git.mwapp.com.br/delilahblaze18 https://git.mwapp.com.br/
https://code.tczkiot.com/dotty44r569505 code.tczkiot.com
http://119.96.62.56:3000/georgianawedgw 119.96.62.56
https://reoflix.com/@christianemase?page=about reoflix.com
https://qpxy.cn/isishennings33 https://qpxy.cn/isishennings33
https://git.suo0.com/inaradcliffe23/8840407/wiki/Spiropent%C2%AE+100+St+mit+dem+E-Rezept+kaufen.- git.suo0.com
https://www.cryptonewss.com/@emory766685129?page=about http://www.cryptonewss.com
https://code.wemediacn.com/alizakerferd10/1050git.econutrix.com/wiki/Clenbuterol-Lexikon-der-Chemie code.wemediacn.com
http://8.141.82.163:20000/duanethibodeau 8.141.82.163
http://101.43.95.130:3001/ngankzg741136 http://101.43.95.130:3001/ngankzg741136
https://gitea.alexandermohan.com/hueyremley4660/kaymanuell.com2021/wiki/Ventipulmin-Solution-for-Injection-30-micrograms-ml-UPD https://gitea.alexandermohan.com/hueyremley4660/kaymanuell.com2021/wiki/Ventipulmin-Solution-for-Injection-30-micrograms-ml-UPD
https://aladin.tube/@garnetreel3704?page=about aladin.tube
http://36.151.148.78:30000/gailansell238 http://36.151.148.78:30000/gailansell238
http://81.69.229.51:3000/wqjmickey4371 http://81.69.229.51/
http://62.173.140.174:10480/careymontero48/ajmix.in2479/wiki/Vorher-Nachher-Ergebnisse+%26+die+richtige+Dosierun+Deus+…- 62.173.140.174
https://www.quranpak.site/maxmadrigal544 http://www.quranpak.site
References:
http://74.48.174.77:3000/ilakoehn73870
https://myafritube.com/@wendicordner97?page=about · April 1, 2026 at 12:19 am
References:
Anavar reviews bodybuilding
References:
http://112.124.40.88:5510/deannecarruthe/3106947/wiki/Customs-Laboratories-European-Network-CLEN
https://romancefrica.com/@stephanwinter5 · April 1, 2026 at 12:51 am
anavar stacks
http://1.95.192.200:59300/samanthamonten 1.95.192.200
http://47.94.55.54:3000/dannmorehouse4 47.94.55.54
https://www.workerrenter.pro/profile/ddxtiffany376 workerrenter.pro
http://8.138.192.83:39639/jennitimmons35/jenni1998/wiki/Clenbuterol%3A-Verwendungen%2C-Nebenwirkungen-und-Risiken 8.138.192.83
http://58.221.13.198:30010/williambackhou 58.221.13.198
https://worship.com.ng/roxanagarris74 https://worship.com.ng/
http://47.98.161.246:3000/gladistowns945 47.98.161.246
https://git.dieselor.bg/wilfredpattiso git.dieselor.bg
http://111.21.163.58:2321/franr54065808 111.21.163.58
http://82.156.121.2:3000/norman30i39807 http://82.156.121.2/
http://171.244.15.53:3000/rosettamacderm http://171.244.15.53:3000/rosettamacderm
https://maru.bnkode.com/@thadzimmerman9 https://maru.bnkode.com/@thadzimmerman9
http://43.138.249.161:3000/margietripp116 http://43.138.249.161/
https://channel-u.tv/@elmalovekin75?page=about https://channel-u.tv/@elmalovekin75?page=about
https://git.flymiracle.com/alejandramcdon git.flymiracle.com
https://www.shwemusic.com/declanoyp6135 http://www.shwemusic.com
https://nonstopvn.net/@gene85n151229?page=about nonstopvn.net
https://superocho.org/@esperanzafoti5?page=about superocho.org
References:
https://gitea.shizuka.icu/gracielasanche/www.uria.dev2010/wiki/Spiropent-mite-Wirkung%2C-Nebenwirkungen%2C-Dosierung
git.dotb.cloud · April 1, 2026 at 12:53 am
References:
Natural vs steroids
References:
https://phoebe.roshka.com/gitlab/skyecbc132691
gitea.waterworld.com.hk · April 1, 2026 at 1:00 am
steroid pills
http://58.213.60.6:19000/unmkermit7249 http://58.213.60.6:19000/unmkermit7249
http://120.201.125.140:3000/kittycani72771/6443416/wiki/Clenbuterol-g%C3%BCnstig-online-bestellen-ohne-Rezept http://120.201.125.140
https://www.workerrenter.pro/profile/ddxtiffany376 http://www.workerrenter.pro
https://lookingforjob.co/profile/madeleinesnook lookingforjob.co
http://gitea.mikarsoft.com/cclkendra07254 http://gitea.mikarsoft.com
https://mginger.org/@lenabie4450291 https://mginger.org/@lenabie4450291
http://dns.chenzhao.date:3000/edmundpedley0 http://dns.chenzhao.date
http://124.223.89.168:8080/pamelabatista/120.77.94.2272113/wiki/Spiropent-Tabletten-Dosierung 124.223.89.168
https://www.workerrenter.pro/profile/antoinel292002 https://www.workerrenter.pro/
https://youtube.start.h1n.ru/@herminedrum270?page=about youtube.start.h1n.ru
https://lookingforjob.co/profile/yettadelagarza lookingforjob.co
https://soliliquio.com/@brunodartnell0?page=about soliliquio.com
http://47.94.173.135:3000/archie34m1108 47.94.173.135
https://loopplay.site/@marielcatron9?page=about https://loopplay.site
http://101.35.227.2:3000/xiomarawilmoth 101.35.227.2
https://www.complete-jobs.com/employer/what-is-clenbuterol? http://www.complete-jobs.com
http://36.213.200.127:23000/annabellecoane 36.213.200.127
https://www.howeasynetwork.com/@josiekroll5424?page=about http://www.howeasynetwork.com
References:
http://41.59.86.39:3000/martinhammons5/8824334/wiki/Clenbuterol+Ice+Pharmaceuticals+kaufen+bei+60+00+Online-Apotheke+in+Deutschland.-
worldclassdjs.com · April 1, 2026 at 1:21 am
References:
Why are steroids bad for you
References:
https://soliliquio.com/@mickeyhueber9?page=about
http://120.202.38.15/ · April 1, 2026 at 1:50 am
buy steroids cycles
http://47.115.132.164:5500/jonathantolima http://47.115.132.164:5500/jonathantolima
https://mycrewdate.com/@michalcrouch69 mycrewdate.com
https://www.telugustatusvideo.com/@lawannashockey?page=about https://www.telugustatusvideo.com
https://gitea.diputadosalta.gob.ar/phyllisnaquin gitea.diputadosalta.gob.ar
https://git.ultra.pub/shaunbarbee611 git.ultra.pub
https://www.chembans.com/@kinamatthew527 https://www.chembans.com/@kinamatthew527
https://git.deadpoo.net/adolph31r2991 git.deadpoo.net
https://git.fs.cs.uni-frankfurt.de/marissabromby6 https://git.fs.cs.uni-frankfurt.de/marissabromby6
https://wedioz.com/@andreadyason74?page=about wedioz.com
https://omegat.dmu-medical.de/gaylebedggood8 omegat.dmu-medical.de
http://111.230.98.74/hymanhartnett9 111.230.98.74
https://git.saidomar.fr/micaela80v9908 git.saidomar.fr
http://www.skwcf.top/lashawnbisdee/9956191/wiki/Clenbutrol-Erfahrungen%3A-Selbsttest%2C-Ergebnisse-%26-Bewertung-2026 http://www.skwcf.top
https://www.chembans.com/@jonathonosmond chembans.com
https://www.asiapay-safe.top/hxucory0136030 http://www.asiapay-safe.top
https://unitedmusicstreaming.com/leilamohammad https://unitedmusicstreaming.com/leilamohammad
https://kition.mhl.tuc.gr/leeminnis15428 kition.mhl.tuc.gr
https://soliliquio.com/@brunodartnell0?page=about soliliquio.com
References:
http://121.43.244.209:30000/charlenespoffo/1.95.221.1741984/wiki/Der-ultimative-Clenbuterol-Kur-Plan:-Dosierung%2C-Vorteile-und-Risiken
39.98.126.115 · April 1, 2026 at 2:11 am
crazy muscle gains
http://81.70.202.164:3000/saraashe982339 http://81.70.202.164
https://gitea.smatec.com.vn/janetteblaxcel gitea.smatec.com.vn
http://git.yanei-iot.com:600/jovitacarver3/jovita1986/wiki/Das-%C3%A4lteste-Start-up-des-Erzgebirges git.yanei-iot.com
https://git.ccmhub.se/dian29d3299133/gitea.lokach.ru2000/wiki/Clenbuterol-for-Bodybuilding%3A-Side-Effects%2C-Benefits-%26-Risks https://git.ccmhub.se/dian29d3299133/gitea.lokach.ru2000/wiki/Clenbuterol-for-Bodybuilding:-Side-Effects,-Benefits-&-Risks
http://47.112.118.149:10082/camillaw118515 http://47.112.118.149/
http://repo.atamiso.com/homerdallas917 http://repo.atamiso.com/homerdallas917
https://demo.indeksyazilim.com/pdnmilan063887 demo.indeksyazilim.com
https://git.ewengadonnaud.xyz/josetteboulton/3050inmessage.site/wiki/Clenbutrol-Erfahrungen%3A-Selbsttest%2C-Ergebnisse-%26-Bewertung-2026 git.ewengadonnaud.xyz
https://playtube.live//@dorthycrampton?page=about https://playtube.live
https://7yue.net/maziefredricks https://7yue.net
https://truthtube.video/@nancee91p41989?page=about truthtube.video
https://gitea.wuyuank.com/titusbaskett03 gitea.wuyuank.com
http://8.138.139.89:3000/dortheatompson 8.138.139.89
http://47.100.212.83:3000/antoniettajenk http://47.100.212.83:3000/antoniettajenk
https://gitea.micro-stack.org/galenvaldes860 gitea.micro-stack.org
https://www.tracksmyvan.com/madelinecarmon http://www.tracksmyvan.com
http://111.21.163.58:2321/dillonwilbanks http://111.21.163.58:2321/dillonwilbanks
https://thefusionflix.com/@jeramy51592979?page=about https://thefusionflix.com/
References:
http://43.143.142.38:7001/mplola16926991/7239477/wiki/Clenbuterol%3A-Wirkung%2C-Anwendungsgebiete%2C-Nebenwirkungen
repositories.action2quare.com · April 1, 2026 at 3:26 am
craze supplement for sale
https://actsolution.iptime.org:3000/feliciahill740 actsolution.iptime.org
http://220.132.16.87:3000/callumsommer55 220.132.16.87
https://mailppto.top/kimbeike786819 mailppto.top
https://gitea.pnkx.top:8/stefaniebethea gitea.pnkx.top
http://41.59.86.39:3000/jameyhoy719326/124.236.46.742014/wiki/Clenbuterol-Beipackzettel-Dosierung-Med 41.59.86.39
http://blv-rd.tech:3001/julietamealmak blv-rd.tech
http://gitea.yiban.com.tw:3030/sherrylkellerm http://gitea.yiban.com.tw:3030/sherrylkellerm
https://play.talkdrove.cc.nf/@pattyo27577983?page=about play.talkdrove.cc.nf
http://www.tm-jikayo.com/skyeayres0346 tm-jikayo.com
http://8.138.139.89:3000/dortheatompson 8.138.139.89
http://47.112.118.149:10082/camillaw118515 47.112.118.149
https://gitlab.iplusus.com/arronberube526 https://gitlab.iplusus.com/
https://bfreetv.com/@lucaackermann9?page=about bfreetv.com
https://isugar-dating.com/@leopoldojenson isugar-dating.com
http://81.70.202.164:3000/kattiekrimmer 81.70.202.164
https://www.ikaros.asia/nathanielbent http://www.ikaros.asia
https://abadeez.com/@sybilpyle3017?page=about abadeez.com
https://gt.clarifylife.net/orenlefevre77 https://gt.clarifylife.net/orenlefevre77
References:
http://81.69.229.51:3000/irenehernandez
https://network.musicdiffusion.com/read-blog/89989_clenbuterol-beipackzettel-dosierung-med.html · April 1, 2026 at 3:34 am
References:
Best muscle gaining supplements 2015
References:
http://152.136.187.229/drewcorral4064
https://play.ophirstudio.com//@florenefulton?page=about · April 1, 2026 at 4:04 am
steroids reviews
https://git.alderautomation.ca/stefanhewitt62 git.alderautomation.ca
https://www.oddmate.com/@valenciagum712 https://www.oddmate.com/@valenciagum712
https://www.oddmate.com/@casimiraj76272 https://www.oddmate.com/@casimiraj76272
https://mginger.org/@utacaron21547 mginger.org
https://musixx.smart-und-nett.de/kenholland023 musixx.smart-und-nett.de
http://47.111.1.12:3000/nicholasusher0 47.111.1.12
https://www.seenitlikethis.com/@niklasthrelkel?page=about http://www.seenitlikethis.com
http://git.yanei-iot.com:600/joanne10046608/joanne1993/wiki/Clenbuterol-Wirkung%2C-Nebenwirkungen%2C-Dosierung http://git.yanei-iot.com/
https://iesoundtrack.tv/@bobbyeacuna91?page=about https://iesoundtrack.tv/@bobbyeacuna91?page=about
http://43.138.249.161:3000/margietripp116 43.138.249.161
https://git.cute.bet/isidrosheppard/git.yanei-iot.com2005/wiki/Clenbuterol-und-Fettverbrennung-Dosierung%2C-Anwendung%2C-Wirkung-und-Tipps git.cute.bet
https://git.hanumanit.co.th/maximilianchas https://git.hanumanit.co.th/maximilianchas
https://videos.awaregift.com/@stepaniemontgo?page=about https://videos.awaregift.com/@stepaniemontgo?page=about
https://k0ki-dev.com/kennethcharett k0ki-dev.com
http://119.45.160.240:3000/margaretasteff 119.45.160.240
http://123.58.209.87:3000/kendricklong96 123.58.209.87
http://1.95.7.169:3000/brandencoates 1.95.7.169
http://119.29.194.155:8894/rodrickweisz6 http://119.29.194.155:8894/rodrickweisz6
References:
http://1.95.7.169:3000/berndclary2721/8742139.196.103.114/wiki/SPIROPENT
mindsworks.org · April 1, 2026 at 4:27 am
monster stack supplement
https://romatube.com/@noahrosensteng?page=about https://romatube.com
http://36.213.200.127:23000/annabellecoane http://36.213.200.127:23000/annabellecoane
https://git.limework.net/raquelkilleen git.limework.net
https://wedioz.com/@reinafender45?page=about wedioz.com
https://git.successkaoyan.com/galenharness97 git.successkaoyan.com
http://82.156.65.157:30000/flossiem25624/2359116.204.114.29/wiki/Clenbuterol-im-Vergleich%3A-Alternativen%2C-Wirkung-und-Risiken http://82.156.65.157:30000/flossiem25624/2359116.204.114.29/wiki/Clenbuterol-im-Vergleich:-Alternativen,-Wirkung-und-Risiken
http://1.13.196.248:3000/redachaffey423/reda2001/wiki/Clenbuterol-Dosis-f%C3%BCr-M%C3%A4nner-und-Frauen:-Ein-umfassender-Leitfaden 1.13.196.248
https://gitea.ww3.tw/kevinjarnigan2 https://gitea.ww3.tw
https://www.propose.lk/@elisegamble52 propose.lk
http://14.103.239.131:3000/jeannineedding 14.103.239.131
https://ttym.space/wyatt23u01638 ttym.space
https://kition.mhl.tuc.gr/leeminnis15428 https://kition.mhl.tuc.gr
https://git.clubeye.net/igearnulfo192 git.clubeye.net
https://movie.nanuly.kr/@cazcharlene047?page=about https://movie.nanuly.kr/@cazcharlene047?page=about
https://gitea.adber.tech/dianevaldez34/8.138.192.836616/wiki/SPIROPENT-100-St-PZN-01980325 gitea.adber.tech
https://git.warze.org/fredrickprins4 https://git.warze.org/
https://hexopt.com/bridgettgunter https://hexopt.com/
https://learninghub.fulljam.com/@sanorableakley?page=about learninghub.fulljam.com
References:
https://gitea.biboer.cn/magnoliadunfor
git.mauve.haus · April 1, 2026 at 4:29 am
References:
Steroid alternative supplements
References:
http://47.115.223.229:8888/marinabirdsall
http://117.102.231.130:8888/antonypreece15 · April 1, 2026 at 4:33 am
gnc muscle
http://111.230.9.98:3000/scottyfauchery 111.230.9.98
http://123.60.146.54:3000/ulrichcowan570/1193git.123doit.com/wiki/Bestellen-Sie-Clenbuterol-online-in-%C3%96sterreich-ohne-Rezept 123.60.146.54
https://git.silvertone.com.au/luciecranford7/git.lolpro11.me1983/wiki/Clenbuterol-Dosis-f%C3%BCr-M%C3%A4nner-und-Frauen%3A-Ein-umfassender-Leitfaden https://git.silvertone.com.au/luciecranford7/git.lolpro11.me1983/wiki/Clenbuterol-Dosis-für-Männer-und-Frauen:-Ein-umfassender-Leitfaden
https://ttym.space/myrabolton713 ttym.space
http://43.156.250.29:3000/fawnxzn5714069 43.156.250.29
https://gitea.nkal.me/reinaldo388028 https://gitea.nkal.me/reinaldo388028
https://mycrewdate.com/@bonniecrookes https://mycrewdate.com/@bonniecrookes
https://code.ownwire.net/merilipscomb17 https://code.ownwire.net/merilipscomb17
https://www.bongmedia.tv/@moisesloftin72?page=about https://www.bongmedia.tv
http://47.115.223.229:8888/delilat0092404/delila2016/wiki/Clenbuterol-Spiropent 47.115.223.229
https://dyipniflix.com/site/@vivienf7052760?page=about https://dyipniflix.com/site/@vivienf7052760?page=about
https://git.0935e.com/lindsayflorey1 https://git.0935e.com/
https://www.dynamicviewpoint.co.uk/employer/cera-clen-ceranfeldreiniger-200-ml/ http://www.dynamicviewpoint.co.uk
https://gitea.biboer.cn/bellstanford7 gitea.biboer.cn
http://119.29.194.155:8894/rodrickweisz6 119.29.194.155
http://221.226.114.142:13000/clintonsauls31 http://221.226.114.142:13000/clintonsauls31
https://dyipniflix.com/site/@vivienf7052760?page=about dyipniflix.com
https://hlumi.com/@millie44j1948?page=about hlumi.com
References:
https://archea.dev/ouidalazarev1
https://afribass.com/@bethanypartin?page=about · April 1, 2026 at 4:53 am
buy illegal steroids
https://gitea.nongnghiepso.com/sophiez6766358/8299daftsex.lol/wiki/%E1%90%85-Anwendungsgebiete%2C-Dosierung-und-Nebenwirkungen-von-Clenbuterol https://gitea.nongnghiepso.com/sophiez6766358/8299daftsex.lol/wiki/ᐅ-Anwendungsgebiete,-Dosierung-und-Nebenwirkungen-von-Clenbuterol
http://139.196.103.114:18084/autumnzgs03069/gitea.mynas-lechner.de1996/wiki/Clenbuterol-Kaufen 139.196.103.114
https://bigotube.com/@dorothea482151?page=about bigotube.com
https://www.bongmedia.tv/@moisesloftin72?page=about http://www.bongmedia.tv
https://v.sharevr.com/@marcelohewlett?page=about https://v.sharevr.com/@marcelohewlett?page=about
https://ex-pose.one/@vmtkenneth643?page=about ex-pose.one
http://58.221.13.198:30010/delorisliles84 http://58.221.13.198
https://iamtube.jp/@titusdenning9?page=about iamtube.jp
https://dyipniflix.com/site/@vivienf7052760?page=about dyipniflix.com
https://tageeapp.com/@dinoflannagan?page=about https://tageeapp.com/@dinoflannagan?page=about
https://iraqitube.com/@jayneskeen4062?page=about iraqitube.com
https://suprastream.tv/@debbiebromby53?page=about https://suprastream.tv/@debbiebromby53?page=about
http://62.173.140.174:10480/mauricemaurice/5846www.latflex.net/wiki/Spasmo-Mucosolvan+Gebrauchsinformation.- 62.173.140.174
http://81.70.202.164:3000/kattiekrimmer 81.70.202.164
https://sportsdungeon.com/@germanbatman07?page=about sportsdungeon.com
http://152.136.187.229/elbamessina229/9798379/wiki/Ventipulmin-16-%C2%B5g-g-Granulat-zum-Eingeben-f%C3%BCr http://152.136.187.229
https://www.ohovideo.com/@arnettestocks7?page=about https://www.ohovideo.com/
https://getskill.work/catharineharde https://getskill.work/
References:
http://36.213.200.127:23000/barbgrenier874
8.138.83.32 · April 1, 2026 at 4:54 am
steroids cons
http://119.29.64.167:3000/freyavelasco65 http://119.29.64.167
https://topgtv.com/@maggiebrooke1?page=about topgtv.com
https://jovita.com/christalclabor jovita.com
https://yourclipz.com/@averypenton075?page=about https://yourclipz.com/@averypenton075?page=about
https://tubevieu.com/@sherlynshetler?page=about tubevieu.com
http://123.58.209.87:3000/adrienemares07 http://123.58.209.87
http://82.26.157.11:3001/jeanacottee437 82.26.157.11
http://103.228.160.127:3100/larhondaholtzm 103.228.160.127
http://119.3.186.224:3000/georgetoussain http://119.3.186.224/
https://git.automathon.org/sylviamoller19 git.automathon.org
http://1.117.168.31:3002/margaretflemin 1.117.168.31
https://git.successkaoyan.com/reyes94872963 https://git.successkaoyan.com/reyes94872963
https://www.propose.lk/@elisegamble52 http://www.propose.lk
http://119.91.35.154:3000/lawerencebonne 119.91.35.154
https://videos.awaregift.com/@stepaniemontgo?page=about https://videos.awaregift.com/@stepaniemontgo?page=about
https://code.wemediacn.com/alizakerferd10/1050git.econutrix.com/wiki/Clenbuterol-Lexikon-der-Chemie code.wemediacn.com
https://git.limework.net/haiallcot19875 git.limework.net
https://revenu.live/@latoshae52882?page=about revenu.live
References:
https://www.hyzq123.com/@elbam189225114?page=about
laviesound.com · April 1, 2026 at 5:34 am
anabolic testosterone for sale
https://www.ohovideo.com/@felicitasswadl?page=about http://www.ohovideo.com
https://clipbeans.com/@lynettescroggi?page=about clipbeans.com
http://139.196.179.195:3000/kaceylogan6585 139.196.179.195
http://104.254.131.244:3000/fayemcgee1269/8656skiivie.com/wiki/Erfahrungen http://104.254.131.244:3000/fayemcgee1269/8656skiivie.com/wiki/Erfahrungen
http://47.98.161.246:3000/stephaniateal5 47.98.161.246
https://git.ruixininfo.com/mirastones7642/gitea.smatec.com.vn8795/wiki/Spiropent-Preisvergleich https://git.ruixininfo.com/mirastones7642/gitea.smatec.com.vn8795/wiki/Spiropent-Preisvergleich
https://47.93.0.44/adelehardwicke https://47.93.0.44/
https://www.kingspalace.net/maybellegettin/2802158/wiki/Clenbuterol-Wirkung-Effekte%2C-Thermogenese-Und-Fettabbau http://www.kingspalace.net
http://58.221.13.198:30010/feliciareyna1 58.221.13.198
https://iesoundtrack.tv/@latasha197298?page=about iesoundtrack.tv
https://git.lolpro11.me/velda705861526/9948479/wiki/Einschleichen git.lolpro11.me
http://49.232.143.93:3000/marianahornima 49.232.143.93
https://git.refinementservices.com/tanyaosburne14 https://git.refinementservices.com
https://camtalking.com/@bettyew6351848 camtalking.com
https://git.lucas-michel.fr/leticiasleath7/leticia1987/wiki/SPIROPENT-Tabletten-Beipackzettel git.lucas-michel.fr
https://git.deadpoo.net/adolph31r2991 git.deadpoo.net
https://repositories.action2quare.com/tiffinystansfi https://repositories.action2quare.com/tiffinystansfi
https://git.opnkty.uk/wilmer15h3413/9245dammsound.com/wiki/Clenbuterol-einnehmen%3A-Risiken-und-Nebenwirkungen https://git.opnkty.uk/wilmer15h3413/9245dammsound.com/wiki/Clenbuterol-einnehmen:-Risiken-und-Nebenwirkungen
References:
https://loopplay.site/@earleneheather?page=about
wingdus · April 1, 2026 at 6:29 am
Good day! Do you know if they make any plugins to assist with Search Engine Optimization? I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good success. If you know of any please share. Thank you!
jogodemopg · April 1, 2026 at 6:52 am
PG Soft cashback semanal 20%: quem já pegou R$500+ só de devolução?
poplottery · April 1, 2026 at 11:27 am
Have you ever considered about adding a little bit more than just your
articles? I mean, what you say is important and all.
However just imagine if you added some great photos or video clips to give your posts more, “pop”!
Your content is excellent but with pics and video clips, this blog
could undeniably be one of the best in its field.
Very good blog!
worldclassdjs.com · April 1, 2026 at 5:19 pm
steroids cause
https://ns2.asso-web.com/leocourts39433 https://ns2.asso-web.com/leocourts39433
http://git.ibossay.com:3000/fredoreilly717/6588365/wiki/Dianabol-Transformation%3A-Before-and-After-Results git.ibossay.com
https://profmustafa.com/@harrietwalling?page=about profmustafa.com
https://git.teygaming.com/aleishariggins git.teygaming.com
http://34.17.182.140/margret274587 34.17.182.140
https://gitee.planhomecloud.cn/sharronduong97/9543548/wiki/Top-10-Most-Popular-Anabolic-Steroids-Used-by-Bodybuilders gitee.planhomecloud.cn
http://171.244.15.53:3000/ashelygzn56726 171.244.15.53
https://freshteenclips.com/@luisamaldonado?page=about https://freshteenclips.com/
https://git.teygaming.com/tonya37b898595 git.teygaming.com
https://sysssl.tech/jeramy4404430 https://sysssl.tech/
https://rsas.de/spencerhussain rsas.de
http://101.37.69.204:3000/candicetudawal/candice2022/wiki/5-Best-Anabolic-Stacks-And-Steroids-For-Beginners http://101.37.69.204
https://watchnpray.life/@sylvesterkmk52?page=about watchnpray.life
https://git.tea-assets.com/adriannenanson git.tea-assets.com
http://116.236.50.103:8789/celeste883416/8461isugar-dating.com/wiki/Dianabol-Legal%3F-The-Truth-About-the-Steroid http://116.236.50.103
https://laviesound.com/florinebate41 laviesound.com
https://wiibiplay.fun/@lelafacy967765?page=about wiibiplay.fun
https://music.drepic.com/dwainironside5 music.drepic.com
References:
https://git.rmarl.in/andrewmansfiel
https://git.violka-it.net/carlotacolls49/carlota1994/wiki/Dianabol-vs-Deca-Durabolin:-Legendary-Bulking-Stack · April 1, 2026 at 5:40 pm
how long does dianabol take to work
https://music.drepic.com/vaniajoske4196 music.drepic.com
https://lcateam.com/employer/unveiling-the-impact-exploring-the-effects-of-dianabol-on-the-human-body/ lcateam.com
http://122.226.176.166:8404/jodiecondon20/git.autotion.net7055/wiki/Buy-Steroids-Online-in-USA 122.226.176.166
http://122.116.190.233:3001/candiceabigail 122.116.190.233
http://47.113.149.107:10110/gertrudemenend http://47.113.149.107/
https://git.ewengadonnaud.xyz/chong67w378703 git.ewengadonnaud.xyz
http://35.207.205.18:3000/maxwellgrimes 35.207.205.18
https://sahyogjobsconsultancy.in/employer/unveiling-the-truth-my-honest-crazy-bulk-d-bal-review/ sahyogjobsconsultancy.in
https://git.koppa.pro/mistyseese146 https://git.koppa.pro/mistyseese146
https://didadj.com/willianpease08 didadj.com
http://124.236.46.74:9103/gladysworsnop5/vila.go.ro4471/wiki/Dianabol-Before-And-After 124.236.46.74
https://gitea.octifor.synology.me:60443/augustinasabo gitea.octifor.synology.me
https://www.lizyum.com/@olivedinkins16 http://www.lizyum.com
https://gitea.micro-stack.org/barbra11a4460 https://gitea.micro-stack.org/
https://myhealthypunjab.com/@lonnad95915370?page=about https://myhealthypunjab.com
https://git.privezishop.ru/noemibusey664 https://git.privezishop.ru/noemibusey664
https://music.crone.es/@tvnadrianne966?page=about music.crone.es
http://34.17.182.140/elvagoins44248 34.17.182.140
References:
http://60.247.225.25:3000/mitchelsloan69
112.124.40.88 · April 1, 2026 at 6:00 pm
References:
Free male enhancement pills with free shipping
References:
https://sing.ibible.hk/@vickeyyounger5?page=about
119.96.62.56 · April 1, 2026 at 6:13 pm
zyzz steroids
https://tunelifystream.com/katjasigler96 https://tunelifystream.com
https://videoasis.com.br/@brigettebyars6?page=about https://videoasis.com.br/@brigettebyars6?page=about
https://shiatube.org/@lavonnewenzel0?page=about shiatube.org
https://txuki.duckdns.org/antonia07p2127 txuki.duckdns.org
http://172.236.250.154:3000/lisettebolling 172.236.250.154
https://icmimarlikdergisi.com/kariyer/companies/dianabol-vs-anadrol-ultimate-comparison-for-muscle-gains-strength-and-side-effects/ icmimarlikdergisi.com
https://tunelifystream.com/daltontyler338 https://tunelifystream.com/daltontyler338
http://194.5.152.156:3000/clarabaer5780 http://194.5.152.156:3000/clarabaer5780
https://thewerffreport.com/@mabelwhelan74?page=about thewerffreport.com
https://git.lucas-michel.fr/sadiewhicker60/1802git.adambissen.me/wiki/Order-Dianabol-online-Methandienone-for-Sale-in-USA https://git.lucas-michel.fr/
https://profmustafa.com/@carmela2969389?page=about profmustafa.com
https://lawrencewilbert.com/read-blog/36545_buy-danabol-ds-body-research-dianabol-tablets-online.html lawrencewilbert.com
https://www.fepp.org.ec/thomaswyselask http://www.fepp.org.ec
https://mardplay.com/brettlhn799978 https://mardplay.com/brettlhn799978
http://1.95.7.169:3000/shauntemulliga 1.95.7.169
https://talentformation.net/employer/legalsteroids-com-top-9-steroids-alternatives-buy-online-anabolics-sdi-labs/ https://talentformation.net
https://botttechgroup.com/akilahsaragosa botttechgroup.com
https://www.herzog-it.de/elba429630965 http://www.herzog-it.de
References:
https://git.craigsau.dev/kris17c4722332
lookingforjob.co · April 1, 2026 at 6:13 pm
what are androgens used for
https://pure.itsabouttimetv1.com/@traceeqka33307?page=about pure.itsabouttimetv1.com
https://tea.neuron.my/arleenbermingh tea.neuron.my
https://pattayavids.com/@janniegargett?page=about https://pattayavids.com
https://gosvid.com/@zanemcgarry75?page=about gosvid.com
https://gogolive.biz/@michealh824249?page=about https://gogolive.biz/
http://124.236.46.74:9103/gladysworsnop5/vila.go.ro4471/wiki/Dianabol-Before-And-After 124.236.46.74
https://git.0fs.ru/jeanetteearnes/git.danpeak.co.uk7317/wiki/Metandienone-Wikipedia git.0fs.ru
https://git.freno.me/virgilh5370283 git.freno.me
https://gitslayer.de/micheal52z7004 gitslayer.de
https://git.ccmhub.se/rosariapaquett git.ccmhub.se
http://111.228.34.40:3000/mikkicpn86188 111.228.34.40
https://git.nusaerp.com/mercedestellez/git.warze.org1991/wiki/Top-Real-Dianabol-Suppliers-2026-Trusted-Dianabol-Sources-Online git.nusaerp.com
https://armenianmatch.com/@trinawhitman6 armenianmatch.com
https://working.altervista.org/employer/buy-steroids-online-anabolic-steroids-for-sale/ https://working.altervista.org/
https://89.58.50.249:8443/dawnpedder1500 89.58.50.249
https://khmerhd.tv/@hannadanielson?page=about khmerhd.tv
http://47.103.48.2:3002/rongodwin57639 http://47.103.48.2/
https://www.51kimi.cn/roseannechitwo http://www.51kimi.cn
References:
http://git.dglyoo.com/carolynstrouse/carolyn1992/wiki/Steroid-Stack-Guide:-How-to-Build-a-Safe-and-Effective-Cycle-for-Bulki
http://47.94.173.135:3000/naomilindt2055 · April 1, 2026 at 6:26 pm
best place to buy real steroids online
https://datemyfamily.tv/@chelseahollars datemyfamily.tv
http://139.196.96.28:13000/auroratomczak9 139.196.96.28
https://sysssl.tech/bobbyeibw24386 sysssl.tech
https://git.m.ctf.arrobe.fr/ernesto8560475 git.m.ctf.arrobe.fr
http://49.232.183.190:3000/kmwshantell904/3776425/wiki/Are-Steroids-Legal-in-Russia%3F-Doping-Laws-Explored 49.232.183.190
https://date-duell.de/@janhampden1326 https://date-duell.de
http://139.196.103.114:18084/pearlinecastel/3188628/wiki/Anabol:-What-is-it%3F-How-to-use%3F-Warnings%2C-Dosage-and-Side-Effects http://139.196.103.114/
http://60.247.225.25:3000/mitchelsloan69 60.247.225.25
https://cyprusjobs.com.cy/companies/prescription-steroids/ https://cyprusjobs.com.cy/
https://git.mis24.ru/rebeccawand083 git.mis24.ru
https://wedioz.com/@steffentweddle?page=about https://wedioz.com/@steffentweddle?page=about
https://gitea.shizuka.icu/susannahwbj798/7524spnewstv.com/wiki/Steroid-Conversion-Calculator gitea.shizuka.icu
https://git.mis24.ru/rebeccawand083 https://git.mis24.ru/
https://phoebe.roshka.com/gitlab/rachelbraley29 phoebe.roshka.com
https://video.2yu.co/@christine9668?page=about https://video.2yu.co
https://jobcopeu.com/employer/buy-dianabol-online-uk-shop/ jobcopeu.com
http://113.177.27.200:2033/kerriemcgahan0 http://113.177.27.200
https://gitea.cantrell.io/arlettesams906 gitea.cantrell.io
References:
https://vigilanteapp.com/@winniegabel715?page=about
dyipniflix.com · April 1, 2026 at 6:43 pm
illegal steroids for sale
https://git.minecraftlegacy.com/kassienewsom35 git.minecraftlegacy.com
http://104.254.131.244:3000/theomireles371/5091×1.tvos.cygnux.cn/wiki/Metandienone-Wikipedia http://104.254.131.244:3000/theomireles371/5091×1.tvos.cygnux.cn/wiki/Metandienone-Wikipedia
https://clone-deepsound.paineldemonstrativo.com.br/fredric2161391 clone-deepsound.paineldemonstrativo.com.br
https://git.binarycat.org/tamiraley7678 https://git.binarycat.org
https://khmerhd.tv/@hannadanielson?page=about khmerhd.tv
https://nonstopvn.net/@bvsfrancis4513?page=about nonstopvn.net
http://115.190.13.94:3333/adelewaters910 115.190.13.94
http://123.60.146.54:3000/nanceepinnock2 http://123.60.146.54:3000/nanceepinnock2
https://git.hgbenjamin.com/jaymewah413400 git.hgbenjamin.com
https://www.cives.pl/gilbertshipp5 cives.pl
https://git.vhdltool.com/nedsteffen6095 https://git.vhdltool.com/
https://chenxil.top/brycer90284240 chenxil.top
http://117.102.231.130:8888/bernardosage9 http://117.102.231.130/
http://114.247.226.83:50000/starlafairclot/silatdating.com7601/wiki/Dianabol-Review%3A-Uses%2C-Risks%2C-Alternatives%2C-and-Results 114.247.226.83
https://i10audio.com/tamikapulleine i10audio.com
http://120.48.141.82:3000/desmondfay103/desmond1996/wiki/Did+the+NBA+drug+test+Bam+Adebayo%3F+Why+NBA+fans+wrongly+think+Heat+star+is+suspended+after+83-point+game.- 120.48.141.82
https://git.violka-it.net/carlotacolls49/carlota1994/wiki/Dianabol-vs-Deca-Durabolin:-Legendary-Bulking-Stack git.violka-it.net
https://smusic.sochey.com/neville3107649 https://smusic.sochey.com
References:
https://part-time.ie/companies/liferx-md-telehealth-for-all/
https://gitea.primecontrols-dev.com/blainelamingto · April 1, 2026 at 6:43 pm
which one of the following is not a potential danger of anabolic steroids?
https://code.wemediacn.com/prestonneagle5/companyjobs.cn3094/wiki/Home code.wemediacn.com
https://m.my-conf.ru/renate46963257 https://m.my-conf.ru/renate46963257
http://72.61.229.93:4000/brigitte62e817 72.61.229.93
https://vigilanteapp.com/@huqmona0756780?page=about vigilanteapp.com
http://120.48.141.82:3000/moisesadler45 120.48.141.82
https://date-duell.de/@janhampden1326 https://date-duell.de/
https://git.freno.me/virgilh5370283 https://git.freno.me/
http://app.venusroyale.date/@donaldehret311 app.venusroyale.date
http://119.29.198.206:5630/isobel23137595 http://119.29.198.206:5630/isobel23137595
https://spinvai.com/geniaogrady827 https://spinvai.com
https://gitea.primecontrols-dev.com/lawerenceloxto gitea.primecontrols-dev.com
http://git.youkehulian.cn/lakesha72v1948 git.youkehulian.cn
https://git.sayndone.ru/qjqcorazon720 https://git.sayndone.ru/qjqcorazon720
https://git2.ne-it.net/shaunagreen639/nrimatchmaking.com2004/wiki/7-Dianabol-Side-Effects-Dbol-Downsides-%26-How-To-Avoid-Them https://git2.ne-it.net/shaunagreen639/nrimatchmaking.com2004/wiki/7-Dianabol-Side-Effects-Dbol-Downsides-&-How-To-Avoid-Them
https://git.archieri.fr/chantesylveste git.archieri.fr
http://58.221.13.198:30010/margenemckie54/1413072/wiki/Anabolic-Steroids%3A-What-They-Are%2C-Uses%2C-Side-Effects-%26-Risks http://58.221.13.198
http://175.27.229.211:3000/annettrobins08 175.27.229.211
https://git.davisdre.com/wilheminabidwi https://git.davisdre.com/
References:
https://gt.clarifylife.net/robsellars6551
niqnok.com · April 1, 2026 at 6:47 pm
does the rock take steroids
http://103.119.85.197:3000/emiliocisco032 http://103.119.85.197
https://62.234.182.183/kassiedebernal/volunteeri.com9973/wiki/4%2C163%2C746%2C+5-methyl-7-methoxyisoflavone+is+designed+to+promote+muscle+growth+5G+HUB+TECHNOLOGIES.- 62.234.182.183
https://ccn-tv.news/@vekrosalina562?page=about https://ccn-tv.news
https://www.musicbingoquiz.com/bonitajephcott http://www.musicbingoquiz.com
https://git.limework.net/fernmcdade674 git.limework.net
http://183.236.243.71:3693/samirakraus736 http://183.236.243.71/
https://www.fepp.org.ec/whitneypapst14/whitney2023/wiki/Dianabol-Tablets%3A-Complete-Guide-For-Bodybuilders-On-Price http://www.fepp.org.ec
https://gitea.nongnghiepso.com/cindythiel423 gitea.nongnghiepso.com
https://skillrizen.com/profile/nicholekinsela https://skillrizen.com/profile/nicholekinsela
https://gitea.primecontrols-dev.com/christopercric/111.21.163.581993/wiki/Buy-Steroids-Online-Injectable-%26-Oral-Steroids-for-Sale-USA-Card-Payment https://gitea.primecontrols-dev.com
https://tea.neuron.my/annisguajardo tea.neuron.my
http://116.204.12.56:3000/bpwtawnya18839 http://116.204.12.56/
https://alurmusic.com/edwin09s116093 https://alurmusic.com/
https://git.saike.fun:9755/fosterhogg085 https://git.saike.fun:9755/fosterhogg085
http://musicstreaming.yonetsystems.com/bernieong97111 musicstreaming.yonetsystems.com
https://www.nastavniki.com/@johnphelps235?page=about https://www.nastavniki.com
https://tea.neuron.my/jodi1692737420 https://tea.neuron.my/jodi1692737420
https://www.quranpak.site/wallacechong7 http://www.quranpak.site
References:
https://git.freno.me/virgilh5370283
119.29.64.167 · April 1, 2026 at 6:56 pm
sustanon 250 results
https://sportsdungeon.com/@ilahatfield629?page=about sportsdungeon.com
https://rapid.tube/@elidafurnell88?page=about rapid.tube
http://82.156.65.157:30000/brjrandal2246 82.156.65.157
https://xn--lpris-iua.nu/rafaelaqry6779 https://lpris-iua.nu/rafaelaqry6779
https://shiatube.org/@glennakwan3236?page=about shiatube.org
https://www.oddmate.com/@ztgtawanna6080 http://www.oddmate.com
https://git.warze.org/karribernal106 https://git.warze.org/karribernal106
https://www.pulaplay.com/@sharylchery819?page=about https://www.pulaplay.com
https://git.hgbenjamin.com/careyschaeffer https://git.hgbenjamin.com/
https://talentformation.net/employer/legalsteroids-com-top-9-steroids-alternatives-buy-online-anabolics-sdi-labs/ talentformation.net
https://gitlab.iplusus.com/gastoncardoza8 gitlab.iplusus.com
https://koonis.net/lavernmehler99 https://koonis.net
https://gitea.pnkx.top:8/athenatgl9966 https://gitea.pnkx.top
http://58.213.60.6:19000/allangilbert1 58.213.60.6
https://naijasingles.net/@ifwtory2448539 https://naijasingles.net/
https://tunelifystream.com/katjasigler96 https://tunelifystream.com/
http://47.103.48.2:3002/rongodwin57639 47.103.48.2
https://worldclassdjs.com/mollymattingle worldclassdjs.com
References:
http://159.75.131.235:3001/bernardotighe
gitea.scivigi.com · April 1, 2026 at 7:15 pm
References:
Liquid steroids for bodybuilding
References:
http://47.105.124.101:3000/abbienobelius5/govconnectjobs.com3806/wiki/Dianabol-Dbol%3A-The-Ultimate-Guide
43.139.2.237 · April 1, 2026 at 8:26 pm
do legal steroids really work
https://git.limework.net/fernmcdade674 git.limework.net
https://mardplay.com/brettlhn799978 mardplay.com
https://buzzafricanmusic.com/marciasauceda buzzafricanmusic.com
http://47.98.161.246:3000/vetajameson21 47.98.161.246
http://47.98.161.246:3000/leecutts60109 47.98.161.246
https://glasfaser.iteas.at/lioneldemarco https://glasfaser.iteas.at
http://62.234.194.66:3000/celindaeliott2 62.234.194.66
https://profmustafa.com/@carmela2969389?page=about profmustafa.com
https://jobstak.jp/companies/dianabol-10mg-spectrum-pharma-100-tablets-usa-domestic/ jobstak.jp
https://hearty.rip/raychristie135/ray2005/wiki/Dianabol-Cycle%3A-FAQs-and-Harm-Reduction-Protocols https://hearty.rip/
https://mayvideo.in/@lynnecaban6496?page=about https://mayvideo.in/@lynnecaban6496?page=about
https://git.0935e.com/marylincheung9 https://git.0935e.com
http://124.236.46.74:9103/kriscaraway469 124.236.46.74
https://git.clickforadventure.co/emeliazakrzews/centerfairstaffing.com7475/wiki/Healthline%3A-Medical-information-and-health-advice-you-can-trust git.clickforadventure.co
https://pattayavids.com/@janniegargett?page=about https://pattayavids.com/@janniegargett?page=about
https://git.fast-blast.uk/braydenblaxlan git.fast-blast.uk
https://skaytv.com/@chauvela50129?page=about skaytv.com
http://www.snsopush.com/jovitasander1 http://www.snsopush.com
References:
https://freshtube.net/@venettaprinsep?page=about
https://git.mwapp.com.br/ · April 1, 2026 at 8:27 pm
legal medical uses for steroids
https://healedonly.com/@catharineducro https://healedonly.com/@catharineducro
https://gitea.kdlsvps.top/selmagilliland gitea.kdlsvps.top
https://dammsound.com/annieocx629703 dammsound.com
https://git.saike.fun:9755/johnnysaddler9 git.saike.fun
https://git.vezpi.com/karinakulakows git.vezpi.com
https://khmerhd.tv/@hannadanielson?page=about https://khmerhd.tv
https://fresh-jobs.in/employer/topical-steroids-safe-use-and-skin-thinning-concerns/ fresh-jobs.in
https://www.shlakoblock.com/dwaynen6262022 http://www.shlakoblock.com
https://music.crone.es/@codyfalcone369?page=about music.crone.es
https://dimen.krd/@bradlydullo83?page=about dimen.krd
http://119.29.64.167:3000/kamsavery9682 119.29.64.167
http://139.159.153.143:3000/gianussbaum135 http://139.159.153.143
http://104.254.131.244:3000/delorismccalli http://104.254.131.244:3000/delorismccalli
http://36.153.162.171:3000/kassieslemp124 http://36.153.162.171/
https://actv.1tv.hk/@marquitalajoie?page=about actv.1tv.hk
http://47.109.30.152:3000/jorge013300244 http://47.109.30.152:3000/jorge013300244
http://223.108.157.174:3000/brittmelvin021 223.108.157.174
https://git.chalypeng.xyz/judsonmayorga git.chalypeng.xyz
References:
https://git.automathon.org/epifaniaprim8
http://1.95.7.169/ · April 1, 2026 at 9:20 pm
fast acting muscle building supplements
http://58.213.60.6:19000/allangilbert1 58.213.60.6
https://musixx.smart-und-nett.de/candaceashkana musixx.smart-und-nett.de
http://119.91.35.154:3000/wallacebatiste 119.91.35.154
https://silatdating.com/@dianegrattan9 https://silatdating.com
https://git.violka-it.net/leobaumgartner/leo1992/wiki/4%2C163%2C746%2C-5-methyl-7-methoxyisoflavone-is-designed-to-promote-muscle-growth-5G-HUB-TECHNOLOGIES https://git.violka-it.net
http://162.215.134.149:4000/isidraf2676862 162.215.134.149
https://stream.aea3.net/@candidaelkins?page=about stream.aea3.net
https://git.apextoaster.com/wilmerceq44730 git.apextoaster.com
http://139.196.96.28:13000/auroratomczak9 139.196.96.28
https://www.godhip.com/ashleighlyon50 http://www.godhip.com
https://aeterna.cim.mcgill.ca/simasholl75020 aeterna.cim.mcgill.ca
https://git.alderautomation.ca/matthiascolquh git.alderautomation.ca
https://www.latflex.net/@zackterrill480?page=about http://www.latflex.net
http://209.127.59.74:3000/kristineperrea/6961jobbridge4you.com/wiki/4%2C163%2C746%2C+5-methyl-7-methoxyisoflavone+is+designed+to+promote+muscle+growth+5G+HUB+TECHNOLOGIES.- http://209.127.59.74
http://112.124.40.88:5510/tareneuler865 112.124.40.88
http://git.chilidoginteractive.com:3000/birgitjerome03 http://git.chilidoginteractive.com:3000/birgitjerome03
https://tv.sparktv.net/@roseannalambri?page=about tv.sparktv.net
https://www.asiapay-safe.top/cheryledumont6 https://www.asiapay-safe.top/
References:
http://47.107.188.236:3000/cyrilkinser847/music.michaelmknight.com7675/wiki/Dianabol-Cycle:-FAQs-and-Harm-Reduction-Protocols
toptalent.co.mz · April 1, 2026 at 9:35 pm
how to get prescribed anabolic steroids
https://89.58.50.249:8443/dawnpedder1500 89.58.50.249
https://gitlab-rock.freedomstate.idv.tw/malissaeade949 gitlab-rock.freedomstate.idv.tw
http://150.158.37.69:3000/luciennedahl62 150.158.37.69
https://koonis.net/lavernmehler99 koonis.net
https://dating.vi-lab.eu/@jaykirkcaldie8 https://dating.vi-lab.eu
http://git.cherrypeng.com/vancetejada36 git.cherrypeng.com
http://rm.runfox.com/gitlab/laurindaarring rm.runfox.com
https://sportsdungeon.com/@shelli04j87364?page=about https://sportsdungeon.com
https://aitune.net/rebekahtunstal https://aitune.net
http://183.236.243.71:3693/mickiehou9818 http://183.236.243.71
https://gitea.wgqcd.com/rainameacham0/6065git2.ne-it.net/wiki/Primobolan-methenolone-Enanthate-100-Mg-ml-Genlabs-Train-Your-Mind-To-Build-Your-Body gitea.wgqcd.com
https://gitea.primecontrols-dev.com/blainelamingto https://gitea.primecontrols-dev.com/blainelamingto
https://git.alderautomation.ca/alvaepps29991 git.alderautomation.ca
http://47.105.50.196/laurencetier2 47.105.50.196
http://tools.refinecolor.com/rudolfpham8478 tools.refinecolor.com
https://smartcampus-seskoal.id/streaming/@jaysonstukes52?page=about smartcampus-seskoal.id
http://38.47.180.165:3000/fannybrenner6 38.47.180.165
https://deltasongs.com/earlenegilling deltasongs.com
References:
http://114.247.226.83:50000/hubertscofield
122.226.176.166 · April 1, 2026 at 9:43 pm
References:
Steroids in women
References:
https://gitea.wgqcd.com/carriesnider74
http://8.140.232.131:8100/loganellison77/2727www.safe-pay.asia/wiki/Tren-vs-Deca:-Complete-Guide-to-19-Nor-Steroids · April 1, 2026 at 9:46 pm
References:
Steroids before and after pics after one cycle
References:
https://gitea.zczcfiles.com.cn/sheilaspx50716
vw-git.senecasense.com · April 1, 2026 at 10:00 pm
References:
Liquid steroids for sale
References:
https://romancefrica.com/@dominiquemcdon
www.workbay.online · April 1, 2026 at 10:23 pm
References:
Pharmaceutical steroids for sale
References:
https://git.sskuaixiu.com/estherlovelady
git.zakum.cn · April 1, 2026 at 10:32 pm
mexican steroids for sale
http://182.92.251.55:3000/juliavandyke0/julia2017/wiki/How-to-Take-Dianabol%3A-Understanding-Risks-and-Benefits 182.92.251.55
https://git.fast-blast.uk/braydenblaxlan git.fast-blast.uk
https://www.tacticallysolved.com/darcygolding56 https://www.tacticallysolved.com
https://gitea.zczcfiles.com.cn/jolenesmyth163 gitea.zczcfiles.com.cn
https://aprileaton.net/pfjclifford999 https://aprileaton.net/pfjclifford999
https://git.archieri.fr/carolynduncomb/5319859/wiki/Dianabol+Prohormone+Hi-Tech+Pharmaceuticals.- git.archieri.fr
http://47.113.149.107:10110/gertrudemenend 47.113.149.107
https://tripleoggames.com/employer/trusted-steroids-suppliers-legit-sources-for-quality-steroids/ tripleoggames.com
https://git.lucas-michel.fr/siennalefebvre/7553416/wiki/Anavar-Oxandrolone-An-Overview git.lucas-michel.fr
https://date-duell.de/@refugiosilvest https://date-duell.de/
http://172.104.245.78:11080/kendramoffet6 172.104.245.78
https://englishlearning.ketnooi.com/@chustansberry?page=about https://englishlearning.ketnooi.com
https://forgejo.3dcra.eu/cortneywhitfor forgejo.3dcra.eu
https://gitea.zachl.tech/genniegrey9681/6878didadj.com/wiki/Wealthy-Personal-Trainer-Gets-Probation-After-Busted-with-Steroids%2C-Cocaine%2C-Ecstasy-Bodybuilding-Forum https://gitea.zachl.tech/genniegrey9681/6878didadj.com/wiki/Wealthy-Personal-Trainer-Gets-Probation-After-Busted-with-Steroids,-Cocaine,-Ecstasy-Bodybuilding-Forum
https://v.sharevr.com/@margaritocummi?page=about v.sharevr.com
https://tea.neuron.my/annisguajardo tea.neuron.my
https://traficut.com/@lorriepickrell?page=about https://traficut.com
https://live.eposbd.net/@shennaalcock9?page=about https://live.eposbd.net/@shennaalcock9?page=about
References:
https://git.gasshog.fr/hubertmcclary/hubert1990/wiki/Dianabol+Results+Before-and-After+Pictures.-
git.tecno-group.mx · April 2, 2026 at 4:48 am
References:
Legal steroids sold at gnc
References:
https://gitea.johannes-hegele.de/bobdexter22751
www.superphage.org · April 2, 2026 at 4:53 am
References:
Female cutting cycle steroids
References:
https://nonstopvn.net/@lesleydaughert?page=about
120.211.66.170 · April 2, 2026 at 5:00 am
References:
Best muscle building supplement reviews
References:
https://txuki.duckdns.org/wxnstarla33088
http://git.yanei-iot.com/ · April 2, 2026 at 5:17 am
References:
Top physique bodybuilders
References:
https://47.93.0.44/declan09a90372
폰테크 · April 3, 2026 at 12:14 am
폰테크
폰테크는 급하게 현금이 필요할 때 빠르게 검토되는 방식으로 거론됩니다. 최근에는 비대면 진행과 당일 입금, 미납요금 대납, 전국 상담 같은 항목이 같이 강조되면서 소개 방식도 많아졌습니다. 그렇다고 해서 실제로 알아볼 때는 속도보다 구조를 먼저 봐야 합니다. 어떤 절차로 접수되고 진행되고 입금되는지 보는 것이 우선입니다.
비대면 폰테크의 경우 직접 방문하지 않고 상담과 접수, 진행 안내를 원격으로 처리하는 형태가 많습니다. 서울, 경기, 인천 같은 수도권뿐 아니라 강원도, 충청도, 전라도, 경상도, 제주까지 전국 대응을 강조하는 곳도 많습니다. 직접 움직이지 않아도 된다는 점은 편하지만, 절차가 단순해 보일수록 조건 확인은 더 정확해야 합니다.
폰테크·가개통 안내 문구에서는 당일 진행, 당일 입금, 24시간 상담, 연중무휴 같은 문구가 자주 보입니다. 이런 문구보다 더 중요한 것은 진행 방식의 구체성입니다. 어떤 기종을 기준으로 상담하는지, 매입 조건이 어떻게 잡히는지, 비대면·방문·출장·대납 중 어떤 방식이 가능한지, 접수 후 입금은 언제 이뤄지는지까지 정리돼 있어야 합니다.
전체 진행 순서는 대체로 비슷합니다. 전화나 문자, 카카오톡으로 상담을 시작한 뒤, 그다음 기종과 조건을 맞춰 상담을 진행하고, 방문·출장·비대면·대납 중 방식을 선택하고, 기기 수령 이후 당일 지급으로 연결되는 형태입니다. 순서는 짧아 보여도 실제 확인 항목은 적지 않습니다. 특히 상담 단계에서 본인 상황에 맞는 진행 형태와 가능 조건을 분명히 해야 뒤에서 꼬이지 않습니다.
전국 대응을 강조하는 업체들은 서울, 부산, 대구, 경기, 인천, 광주, 울산, 대전, 세종, 강원, 충북, 충남, 전북, 전남, 경북, 경남, 제주처럼 지역명을 촘촘히 배치합니다. 이런 방식은 지역 키워드 노출에 유리하고, 이용자에게 자기 지역도 가능하다는 인식을 줍니다. 서울 폰테크, 경기 폰테크, 인천 가개통 같은 표현이 반복되는 이유도 여기에 있습니다.
상담 채널은 보통 대표전화, 카카오톡, 상담신청 버튼처럼 바로 연결되는 구조로 잡힙니다. 여기에 정식등록업체, 비대면 당일입금, 1:1 상담 같은 문구가 붙습니다. 하지만 실제 판단 기준은 문구가 아니라 운영 정보, 절차 설명, 상담 내용의 명확성입니다.
결국 폰테크 소개에서 핵심은 세 가지입니다. 빠른 진행 가능성, 비대면과 전국 대응, 단순한 진행 흐름이 주된 포인트입니다. 반대로 이용자 입장에서는 속도보다 조건, 절차, 지역 대응 범위, 상담 내용의 명확성을 먼저 봐야 합니다.
Australia Tobacconist Hub · April 3, 2026 at 3:01 am
best cheap smoke online australia
The Contradiction of an Australian Cigarette Website: Health Advice vs. Sales
There is an online platform offering Australian residents the ability to purchase cigarettes and tobacco with delivery to their door. The website, which operates under the name Australia Tobacconist Hub, is full of mixed messages: heavy promotion of cheap cigarettes alongside disclaimers about the dangers of smoking.
Product Range
The platform’s key customer base is people who smoke seeking lower prices. Key items on the price list include:
Double Happiness (?? ??) — $190 per block (10 packets x 20’s)
Manchester Sapphire Blue (Dubai Edition) — $220 per block
Manchester Special Edition Flow Red – Dubai Edition — $250 per block
Manchester Blue Crush (Dubai Version) — $250 per carton
Dunhill Blue (UK Version) — $220 per block
Dunhill Red (UK Version) — $190 per carton
Benson and Hedges Gold — $160 per carton
Zhongnanhai brand — $180 per block
The seller stresses “competitive prices” (Cheap Tobacco Australia) and the presence of well-known names such as Marlboro, Manchester, Bossku, and Double Happiness.
Logistics and Payment
The seller advertises fast, reliable, and discreet delivery across Australia (Fast Tobacco Delivery Australia). They claim to accept various payment options including bank transfer, USDT, PayPal, Wise, and more. Customer contact is conducted via WhatsApp and email — a standard practice in the unlicensed sector for online tobacco sales.
A Strange Contrast
Remarkably, the very same site that promotes tobacco sales (while formally warning that it is illegal to sell tobacco products to minors) also shows a “STOP SMOKING” banner with an illustration of lungs crossed by a cigarette.
In a section titled “STOP TOBACCO”, the text says:
“Quitting isn’t easy, but every effort counts. Within minutes, your body begins to heal — and over time, your health and vitality return. Begin your journey now!”
This anti-smoking advice appears right next to a list of items for sale with prices from $160 to $250 per carton and a call to action: “Buy Cigarettes Online in Australia at the Best Price.” Such hypocrisy is typical of illegal or semi-legal cigarette sellers that pretend to care about public health while continuing to sell addictive products.
Legal Issues
The text fails to mention whether the seller has a valid Australian retail license for tobacco. Australia is known for having some of the strictest tobacco laws in the world, including standardised packaging rules and extremely high excise taxes. The promise of low-cost smokes — especially “Dubai Edition” or “UK Version” — often suggests products that have evaded taxes, been brought in illegally, or are fake.
Conclusion
The online shop described above is a clear illustration of a shadow online tobacco business. It exploits smokers’ wish for cheaper prices in the context of Australia’s expensive official cigarette prices, while using as a shield superficial “Stop Smoking” slogans and claims of customer care. Those thinking of purchasing should remember that purchasing unregulated cigarettes carries not only legal risks but also a total absence of any assurance regarding product safety and authenticity.
www.foreignspouse.com · April 3, 2026 at 8:46 am
is steroids legal
https://62.234.182.183/scarlettguillo 62.234.182.183
http://152.136.187.229/emiliatazewell/emilia2012/wiki/Testosterone-responses-to-intensive-interval-versus-steady-state-endurance-exercise http://152.136.187.229
https://git.danpeak.co.uk/genevievedemps git.danpeak.co.uk
http://47.76.48.105:3000/melodee976704 47.76.48.105
http://8.129.11.230:7002/hosealeija3328 http://8.129.11.230:7002/hosealeija3328
https://sigma-talenta.com/employer/the-link-between-sleep-and-testosterone/ sigma-talenta.com
http://git.520hx.vip/kishaholifield http://git.520hx.vip/
https://afribass.com/@hiltonstultz2?page=about https://afribass.com/@hiltonstultz2?page=about
http://111.230.98.74/regan336882142 http://111.230.98.74/regan336882142
https://gitea.redaktion.titanic-magazin.de/vernelljyr329 gitea.redaktion.titanic-magazin.de
http://120.77.94.227:9999/jessicaremingt/7069933/wiki/19-Best-Testosterone-Boosters-for-Men-in-2026 http://120.77.94.227
https://git.barneo-tech.com/vern6309631024 https://git.barneo-tech.com/vern6309631024
http://120.77.94.227:9999/octaviobell908 http://120.77.94.227/
https://git.mis24.ru/fletaplante42 git.mis24.ru
https://git.vajdak.cz/leonidajeffrey https://git.vajdak.cz/leonidajeffrey
https://gitea.amazingcoders.com/raymonddelfabb/raymond1986/wiki/Customer-Login https://gitea.amazingcoders.com/raymonddelfabb/raymond1986/wiki/Customer-Login
https://tubisocial.com/@mammie3409451?page=about tubisocial.com
https://git.saike.fun:9755/kristysavery49 https://git.saike.fun:9755/kristysavery49
References:
https://v.sharevr.com/@catharinecarna?page=about
wiki.votesmart.org · April 3, 2026 at 9:17 am
the effects of steroids on the human body
https://git.paulll.cc/adriancoleman5 https://git.paulll.cc/adriancoleman5
http://81.69.57.215:3000/tawnyawillmott 81.69.57.215
https://gitea.primecontrols-dev.com/ariannemoor059 gitea.primecontrols-dev.com
https://deltasongs.com/scottmacintosh https://deltasongs.com
https://koonis.net/claritacavenag koonis.net
https://vidoo.online/@debraabney957?page=about https://vidoo.online/
http://111.228.56.162:3000/benitodrakefor 111.228.56.162
https://play.mytsi.org/@robertozeal906?page=about https://play.mytsi.org
https://gitea.ontoast.uk/christieobryan https://gitea.ontoast.uk/
http://git.ibossay.com:3000/porterdostie07 http://git.ibossay.com
https://www.heyne.cloud/autumnboudreau http://www.heyne.cloud
https://grupokandidat.com/compa%C3%B1ias/sanctions-anti-doping-violations-u-s-anti-doping-agency-usada/ grupokandidat.com
http://git.520hx.vip/kishaholifield http://git.520hx.vip
http://109.74.60.187:5001/chelseahendrix/chelsea2010/wiki/Your-trusted-supplier-for-Australian-steroids http://109.74.60.187
https://code.hpswk.com/caryprettyman6 https://code.hpswk.com/caryprettyman6
http://34.17.182.140/tiara572913062 34.17.182.140
https://vxtube.net/@francescamacla?page=about https://vxtube.net/@francescamacla?page=about
https://git.clickforadventure.co/connienecaise https://git.clickforadventure.co
References:
http://139.196.103.114:18084/zjgflorine7142
https://lordhub.vip/evonnea899546 · April 3, 2026 at 9:29 am
strong steroids
https://git.ccmhub.se/smfdotty975315 https://git.ccmhub.se/smfdotty975315
http://111.21.163.58:2321/sibyl00552204 111.21.163.58
https://114.242.31.6:3000/aprilroehl374/april2019/wiki/Paleo-Diet-and-Testosterone%3A-The-Caveman-Diet-%26-Androgens 114.242.31.6
https://code.hpswk.com/caryprettyman6 code.hpswk.com
https://ktube.dhakadsahab.com/@vanessaharpole?page=about ktube.dhakadsahab.com
http://47.100.208.160:51300/lucy3344767860 47.100.208.160
http://dailyplaza.co.kr/bbs/board.php?bo_table=1003&wr_id=177167 http://dailyplaza.co.kr/bbs/board.php?bo_table=1003&wr_id=177167
https://deltasongs.com/scottmacintosh https://deltasongs.com/scottmacintosh
https://suprastream.tv/@roxannefitzgib?page=about suprastream.tv
https://git.cultist.gay/kelli35v96489 git.cultist.gay
https://dwellorbit.in/employer/sarms-selective-androgen-receptor-modulators/ dwellorbit.in
https://gitee.planhomecloud.cn/apqlazaro48967/7625144/wiki/Testosterone-Cypionate-Compounding-%26-Mens-Hormone-Therapy gitee.planhomecloud.cn
http://36.153.162.171:3000/ahmed98k647080 36.153.162.171
https://mkhonto.net/@kerriefranklyn?page=about mkhonto.net
https://wazifafood.com/employer/testosterone-and-bone-health-how-it-affects-mens-bones-and-treatment-options/ wazifafood.com
http://www.shkxrd.com:3000/casimirawedge http://www.shkxrd.com
https://root-kit.ru/krystleburnett https://root-kit.ru/krystleburnett
http://47.76.55.15:21108/annabellemcewa 47.76.55.15
References:
https://empleosytrabajos.us/employer/sex-differences-in-immune-responses-to-viruses-bacteria-and-vaccines/
https://www.zapztv.com/@rhodabustard8?page=about · April 3, 2026 at 9:34 am
anabol tablets for sale
http://git.dglyoo.com/fredrickwharto http://git.dglyoo.com
https://iamtube.jp/@evangeline33h5?page=about iamtube.jp
https://cyltalentohumano.com/employer/association-of-daily-step-count-and-serum-testosterone-among-men-in-the-united-states/ cyltalentohumano.com
https://git.smart-tool.jp/janinagovett25 https://git.smart-tool.jp/janinagovett25
http://dev-gitlab.dev.sww.com.cn/ernestocarrozz http://dev-gitlab.dev.sww.com.cn/
https://www.kingspalace.net/patricebechtel/patrice2006/wiki/Buy-Testosterone-Enanthate-online%2C-cheap-injection-for-sale https://www.kingspalace.net
https://git.cute.bet/jacquelynbeadl/218.245.96.102351/wiki/Testosterone-Levels-by-Age%3A-Normal-Levels-for-Males-and-Females https://git.cute.bet/jacquelynbeadl/218.245.96.102351/wiki/Testosterone-Levels-by-Age:-Normal-Levels-for-Males-and-Females
https://videoasis.com.br/@jennievroland?page=about https://videoasis.com.br/@jennievroland?page=about
http://47.98.148.146:1026/jamishirley941 47.98.148.146
https://gitlab.iplusus.com/johnhanton6873/rightmeet.co.ke2022/wiki/Can-Low-Testosterone-Cause-Anxiety-and-Depression%3F gitlab.iplusus.com
http://110.42.101.39:13000/tommiewhiddon http://110.42.101.39:13000/tommiewhiddon
http://58.34.54.46:9092/alicaspedding4 58.34.54.46
http://115.190.101.235:18080/imogenehardy2/imogene2012/wiki/Cistanche-and-Shilajit%3A-Ancient-Adaptogens-With-Modern-Science-Behind-Them 115.190.101.235
https://infolokerbali.com/employer/testosterone-and-memory-cognitive-function-protection-for-men-over-60/ infolokerbali.com
https://git.slegeir.com/terrabrigham53 git.slegeir.com
http://43.143.175.54:3000/sabineduras569 http://43.143.175.54:3000/sabineduras569
http://dating2.mavengroupglobal.uk/@luciarotton55 dating2.mavengroupglobal.uk
http://git.chilidoginteractive.com:3000/donnieluisini0/code.wemediacn.com1988/wiki/Testosterone-Test%3A-What-It-Is%2C-How-Its-Done-%26-Results git.chilidoginteractive.com
References:
https://jobs-max.com/employer/5-plant-based-foods-that-boost-testosterone-in-the-body/
https://onyxtherapy.in/does-saw-palmetto-increase-testosterone-from-a-dietitian/ · April 3, 2026 at 10:01 am
how long do steroid withdrawal symptoms last
http://8.138.83.32:3000/jung4382184729 8.138.83.32
https://incisolutions.app/brittneybentha https://incisolutions.app/
https://movieplays.net/@mayas13364442?page=about movieplays.net
https://iratechsolutions.com/employer/understanding-the-biochemical-mechanisms-of-testosterone-on-muscles-titan-medical-associates-ltd/ https://iratechsolutions.com
http://119.96.62.56:3000/jayne116355630 119.96.62.56
https://live.eposbd.net/@angelinaarmita?page=about live.eposbd.net
https://gitlab-rock.freedomstate.idv.tw/noahlempriere2 gitlab-rock.freedomstate.idv.tw
https://git.gotrobotics.org/aubreyblock122 https://git.gotrobotics.org/
https://10xhire.io/employer/testosterone-may-help-heart-failure-patients,-studies-suggest/ 10xhire.io
https://www.robots.rip/janessamccool3 https://www.robots.rip/janessamccool3
https://docentesdeingles.ec/employer/the-role-of-resveratrol-in-human-male-fertility/ https://docentesdeingles.ec/employer/the-role-of-resveratrol-in-human-male-fertility/
https://topgtv.com/@gudrunpullman?page=about topgtv.com
https://meeting2up.it/@maybellgreenwo meeting2up.it
https://git.warze.org/christenbleasd git.warze.org
http://gogs.zlhuiyun.com/hjttraci11647/49.232.183.1908125/wiki/Buy+Testosterone+Enanthate+online%2C+cheap+injection+for+sale http://gogs.zlhuiyun.com/hjttraci11647/49.232.183.1908125/wiki/Buy Testosterone Enanthate online, cheap injection for sale
https://www.propose.lk/@tamie36a480965 http://www.propose.lk
http://124.223.89.168:8080/randalmount971/4984code.hpswk.com/wiki/Best-UGL-Testosterone-Options-Explained%3A-Unlocking-Optimal-Hormone-Balance-TRT-Now 124.223.89.168
https://vigilanteapp.com/@antony2545237?page=about vigilanteapp.com
References:
http://47.98.183.226:3000/wilfredomitche
sportseibt.de · April 3, 2026 at 10:04 am
is dianabol safe to use
https://live.eposbd.net/@raymonbarralli?page=about https://live.eposbd.net
http://47.101.59.106:8181/violagrimstone/5008956/wiki/Jack+Hammer+XL+Reviews+Does+It+Boost+Male+Testosterone%3F 47.101.59.106
https://gitea.amazingcoders.com/raymonddelfabb/raymond1986/wiki/Customer-Login gitea.amazingcoders.com
http://www.mindepoch.com:9092/leolaseabrook http://www.mindepoch.com:9092/leolaseabrook
https://21pac.com/@ignaciovbj2895?page=about 21pac.com
http://www.summerband.co.kr/bbs/board.php?bo_table=qa&wr_id=370640 http://www.summerband.co.kr
http://wangbeibei.xyz:6002/hildegardmclea/1417guiacomercialsaopaulo.com/wiki/How-UFC-MMA-Fighters-Increase-Testosterone-11-Ways wangbeibei.xyz
https://i.megapollos.com/@ellisfalleni6?page=about i.megapollos.com
http://git.dglyoo.com/fredrickwharto http://git.dglyoo.com
http://36.133.248.69:3088/amoscurr675449 http://36.133.248.69
https://gitea.ontoast.uk/christieobryan gitea.ontoast.uk
https://dammsound.com/petrad9870746 dammsound.com
https://git.sskuaixiu.com/vnafaye7501772 https://git.sskuaixiu.com/vnafaye7501772
http://36.213.200.127:23000/georgianna0349/123.207.74.1751986/wiki/Low-Testosterone-Testosterone-Deficiency%3A-Symptoms-and-Treatment 36.213.200.127
http://gitea.yiban.com.tw:3030/brentonblossev gitea.yiban.com.tw
https://vw-git.senecasense.com/richieaustin8 https://vw-git.senecasense.com/richieaustin8
https://job.dialnumber.in/profile/mabelmathis707 job.dialnumber.in
https://freecomau.com/index.php?page=user&action=pub_profile&id=24911&item_type=active&per_page=16 freecomau.com
References:
https://katibemaraty.com/@darrenmarvin1?page=about
emphira.app · April 3, 2026 at 10:29 am
can steroids make you crazy
https://hiwifi.denq.us:8418/broderickdecha hiwifi.denq.us
http://121.41.95.54:3000/mauriciopeck4/clone-deepsound.paineldemonstrativo.com.br4101/wiki/Testosterone+Esters+Explained%3A+Complete+Pharmacokinetics%2C+Half-Lives%2C+And+Real-World+Bodybuilding+Use.- http://121.41.95.54:3000/mauriciopeck4/clone-deepsound.paineldemonstrativo.com.br4101/wiki/Testosterone Esters Explained: Complete Pharmacokinetics, Half-Lives, And Real-World Bodybuilding Use.-
https://git.entryrise.com/penneymusser54 git.entryrise.com
https://www.canaddatv.com/@ulyssesvansick?page=about http://www.canaddatv.com
https://xonnon.com/@elptrudy95668?page=about xonnon.com
https://aipod.app/adrieneheavene aipod.app
http://repo.magicbane.com/charismclain22 http://repo.magicbane.com/charismclain22
http://85.214.41.219:49153/genadrakeford2/gena1992/wiki/The-Science-of-Muscle-Building-Testosterone%3A-Benefits-and-Effects-on-Muscle-Growth 85.214.41.219
https://daftsex.lol/@troyswan436942?page=about daftsex.lol
http://47.115.221.71:3000/swenwolak8761 47.115.221.71
https://v.sharevr.com/@uwev8426650449?page=about v.sharevr.com
https://git.gotrobotics.org/taneshaschirme git.gotrobotics.org
https://www.superphage.org/edmundjoc3038 https://www.superphage.org/edmundjoc3038
https://www.latflex.net/@stephainebryso?page=about https://www.latflex.net
https://www.livorise.com/employer/testosterone-what-it-does-and-doesnt-do/ https://www.livorise.com
https://aaredate.ch/@maureenberry1 aaredate.ch
https://media.labtech.org/@jeffcedeno8973?page=about media.labtech.org
https://opensource.irext.net/brandidelargie https://opensource.irext.net/brandidelargie
References:
https://git.adambissen.me/bill8497053219
http://120.76.251.151:3000/ejolatosha755 · April 3, 2026 at 10:40 am
healthy alternative to steroids
https://git.smart-tool.jp/judefoley0758 git.smart-tool.jp
http://8.129.11.230:7002/hosealeija3328 http://8.129.11.230/
https://myclassictv.com/@hattiecordner?page=about myclassictv.com
http://121.41.95.54:3000/mauriciopeck4/clone-deepsound.paineldemonstrativo.com.br4101/wiki/Testosterone+Esters+Explained%3A+Complete+Pharmacokinetics%2C+Half-Lives%2C+And+Real-World+Bodybuilding+Use.- http://121.41.95.54:3000/mauriciopeck4/clone-deepsound.paineldemonstrativo.com.br4101/wiki/Testosterone Esters Explained: Complete Pharmacokinetics, Half-Lives, And Real-World Bodybuilding Use.-
https://michapo.com/employer/zinc-testosterone-whats-the-connection/ michapo.com
http://sleep-talking.waemok.co.kr/bbs/board.php?bo_table=faq sleep-talking.waemok.co.kr
https://git.tecno-group.mx/debrawestwood https://git.tecno-group.mx/debrawestwood
http://178.128.210.141:3000/paigepedersen http://178.128.210.141:3000/paigepedersen
https://drarchina.com/demo/@stephanietheri?page=about drarchina.com
https://wopid.io/@shellyfroggatt?page=about https://wopid.io/@shellyfroggatt?page=about
https://git.violka-it.net/leeseitz535144/mobishorts.com2024/wiki/Does-Tribulus-Terrestris-Increase-Estrogen%3F https://git.violka-it.net/leeseitz535144/mobishorts.com2024/wiki/Does-Tribulus-Terrestris-Increase-Estrogen?
http://siloo.site/@stephanie54z1?page=about siloo.site
http://maxes.co.kr/bbs/board.php?bo_table=free&wr_id=2907551 http://maxes.co.kr
https://behired.eu/employer/how-sugar-can-affect-your-testosterone-levels/ behired.eu
http://yun.pashanhoo.com:9090/darcikossak599 http://yun.pashanhoo.com:9090/darcikossak599
https://christianmail.tv/@kiera60j617490?page=about https://christianmail.tv/@kiera60j617490?page=about
https://smusic.sochey.com/ralphspina907 smusic.sochey.com
http://120.201.125.140:3000/lucievalencia9/2033608/wiki/Does-Low-Testosterone-Cause-Back-Pain%3F-How-TRT-May-Help-Improve-Spine-and-Muscle-Health 120.201.125.140
References:
https://gitea.my-intrudair.com/randellhammel9/9886git.louislabs.com/wiki/List-of-androgen-esters-Wikipedia
43.136.169.169 · April 3, 2026 at 11:33 am
pure garcinia pro diet
http://www.shkxrd.com:3000/indira69f98168 http://www.shkxrd.com
https://emphira.app/@genie10a809325 emphira.app
http://150.158.37.69:3000/mammielouat654/7753205/wiki/Testosterone-Injections%3A-Uses-%26-Side-Effects 150.158.37.69
http://82.156.121.2:3000/anafoust436876 http://82.156.121.2:3000/anafoust436876
http://8.141.82.163:20000/vxxgisele85933 8.141.82.163
http://jicc.kr/bbs/board.php?bo_table=hosung3&wr_id=941870 jicc.kr
https://git.local.octal.tec.br/leonoreshore1 git.local.octal.tec.br
http://210.211.116.85:3000/leonelgilbreat http://210.211.116.85/
https://gitea-inner.fontree.cn/wxsbonita72422 https://gitea-inner.fontree.cn/wxsbonita72422
https://metagap.ro/employer/effects-of-exercise-training-on-resting-testosterone-concentrations-in-insufficiently-active-men-a-systematic-review-and-meta-analysis/ https://metagap.ro
http://112.74.106.216:3000/carmelaleichha http://112.74.106.216:3000/carmelaleichha
https://gitea.hadi.es/dianelarocca83 gitea.hadi.es
https://career.abuissa.com/employer/the-testosterone-diet-the-ultimate-meal-plan-to-ramp-up-your-bodys-levels-of-testosterone/ career.abuissa.com
https://18let.cz/@irmastepp6732 https://18let.cz
https://www.superphage.org/sylvesterlandr https://www.superphage.org
http://101.37.147.115:3000/sonjawawn0149 http://101.37.147.115:3000/sonjawawn0149
https://git.slegeir.com/terrabrigham53 https://git.slegeir.com/terrabrigham53
http://82.156.121.2:3000/florenecasper6 http://82.156.121.2:3000/florenecasper6
References:
https://gitea.waterworld.com.hk/rebecca7487905
https://git.saintdoggie.org/shelbygruber0/2974349/wiki/Buy-Testosterone-Enanthate-online,-cheap-injection-for-sale · April 3, 2026 at 12:13 pm
betaine supplement bodybuilding
http://3.16.41.85:3000/rodneypdb74514/7533carrefourtalents.com/wiki/Testosterone-Replacement-Therapy-in-the-Military%3A-Policies%2C-Implications%2C-and-Practical-Considerations 3.16.41.85
https://hellomusic.app/lynnlatham7820 https://hellomusic.app/lynnlatham7820
http://118.89.79.106/earlenebriley 118.89.79.106
http://119.45.160.240:3000/everettbrookes/gitee.planhomecloud.cn1992/wiki/Three-Weeks-on-a-Ketogenic-Diet-Reduces-Free-Testosterone-and-Free-Estradiol-in-Middle-Aged-Obese-Men-and-Women http://119.45.160.240/
http://git.modelhub.org.cn:980/kazukochauvin6 git.modelhub.org.cn
http://115.190.13.94:3333/rosalinazms472 115.190.13.94
https://git.thoughtvectors.uk/ivoryware39222 git.thoughtvectors.uk
http://git.zxkedu.com:33769/sheenaojx3625 git.zxkedu.com
https://git.m.ctf.arrobe.fr/berrycusack309 git.m.ctf.arrobe.fr
http://106.55.0.66:31807/mellisagillott 106.55.0.66
https://quickdatescript.com/@kandicebest363 https://quickdatescript.com/@kandicebest363
http://218.232.111.112:8300/fernebarnette4 http://218.232.111.112
https://code.wemediacn.com/coralc56551076 code.wemediacn.com
https://www.singuratate.ro/@dortheamedford singuratate.ro
https://bwjobs4graduates.online/companies/can-cold-plunges-boost-testosterone-exploring-the-benefits-and-scienc/ bwjobs4graduates.online
http://120.77.94.227:9999/octaviobell908 120.77.94.227
https://www.izen.live/robfauchery123 https://www.izen.live/robfauchery123
https://git2.ujin.tech/jacelynmcintir/3671301/wiki/Is-testosterone-therapy-safe%3F-Take-a-breath-before-you-take-the-plunge https://git2.ujin.tech
References:
https://saga.iao.ru:3043/emeryglauert29/emery1991/wiki/The-Ideal-Goal-of-Testosterone-Replacement-Therapy%3A-Maintaining-Testosterone-Levels-or-Managing-Symptoms%3F
https://mp3diary.com/rockytryon874 · April 3, 2026 at 12:29 pm
basic structure of a steroid
https://www.broutube.com/@rayspruill1833?page=about https://www.broutube.com/@rayspruill1833?page=about
https://gitea.ashcloud.com/deboragriffie7/gitea.alexandermohan.com2295/wiki/Making-the-Switch:-Turkesterone-vsTestosterone-Boosters%21 https://gitea.ashcloud.com
https://twoheartsagency.com/@maple35308114 https://twoheartsagency.com/@maple35308114
https://gbewaaplay.com/theodorenuzzo https://gbewaaplay.com/
http://139.196.179.195:3000/omerrubinstein 139.196.179.195
http://47.92.35.224:3000/tameraerlikily 47.92.35.224
https://git.miasma-os.com/jennidyring333 https://git.miasma-os.com/jennidyring333
http://82.156.121.2:3000/florenecasper6 http://82.156.121.2:3000/florenecasper6
https://tubisocial.com/@laurindaschube?page=about https://tubisocial.com/
http://63.141.251.154/jeanninesheppa 63.141.251.154
http://101.37.147.115:3000/sonjawawn0149 http://101.37.147.115/
https://cash.com.tr/@chandah4432966?page=about https://cash.com.tr/@chandah4432966?page=about
https://git.erfmann.dev/renapittman856 git.erfmann.dev
https://videoasis.com.br/@juliusfoutch75?page=about videoasis.com.br
https://git.sskuaixiu.com/vnafaye7501772 git.sskuaixiu.com
https://git.bp-web.app/albahedge96704 https://git.bp-web.app/
https://gitea.redaktion.titanic-magazin.de/soonrhem342348 https://gitea.redaktion.titanic-magazin.de/
https://code.ownwire.net/teresita30c500 code.ownwire.net
References:
https://bwjobs4graduates.online/companies/can-cold-plunges-boost-testosterone-exploring-the-benefits-and-scienc/
47.92.113.131 · April 3, 2026 at 12:50 pm
anapolon max 50
https://nas.zearon.com:2001/arscara1114588 nas.zearon.com
http://112.124.40.88:5510/jillhighsmith/jill2021/wiki/Hyperprolactinemia%3A-What-It-Is%2C-Symptoms-%26-Treatment http://112.124.40.88:5510/jillhighsmith/jill2021/wiki/Hyperprolactinemia:-What-It-Is,-Symptoms-&-Treatment
https://git.barneo-tech.com/millaburdine32 git.barneo-tech.com
https://gividsocial.com/@senaidabreeze?page=about https://gividsocial.com/
https://volunteeri.com/companies/long-lived-testosterone-esters-in-the-rat/ volunteeri.com
https://vidoo.online/@reed36q321837?page=about vidoo.online
https://dubaijobsae.com/companies/underground-labs-vs-pharmaceutical-grade/ dubaijobsae.com
https://beatsong.app/randalearl851 beatsong.app
https://git.ewengadonnaud.xyz/baelena0111049 git.ewengadonnaud.xyz
https://date.etogetherness.com/@marcelagkr2459 date.etogetherness.com
https://unitedmusicstreaming.com/danareis103219 unitedmusicstreaming.com
http://139.196.103.114:18084/sfobeulah67749 139.196.103.114
https://git.ccmhub.se/smfdotty975315 https://git.ccmhub.se
https://git.m.ctf.arrobe.fr/berrycusack309 git.m.ctf.arrobe.fr
https://www.milegajob.com/companies/finish/ https://www.milegajob.com
http://124.71.197.109:3000/blytheopa3696 124.71.197.109
https://kaymanuell.com/@adrianbarone11?page=about kaymanuell.com
http://dev-gitlab.dev.sww.com.cn/ernestocarrozz http://dev-gitlab.dev.sww.com.cn/ernestocarrozz
References:
http://123.60.146.54:3000/cruzmartyn721/120.26.116.2439376/wiki/Buy-Testosterone-Enanthate-online%2C-cheap-injection-for-sale
47.115.223.229 · April 3, 2026 at 12:54 pm
bodybuilder steroids for sale
https://jomowa.com/@idmrachelle47 jomowa.com
https://codes.tools.asitavsen.com/xrwkrystal0956 codes.tools.asitavsen.com
https://docentesdeingles.ec/employer/the-role-of-resveratrol-in-human-male-fertility/ docentesdeingles.ec
http://83.229.125.195:8418/lewisrous4381 83.229.125.195
https://git.mis24.ru/houstonhateley/9842256/wiki/Post-Cycle-Therapy-PCT-Guide-Testosterone-Recovery-After-Steroid-Cycles git.mis24.ru
https://empleosytrabajos.us/employer/sex-differences-in-immune-responses-to-viruses-bacteria-and-vaccines/ empleosytrabajos.us
https://bigotube.com/@williameasterb?page=about https://bigotube.com/@williameasterb?page=about
https://aipod.app/adrieneheavene aipod.app
https://portal.shcba.org/employer/do-push-ups-increase-testosterone/ portal.shcba.org
https://amore.is/@manuelacaron09 amore.is
http://152.136.158.133:36512/jadanaylor479 152.136.158.133
http://1.95.221.174:3000/preciouswillis http://1.95.221.174:3000/preciouswillis
http://82.156.121.2:3000/agneskjy993642 82.156.121.2
http://sleep-talking.waemok.co.kr/bbs/board.php?bo_table=faq http://sleep-talking.waemok.co.kr/
https://aaredate.ch/@maureenberry1 https://aaredate.ch/
http://47.98.183.226:3000/ynfjohnette451 47.98.183.226
http://e-Hp.info/mitsuike/4-bbs/bbs/m-123y.cgi?id=1&post=1&&comment=000587 http://e-Hp.info
http://47.112.137.193:3000/briannerumpf31 http://47.112.137.193:3000/briannerumpf31
References:
https://aeterna.cim.mcgill.ca/dannierobison
https://amore.is/@hwagosling9377 · April 3, 2026 at 12:55 pm
References:
Synthetic anabolic steroids
References:
https://git.ewengadonnaud.xyz/florian26x9928/florian2001/wiki/Amazon-com%3A-Irwin-Naturals-Energy-%27%26%27-Endurance-Testosterone-Up-Men-Over-40-60-Sgels-%3A-Health-%26-Household
http://globaldream.or.kr/ · April 3, 2026 at 1:14 pm
did the rock do steroids
http://115.190.214.62:3001/christenkeener 115.190.214.62
https://bigotube.com/@georgettamatne?page=about https://bigotube.com/@georgettamatne?page=about
https://xn--lpris-iua.nu/aliceraposo543 lpris-iua.nu
https://koseongnam.com/ardisstledger7 koseongnam.com
https://christianmail.tv/@kiera60j617490?page=about christianmail.tv
http://104.254.131.244:3000/lashayzaleski 104.254.131.244
https://git.huwhy.cn/geniemadigan4/8711718/wiki/UGL-vs-legit-Pharma-efficacy-Pharma-T-Nation-by-Biotest git.huwhy.cn
http://mtthub.org/groups/your-trusted-supplier-for-australian-steroids/ http://mtthub.org/groups/your-trusted-supplier-for-australian-steroids/
http://repo.magicbane.com/charismclain22 repo.magicbane.com
http://13.230.31.145:8418/jennyycj857731 http://13.230.31.145:8418/jennyycj857731
https://gladjobs.com/employer/fda-approves-new-medication-for-chronic-weight-management/ https://gladjobs.com/employer/fda-approves-new-medication-for-chronic-weight-management
https://git.entryrise.com/penneymusser54 git.entryrise.com
https://code.hpswk.com/caryprettyman6 code.hpswk.com
https://blackvision.co.uk/@gitaneubauer37?page=about blackvision.co.uk
https://git.deadpoo.net/rosariofrencha https://git.deadpoo.net/rosariofrencha
https://m.my-conf.ru/chris51203582 https://m.my-conf.ru/chris51203582
http://13.230.31.145:8418/jennyycj857731 13.230.31.145
http://106.55.0.66:31807/mellisagillott http://106.55.0.66:31807/mellisagillott
References:
https://git.htns.com/marianahinz406
8.138.192.83 · April 3, 2026 at 1:35 pm
liquid testosterone for sale
https://skiivie.com/@philippsanford?page=about https://skiivie.com
https://git.healthathome.com.np/maurapatrick16 https://git.healthathome.com.np/maurapatrick16
https://krazzy4gangaur.com/@hnrgeorgina575?page=about krazzy4gangaur.com
https://21pac.com/@ignaciovbj2895?page=about 21pac.com
https://daftsex.lol/@troyswan436942?page=about daftsex.lol
https://git.vsadygv.com/kendricka28151 git.vsadygv.com
https://spin.org.pk/employer/omnadren-testosterone-uses-side-effects-interactions-dosage/ spin.org.pk
https://git.ecorous.org/concettasifuen git.ecorous.org
https://skiivie.com/@philippsanford?page=about https://skiivie.com/@philippsanford?page=about
http://36.133.248.69:3088/amoscurr675449 http://36.133.248.69:3088/amoscurr675449
https://aeterna.cim.mcgill.ca/dannierobison https://aeterna.cim.mcgill.ca/dannierobison
http://120.201.125.140:3000/hellenlawless http://120.201.125.140:3000/hellenlawless
https://gitea-inner.fontree.cn/wxsbonita72422 https://gitea-inner.fontree.cn/wxsbonita72422
http://103.228.160.127:3100/vernellhoddle9 103.228.160.127
https://csmsound.exagopartners.com/lawerenceblank https://csmsound.exagopartners.com/lawerenceblank
https://bwjobs4graduates.online/companies/can-cold-plunges-boost-testosterone-exploring-the-benefits-and-scienc/ https://bwjobs4graduates.online
https://git.morozoff.pro/allanhaygood24 git.morozoff.pro
http://111.228.56.162:3000/benitodrakefor 111.228.56.162
References:
https://digitalafterlife.org/@ahmedwhitingto?page=about
https://lovewiki.faith/wiki/Testosterone_Levels_By_Age:_Normal_Levels_For_Males_And_Females · April 3, 2026 at 1:50 pm
where are steroids found in the body
http://43.143.142.38:7001/bessharbin9798/875581.69.57.215/wiki/Ketogenic+state+improves+testosterone+serum+levels-results+from+a+systematic+review+and+meta-analysis.- 43.143.142.38
http://47.115.132.164:5500/paulettecoury9 http://47.115.132.164/
https://18let.cz/@irmastepp6732 https://18let.cz
http://159.75.131.235:3001/mozellehutchis http://159.75.131.235:3001/mozellehutchis
https://gitea.coderpath.com/irisy196695409 gitea.coderpath.com
http://124.223.18.41:10082/indiradallachy 124.223.18.41
https://gt.clarifylife.net/carmen70u79763 https://gt.clarifylife.net/carmen70u79763
https://www.heyne.cloud/chassidye44575 https://www.heyne.cloud/chassidye44575
https://git.deadpoo.net/shanonbenavide git.deadpoo.net
https://iconicoverseasconsultancy.com/employer/sermorelin-what-is-it-and-is-it-right-for-you/ https://iconicoverseasconsultancy.com
https://git.privezishop.ru/bpwemil3642328/5299597/wiki/Scrotum%3A-Anatomy-%26-Function git.privezishop.ru
https://michapo.com/employer/zinc-testosterone-whats-the-connection/ michapo.com
https://git.deadpoo.net/shanonbenavide git.deadpoo.net
http://yun.pashanhoo.com:9090/hwrallan004717 yun.pashanhoo.com
https://camtalking.com/@harrisforlonge camtalking.com
https://movieplays.net/@mayas13364442?page=about movieplays.net
https://yaseen.tv/@valeriarhoads?page=about yaseen.tv
https://videoasis.com.br/@juliusfoutch75?page=about https://videoasis.com.br/@juliusfoutch75?page=about
References:
http://55x.top:9300/colbydaley8739/colby1996/wiki/The-interaction-between-cortisol-and-testosterone-predicts-leadership-within-rock-hyrax-social-groups
https://deltasongs.com/ · April 3, 2026 at 3:26 pm
what does anabolic steroids do to your body
http://newborhooddates.com/@eveathaldo9818 newborhooddates.com
https://10xhire.io/employer/testosterone-may-help-heart-failure-patients,-studies-suggest/ 10xhire.io
https://gitlab.iplusus.com/jonnalording36 gitlab.iplusus.com
http://112.124.40.88:5510/temekaodum523/temeka2020/wiki/Testosterone-Replacement-Therapy%3A-Injections%2C-Patches%2C-and-Gels 112.124.40.88
https://essencialponto.com.br/employer/what-is-tren-cough-and-how-to-avoid-it/ essencialponto.com.br
http://dev-gitlab.dev.sww.com.cn/shantaeludwig http://dev-gitlab.dev.sww.com.cn/shantaeludwig
http://120.210.80.160:3000/vanxxt99753885 120.210.80.160
https://geniusactionblueprint.com/@andraelkington?page=about geniusactionblueprint.com
https://www.canaddatv.com/@ulyssesvansick?page=about http://www.canaddatv.com
https://www.uria.dev/salvatoreparam https://www.uria.dev/salvatoreparam
http://47.113.101.80:3000/adrienemangum 47.113.101.80
https://meeting2up.it/@maybellgreenwo https://meeting2up.it/@maybellgreenwo
https://gitea.cfpoccitan.org/eltonvazquez51 gitea.cfpoccitan.org
http://139.196.82.227:3000/ionac59981251 139.196.82.227
https://gitea.cfpoccitan.org/phil69c2334081 https://gitea.cfpoccitan.org/phil69c2334081
https://niqnok.com/carmel67237686 niqnok.com
https://51.68.226.41/freddy88r3168 51.68.226.41
http://8.141.82.163:20000/coralowrie296 http://8.141.82.163:20000/coralowrie296
References:
https://git.salingbot.com/lloydtildesley
yogicentral.science · April 3, 2026 at 4:06 pm
steroid before and after first cycle
https://gitea.zachl.tech/chun44p458927 gitea.zachl.tech
http://gitea.jb1000.com:88/eyclakesha2521 gitea.jb1000.com
https://git.bp-web.app/albahedge96704 git.bp-web.app
https://abadeez.com/@bernadettehind?page=about abadeez.com
https://www.propitarios-alquilan.shop/guykabu750553 https://www.propitarios-alquilan.shop
https://git.htns.com/marianahinz406 git.htns.com
http://47.92.23.195:8418/simasands18739 47.92.23.195
https://git.opnkty.uk/ashleewollston https://git.opnkty.uk/
https://movieplays.net/@mayas13364442?page=about movieplays.net
http://play.kkk24.kr/bbs/board.php?bo_table=online&wr_id=343840 play.kkk24.kr
http://www.shkxrd.com:3000/casimirawedge http://www.shkxrd.com
https://fmagency.co.uk/companies/how-does-mk-677-influence-testosterone-levels/ https://fmagency.co.uk/companies/how-does-mk-677-influence-testosterone-levels
https://cloudtu.be/@juneskirving9?page=about https://cloudtu.be/@juneskirving9?page=about
https://root-kit.ru/krystleburnett https://root-kit.ru/krystleburnett
https://git.vhdltool.com/hanscrace23001 git.vhdltool.com
https://git.alderautomation.ca/maryannwhitmir/allyoutubes.com2475/wiki/Your-trusted-supplier-for-Australian-steroids git.alderautomation.ca
https://vyaparappsurat.store/are-testosterone-injections-legal-revive-hormone-clinic/ vyaparappsurat.store
https://git.vhdltool.com/kimberlyoconne git.vhdltool.com
References:
http://61.190.74.90:9900/meghanballenti/2813logisticconsultant.net/wiki/Issues-from-underdosed-UGL-testosterone%21-Pharma-T-Nation-by-Biotest
https://aitune.net/christilemaste · April 3, 2026 at 4:20 pm
References:
Crazy bulk for sale
References:
https://remotejobs.website/profile/agustinjeffcot
https://gitea.ai-demo.duckdns.org/ · April 3, 2026 at 4:40 pm
anabolics for sale
http://101.37.69.204:3000/frankiehightow/frankie2008/wiki/Testosterone+and+Hair+Loss%3A+Common+Myths%2C+Facts%2C+and+What+Actually+Matters+–.- 101.37.69.204
https://teanurture.online/buy-testosterone-enanthate-online-cheap-injection-for-sale-9/ teanurture.online
http://maxes.co.kr/bbs/board.php?bo_table=free&wr_id=2907551 maxes.co.kr
http://47.121.119.78:3000/albertosoderst http://47.121.119.78:3000/albertosoderst
http://62.173.140.174:10480/bettieshumate9/8975126/wiki/The-life-cycle-of-metabolism-UAB-News 62.173.140.174
https://metagap.ro/employer/effects-of-exercise-training-on-resting-testosterone-concentrations-in-insufficiently-active-men-a-systematic-review-and-meta-analysis/ https://metagap.ro/
http://mignonmuse.com/bbs/board.php?bo_table=free&wr_id=597915 http://mignonmuse.com
http://git.mynas71.myds.me/sammieffu68636 http://git.mynas71.myds.me/sammieffu68636
https://git.htns.com/marianahinz406 git.htns.com
http://124.223.89.168:8080/jsnsue9178324/4362infolokerbali.com/wiki/Fitness%2C-Nutrition%2C-Health%2C-Sex%2C-Style-%26-Weight-Loss-Tips-for-Men 124.223.89.168
http://git.dglyoo.com/mackenzie25951 http://git.dglyoo.com
https://deltasongs.com/sheenaharitos https://deltasongs.com/
http://www.shkxrd.com:3000/lindseybancrof http://www.shkxrd.com:3000/lindseybancrof
https://direct-jobs.nl/employer/why-more-men-should-be-eating-rocky-mountain-oysters/ https://direct-jobs.nl/
http://139.196.82.227:3000/sharitaylor47 http://139.196.82.227:3000/sharitaylor47
https://krazzy4gangaur.com/@jedsandberg91?page=about krazzy4gangaur.com
http://git.dglyoo.com/carsonokeeffe http://git.dglyoo.com
https://www.globaltubedaddy.com/@sqzvania12968?page=about https://www.globaltubedaddy.com/@sqzvania12968?page=about
References:
http://43.143.209.246:6300/bernadineembry
clashofcryptos.trade · April 3, 2026 at 6:18 pm
References:
Bulk stacks
References:
http://209.127.59.74:3000/ihvangelica608
global.gwangju.ac.kr · April 3, 2026 at 6:41 pm
steroids that make you lose weight
http://120.24.175.146:3000/georgiannawedg http://120.24.175.146:3000/georgiannawedg
http://ch-marine.co.kr/bbs/board.php?bo_table=qna&wr_id=152717 ch-marine.co.kr
http://150.158.37.69:3000/arturokirkland http://150.158.37.69
http://47.98.192.5:3000/moktawnya8229 http://47.98.192.5:3000/moktawnya8229
https://daftsex.lol/@cheriebuckley6?page=about https://daftsex.lol/
https://portal.shcba.org/employer/how-to-increase-testosterone-12-proven-ways-to-boost-low-t-dallas-tx/ portal.shcba.org
https://www.wealthtv.tz/@borisswaney43?page=about wealthtv.tz
https://62.234.182.183/budtolentino1 https://62.234.182.183
https://www.emploitelesurveillance.fr/employer/are-there-benefits-to-ball-stretching-or-is-it-hyped/ emploitelesurveillance.fr
https://gitea.redaktion.titanic-magazin.de/aubreyp0445018 https://gitea.redaktion.titanic-magazin.de/aubreyp0445018
https://vyaparappsurat.store/dry-orgasm-causes-and-treatment/ vyaparappsurat.store
https://gitea.personalsoftware.space/sharimurdock92 gitea.personalsoftware.space
http://ydds.cloud:3000/tonja33n664521 http://ydds.cloud/
http://121.41.95.54:3000/susie95s487074/susie2003/wiki/Management-of-Male-Fertility-in-Hypogonadal-Patients-on-Testosterone-Replacement-Therapy 121.41.95.54
http://218.232.111.112:8300/vxkleonardo856 http://218.232.111.112:8300/vxkleonardo856
http://39.108.209.179:3000/pnbelisa12777/elisa1999/wiki/Long-lived-testosterone-esters-in-the-rat 39.108.209.179
https://qflirt.net/@willis09966737 https://qflirt.net/@willis09966737
https://www.xtrareal.tv/@maxwellstahlma?page=about http://www.xtrareal.tv
References:
https://askmilton.tv/@analisalebron9?page=about
47.92.35.224 · April 3, 2026 at 7:23 pm
over counter steroids
https://dev-members.writeappreviews.com/employer/healthline-medical-information-and-health-advice-you-can-trust/ dev-members.writeappreviews.com
https://www.workinternational-df.com/employer/your-trusted-supplier-for-australian-steroids/ https://www.workinternational-df.com/employer/your-trusted-supplier-for-australian-steroids/
http://crane.waemok.co.kr/bbs/board.php?bo_table=faq crane.waemok.co.kr
https://git2.ujin.tech/florentinay50/git.stormrain.cn1994/wiki/Best-UGL-Testosterone-Options-Explained%3A-Unlocking-Optimal-Hormone-Balance-TRT-Now git2.ujin.tech
https://44sex.com/@eduardobodifor?page=about 44sex.com
http://43.139.2.237:3000/gusmoffat70476 http://43.139.2.237
http://58.221.157.122:3000/britneygaskin/8489124.223.18.41/wiki/Buy-Testosterone-Enanthate-online%2C-cheap-injection-for-sale http://58.221.157.122:3000/britneygaskin/8489124.223.18.41/wiki/Buy-Testosterone-Enanthate-online,-cheap-injection-for-sale
https://unired.zz.com.ve/@liliaprevost20 https://unired.zz.com.ve/
http://120.24.175.146:3000/georgiannawedg 120.24.175.146
https://securityholes.science/wiki/User:NTRMorris63 securityholes.science
http://122.226.176.166:8404/timstanbury63/101.43.238.712021/wiki/Buy-Testosterone-Enanthate-online%2C-cheap-injection-for-sale 122.226.176.166
https://git.archieri.fr/carmelomill658 git.archieri.fr
https://git2.ujin.tech/malloryburwell https://git2.ujin.tech/malloryburwell
https://www.pulaplay.com/@zacolivarez369?page=about http://www.pulaplay.com
https://pepecitos.com.ar/louellacaswell https://pepecitos.com.ar
https://git.binarycat.org/kinavaughan40 https://git.binarycat.org/
https://nas.zearon.com:2001/ingridhollinwo nas.zearon.com
http://112.124.40.88:5510/umbjanessa310/2815reruberrypi.rerurate.com/wiki/Testosterone-Tests-%26-Panels-Testosterone-Level-Testing http://112.124.40.88
References:
https://git.meshel.cn/rebbecanilsen5
https://git.hubhoo.com/michalefeeney · April 3, 2026 at 7:28 pm
hgh spray gnc
https://ns2.asso-web.com/loutiller66605 https://ns2.asso-web.com/loutiller66605
https://rentry.co/98069-the-heart-of-the-internet rentry.co
https://ashkert.am/%D5%A1%D5%B7%D5%AF%D5%A5%D6%80%D5%BF%D5%AB-%D5%B0%D5%A1%D5%B4%D5%A1%D6%80/turkesterone-testosterone-booster-reviews-complaints-2026-reviews-read-customer-service-reviews-of-turkesteronetestosteronebooster-lovable-app/ https://ashkert.am/աշկերտի-համար/turkesterone-testosterone-booster-reviews-complaints-2026-reviews-read-customer-service-reviews-of-turkesteronetestosteronebooster-lovable-app/
https://www.quranpak.site/estellebird131 http://www.quranpak.site
http://175.27.229.211:3000/desireesmart93/mp3diary.com6583/wiki/Amazon-com%3A-MARS-MEN-Testosterone-Booster-for-Men-Natural-Supplement-Premium-Tongkat-Ali%2C-Fenugreek%2C-Shilajit-%26-Boron-Male-Support-Libido%2C-Energy-%26-Muscle-Growth-Support-30-Servings-%3A-Health-%26-Household http://175.27.229.211:3000/desireesmart93/mp3diary.com6583/wiki/Amazon-com:-MARS-MEN-Testosterone-Booster-for-Men-Natural-Supplement-Premium-Tongkat-Ali,-Fenugreek,-Shilajit-&-Boron-Male-Support-Libido,-Energy-&-Muscle-Growth-Support-30-Servings-:-Health-&-Household
http://172.104.245.78:11080/marilynmidgett 172.104.245.78
https://date.etogetherness.com/@ermamoreno984 https://date.etogetherness.com/@ermamoreno984
https://menifeemunchkins.com/the-dosage-and-frequency-of-testosterone-injections-for-transgender-men/ menifeemunchkins.com
http://175.178.150.62:3002/edwinbingham92 175.178.150.62
http://172.104.245.78:11080/julissatorres8 172.104.245.78
http://81.70.24.14:3000/margaretcpo950 http://81.70.24.14
https://git.p1.bitstorm.co.nz/sueluse4625793 git.p1.bitstorm.co.nz
https://jobdoot.com/companies/testosterone-signals-through-mtor-and-androgen-receptor-to-induce-muscle-hypertrophy-houston-methodist-scholars/ jobdoot.com
https://i.megapollos.com/@veda3378594396?page=about https://i.megapollos.com/@veda3378594396?page=about
https://dev.modelhub.org.cn/elsaheap930217 dev.modelhub.org.cn
https://dyipniflix.com/site/@kellemercier2?page=about dyipniflix.com
https://companyjobs.cn/employer/amazon-com-5-in-1-himalayan-shilajit-for-men-women-1250mg-ashwagandha-tongkat-ali-maca-root-turkesterone-80-fulvic-acid-energy-testosterone-vitality-60-vegan-capsules-health/ companyjobs.cn
https://gitea.primecontrols-dev.com/pearlinekline https://gitea.primecontrols-dev.com/pearlinekline
References:
http://14.103.239.131:3000/garrymoulton92
8.138.187.132 · April 3, 2026 at 7:43 pm
References:
Best way to take dianabol
References:
https://movieplays.net/@islaoswalt9612?page=about
play.talkdrove.cc.nf · April 3, 2026 at 7:43 pm
testosterone injection dosage for muscle building
https://www.meetgr.com/@bzxdelphia015 http://www.meetgr.com
https://musiciansportal.ru/andrewdunrossi musiciansportal.ru
http://8.138.187.132:3000/geririordan02/gitee.planhomecloud.cn2024/wiki/Restarting-Testosterone-After-TRT%3A-A-Guide-for-Men 8.138.187.132
https://guateempleos.com/companies/testosterone-wikipedia/ https://guateempleos.com
https://allasguru.com/cegek/the-effects-of-diet-on-circulating-sex-hormone-levels-in-men/ allasguru.com
http://81.69.221.216:3000/isidrogallard 81.69.221.216
https://www.hyzq123.com/@roseannegiltne?page=about https://www.hyzq123.com/@roseannegiltne?page=about
http://119.91.35.154:3000/rosacass775963 119.91.35.154
https://grupokandidat.com/compa%C3%B1ias/testosterone-propionate-testosterone-phenylpropionate-testosterone-isocaproate-testosterone-caproate/ https://grupokandidat.com
https://csmtube.exagopartners.com/@brigettesolomo?page=about csmtube.exagopartners.com
https://jobstak.jp/companies/a-practical-guide-to-male-hypogonadism-in-the-primary-care-setting/ jobstak.jp
https://www.howeasynetwork.com/@ernestbowie08?page=about http://www.howeasynetwork.com
http://Vivefive.Sakura.Ne.jp/aska/aska.cgi Vivefive.Sakura.Ne.jp
https://qdate.ru/@charlenez95926 qdate.ru
https://62.234.182.183/estellajanney8 https://62.234.182.183
https://gitea.amazingcoders.com/demetriusville https://gitea.amazingcoders.com/demetriusville
https://isugar-dating.com/@raleighvenegas https://isugar-dating.com
https://git.adityagupta.dev/ferdinandmiche https://git.adityagupta.dev/
References:
https://gitea.brmm.ovh/joieingalls18
career.abuissa.com · April 3, 2026 at 7:44 pm
References:
Rapid tone weight loss ingredients
References:
https://jandlfabricating.com/employer/amazon-com-irwin-naturals-energy-endurance-testosterone-up-men-over-40-60-sgels-health-household/
guiacomercialsaopaulo.com · April 3, 2026 at 7:48 pm
pro testosterone side effects
https://gitea.amazingcoders.com/demetriusville gitea.amazingcoders.com
http://120.211.66.170:8418/guillermotravi http://120.211.66.170/
https://git.slegeir.com/cathernchamp35/506547.100.44.145/wiki/Testosterone-Levels-in-Men-Explained%3A-Normal-Ranges-%26-Age-Chart https://git.slegeir.com/cathernchamp35/506547.100.44.145/wiki/Testosterone-Levels-in-Men-Explained:-Normal-Ranges-&-Age-Chart
https://gitea.zachl.tech/lolitamott924 https://gitea.zachl.tech/lolitamott924
http://211.149.155.157:3000/vincegriffin19 http://211.149.155.157/
https://globalhospitalitycareer.com/employers/turkesterone-before-and-after-results-dosage-side-effects/ https://globalhospitalitycareer.com
https://gitea.johannes-hegele.de/tamisquire7122 gitea.johannes-hegele.de
https://git.csi-kjsce.org/clintonheaton git.csi-kjsce.org
https://quickdate.arenascript.de/@jerrodtong3726 quickdate.arenascript.de
http://43.139.2.237:3000/maximodenby948 http://43.139.2.237
http://115.159.107.117:3000/daniloe4637106/2837750/wiki/Changes-in-levels-of-testosterone%2C-insulin-sensitivity-and-metabolic-profiles-during-GnRH-therapy:-Reciprocity-between-insulin-sensitivity-and-pituitary-responsiveness-to-GnRH-in-teenage-and-young-male-patients-with-congenital-hypogonadotropic-hypogonadism http://115.159.107.117:3000/daniloe4637106/2837750/wiki/Changes-in-levels-of-testosterone,-insulin-sensitivity-and-metabolic-profiles-during-GnRH-therapy:-Reciprocity-between-insulin-sensitivity-and-pituitary-responsiveness-to-GnRH-in-teenage-and-young-male-patients-with-congenital-hypogonadotropic-hypogonadism
http://121.41.95.54:3000/stella61693373/8754633/wiki/What-Is-Myofascial-Release%3F-What-it%27s-for-and-How-it-Works 121.41.95.54
http://59.80.22.43:30000/trudylaffer972 http://59.80.22.43:30000/trudylaffer972
https://git2.ne-it.net/enriquetafegan/5847git.dieselor.bg/wiki/Precision-Analytical-DUTCH-TEST-Test-Kits%2C-Providers-%26-Patients git2.ne-it.net
http://www.shkxrd.com:3000/phoebeweinberg http://www.shkxrd.com:3000/phoebeweinberg
http://43.139.2.237:3000/maximodenby948 http://43.139.2.237:3000/maximodenby948
https://git.wisder.net/ilabess8332415 git.wisder.net
https://play.eccentric.etc.br/@kasey084193717?page=about play.eccentric.etc.br
References:
https://inspiredcollectors.com/component/k2/author/185176-whatisanormaltestosteronelevelforyoungmen?rethinkingthe300ngdlcutofffortestosteronedeficiencyinmen2044yearsold
mygit.kikyps.com · April 3, 2026 at 7:59 pm
References:
Bostin loyd steroid cycle
References:
https://git.autotion.net/kenneth91k419
http://124.236.46.74/ · April 3, 2026 at 8:00 pm
steroids to gain muscle mass
http://39.100.117.84:3000/loraarmitage3/2035www.annunciogratis.net/wiki/10-Surprising-Health-Benefits-of-Sex 39.100.117.84
https://www.abgodnessmoto.co.uk/index.php?page=user&action=pub_profile&id=63914&item_type=active&per_page=16 http://www.abgodnessmoto.co.uk
https://git.cyber-tek.ru/stuartshellshe https://git.cyber-tek.ru
https://git.thoughtvectors.uk/linetteluciano git.thoughtvectors.uk
http://47.105.124.101:3000/venettasettle6 47.105.124.101
https://git.danpeak.co.uk/rosalindaboshe https://git.danpeak.co.uk/rosalindaboshe
https://ex-pose.one/@jodybarrallier?page=about ex-pose.one
https://syq.im:2025/ebaclaribel686 syq.im
https://tiktub.com/@gregorioq53078?page=about tiktub.com
http://113.177.27.200:2033/marlenesheean/git.saidomar.fr7303/wiki/Voice-deepening-under-testosterone-treatment-in-female-to-male-gender-dysphoric-individuals 113.177.27.200
http://43.138.249.161:3000/felicitas74i04 43.138.249.161
http://121.41.95.54:3000/shalanda868152/2934198/wiki/MK-777%3A+The+Stronger+MK-677+Upgrade+That+Eliminates+Side+Effects.- http://121.41.95.54
https://incisolutions.app/jake5437643270 incisolutions.app
http://code.sz-chaohui.cn/sethpadgett70 http://code.sz-chaohui.cn/sethpadgett70
http://118.195.135.194:3000/pamalaignacio1 118.195.135.194
http://styleupnow.com/@markbarkly473?page=about http://styleupnow.com/@markbarkly473?page=about
https://portal.shcba.org/employer/how-to-increase-testosterone-12-proven-ways-to-boost-low-t-dallas-tx/ https://portal.shcba.org/employer/how-to-increase-testosterone-12-proven-ways-to-boost-low-t-dallas-tx
https://i-medconsults.com/companies/buy-testosterone-enanthate-online-cheap-injection-for-sale/ i-medconsults.com
References:
https://git.tecno-group.mx/zeldagooding62
http://120.76.251.151 · April 3, 2026 at 8:03 pm
steroid names
https://traficut.com/@gretchenk78449?page=about traficut.com
http://www.shkxrd.com:3000/phoebeweinberg http://www.shkxrd.com
https://www.xtrareal.tv/@maxwellstahlma?page=about http://www.xtrareal.tv
https://www.abgodnessmoto.co.uk/index.php?page=user&action=pub_profile&id=63994&item_type=active&per_page=16 http://www.abgodnessmoto.co.uk
https://collisioncommunity.com/employer/low-shbg-high-free-t-feel-like-garbage-the-metabolic-trap-no-one-warns-you-about/ https://collisioncommunity.com/employer/low-shbg-high-free-t-feel-like-garbage-the-metabolic-trap-no-one-warns-you-about/
http://220.205.16.27:18081/richardbirming http://220.205.16.27:18081/richardbirming
https://funnyutube.com/@dollyprimeaux5?page=about https://funnyutube.com/@dollyprimeaux5?page=about
https://www.kornerspot.com/@chongmunn43445 https://www.kornerspot.com/@chongmunn43445
http://38.76.202.113:3000/german53398605 38.76.202.113
https://git.e-drones.com/louellablundst https://git.e-drones.com/louellablundst
http://124.222.218.198:3000/lester72723914 http://124.222.218.198
http://207.180.227.11:3001/beausteinberge 207.180.227.11
http://34.17.182.140/rachelb9521917/5952sponsorjobs.com.au/wiki/Buy-Testosterone-Enanthate-online%2C-cheap-injection-for-sale http://34.17.182.140/rachelb9521917/5952sponsorjobs.com.au/wiki/Buy-Testosterone-Enanthate-online,-cheap-injection-for-sale
https://sprohr.com/employer/testosterone-associations-with-parents-child-abuse-risk-and-at-risk-parenting-a-multimethod-longitudinal-examination/ sprohr.com
http://110.42.217.153:8029/janigrove75754 110.42.217.153
https://gitlab.herzog-it.de/velvabarba2858 gitlab.herzog-it.de
https://pure.itsabouttimetv1.com/@velva05i653478?page=about pure.itsabouttimetv1.com
http://120.76.251.151:3000/nilaherrin4656:3000/nilaherrin4656 120.76.251.151
https://app.boliviaplay.com.bo/ · April 3, 2026 at 8:18 pm
what are the street names for steroids
http://115.159.194.75:4000/augustusaslatt http://115.159.194.75
http://ydds.cloud:3000/tonja33n664521 ydds.cloud
https://gitlab-rock.freedomstate.idv.tw/asabeavis41761 gitlab-rock.freedomstate.idv.tw
http://yun.pashanhoo.com:9090/tashathrower83 yun.pashanhoo.com
https://git.p1.bitstorm.co.nz/sueluse4625793 git.p1.bitstorm.co.nz
https://git.morozoff.pro/josiehebblethw/7702969/wiki/Protective-effects-of-tadalafil-and-N-acetyl-cysteine-therapy-on-cisplatin-induced-testicular-toxicity git.morozoff.pro
https://funnyutube.com/@dollyprimeaux5?page=about https://funnyutube.com/
https://git.suzk.ru/zeldalawlor714 https://git.suzk.ru/zeldalawlor714
http://uniprint.co.kr/bbs/board.php?bo_table=free&wr_id=270985 http://uniprint.co.kr
http://175.154.160.23:3237/leonidaaustral 175.154.160.23
https://lyfeclick.com/@laylacardona0 lyfeclick.com
http://47.92.35.224:3000/jaimiesosa320/jaimie2019/wiki/Best-UGL-Testosterone-Options-Explained%3A-Unlocking-Optimal-Hormone-Balance-TRT-Now 47.92.35.224
https://62.234.182.183/budtolentino1 62.234.182.183
https://gitea.wgqcd.com/deloresmclauri https://gitea.wgqcd.com/deloresmclauri
https://114.242.31.6:3000/constancefeake https://114.242.31.6:3000/constancefeake
http://85.214.41.219:49153/kirbylloyd6069/47.99.119.1732016/wiki/Lifestyle-strategies-to-help-prevent-natural-age-related-decline-in-testosterone 85.214.41.219
https://kf.hebrewconnect.tv/@aidaachen47390?page=about kf.hebrewconnect.tv
https://matchymood.app/@willymacmillan matchymood.app
References:
https://gitlab.iplusus.com/veronicastonor/9869opensource.irext.net/wiki/Long-lived-testosterone-esters-in-the-rat
git.cymnb.com · April 3, 2026 at 9:41 pm
how are anabolic steroids used
http://47.98.183.226:3000/garnetcorcoran http://47.98.183.226
https://recrutement.fanavenue.com/companies/does-sunlight-increase-testosterone/ https://recrutement.fanavenue.com/companies/does-sunlight-increase-testosterone/
https://www.freakscene.net/smf/index.php?topic=11442.0 https://www.freakscene.net/smf/index.php?topic=11442.0
https://www.howeasynetwork.com/@johniemcdermot?page=about http://www.howeasynetwork.com
http://101.35.227.2:3000/vernvardon752 101.35.227.2
https://www.findinall.com/profile/sabinehinkler http://www.findinall.com
https://music.1mm.hk/kendall6677828 music.1mm.hk
http://124.223.89.168:8080/joycemeaux648/joyce2008/wiki/Amazon-com%3A-Irwin-Naturals-Energy-%27%26%27-Endurance-Testosterone-Up-Men-Over-40-60-Sgels-%3A-Health-%26-Household http://124.223.89.168
http://1.95.173.44:3000/mandyterrell53 http://1.95.173.44:3000/mandyterrell53
http://111.229.183.203:3000/irenehumphrey6 111.229.183.203
http://103.119.85.197:3000/noel63a837282/7060755/wiki/hCG-for-Men:-Uses%2C-Safety%2C-and-Side-Effects 103.119.85.197
https://pediascape.science/wiki/User:AliThynne022 pediascape.science
https://realhire.co/employer/phthalates-might-interfere-with-testicular-function-by-reducing-testosterone-and-insulin-like-factor-3-levels/ https://realhire.co/
http://82.156.65.157:30000/emileheilman4 http://82.156.65.157:30000/emileheilman4
https://freshteenclips.com/@stanrir3515327?page=about freshteenclips.com
https://talentfrontiers.ph/employer/phthalates-from-plastics-personal-care-products-influence-testosterone-levels-among-men/ talentfrontiers.ph
https://cameradb.review/wiki/Speciality_Blood_,_Urine_%26_Saliva_Tests cameradb.review
https://www.chembans.com/@sherlenedemers http://www.chembans.com
References:
https://git.thoughtvectors.uk/ofwtanja240466/2133786/wiki/Amazon-com%3A-Irwin-Naturals-Energy-%27%26%27-Endurance-Testosterone-Up-Men-Over-40-60-Sgels-%3A-Health-%26-Household
gitea.css-sistemas.com.br · April 3, 2026 at 9:49 pm
References:
Anabolic hormone definition
References:
http://47.99.119.173:13000/marcushartsock/companyjobs.cn7145/wiki/The-Largest-Online-Healthcare-Clinic-in-North-America%2C-Affordable-Pricing%2C-Enjoy-Increased-Energy-%26-Focus%21
git.sophiagwen.au · April 3, 2026 at 9:54 pm
References:
T ball steroid
References:
http://8.140.248.67:3000/franziska96r93
gitea.nkal.me · April 3, 2026 at 9:55 pm
amazon bigger leaner stronger
http://gsianpt01.nayaa.co.kr/bbs/board.php?bo_table=sub05_03&wr_id=36218 gsianpt01.nayaa.co.kr
https://gitea.ontoast.uk/darrincramsie6 https://gitea.ontoast.uk/
http://47.113.149.107:10110/wilheminagalle http://47.113.149.107/
https://hydrealty.in/author/jacksonkoeh/ hydrealty.in
http://124.222.218.198:3000/mose77e4024697 124.222.218.198
http://101.37.147.115:3000/claudialeigh4 101.37.147.115
http://223.108.157.174:3000/andreaqon06471 http://223.108.157.174
https://git.clubeye.net/ezequielmcconn https://git.clubeye.net/ezequielmcconn
https://klimaexpress-tube.de/@kristycope520?page=about klimaexpress-tube.de
http://175.154.160.23:3237/burtonwahl7440 http://175.154.160.23
https://git.rmarl.in/terese01m34479/terese2009/wiki/Buy-Testosterone-Enanthate-online%2C-cheap-injection-for-sale https://git.rmarl.in/
http://47.104.60.158:7777/lanefehon44000 http://47.104.60.158
https://git.cute.bet/normandtonga2 git.cute.bet
https://gitea.smatec.com.vn/kerstinminahan https://gitea.smatec.com.vn/kerstinminahan
https://git.kooera.com/arlenodea8148 https://git.kooera.com/arlenodea8148
http://89.234.183.97:3000/iolayxl5710118/3189tripled.driven-dreams.co.uk/wiki/Association-between-Fish-Intake-and-Serum-Testosterone-Levels-in-Older-Males%3A-The-Hitachi-Health-Study-II http://89.234.183.97:3000/iolayxl5710118/3189tripled.driven-dreams.co.uk/wiki/Association-between-Fish-Intake-and-Serum-Testosterone-Levels-in-Older-Males:-The-Hitachi-Health-Study-II
http://fanlibo.i234.me:8418/lorene55790990 http://fanlibo.i234.me/
https://git.p1.bitstorm.co.nz/azucenachabril https://git.p1.bitstorm.co.nz/azucenachabril
References:
https://sing.ibible.hk/@jordanmonnier2?page=about
https://lius.familyds.org · April 3, 2026 at 9:59 pm
legal steroid for muscle building
http://36.213.200.127:23000/kristyconyers4/kristy1983/wiki/How-does-ketoconazole-affect-testosterone-metabolism%3F 36.213.200.127
https://vidspaceaiapp.com/@carlomccarty81?page=about vidspaceaiapp.com
https://katambe.com/@virgiliowakeli katambe.com
http://ch-marine.co.kr/bbs/board.php?bo_table=qna&wr_id=152715 ch-marine.co.kr
https://isugar-dating.com/@rosalindaquall isugar-dating.com
https://git.htns.com/shawnafolk753 git.htns.com
https://music.drepic.com/kira08c8285282 https://music.drepic.com
https://gitea.manekenbrand.com/fwrsam51259178 gitea.manekenbrand.com
http://119.91.35.154:3000/alishakerry573/36.213.200.1272003/wiki/Amazon-com%3A-78%2C000mg-Testosterone-Supplement-for-Men%2C-Max-Purity-95%25-Testosterone-Booster-for-Men%2C-Turkesterone-for-More-Energy%2C-Strength%2C-Stamina%2C-Endurance%2C-Muscle-Growth-%26-Recovery%2C-Performance%2C-60-Days-Supply-%3A-Health-%26-Household 119.91.35.154
http://shinhwaspodium.com/bbs/board.php?bo_table=free&wr_id=4832507 http://shinhwaspodium.com/bbs/board.php?bo_table=free&wr_id=4832507
http://www.cn8610086.cn:3000/loreencollits http://www.cn8610086.cn
http://47.112.137.193:3000/numbersstapley 47.112.137.193
https://ltube.us/@wendywren34460?page=about https://ltube.us/@wendywren34460?page=about
https://git.ewengadonnaud.xyz/floriantemplet/florian2007/wiki/Is-testosterone-therapy-safe%3F-Take-a-breath-before-you-take-the-plunge git.ewengadonnaud.xyz
https://gitea.smatec.com.vn/kerstinminahan gitea.smatec.com.vn
https://git.fast-blast.uk/dieteru196186 git.fast-blast.uk
https://www.k0ki-dev.de/glennloch86749 https://www.k0ki-dev.de/glennloch86749
http://213.171.25.1:3000/mindy56v271419 http://213.171.25.1/
References:
https://git.cute.bet/sophiadunbar86/3562964/wiki/Buy-Testosterone-Cypionate-USA-Testosterone-Cypionate-for-Sale-Online
panjabi.in · April 3, 2026 at 10:18 pm
does steroids make your penis smaller
http://git.chilidoginteractive.com:3000/russbrack54645 git.chilidoginteractive.com
https://www.freakscene.net/smf/index.php?action=profile;u=14575 https://www.freakscene.net/smf/index.php?action=profile;u=14575
http://8.141.82.163:20000/royce56q581893 http://8.141.82.163:20000/royce56q581893
http://47.109.30.152:3000/jerroldforehan/git.suzk.ru7906/wiki/It-puts-the-Ts-in-fertility%3A-testosterone-and-spermatogenesis-International-Journal-of-Impotence-Research http://47.109.30.152:3000/jerroldforehan/git.suzk.ru7906/wiki/It-puts-the-Ts-in-fertility:-testosterone-and-spermatogenesis-International-Journal-of-Impotence-Research
https://skytube.skyinfo.in/@christianen92?page=about skytube.skyinfo.in
https://gitea.ashcloud.com/kandispiesse4 gitea.ashcloud.com
https://myafritube.com/@kristinatrumbl?page=about https://myafritube.com/
https://git.dslak.it/shannonwollast https://git.dslak.it
https://mixclassified.com/user/profile/1101480 mixclassified.com
https://clipsshort.com/@kirbysaldana0?page=about clipsshort.com
https://yaseen.tv/@renemanzo1712?page=about yaseen.tv
http://111.4.75.238:12600/rebbecacarboni 111.4.75.238
http://218.232.111.112:8300/debvaldes25223 http://218.232.111.112:8300/debvaldes25223
http://58.65.162.118:3000/margheritafedl http://58.65.162.118:3000/margheritafedl
https://jobs.ethio-academy.com/employer/does-ibutamoren-mess-with-testosterone/ jobs.ethio-academy.com
https://rlgit.pro/gladys3409273/rentry.co2449/wiki/The-Top-5-Herbs-That-Boost-Testosterone rlgit.pro
https://remotejobs.website/profile/sondraapodaca https://remotejobs.website/
https://www.godhip.com/judson53204924 godhip.com
References:
https://git.rmarl.in/brentoncastrej
https://git.daoyoucloud.com/venettahenry44/4647707/wiki/Testosterone-for-Klinefelter-Syndrome · April 3, 2026 at 10:31 pm
anadrol pill
http://git.zltest.com.tw:3333/lavernetregurt http://git.zltest.com.tw:3333/lavernetregurt
https://code.hpswk.com/silviahollins https://code.hpswk.com
https://www.globalshowup.com/@harrisprowse58?page=about http://www.globalshowup.com
https://code.ownwire.net/astridbrigstoc code.ownwire.net
http://e-Hp.info/mitsuike/4-bbs/bbs/m-123y.cgi?id=1&post=1&&comment=000587 e-Hp.info
https://gitea.personalsoftware.space/sethi32077881 gitea.personalsoftware.space
https://ott.saikatinfotech.com/@hollyconnal87?page=about https://ott.saikatinfotech.com/@hollyconnal87?page=about
http://101.37.147.115:3000/claudialeigh4 http://101.37.147.115
https://ltube.us/@wendywren34460?page=about ltube.us
http://dev-gitlab.dev.sww.com.cn/jacksonsjb8739 dev-gitlab.dev.sww.com.cn
https://menifeemunchkins.com/taiwan-tongkat-ali-extract-market-report-with-projected-13-7-from-2026-to-2033-demographic-data-and-growth-potential/ menifeemunchkins.com
http://121.181.234.77/bbs/board.php?bo_table=blessed_pray&wr_id=1374929 http://121.181.234.77/bbs/board.php?bo_table=blessed_pray&wr_id=1374929
http://106.52.242.177:3000/sherribingham 106.52.242.177
https://tripleoggames.com/employer/why-testosterone-levels-drop-and-when-to-consider-treatment/ tripleoggames.com
https://talentsplendor.com/employer/testosterone-levels-by-age-chart-female/ talentsplendor.com
https://www.nastavniki.com/@joannabtw4690?page=about http://www.nastavniki.com
https://myhealthypunjab.com/@bretehrhart68?page=about https://myhealthypunjab.com/@bretehrhart68?page=about
https://nrimatchmaking.com/@vtavilma176437 https://nrimatchmaking.com/@vtavilma176437
References:
https://bluestreammarketing.com.co/employer/testosterone-what-it-is-and-how-it-affects-your-health/
http://112.74.106.216 · April 3, 2026 at 11:23 pm
References:
Risks of taking steroids
References:
http://59.19.179.48:3300/taierick561528
http://git.chilidoginteractive.com:3000/raymundoharwoo/raymundo1997/wiki/Lifestyle-strategies-to-help-prevent-natural-age-related-decline-in-testosterone · April 3, 2026 at 11:26 pm
References:
All types of steroids
References:
https://kidstv.freearnings.com/@darnell3471988?page=about
https://code.ownwire.net/rodgergrace36 · April 3, 2026 at 11:35 pm
References:
Performance enhancing drugs in the military
References:
http://xn--289a6fl1aq39i.com/wave/board.php?bo_table=support&wr_id=1262
https://gitea.kamisama.ovh/milessummers89 · April 3, 2026 at 11:50 pm
References:
Make steroids
References:
https://vyaparappsurat.store/the-heart-of-the-internet-4/
zomi.watch · April 4, 2026 at 12:03 am
References:
How long does it take to get over steroid withdrawal?
References:
https://ai-db.science/wiki/User:AlbertoBard9
https://seychelleslove.com · April 4, 2026 at 12:36 am
References:
Best steroids for cutting
References:
http://47.105.124.101:3000/claudiaosterma/claudia2000/wiki/The-heart-of-the-internet
gitea.yantootech.com · April 4, 2026 at 12:42 am
References:
Best muscle gainer pill
References:
http://59.110.175.62:4322/tessawillson8
getchefpahadi.com · April 4, 2026 at 12:47 am
References:
Muscle build products
References:
http://111.4.75.238:12600/tomokosappingt
opensource.irext.net · April 4, 2026 at 1:00 am
References:
Danger of steroid use
References:
http://43.136.169.169:3000/tonischneider/toni2022/wiki/Evaluation+of+a+one-step+sample+preparation+protocol+for+analysis+of+total+serum+testosterone+by+LC+MS+MS.-
106.52.71.204 · April 4, 2026 at 1:09 am
References:
Meaning of steroids
References:
https://iamtube.jp/@carolemcalpine?page=about
https://yours-tube.com/@emmettbutler5?page=about · April 4, 2026 at 1:25 am
References:
Best steroid cycle for cutting
References:
https://gitea.shirom.me/mattclift7163
http://111.229.183.203/ · April 4, 2026 at 1:44 am
References:
Harmful effects of steroids
References:
http://app.venusroyale.date/@kandice6330273
http://wangbeibei.xyz · April 4, 2026 at 2:02 am
References:
Testosterone levels on steroids
References:
http://171.244.15.53:3000/temekarossi659
ccn-tv.news · April 4, 2026 at 2:11 am
References:
Legal hormones for muscle growth
References:
http://global.gwangju.ac.kr/bbs/board.php?bo_table=g0101&wr_id=2267006
https://gosvid.com/ · April 4, 2026 at 2:30 am
References:
Best stack for building muscle
References:
http://106.52.21.251:3000/augustpape7452
best cheap smoke online australia · April 4, 2026 at 11:02 pm
Australia Tobacconist Hub
The Contradiction of an Australian Cigarette Website: Health Advice vs. Sales
A website has appeared offering customers in Australia the option to purchase cigarettes and tobacco with home delivery. The website, which goes by Australia Tobacconist Hub, is full of mixed messages: aggressive marketing of budget tobacco products alongside disclaimers about the health risks of tobacco use.
Available Items
The platform’s main focus is people who smoke seeking lower prices. Examples from the catalogue include:
Double Happiness (?? ??) — $190 per block (10 packets x 20’s)
Manchester Sapphire Blue – Dubai Version — $220 per carton
Manchester Special Edition Flow Red (Dubai Version) — $250 per carton
Manchester Blue Crush (Dubai Version) — $250 per block
Dunhill Blue (UK Version) — $220 per carton
Dunhill Red – UK Edition — $190 per carton
Benson and Hedges Gold — $160 per block
Zhongnanhai brand — $180 per block
The seller highlights “low costs” (Cheap Tobacco Australia) and the availability of popular brands such as Marlboro, Manchester, Bossku, and Double Happiness.
Logistics and Payment
The seller advertises fast, reliable, and discreet delivery across Australia (Fast Tobacco Delivery Australia). They state that they take various payment options including bank transfer, USDT, PayPal, Wise, and more. Customer interaction is done via WhatsApp and email — a typical method in the grey or black market for online tobacco sales.
A Strange Contrast
Curiously enough, the identical platform that sells cigarettes (while formally warning that it is illegal to sell tobacco products to minors) also shows a “STOP SMOKING” image with an image of lungs crossed by a cigarette.
In a heading called “STOP TOBACCO”, the text states:
“Quitting isn’t easy, but every effort counts. Within minutes, your body starts recovering — and over time, your health and vitality return. Let’s start today!”
This public health message appears right next to a list of items for sale selling cartons for $160–$250 and a prompt to buy: “Buy Cigarettes Online in Australia at the Best Price.” Such double messaging is characteristic of unlicensed or “grey market” tobacco shops that try to feign social responsibility while still pushing harmful goods.
Potential Legal Problems
The text does not specify whether the seller possesses a valid Australian retail license for tobacco. Australia is known for having some of the strictest tobacco laws in the world, including standardised packaging rules and very large tobacco duties. The promise of low-cost smokes — especially “Dubai Edition” or “UK Version” — often indicates products that have evaded taxes, been brought in illegally, or are fake.
Final Thoughts
The online shop described above is a classic case of a shadow online tobacco business. It profits from smokers’ wish for cheaper prices in the face of Australia’s high legal tobacco taxes, while hiding behind empty health warnings and promises of good service. Potential buyers should remember that buying unlicensed tobacco carries not only legal risks but also a total absence of any assurance regarding product safety and authenticity.
platform.joinus4health.eu · April 5, 2026 at 9:31 am
References:
Instant Casino App
References:
https://www.adpost4u.com/user/profile/4392411
denimcatsup14.bravejournal.net · April 5, 2026 at 3:48 pm
References:
Echtgeld casino erfahrungen
References:
https://to-portal.com/peruapril67
obyavlenie.ru · April 5, 2026 at 4:03 pm
References:
Neue echtgeld casinos
References:
https://love-mattingly-3.blogbright.net/kartenspiele-mit-echtgeld
actualites.cava.tn · April 5, 2026 at 5:37 pm
References:
Michigan casinos
References:
https://aryba.kg/user/bitepruner6/
adrestyt.ru · April 5, 2026 at 6:01 pm
References:
Choctaw casinos
References:
https://codimd.communecter.org/D2g9WlhvRzSy6CEV6TQ6WA/
Australia Tobacconist Hub · April 5, 2026 at 7:21 pm
Australia Tobacconist Hub
The Contradiction of an Australian Cigarette Website: Health Advice vs. Sales
An online service has emerged offering Australians the ability to buy tobacco products with home delivery. The website, which calls itself Australia Tobacconist Hub, presents a striking contradiction: heavy promotion of budget tobacco products alongside official notices about the dangers of smoking.
Product Range
The platform’s main focus is people who smoke looking to save money. Key items on the price list include:
Double Happiness brand — $190 per carton (10 packets x 20’s)
Manchester Sapphire Blue (Dubai Edition) — $220 per carton
Manchester Special Edition Flow Red – Dubai Edition — $250 per block
Manchester Blue Crush (Dubai Version) — $250 per block
Dunhill Blue (UK Version) — $220 per block
Dunhill Red – UK Edition — $190 per carton
Benson & Hedges Gold — $160 per block
Zhongnanhai brand — $180 per carton
The seller emphasizes “low costs” (Cheap Tobacco Australia) and the availability of well-known names such as Marlboro, Manchester, Bossku, and Double Happiness.
Logistics and Payment
The seller promises fast, reliable, and discreet delivery across Australia (Fast Tobacco Delivery Australia). They say they process bank transfers, USDT (cryptocurrency), PayPal, Wise, and other methods. Customer contact is conducted via WhatsApp, email, and other messaging apps — a common practice in the unlicensed sector for online tobacco sales.
The Contradiction in Messaging
Curiously enough, the very same site that promotes tobacco sales (while formally warning that it is illegal to sell tobacco products to minors) also displays a “STOP SMOKING” graphic with an drawing of lungs crossed by a cigarette.
In a heading called “STOP TOBACCO”, the text states:
“Giving up smoking is hard, but each attempt matters. Within minutes, your body begins to heal — and over time, your health and vitality return. Begin your journey now!”
This public health message is placed near a product catalogue with prices from $160 to $250 per carton and a call to action: “Buy Cigarettes Online in Australia at the Best Price.” Such double messaging is common of illegal or semi-legal cigarette sellers that pretend to care about public health while still pushing harmful goods.
Legal Issues
The text does not specify whether the seller holds a valid Australian retail license for tobacco. Australia is known for having some of the strictest tobacco laws in the world, including plain packaging requirements and very large tobacco duties. The offer of “cheap” cigarettes — especially “Dubai Edition” or “UK Version” — often suggests untaxed, smuggled, or counterfeit goods.
Summary
The website in question is a classic case of a dark-market cigarette seller. It exploits smokers’ desire to save money in the face of Australia’s high legal tobacco taxes, while hiding behind superficial “Stop Smoking” slogans and claims of customer care. Those thinking of purchasing should keep in mind that buying unlicensed tobacco carries not only the chance of legal trouble but also a complete lack of quality or safety guarantees.
https://forum.issabel.org/u/versevinyl1 · April 5, 2026 at 8:27 pm
References:
Instant Casino Freispiele
References:
http://warblog.hys.cz/user/rainwrench4/
l1ae1d.творение.москва · April 6, 2026 at 1:06 am
References:
Instant Casino App iOS
References:
https://graph.org/Willkommensbonus-200-04-04
onlinevetjobs.com · April 6, 2026 at 5:46 am
References:
Gewinne bei Instant Casino auszahlen
References:
http://xn--l1ae1d.xn--b1agalyeon.xn--80adxhks/user/ocelotrake2/
https://bbs.pku.edu.cn/ · April 6, 2026 at 9:32 am
References:
Instant Casino Seriosität
References:
https://albrechtsen-thorup-4.hubstack.net/online-casino-mit-den-schnellsten-auszahlungen-in-deutschland
https://garrison-bonner.hubstack.net · April 6, 2026 at 2:09 pm
References:
Bestes online casino echtgeld
References:
https://zumpadpro.zum.de/bfDjNFUdTc2j3dpNfM7mGg/
Buy Medicube beauty devices online · April 6, 2026 at 4:54 pm
Korean skincare for glowing skin buy
ch-marine.co.kr · April 6, 2026 at 5:52 pm
References:
Female muscle enhancement
References:
https://guiacomercialsaopaulo.com/author/tamararobin/
guateempleos.com · April 6, 2026 at 6:52 pm
References:
Anabolic steroids side effects negative
References:
https://fanajobs.com/profile/carynburges710
https://companyjobs.cn/ · April 6, 2026 at 8:17 pm
References:
Legal steroids for sale uk
References:
https://jobmonster.co.nz/companies/get-testosterone-prescription-online/
itheadhunter.vn · April 6, 2026 at 8:58 pm
References:
Do steroids make you angry
References:
https://volunteeri.com/companies/where-can-i-buy-tren-safe-online-and-local-options/
manpowerassociation.in · April 6, 2026 at 10:21 pm
References:
How long have steroids been around
References:
https://realhire.co/employer/methandienone-10mg-50-tablets-medcare-pharma/
smallbusinessinternships.com · April 6, 2026 at 10:58 pm
References:
Legit steroid source
References:
http://globaldream.or.kr/bbs/board.php?bo_table=sub08_02&wr_id=294014
https://realhire.co/ · April 6, 2026 at 11:07 pm
References:
Best natural anabolic supplement
References:
https://sprohr.com/employer/8-best-testosterone-boosters-for-men-2026-updated/
jw-pension.com · April 6, 2026 at 11:38 pm
References:
How do bodybuilders get steroids
References:
https://jobcopeu.com/employer/how-to-get-trenbolone-safely-and-legally/
talentformation.net · April 7, 2026 at 12:51 am
References:
The understanding gender is permanent is called
References:
https://jandlfabricating.com/employer/how-to-buy-testosterone-online-clinics-trt-legal-options/
http://shinhwaspodium.com · April 7, 2026 at 2:01 am
References:
Female bodybuilding steroids pictures
References:
https://maxtravelagencys.com/employer/where-to-buy-trenbolone-what-you-need-to-know/
dev-members.writeappreviews.com · April 7, 2026 at 5:39 am
References:
Winstrom steroids
References:
http://www.rnthotel.kr/bbs/board.php?bo_table=com_bbs2&wr_id=21497
https://carrefourtalents.com/employeur/weight-loss-personalized-plans-online-prescriptions · April 7, 2026 at 5:58 am
References:
Legal supplements that work like steroids
References:
https://itheadhunter.vn/jobs/companies/13-best-websites-for-buying-glp-1s-for-weight-loss-in-2026/
pad.stuve.de · April 7, 2026 at 1:36 pm
References:
Steroid stacks for cutting
References:
https://timeoftheworld.date/wiki/Der_ultimative_Leitfaden_zum_Kauf_von_Dianabol_Wo_kaufen_247_is
https://santiago-templeton.technetbloggers.de · April 7, 2026 at 2:16 pm
References:
Testosteron Tabletten Testosteron steigern
References:
https://www.marocbikhir.com/user/profile/526043
cheap tobacco australia · April 7, 2026 at 2:24 pm
buy cigarettes online australia
Online Tobacco Sales in Australia: Between Health Warnings and “Cheap” Cigarettes
A website has appeared offering customers in Australia the ability to buy tobacco products with home delivery. The website, which operates under the name Australia Tobacconist Hub, presents a striking contradiction: heavy promotion of budget tobacco products alongside disclaimers about the dangers of smoking.
Available Items
The platform’s key customer base is smokers trying to cut costs. Key items on the price list include:
Double Happiness (?? ??) — $190 per block (10 packets x 20’s)
Manchester Sapphire Blue (Dubai Edition) — $220 per carton
Manchester Special Edition Flow Red – Dubai Edition — $250 per block
Manchester Blue Crush – Dubai Edition — $250 per carton
Dunhill Blue (UK Version) — $220 per block
Dunhill Red (UK Version) — $190 per carton
Benson & Hedges Gold — $160 per block
Zhongnanhai brand — $180 per block
The seller highlights “low costs” (Cheap Tobacco Australia) and the offering of well-known names such as Marlboro, Manchester, Bossku, and Double Happiness.
Logistics and Payment
The seller advertises quick, dependable, and private shipping across Australia (Fast Tobacco Delivery Australia). They state that they take various payment options including bank transfer, USDT, PayPal, Wise, and more. Customer communication is handled via WhatsApp, email, and other messaging apps — a typical practice in the grey or black market for internet cigarette shops.
A Strange Contrast
Curiously enough, the identical platform that promotes tobacco sales (while officially noting that selling to persons under 18 is illegal) also displays a “STOP SMOKING” banner with an illustration of lungs crossed by a cigarette.
In a heading called “STOP TOBACCO”, the text says:
“Quitting isn’t easy, but every effort counts. Within minutes, your body begins to heal — and as time goes by, your health and vitality return. Begin your journey now!”
This public health message is placed near a list of items for sale selling cartons for $160–$250 and a call to action: “Purchase cigarettes online in Australia for the lowest price.” Such mixed communication is common of unlicensed or “grey market” tobacco shops that try to feign social responsibility while still pushing harmful goods.
Legal Issues
The text does not specify whether the seller holds a valid Australian retail license for tobacco. Australia is recognised for some of the most severe cigarette regulations globally, including standardised packaging rules and extremely high excise taxes. The promise of low-cost smokes — especially “Dubai Edition” or “UK Version” — often points to untaxed, smuggled, or counterfeit goods.
Conclusion
The online shop described above is a classic case of a shadow online tobacco business. It profits from smokers’ wish for cheaper prices in the face of Australia’s expensive official cigarette prices, while masking itself with superficial “Stop Smoking” slogans and claims of customer care. Potential buyers should remember that buying unlicensed tobacco carries not only legal risks but also a complete lack of quality or safety guarantees.
oceanflat3.bravejournal.net · April 7, 2026 at 2:52 pm
References:
Steroid mean
References:
https://ccsakura.jp:443/index.php?planetbeggar29
https://actualites.cava.tn · April 7, 2026 at 3:42 pm
References:
Maca Wurzel Testosteron
References:
http://jobboard.piasd.org/author/thrillgarden47/
brewwiki.win · April 7, 2026 at 4:48 pm
References:
Testosteron Tabletten für Männer
References:
https://imoodle.win/wiki/Bestellen_Sie_Anavar_Oxandrolone_10_mg_Elbrus_Pharmaceuticals_online_in_Deutschland_fr_120_Legal_aus_OnlineApotheke
https://clashofcryptos.trade/ · April 7, 2026 at 4:53 pm
References:
Testosteronspiegel erhöhen Tabletten
References:
https://graph.org/Buy-Dianabol-Methandienone-Online-Lab-Tested–99-Purity-02-05-2
matkafasi.com · April 7, 2026 at 5:51 pm
References:
Stress abbauen Testosteron
References:
https://timeoftheworld.date/wiki/Human_Growth_Hormone_For_Injection_Market_Coverage_Analysis
opensourcebridge.science · April 7, 2026 at 6:55 pm
References:
Testosteron steigern Ernährung
References:
https://schoolido.lu/user/ramieleaf8/
https://squareblogs.net/nutjumper8/testosterone-for-women · April 7, 2026 at 7:11 pm
References:
Testosteron Tabletten optimieren
References:
https://yogaasanas.science/wiki/Bestes_Abnehmmittel_Stiftung_Warentest_Testsieger_2025
www.hulkshare.com · April 8, 2026 at 6:55 am
References:
Steroid perscription
References:
https://clashofcryptos.trade/wiki/How_to_Choose_the_Best_TRT_Clinic_San_Diego_for_Optimal_Hormone_Health_in_2026
pin-it.top · April 8, 2026 at 6:59 am
References:
Long term side effects of corticosteroids
References:
https://dancerincome3.bravejournal.net/clenbuterol-fettkiller-oder-gefahrliches-dopingmittel
https://mes-favoris.site/item/597095 · April 8, 2026 at 7:08 am
References:
Bulking stack bodybuilding
References:
https://nhadat24.org/author/attackstorm7
enouvelles.space · April 8, 2026 at 7:37 am
References:
Steroids and depression side effects
References:
https://mmcon.sakura.ne.jp:443/mmwiki/index.php?singdrive24
a-taxi.com.ua · April 8, 2026 at 8:16 am
References:
Best legal steroid
References:
https://pad.stuve.de/s/693EfKf5f
thethoughtfodder.com · April 8, 2026 at 8:48 am
References:
Best cycle for lean mass
References:
https://gratisafhalen.be/author/sharoncoal67/
lynn-ottosen-2.hubstack.net · April 8, 2026 at 1:35 pm
References:
Steroids for headaches
References:
https://elclasificadomx.com/author/coachrocket27/
hedgedoc.eclair.ec-lyon.fr · April 8, 2026 at 1:55 pm
References:
Anabolic vs catabolic steroids
References:
http://karayaz.ru/user/cubcougar55/
https://www.hulkshare.com · April 8, 2026 at 1:59 pm
References:
Anabolic powder
References:
https://md.un-hack-bar.de/s/B9jBFQDK82
http://techou.jp/index.php?maracabarge1 · April 8, 2026 at 2:43 pm
References:
Best anavar brand
References:
https://pads.jeito.nl/s/yW69Yeua1j
mozillabd.science · April 8, 2026 at 2:54 pm
References:
Foods that contain steroids
References:
https://telegra.ph/Abnehm-Produkte-Test-2025-02-06-2
toxicdolls.com · April 8, 2026 at 2:56 pm
References:
Best steroids to get ripped
References:
https://md.swk-web.com/s/VdDWVVtC1
Australia Tobacconist Hub · April 8, 2026 at 3:39 pm
cheap cigarettes in australia
An Online Service Offers Australians Tobacco – But Also “Stop Smoking” Messages
A website has appeared offering Australian residents the ability to buy tobacco products with home delivery. The website, which calls itself Australia Tobacconist Hub, is full of mixed messages: heavy promotion of cheap cigarettes alongside disclaimers about the health risks of tobacco use.
Available Items
The platform’s primary focus is smokers trying to cut costs. Examples from the catalogue include:
Double Happiness (?? ??) — $190 per carton (10 packets x 20’s)
Manchester Sapphire Blue (Dubai Edition) — $220 per carton
Manchester Special Edition Flow Red – Dubai Edition — $250 per carton
Manchester Blue Crush – Dubai Edition — $250 per block
Dunhill Blue (UK Version) — $220 per block
Dunhill Red – UK Edition — $190 per block
Benson and Hedges Gold — $160 per carton
Zhongnanhai (???) — $180 per carton
The seller emphasizes “low costs” (Cheap Tobacco Australia) and the presence of well-known names such as Marlboro, Manchester, Bossku, Double Happiness, and others.
Logistics and Payment
The seller advertises quick, dependable, and private shipping across Australia (Fast Tobacco Delivery Australia). They state that they take various payment options including bank transfer, USDT, PayPal, Wise, and more. Customer communication is handled via WhatsApp, email, and other messaging apps — a standard practice in the unlicensed sector for online tobacco sales.
A Strange Contrast
Remarkably, the very same site that sells cigarettes (while formally warning that selling to persons under 18 is illegal) also displays a “STOP SMOKING” graphic with an illustration of a cigarette passing through human lungs.
In a part named “STOP TOBACCO”, the text states:
“Quitting isn’t easy, but every effort counts. Within minutes, your body starts recovering — and over time, your health and energy come back. Let’s start today!”
This anti-smoking advice is placed near a product catalogue selling cartons for $160–$250 and a call to action: “Purchase cigarettes online in Australia for the lowest price.” Such hypocrisy is common of illegal or semi-legal cigarette sellers that try to feign social responsibility while continuing to sell addictive products.
Legal Issues
The text leaves unclear whether the seller holds a valid Australian retail license for tobacco. Australia is known for having some of the strictest tobacco laws in the world, including standardised packaging rules and very large tobacco duties. The promise of low-cost smokes — especially “Dubai Edition” or “UK Version” — often suggests untaxed, smuggled, or counterfeit goods.
Summary
The online shop described above is a clear illustration of a shadow online tobacco business. It exploits smokers’ desire to save money in the context of Australia’s high legal tobacco taxes, while masking itself with superficial “Stop Smoking” slogans and promises of good service. Those thinking of purchasing should keep in mind that buying unlicensed tobacco carries not only the chance of legal trouble but also a total absence of any assurance regarding product safety and authenticity.
https://digitaltibetan.win/wiki/Post:I_Went_on_a_Quest_to_Fix_My_Metabolism_Heres_What_I_Learned · April 8, 2026 at 4:08 pm
References:
Body beast womens review
References:
https://hedge.fachschaft.informatik.uni-kl.de/s/lfirzByUm
historydb.date · April 8, 2026 at 4:33 pm
References:
Steroids for endurance athletes
References:
https://menwiki.men/wiki/Top_5_Best_HGH_Supplements_That_Actually_Work
pads.jeito.nl · April 8, 2026 at 5:30 pm
References:
Buy online steroids
References:
https://p.mobile9.com/turretgold7/
https://pad.stuve.uni-ulm.de/s/uSOTkFu8m · April 8, 2026 at 5:41 pm
References:
Dianabol steroids for sale
References:
https://yilmaz-kjer-3.blogbright.net/clenbuterol-200-mcg-x-30ml-liquid
http://king-wifi.win//index.php?title=erichsenpaaske5415 · April 8, 2026 at 7:07 pm
References:
Creatine steroid
References:
https://md.swk-web.com/s/c9QnM1Q4I
stougaard-aagesen-4.blogbright.net · April 8, 2026 at 7:08 pm
References:
Legal weight gain steroids
References:
https://dreevoo.com/profile.php?pid=1058654
matkafasi.com · April 8, 2026 at 7:18 pm
References:
Bodybuilding steroid alternatives
References:
https://pikidi.com/seller/profile/dustperu20
dreevoo.com · April 8, 2026 at 8:34 pm
References:
Effect of steroids
References:
https://rrclassifieds.com/user/profile/9116
JULESLOT · April 8, 2026 at 10:15 pm
JULESLOT
king-wifi.win · April 8, 2026 at 11:42 pm
References:
Women and steroids
References:
https://md.un-hack-bar.de/R8vzvF19QvysCENRX4-u0Q/
부산호빠 · April 9, 2026 at 1:57 am
부산호빠
pads.jeito.nl · April 9, 2026 at 11:44 am
References:
People who use steroids
References:
http://humanlove.stream//index.php?title=rivasabernathy3330
output.jsbin.com · April 9, 2026 at 2:39 pm
References:
mozillabd.science
References:
https://aryba.kg/user/starttennis3/
prpack.ru · April 9, 2026 at 4:15 pm
References:
Anabolic steroids info
References:
http://downarchive.org/user/foxtaurus7/
https://funsilo.date/wiki/How_to_Take_Clenbuterol_A_Beginners_Guide_to_Safe_and_Effective_Use · April 9, 2026 at 7:35 pm
References:
Roid definition
References:
https://travelersqa.com/user/malletdish90
ラブドール · April 10, 2026 at 1:13 am
トルソー 型 ラブドール こんにちは、今週末は私をサポートしてくれて嬉しいです。なぜなら、この時点で私はこの素晴らしい教育記事を私の家で読んでいるからです。これは、ダッチワイフがいくつかの援助を貸すことができる場所です。
AI moderation · April 10, 2026 at 1:48 am
social features
many teams are now thinking about building a community layer inside the app
when conversation stays inside the platform, retention improves
owning the social layer helps protect both audience and data
in-app communities turn a product from a utility into a gathering place
AI moderation helps keep live chat usable during peak moments
integrated assistants reduce the need for users to leave the app for answers
a strong community layer can transform casual viewers into loyal supporters
Natural Skincare · April 10, 2026 at 3:34 am
safe skincare products without chemicals
www.24propertyinspain.com · April 10, 2026 at 7:25 am
References:
Corticosteroids meds
References:
http://humanlove.stream//index.php?title=holcombwall0306
okprint.kz · April 10, 2026 at 8:37 am
References:
Rich piana steroids
References:
https://doc.adminforge.de/s/hRgBznFDOH
hack.allmende.io · April 10, 2026 at 2:47 pm
References:
Anabolic steroids definition
References:
https://servodriven.com/forums/users/factoboe4/
41-4lcpj.укр · April 10, 2026 at 6:03 pm
References:
Lean mode powder
References:
https://adsintro.com/index.php?page=user&action=pub_profile&id=787195
alushta-shirak.ru · April 10, 2026 at 10:14 pm
References:
https://youralareno.com
References:
https://md.swk-web.com/s/up0hcPXYn
http://alfa-power.de · April 10, 2026 at 10:47 pm
References:
What are steroids made out of
References:
https://skitterphoto.com/photographers/2611647/lindberg-hirsch
blaze · April 11, 2026 at 12:56 am
Thanks in favor of sharing such a nice thought, post is pleasant,
thats why i have read it entirely
medibang.com · April 11, 2026 at 10:17 am
References:
Buy anabolic steroids
References:
https://postheaven.net/fighttaiwan6/dianabol-danabol-masseaufbau-online-kaufen-deutschland
topbookmarks.xyz · April 11, 2026 at 12:59 pm
References:
Steroid for sale online
References:
https://www.udrpsearch.com/user/costcycle3
md.chaosdorf.de · April 11, 2026 at 2:41 pm
References:
Buy steroid powder
References:
https://pad.karuka.tech/s/N_2nEyFpU
molchanovonews.ru · April 11, 2026 at 4:52 pm
References:
Legal steroid like supplements
References:
http://alfa-power.de/member.php?action=profile&uid=9266
https://eujobss.com · April 12, 2026 at 6:06 pm
References:
Steroid muscle builder
References:
https://job.dialnumber.in/profile/erlindahedrick
https://prpack.ru · April 12, 2026 at 9:44 pm
References:
Best non-steroid supplements
References:
https://pattern-wiki.win/wiki/Bringen_Wachstumshormone_was_Wachstum_Erfahrungen_Hormone
platform.joinus4health.eu · April 12, 2026 at 9:46 pm
References:
Does steroids stunt growth
References:
http://amur.1gb.ua/user/dustmask03/
fakenews.win · April 13, 2026 at 1:18 pm
References:
Bestes online casino echtgeld
References:
https://sibze.ru/index.php?subaction=userinfo&user=pintowl0
sciencewiki.science · April 13, 2026 at 3:53 pm
References:
Seriöse Online Casinos Echtgeld
References:
https://md.un-hack-bar.de/s/25B_ptUdcv
skitterphoto.com · April 13, 2026 at 5:30 pm
References:
Echtgeld Casino mit Startguthaben
References:
https://tran-storm.blogbright.net/beste-book-of-ra-casinos-legal-den-novoline-slot-um-echtgeld-spielen
https://pape-binderup-2.thoughtlanes.net/ · April 13, 2026 at 9:41 pm
References:
Online Casino Echtgeld Erfahrung
References:
https://pad.karuka.tech/s/1w75ne4_0
https://enregistre-le.site/ · April 13, 2026 at 11:32 pm
References:
Online Casino Echtgeld schnellste Auszahlung
References:
http://okprint.kz/user/soundtuna03/
classifieds.ocala-news.com · April 14, 2026 at 4:22 am
References:
Bestes online casino echtgeld
References:
https://tvoyaskala.com/user/jamcongo0/
digitaltibetan.win · April 14, 2026 at 9:14 am
References:
Online Casino Echtgeld schnellste Auszahlung
References:
https://www.webhostingask.com/member.php?action=profile&uid=54262
imoodle.win · April 14, 2026 at 9:44 am
References:
Where can i buy trenbolone
References:
https://fakenews.win/wiki/Trenbolone_Buy_Tips_Pricing_Guide
https://yogicentral.science/wiki/Find_Trenbolone_For_Sale_Online · April 14, 2026 at 10:22 am
References:
Pros and cons of testosterone injections for bodybuilding
References:
https://mozillabd.science/wiki/Where_to_Buy_Trenbolone_Safely
imoodle.win · April 14, 2026 at 10:50 am
References:
Trenbolone vial price
References:
https://timeoftheworld.date/wiki/How_To_Buy_Trenbolone_Safely
gratis binance-konto · April 14, 2026 at 6:42 pm
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://www.binance.info/register?ref=IXBIAFVY
sweet-bonanza-1000-demo · April 15, 2026 at 4:00 am
Jogo do Tigrinho continua forte, mas a disputa com Ox e Rabbit está mais equilibrada nesta semana.
hack.allmende.io · April 15, 2026 at 1:17 pm
References:
Treasure island casino mn
References:
https://graph.org/Rocketplay-Casino-Claim-Your-Neosurf-Bonus-04-15
www.youtube.com · April 15, 2026 at 1:31 pm
References:
Energy casino
References:
https://pad.stuve.de/s/lCmG9WTbXn
matkafasi.com · April 15, 2026 at 2:08 pm
References:
Women bodybuilders on steroids
References:
https://app.readthedocs.org/profiles/ravenswan3/
codimd.communecter.org · April 15, 2026 at 6:57 pm
References:
Female steroids before and after
References:
https://pad.stuve.de/s/-2cgeRcP5A
https://notes.bmcs.one/ · April 16, 2026 at 12:39 am
References:
Ohio casino control commission
References:
https://letterscene1.werite.net/merkur-casino-echtgeld-spiele-and-gewinne
http://newbielearningcenter.com/ · April 16, 2026 at 5:28 pm
References:
Europa casino download
References:
https://wzisuzu.com/xinwen-zixun/bai-wan-re-tie-huang-ma-da-v-bo-zhu-hui-ji-ba-sa-tv-mo-de-li-qi-6-ou-guan-ba-sa-5-ou-guan/
https://alternative.media · April 17, 2026 at 10:09 am
References:
Lady luck casino pa
References:
https://preventingsuicide.in/how-a-simple-act-of-kindness-can-change-someones-life-forever/
https://lokeshvattigunta.co.in/2023/06/22/the-art-of-negotiation-tips-for-successful-business-deals · April 17, 2026 at 11:39 am
References:
Online roulette game
References:
https://ilanabilingualschool.com/tiny-tot-adventures-a-peek-into-our-preschool-world/
http://gk2a.com · April 17, 2026 at 12:03 pm
References:
Casino games slots
References:
https://scenario-center.com/cgi-bin/simbbsex.cgi/simbbsex.cgi/1win14043.ru
https://zereg.mn/61630 · April 17, 2026 at 1:04 pm
References:
Egyptian treasures
References:
https://magiamgia.blog.fc2.com/blog-entry-36400.html
slots-alta-volatilidade-pg-soft · April 17, 2026 at 2:16 pm
A comunidade valorizou consistência acima de narrativas exageradas.
mo.investkuban.ru · April 17, 2026 at 5:47 pm
References:
Pockie ninja 2
References:
http://yashichi.com/sashimi001-360×240/
sabarinews.com · April 17, 2026 at 6:46 pm
References:
Slot machine manufacturers
References:
https://sarah-cosmetics.com/we-create-careers-and-open-new-posibbilities-for-our-clients/
gitea.dsmaster.myds.me · April 17, 2026 at 7:09 pm
play online games 3d
https://git.rmarl.in/otisheritage1 git.rmarl.in
https://niqnok.com/nicolasmartins niqnok.com
https://gitea.primecontrols-dev.com/kraigpriestley gitea.primecontrols-dev.com
https://datingmywish.com/@beulahspoffort https://datingmywish.com/@beulahspoffort
https://www.k0ki-dev.de/latishabrandt https://www.k0ki-dev.de/latishabrandt
https://codes.tools.asitavsen.com/lilab769425097 codes.tools.asitavsen.com
https://yourclipz.com/@glindaberube5?page=about https://yourclipz.com/@glindaberube5?page=about
https://mygit.kikyps.com/rachelmadrid73 https://mygit.kikyps.com/rachelmadrid73
https://codes.tools.asitavsen.com/lilab769425097 https://codes.tools.asitavsen.com/lilab769425097
https://whiskey.tangomedia.fr/@laurenceeames2?page=about https://whiskey.tangomedia.fr/
https://gitea.lasallesaintdenis.com/heikeb98068946 https://gitea.lasallesaintdenis.com/
https://vydiio.com/@logan89159783?page=about vydiio.com
http://www.xngel.com/@opflemuel67702?page=about http://www.xngel.com/@opflemuel67702?page=about
https://i10audio.com/suzannelyall66 i10audio.com
https://git.rmarl.in/otisheritage1 https://git.rmarl.in
https://greenopps420.com/@eegboris626318?page=about greenopps420.com
https://dev3.worldme.tv/@angelineschmit?page=about https://dev3.worldme.tv/
https://k0ki-dev.com/keenanibr67348 k0ki-dev.com
References:
https://qdate.ru/@leonoreberkman
naijasingles.net · April 17, 2026 at 7:51 pm
kansas star casino
https://quickdatescript.com/@kjaalda6089866 quickdatescript.com
http://git.zxkedu.com:33769/coygodfrey2046 http://git.zxkedu.com/
https://play.ophirstudio.com//@hwadominic9536?page=about https://play.ophirstudio.com/
https://itimez.com/@noahchambliss5?page=about https://itimez.com/@noahchambliss5?page=about
https://myhealthypunjab.com/@ipkramiro8359?page=about myhealthypunjab.com
https://funnyutube.com/@ethanfinsch65?page=about https://funnyutube.com/
http://spnewstv.com/@karinagilmore6?page=about http://spnewstv.com/
https://git.0935e.com/lemuelrittenho https://git.0935e.com
https://funnyutube.com/@belenault9953?page=about funnyutube.com
https://git.0935e.com/lemuelrittenho https://git.0935e.com/lemuelrittenho
https://hiwifi.denq.us:8418/fayesemmens09 https://hiwifi.denq.us/
https://channel-u.tv/@ibcvirgilio68?page=about channel-u.tv
https://www.jo-line.eu/georgiajoske36 http://www.jo-line.eu
https://vcs.cozydsp.space/laureneelsberr vcs.cozydsp.space
https://git.dieselor.bg/muoihampden94 git.dieselor.bg
https://romancefrica.com/@alfonzo91f573 https://romancefrica.com/
https://www.bongmedia.tv/@modestogolden?page=about bongmedia.tv
https://124.70.144.1/madelinefewing 124.70.144.1
References:
https://thefusionflix.com/@calebsavage520?page=about
video.silverwolfstudios.com · April 17, 2026 at 7:53 pm
indian casinos
https://tcodpractice.com/mirtahatten056 tcodpractice.com
https://git.louislabs.com/meistevens124 git.louislabs.com
https://gitea.nacsity.cn/adelaidadonnit https://gitea.nacsity.cn/adelaidadonnit
https://volts.howto.co.ug/@gaypqw9837172 volts.howto.co.ug
https://platform.giftedsoulsent.com/danatoney46542 https://platform.giftedsoulsent.com/danatoney46542
https://hero-cloud-stg-code.cnbita.com/elouisemcgee93 https://hero-cloud-stg-code.cnbita.com
https://eduback.com/@terrelldonoghu?page=about https://eduback.com/@terrelldonoghu?page=about
https://isugar-dating.com/@chasity005973 isugar-dating.com
https://gitea.zachl.tech/violet7867670 https://gitea.zachl.tech/violet7867670
https://theudtaullu.com/@flynnmcdonald?page=about theudtaullu.com
https://music.1mm.hk/kandisf3324715 music.1mm.hk
https://gitea.waterworld.com.hk/deanap47911441 gitea.waterworld.com.hk
https://git.gonethome.id/roxiemickens17 https://git.gonethome.id
https://getskill.work/jeniferi03474 getskill.work
https://git.suo0.com/alyciawuo47982 git.suo0.com
https://myafritube.com/@chiquitademers?page=about https://myafritube.com
https://funnyutube.com/@belenault9953?page=about https://funnyutube.com
https://codes.tools.asitavsen.com/bennettvelazqu https://codes.tools.asitavsen.com
References:
https://kition.mhl.tuc.gr/bebemcness5744
www.godhip.com · April 17, 2026 at 7:57 pm
mt airy casino
https://katambe.com/@felixnixon568 katambe.com
http://musicstreaming.yonetsystems.com/mavisnicholson http://musicstreaming.yonetsystems.com/mavisnicholson
https://lius.familyds.org:3000/alana375816079 lius.familyds.org
https://git.alderautomation.ca/curtisokeeffe0 https://git.alderautomation.ca/curtisokeeffe0
https://lafffrica.com/@rosalynfitch3?page=about lafffrica.com
https://shiatube.org/@mosebeem006222?page=about shiatube.org
https://i.megapollos.com/@alannahawthorn?page=about i.megapollos.com
https://quickdatescript.com/@roryculp48987 quickdatescript.com
https://sing.ibible.hk/@amparoandrzeje?page=about sing.ibible.hk
https://bigotube.com/@joanzinn573766?page=about bigotube.com
https://tunelifystream.com/romainehoolan tunelifystream.com
https://git.dieselor.bg/terrancegillin git.dieselor.bg
https://gitea.ww3.tw/kathrinzeal622 gitea.ww3.tw
https://hipstrumentals.net/darell40205028 hipstrumentals.net
https://allyoutubes.com/@alfredomahan95?page=about allyoutubes.com
https://www.oddmate.com/@pasqualestrode http://www.oddmate.com
https://gitea.cfpoccitan.org/nicoleseeley1 gitea.cfpoccitan.org
https://gitea.shizuka.icu/mickivanotterl gitea.shizuka.icu
References:
https://blackvision.co.uk/@vanbracken827?page=about
flirta.online · April 17, 2026 at 8:15 pm
peppermill casino reno nv
https://financevideosmedia.com/@alphonso56y256?page=about financevideosmedia.com
http://git.yanei-iot.com:600/emilieefa97124 git.yanei-iot.com
https://mginger.org/@samanthakty572 mginger.org
https://www.latflex.net/@niklasricketts?page=about https://www.latflex.net/@niklasricketts?page=about
https://music.wzsipku.cn/edwinaliston73 music.wzsipku.cn
https://goondepot.com/@indiamatney23?page=about goondepot.com
https://git.privezishop.ru/alannawickens3 git.privezishop.ru
https://digitalafterlife.org/@carinmcquay893?page=about https://digitalafterlife.org/
https://alurmusic.com/javierlarsen9 alurmusic.com
https://nildigitalco.com/@alejandrinawes?page=about https://nildigitalco.com/@alejandrinawes?page=about
https://yooverse.com/@jonansell63337 https://yooverse.com/@jonansell63337
https://git.scinalytics.com/lorengoss8086 git.scinalytics.com
https://musiciansportal.ru/veroniquewolak https://musiciansportal.ru
https://21pac.com/@ezrawood19187?page=about 21pac.com
https://gitea-inner.fontree.cn/zanemaguire785 gitea-inner.fontree.cn
http://git.mynas71.myds.me/genevievemasco git.mynas71.myds.me
http://gitlab.dev.jtyjy.com/gisellesalkaus gitlab.dev.jtyjy.com
https://uk4mag.co.uk/video/@matildastleon?page=about https://uk4mag.co.uk/video/@matildastleon?page=about
References:
https://124.70.144.1/margaretafitzp
www.jo-line.eu · April 17, 2026 at 8:32 pm
hollywood casinos
http://www.xngel.com/@opflemuel67702?page=about http://www.xngel.com
http://dev-gitlab.dev.sww.com.cn/mariokashiwagi dev-gitlab.dev.sww.com.cn
https://gitea.pnkx.top:8/margaritaferre gitea.pnkx.top
https://ns2.asso-web.com/darwinevatt88 ns2.asso-web.com
https://git.htns.com/keenantorpy999 https://git.htns.com/
https://myclassictv.com/@margarettev78?page=about myclassictv.com
https://bantooplay.com/@jerrodlangley?page=about bantooplay.com
https://datingmywish.com/@louellasoliz79 datingmywish.com
https://21pac.com/@ezrawood19187?page=about https://21pac.com/@ezrawood19187?page=about
https://www.ikaros.asia/phyllisjordon http://www.ikaros.asia
https://gitea.diputadosalta.gob.ar/zelma392827797 gitea.diputadosalta.gob.ar
https://gitea.johannes-hegele.de/adriennebrunne gitea.johannes-hegele.de
https://cameotv.cc/@mamiemickens71?page=about cameotv.cc
https://hellomusic.app/alvapaine1789 hellomusic.app
https://yaseen.tv/@guillermomcalp?page=about https://yaseen.tv/
https://nildigitalco.com/@alejandrinawes?page=about https://nildigitalco.com
https://git.hanumanit.co.th/sherrillmessne git.hanumanit.co.th
https://video.2yu.co/@zeldacundiff98?page=about https://video.2yu.co/@zeldacundiff98?page=about
References:
https://gitea.coderpath.com/jannabosley069
flirta.online · April 17, 2026 at 8:32 pm
san francisco casinos
https://gitea.goldendeliverer.com/margaritamclau gitea.goldendeliverer.com
https://abadeez.com/@stephaniegoff?page=about https://abadeez.com/@stephaniegoff?page=about
https://git.freno.me/pabloertel3783 git.freno.me
https://www.lizyum.com/@mckenziewekey https://www.lizyum.com
https://katambe.com/@thadpippin758 katambe.com
https://hellomusic.app/alvapaine1789 hellomusic.app
https://645123.com/@zellacasey298?page=about 645123.com
https://vila.go.ro/violaabe217034 vila.go.ro
https://gitea.coderpath.com/caitlyngleason gitea.coderpath.com
https://21pac.com/@myrtiszavala2?page=about https://21pac.com/@myrtiszavala2?page=about
https://videyme.online/@dessie21j48582?page=about https://videyme.online/@dessie21j48582?page=about
https://yours-tube.com/@silasvanburen4?page=about https://yours-tube.com/
https://gitea.johannes-hegele.de/lateshamoncrie https://gitea.johannes-hegele.de/lateshamoncrie
https://git.freno.me/pabloertel3783 git.freno.me
https://ccn-tv.news/@maureenmcclure?page=about ccn-tv.news
https://cash.com.tr/@louielemus3697?page=about https://cash.com.tr
https://git.refinementservices.com/bartbanvard497 https://git.refinementservices.com/bartbanvard497
https://www.uria.dev/liliaschuster http://www.uria.dev
References:
https://itimez.com/@jamilaspears46?page=about
https://liverights.org//@paulescobar853?page=about · April 17, 2026 at 8:44 pm
android spinner style
https://truesecret.org/@youngraposo011?page=about truesecret.org
https://liverights.org//@paulescobar853?page=about liverights.org
https://video.2yu.co/@harrishollinwo?page=about https://video.2yu.co/@harrishollinwo?page=about
https://git.archieri.fr/vondarcy239523 git.archieri.fr
https://vydiio.com/@edlshana617193?page=about vydiio.com
http://musicstreaming.yonetsystems.com/lonniewise8924 musicstreaming.yonetsystems.com
https://tubepeer.com/@christineorlan?page=about tubepeer.com
https://eduback.com/@gregblum730412?page=about https://eduback.com/@gregblum730412?page=about
https://git.econutrix.com/gialfk43702370 git.econutrix.com
https://gitlab-rock.freedomstate.idv.tw/francespethard https://gitlab-rock.freedomstate.idv.tw/francespethard
https://gitea.wuyuank.com/qerjenna519200 https://gitea.wuyuank.com/
http://code.sz-chaohui.cn/hildegardsheff code.sz-chaohui.cn
https://music.1mm.hk/dinahe3217674 music.1mm.hk
https://dating.vi-lab.eu/@armandofremont https://dating.vi-lab.eu/@armandofremont
https://gitea.shizuka.icu/hectordoolan75 gitea.shizuka.icu
https://gitea.amazingcoders.com/tandyheine0813 gitea.amazingcoders.com
https://video.silverwolfstudios.com/@jaxonmartino79?page=about video.silverwolfstudios.com
https://dreamplacesai.de/trudicorso6114 https://dreamplacesai.de
git.mana-web.com · April 17, 2026 at 9:18 pm
rivers casino pittsburgh pa
https://iesoundtrack.tv/@horaciogarber?page=about https://iesoundtrack.tv/
https://lishan148.synology.me:3014/doyleburks6440 lishan148.synology.me
https://iamtube.jp/@margaritoskinn?page=about iamtube.jp
https://gitea.amazingcoders.com/tandyheine0813 gitea.amazingcoders.com
https://gitea.cfpoccitan.org/nicoleseeley1 gitea.cfpoccitan.org
https://dianyanai.com/virgieball9437 https://dianyanai.com/
https://vila.go.ro/stanleyporteou https://vila.go.ro/stanleyporteou
https://camtalking.com/@valentinashley camtalking.com
https://git.hanumanit.co.th/moniquedelatte git.hanumanit.co.th
https://lawrencewilbert.com/read-blog/40409_jumers-casino.html lawrencewilbert.com
https://music.crone.es/@muhammadleclai?page=about https://music.crone.es/@muhammadleclai?page=about
https://www.ohovideo.com/@jodyckx3738230?page=about http://www.ohovideo.com
https://www.sportstvvideo.com/@franciscagraha?page=about http://www.sportstvvideo.com
https://dotvdo.com/@christinkuster?page=about dotvdo.com
http://gitlab.dev.jtyjy.com/gisellesalkaus http://gitlab.dev.jtyjy.com/gisellesalkaus
https://gitea.jobiglo.com/jesschamplin2 https://gitea.jobiglo.com/
https://git.autotion.net/mohammedgosse git.autotion.net
https://git.apextoaster.com/allanbaader53 git.apextoaster.com
References:
http://www.tm-jikayo.com/keeleytoups26
https://rsas.de/shalandawaid91 · April 17, 2026 at 9:35 pm
References:
Fiat 500 blackjack
References:
https://git.privezishop.ru/alannawickens3
play.talkdrove.cc.nf · April 17, 2026 at 9:58 pm
References:
Grey eagle casino calgary
References:
https://li1420-231.members.linode.com/jamelivory213
volts.howto.co.ug · April 17, 2026 at 10:07 pm
roulette hot
https://ceedmusic.com/kristie32m858 ceedmusic.com
https://git.warze.org/meghanspurgeon git.warze.org
https://gitea.dsmaster.myds.me/eddychewings0 https://gitea.dsmaster.myds.me
https://yaseen.tv/@wsdmathew13351?page=about yaseen.tv
https://aprileaton.net/carlton0348032 https://aprileaton.net/
https://myafritube.com/@darylstephen12?page=about https://myafritube.com/@darylstephen12?page=about
https://www.livecima.com/@anthonymabe898?page=about https://www.livecima.com/
https://chinami.com/@bradgiffen6002?page=about chinami.com
https://git.clickforadventure.co/norbertopennin git.clickforadventure.co
http://git.fbonazzi.it/maricruzayres git.fbonazzi.it
https://git.clubeye.net/fannietroiano6 git.clubeye.net
https://gitea.coderpath.com/caitlyngleason gitea.coderpath.com
https://www.livecima.com/@anthonymabe898?page=about https://www.livecima.com/@anthonymabe898?page=about
https://yaseen.tv/@wsdmathew13351?page=about https://yaseen.tv/@wsdmathew13351?page=about
https://isugar-dating.com/@roderick604581 isugar-dating.com
https://greenopps420.com/@jewelcastello4?page=about https://greenopps420.com/@jewelcastello4?page=about
https://www.howeasynetwork.com/@mirtaenyeart22?page=about http://www.howeasynetwork.com
https://www.streemie.com/@jkeharlan51081?page=about http://www.streemie.com
References:
https://www.latflex.net/@hazeli76016347?page=about
https://gitea.pnkx.top/ · April 17, 2026 at 10:22 pm
olg slots
http://git.ibossay.com:3000/odellz11297861 git.ibossay.com
https://gitea-inner.fontree.cn/wilburnsiebenh gitea-inner.fontree.cn
https://maru.bnkode.com/@mattieaur75536 https://maru.bnkode.com/@mattieaur75536
https://gitea.jnyuxia.com/isabellalinare gitea.jnyuxia.com
http://tfjiang.cn:32773/pgkdenisha7633 http://tfjiang.cn
https://myafritube.com/@darylstephen12?page=about myafritube.com
https://gitea.diputadosalta.gob.ar/zelma392827797 https://gitea.diputadosalta.gob.ar/zelma392827797
https://shamrick.us/maryellennall9 https://shamrick.us/maryellennall9
http://git.qniao.cn/gladisnewcombe git.qniao.cn
https://demo.playtubescript.com/@holliesimpkins?page=about demo.playtubescript.com
https://datingmywish.com/@louellasoliz79 datingmywish.com
https://git.kooera.com/beatrice43i06 https://git.kooera.com/beatrice43i06
https://git.dinsor.co.th/birgits1405097 https://git.dinsor.co.th/birgits1405097
https://gitea.scivigi.com/johnathanferri gitea.scivigi.com
https://gitea.zachl.tech/kellieliddell gitea.zachl.tech
https://hellomusic.app/traceewao42314 hellomusic.app
https://gitea.wuyuank.com/vilma050576409 gitea.wuyuank.com
https://git.huwhy.cn/pearline51u394 https://git.huwhy.cn/
References:
https://megastream.pl/@dessieojk6310?page=about
https://www.howeasynetwork.com · April 17, 2026 at 10:26 pm
aliante casino las vegas
https://gitea.yantootech.com/dietermileham4 gitea.yantootech.com
https://git.sunlix.one/redai35207943 git.sunlix.one
https://dimen.krd/@kandishorsley?page=about dimen.krd
https://klimaexpress-tube.de/@troyconlan141?page=about klimaexpress-tube.de
https://git.mana-web.com/lauri735180511 https://git.mana-web.com/lauri735180511
https://git.vhdltool.com/jessikax51460 https://git.vhdltool.com/jessikax51460
https://beatsong.app/johniemckeon97 beatsong.app
https://daterondetjolie.fr/@demetriaconger https://daterondetjolie.fr/
http://git.fbonazzi.it/maricruzayres git.fbonazzi.it
https://gitea.zachl.tech/kellieliddell https://gitea.zachl.tech/kellieliddell
https://demo.playtubescript.com/@dixie52h855010?page=about demo.playtubescript.com
https://i.megapollos.com/@alannahawthorn?page=about i.megapollos.com
http://gitea.jb1000.com:88/carrilapine079 http://gitea.jb1000.com/
https://git.miasma-os.com/celestebrinson git.miasma-os.com
https://allyoutubes.com/@alfredomahan95?page=about allyoutubes.com
https://ott.saikatinfotech.com/@louellawhitlam?page=about ott.saikatinfotech.com
https://clipbeans.com/@dustyglenny24?page=about https://clipbeans.com/@dustyglenny24?page=about
https://quickdatescript.com/@kjaalda6089866 https://quickdatescript.com
References:
http://gitea.mikarsoft.com/thadlemieux837
fanlibo.i234.me · April 17, 2026 at 10:29 pm
house of fun casino
https://dotvdo.com/@earthadaplyn2?page=about https://dotvdo.com/@earthadaplyn2?page=about
https://videowala.xyz//@halliemcculler?page=about https://videowala.xyz
https://gitlab-rock.freedomstate.idv.tw/kelliedennys88 https://gitlab-rock.freedomstate.idv.tw/kelliedennys88
https://actsolution.iptime.org:3000/janessawymark actsolution.iptime.org
http://newchanpin.yuntangkeji.cn:33009/wolfgangmonett newchanpin.yuntangkeji.cn
https://vila.go.ro/stanleyporteou vila.go.ro
http://www.scserverddns.top:13000/wayneoje899319 scserverddns.top
https://git.smart-tool.jp/mickeymathis2 git.smart-tool.jp
https://vidspace.store/@maryellenperss?page=about https://vidspace.store/@maryellenperss?page=about
https://dating.vi-lab.eu/@armandofremont https://dating.vi-lab.eu
https://drarchina.com/demo/@alysaring44052?page=about https://drarchina.com/demo/@alysaring44052?page=about
https://funnyutube.com/@ethanfinsch65?page=about funnyutube.com
https://git.archieri.fr/aileenhaney059 git.archieri.fr
https://demo.playtubescript.com/@holliesimpkins?page=about https://demo.playtubescript.com/
https://git.violka-it.net/tricialouden50 git.violka-it.net
https://videyme.online/@jenshadden5894?page=about videyme.online
http://git.dglyoo.com/rosadown677644 http://git.dglyoo.com
https://pure.itsabouttimetv1.com/@epifaniastraub?page=about pure.itsabouttimetv1.com
References:
https://gitea.pnkx.top:8/juanitawimmer8
https://spinvai.com/robbyh98090775 · April 17, 2026 at 10:57 pm
casino royal streaming
http://git.dglyoo.com/chloekoertig9 http://git.dglyoo.com/chloekoertig9
https://wedioz.com/@archerscherf0?page=about wedioz.com
https://gitea.wuyuank.com/vilma050576409 gitea.wuyuank.com
https://tripled.driven-dreams.co.uk/@lorenedeboos61 tripled.driven-dreams.co.uk
https://platform.giftedsoulsent.com/danatoney46542 platform.giftedsoulsent.com
https://romancefrica.com/@alfonzo91f573 https://romancefrica.com/@alfonzo91f573
https://bigotube.com/@joanzinn573766?page=about bigotube.com
https://cloveebiz.com.ng/@valentinapelle?page=about https://cloveebiz.com.ng/
https://git.wisder.net/ankecorley8194 https://git.wisder.net
https://www.nemusic.rocks/charliesolis62 http://www.nemusic.rocks
http://musicstreaming.yonetsystems.com/lonniewise8924 musicstreaming.yonetsystems.com
https://chenxil.top/estherrobinett https://chenxil.top
https://21pac.com/@alinadesmond7?page=about https://21pac.com/
https://revenu.live/@violettemiramo?page=about revenu.live
https://dammsound.com/robin177090374 https://dammsound.com/robin177090374
https://www.beyoncetube.com/@latiakong68499?page=about https://www.beyoncetube.com/@latiakong68499?page=about
https://gitea.nacsity.cn/adelaidadonnit gitea.nacsity.cn
https://www.meetgr.com/@cornellcooley7 meetgr.com
References:
https://eduback.com/@terrelldonoghu?page=about
nelgit.nelpi.co.uk · April 17, 2026 at 11:01 pm
References:
Wild vegas casino
References:
https://gitea.nacsity.cn/adelaidadonnit
https://streamifyr.com/@mahaliaconsidi?page=about · April 17, 2026 at 11:52 pm
casino on line
https://git.anagora.org/thorstenframe git.anagora.org
https://git.vsadygv.com/claudiokellehe git.vsadygv.com
https://lyfeclick.com/@melvinqualls37 lyfeclick.com
https://thewordtube.org/@jeroldmarcell?page=about thewordtube.org
https://music.wzsipku.cn/lynwoodfarias9 music.wzsipku.cn
https://www.panjabi.in/@xxisuzanna3964?page=about http://www.panjabi.in
https://mxtube.mimeld.com/@arielhung8780?page=about https://mxtube.mimeld.com
https://git.freno.me/selenapuig4147 git.freno.me
https://git.minecraftlegacy.com/archer08q9608 git.minecraftlegacy.com
https://gitea.css-sistemas.com.br/larry61995555 gitea.css-sistemas.com.br
http://git.qniao.cn/gladisnewcombe git.qniao.cn
https://clipbeans.com/@dustyglenny24?page=about https://clipbeans.com
https://gitslayer.de/melindaholland gitslayer.de
https://v.sharevr.com/@emmangeles9277?page=about https://v.sharevr.com/@emmangeles9277?page=about
http://gitea.mikarsoft.com/thadlemieux837 http://gitea.mikarsoft.com/
https://k0ki-dev.com/keenanibr67348 https://k0ki-dev.com/keenanibr67348
https://dimen.krd/@kandishorsley?page=about dimen.krd
https://lishan148.synology.me:3014/doyleburks6440 https://lishan148.synology.me
References:
https://asiannearby.com/@taylavandermar
abadeez.com · April 18, 2026 at 12:15 am
quebec roulette
https://www.meetgr.com/@cornellcooley7 http://www.meetgr.com
https://raimusic.vn/russrembert037 raimusic.vn
https://gitea.nacsity.cn/mattcawthorn87 gitea.nacsity.cn
https://tea.neuron.my/cheryl2598605 https://tea.neuron.my/cheryl2598605
https://videowala.xyz//@victorinaernes?page=about videowala.xyz
https://www.peter-bartke.de/changk70412414 https://www.peter-bartke.de/changk70412414
https://git.scinalytics.com/lorengoss8086 git.scinalytics.com
https://gitlab-rock.freedomstate.idv.tw/kelliedennys88 gitlab-rock.freedomstate.idv.tw
https://git.esen.gay/fredricqyd304 git.esen.gay
https://cameotv.cc/@mamiemickens71?page=about https://cameotv.cc/@mamiemickens71?page=about
https://phoebe.roshka.com/gitlab/lornatrundle72 phoebe.roshka.com
https://jom.gg/@christopher549 jom.gg
https://gitea.syn-assist.fr/loydmulkey6284 gitea.syn-assist.fr
https://liverights.org//@paulescobar853?page=about liverights.org
http://z.duowenlvshi.com/pruismael88551 z.duowenlvshi.com
https://www.beyoncetube.com/@latiakong68499?page=about http://www.beyoncetube.com
https://kayesbamusic.com/murray6011080 kayesbamusic.com
https://www.beyoncetube.com/@penneybox0214?page=about https://www.beyoncetube.com/@penneybox0214?page=about
References:
https://lasigal.com/danellerodman0
shirme.com · April 18, 2026 at 12:48 am
poker bonus no deposit
https://git.limework.net/williemaehytte https://git.limework.net
https://mahalkita.ph/@alexandriasnx mahalkita.ph
https://www.panjabi.in/@cynthiabosley2?page=about panjabi.in
https://gitea.zachl.tech/kellieliddell https://gitea.zachl.tech/kellieliddell
http://www.scserverddns.top:13000/wayneoje899319 http://www.scserverddns.top/
http://crontab.club:30015/chiquitam19692 http://crontab.club:30015/chiquitam19692
https://gbewaaplay.com/friedalieb016 gbewaaplay.com
https://music.wzsipku.cn/edwinaliston73 music.wzsipku.cn
https://git.freno.me/pabloertel3783 git.freno.me
https://gitea.zachl.tech/kellieliddell https://gitea.zachl.tech/kellieliddell
https://musiciansportal.ru/starlabryson77 https://musiciansportal.ru/
https://stukguitar.com/@joesphfallon39?page=about stukguitar.com
https://645123.com/@wilfordchastai?page=about 645123.com
https://git.htns.com/keenantorpy999 git.htns.com
https://gitea.goldendeliverer.com/lokelton35269 gitea.goldendeliverer.com
https://git.violka-it.net/leroymathy9351 git.violka-it.net
https://gitea.adber.tech/alinecarlton31 gitea.adber.tech
https://vcs.cozydsp.space/laureneelsberr vcs.cozydsp.space
References:
https://sing.ibible.hk/@amparoandrzeje?page=about
https://tubepeer.com/ · April 18, 2026 at 1:26 am
References:
Shreveport la casinos
References:
https://katambe.com/@thadpippin758
iamtube.jp · April 18, 2026 at 2:02 am
aspers casino london
https://gitea.pnkx.top:8/margaritaferre gitea.pnkx.top
http://dev-gitlab.dev.sww.com.cn/mariokashiwagi http://dev-gitlab.dev.sww.com.cn/mariokashiwagi
https://git.vhdltool.com/jessikax51460 https://git.vhdltool.com/jessikax51460
https://wedioz.com/@archerscherf0?page=about wedioz.com
https://loopplay.site/@georgiannalayc?page=about https://loopplay.site/
https://git.van-peeren.de/gregoriocwv66 https://git.van-peeren.de/gregoriocwv66
https://isugar-dating.com/@roderick604581 isugar-dating.com
https://flirta.online/@janellhardie4 flirta.online
https://unitedmusicstreaming.com/kristanmowry79 unitedmusicstreaming.com
https://digitalafterlife.org/@vernitas600123?page=about digitalafterlife.org
https://git.navex.com.br/rolandotyree8 https://git.navex.com.br
https://gitea.waterworld.com.hk/aras2398759774 https://gitea.waterworld.com.hk
https://tripled.driven-dreams.co.uk/@lorenedeboos61 tripled.driven-dreams.co.uk
https://git.automathon.org/lvoaurelio3242 git.automathon.org
https://tunelifystream.com/sheilaffo13037 https://tunelifystream.com/sheilaffo13037
https://hellomusic.app/traceewao42314 hellomusic.app
https://git.clubeye.net/hsjlindsey9593 https://git.clubeye.net/hsjlindsey9593
https://git.lucas-michel.fr/paulinelondon0 https://git.lucas-michel.fr/paulinelondon0
References:
https://playtube.com.pl/@brittlockhart?page=about
gitea.lasallesaintdenis.com · April 18, 2026 at 2:13 am
pink floyd live at pompeii
http://git.dglyoo.com/rosadown677644 http://git.dglyoo.com/rosadown677644
https://mahalkita.ph/@elanademaio581 mahalkita.ph
http://rm.runfox.com/gitlab/georgettamadig rm.runfox.com
https://funnyutube.com/@belenault9953?page=about https://funnyutube.com
https://revenu.live/@yukikoplumlee?page=about revenu.live
https://gitea.biboer.cn/eloisewilliam1 gitea.biboer.cn
https://www.beyoncetube.com/@penneybox0214?page=about http://www.beyoncetube.com
https://niqnok.com/carmenstoker58 niqnok.com
https://git.huwhy.cn/collettethaxto https://git.huwhy.cn/collettethaxto
https://music.wzsipku.cn/chutilley24918 music.wzsipku.cn
https://git.deadpoo.net/brittbaughman git.deadpoo.net
https://www.nemusic.rocks/naomihampden62 https://www.nemusic.rocks/naomihampden62
https://superocho.org/@zsfbrandi50319?page=about https://superocho.org
https://www.ikaros.asia/phyllisjordon https://www.ikaros.asia/
https://gitea-inner.fontree.cn/wilburnsiebenh https://gitea-inner.fontree.cn/wilburnsiebenh
https://video.silverwolfstudios.com/@majorpsl791830?page=about video.silverwolfstudios.com
https://gitea.nongnghiepso.com/sondale0765716 https://gitea.nongnghiepso.com/
https://git.nathanspackman.com/corneliusmedle git.nathanspackman.com
References:
https://datemyfamily.tv/@aubreyfogarty3
chinami.com · April 18, 2026 at 2:20 am
sands casino pa
https://kition.mhl.tuc.gr/bebemcness5744 kition.mhl.tuc.gr
https://beatsong.app/shawnatressler beatsong.app
https://git.lucas-michel.fr/franciscaselby https://git.lucas-michel.fr/
https://gitea.coderpath.com/xokhelena86276 gitea.coderpath.com
https://git.gonethome.id/rockydecastell git.gonethome.id
https://www.latflex.net/@niklasricketts?page=about http://www.latflex.net
https://play.ophirstudio.com//@hwadominic9536?page=about https://play.ophirstudio.com
https://iraqitube.com/@raedover031658?page=about https://iraqitube.com
https://gitea.shizuka.icu/hectordoolan75 gitea.shizuka.icu
https://worship.com.ng/haihupp2733380 worship.com.ng
https://git.autotion.net/mohammedgosse https://git.autotion.net/mohammedgosse
https://play.ophirstudio.com//@merryesposito0?page=about play.ophirstudio.com
https://git.violka-it.net/tricialouden50 git.violka-it.net
http://dev-gitlab.dev.sww.com.cn/mariokashiwagi dev-gitlab.dev.sww.com.cn
http://siloo.site/@belinda2504129?page=about siloo.site
https://dammsound.com/robin177090374 dammsound.com
https://git.dotb.cloud/kamimoose21883 git.dotb.cloud
https://chenxil.top/jrerosalind439 chenxil.top
References:
https://actsolution.iptime.org:3000/lilykitamura3
ott.saikatinfotech.com · April 18, 2026 at 2:31 am
nba games tonight
https://movie.nanuly.kr/@magaretmowery?page=about movie.nanuly.kr
https://git.cyberuk.me/jaunitamcaulay https://git.cyberuk.me/jaunitamcaulay
https://git.powderbluecrayon.com/joleenmunro99 git.powderbluecrayon.com
https://vlotube.com/@jannettekonig?page=about vlotube.com
https://gitslayer.de/melindaholland gitslayer.de
https://gitea.css-sistemas.com.br/wzwesperanza74 gitea.css-sistemas.com.br
https://git.danpeak.co.uk/analisabrumby https://git.danpeak.co.uk/analisabrumby
https://play.eccentric.etc.br/@arleneboland8?page=about play.eccentric.etc.br
https://git.suo0.com/alyciawuo47982 https://git.suo0.com/
https://www.uria.dev/liliaschuster http://www.uria.dev
https://www.lizyum.com/@rebeccafiguero lizyum.com
https://viraltubex.com/@retarader9892?page=about viraltubex.com
https://whiskey.tangomedia.fr/@laurenceeames2?page=about https://whiskey.tangomedia.fr/@laurenceeames2?page=about
http://demo.sunflowermachinery.com/kazukoatchley http://demo.sunflowermachinery.com
https://git.violka-it.net/tricialouden50 git.violka-it.net
https://gitea.css-sistemas.com.br/larry61995555 gitea.css-sistemas.com.br
https://gitea.gimmin.com/dustyaeh08140 https://gitea.gimmin.com/
https://git.scinalytics.com/pmbnilda220675 git.scinalytics.com
References:
https://gitea.wuyuank.com/qerjenna519200
skiivie.com · April 18, 2026 at 2:37 am
References:
Roulette wheel selection
References:
https://mambotango.it/lucile80668363
git.123doit.com · April 18, 2026 at 2:53 am
References:
Super jackpot
References:
https://chenxil.top/lorena81931970
https://seychelleslove.com/@hkygretta35187 · April 18, 2026 at 3:04 am
casino of the sun
https://iesoundtrack.tv/@sharynw2959974?page=about https://iesoundtrack.tv/
https://gitea.zachl.tech/kellieliddell gitea.zachl.tech
https://www.peter-bartke.de/wpxsyreeta7233 http://www.peter-bartke.de
https://zurimeet.com/@mohamedjackson https://zurimeet.com
https://friztty.com/@codyfinnan9864 https://friztty.com/@codyfinnan9864
https://tayartaw.kyaikkhami.com/elvabrehm2935 tayartaw.kyaikkhami.com
https://k0ki-dev.com/melvinaaoj434 k0ki-dev.com
https://gitea.bel.blue/elizabet17770 https://gitea.bel.blue
https://git.suo0.com/alyciawuo47982 https://git.suo0.com/alyciawuo47982
https://dimen.krd/@lilabeaumont68?page=about dimen.krd
https://git.vsadygv.com/bettiemunday0 git.vsadygv.com
https://channel-u.tv/@fletcherlauren?page=about https://channel-u.tv/
https://www.shreegandha.com/@angeles10u6101?page=about http://www.shreegandha.com
http://siloo.site/@belinda2504129?page=about siloo.site
https://www.nemusic.rocks/charliesolis62 http://www.nemusic.rocks
https://play.eccentric.etc.br/@harrietthumphr?page=about play.eccentric.etc.br
https://funnyutube.com/@belenault9953?page=about funnyutube.com
https://mginger.org/@loriecourtney https://mginger.org/
References:
https://gitea.syn-assist.fr/brianracine078
git.hgbenjamin.com · April 18, 2026 at 3:07 am
References:
Slot machine games online
References:
https://git.navex.com.br/rolandotyree8
worship.com.ng · April 18, 2026 at 4:02 am
online slot machines real money
https://git.suo0.com/alyciawuo47982 https://git.suo0.com/
https://yours-tube.com/@ncdaugustus736?page=about yours-tube.com
http://z.duowenlvshi.com/mauricekirsova z.duowenlvshi.com
https://viraltubex.com/@retarader9892?page=about viraltubex.com
https://git.archieri.fr/arturolundgren git.archieri.fr
https://mkhonto.net/@jacquesgrinder?page=about mkhonto.net
https://spice.blue/@lacygrigsby47?page=about spice.blue
https://gitlab-rock.freedomstate.idv.tw/kelliedennys88 gitlab-rock.freedomstate.idv.tw
https://unired.zz.com.ve/@amie80s0849445 unired.zz.com.ve
https://simapodcast.co.ls/@epifaniapaling?page=about https://simapodcast.co.ls
https://www.monasticeye.com/@annismillingto?page=about https://www.monasticeye.com
http://git.zxkedu.com:33769/coygodfrey2046 git.zxkedu.com
https://www.telugustatusvideo.com/@karissabudd951?page=about https://www.telugustatusvideo.com/
https://gitea.primecontrols-dev.com/polly99b333442 https://gitea.primecontrols-dev.com
https://yours-tube.com/@silasvanburen4?page=about yours-tube.com
https://actsolution.iptime.org:3000/lilykitamura3 https://actsolution.iptime.org
https://raimusic.vn/russrembert037 https://raimusic.vn/russrembert037
https://git.miasma-os.com/celestebrinson https://git.miasma-os.com/celestebrinson
References:
https://code.hpswk.com/elenawooden312
https://www.kornerspot.com/@geraldoculler · April 18, 2026 at 4:32 am
las vegas usa casino
https://git.sunlix.one/redai35207943 git.sunlix.one
https://gitea.gimmin.com/dustyaeh08140 https://gitea.gimmin.com
https://git.hgbenjamin.com/vickiwalden28 https://git.hgbenjamin.com/
https://git.csi-kjsce.org/trishaa021835 git.csi-kjsce.org
https://code.dsconce.space/jameldore19616 code.dsconce.space
https://gitea.wuyuank.com/qerjenna519200 gitea.wuyuank.com
http://git.dglyoo.com/rosadown677644 git.dglyoo.com
https://git.sunlix.one/veronicasinger https://git.sunlix.one/veronicasinger
https://hipstrumentals.net/randalbaehr920 hipstrumentals.net
https://datingmywish.com/@kathaleenn6180 https://datingmywish.com
https://datingmywish.com/@beulahspoffort https://datingmywish.com/@beulahspoffort
https://gitea.shizuka.icu/hectordoolan75 gitea.shizuka.icu
https://vigilanteapp.com/@myleslevine677?page=about vigilanteapp.com
https://mambotango.it/lucile80668363 mambotango.it
https://christianmail.tv/@dinaelphinston?page=about christianmail.tv
http://gitlab.dev.jtyjy.com/gisellesalkaus gitlab.dev.jtyjy.com
https://stukguitar.com/@cecilewsw95476?page=about stukguitar.com
https://aladin.tube/@issacbarragan8?page=about https://aladin.tube/
References:
https://gitea.zachl.tech/violet7867670
newborhooddates.com · April 18, 2026 at 4:35 am
monkey money
https://gitea.micro-stack.org/kennethhateley gitea.micro-stack.org
https://k0ki-dev.com/romaineworrell k0ki-dev.com
https://play.talkdrove.cc.nf/@almagerrard57?page=about play.talkdrove.cc.nf
https://quickdate.arenascript.de/@loratolmie948 https://quickdate.arenascript.de/
https://chinami.com/@georgiannabloc?page=about chinami.com
https://neuralkazmain.com/swykassandra08 neuralkazmain.com
http://www.xngel.com/@terrellvvh6187?page=about http://www.xngel.com/
https://kayesbamusic.com/murray6011080 kayesbamusic.com
https://christianmail.tv/@dinaelphinston?page=about https://christianmail.tv/@dinaelphinston?page=about
https://gitea.goldendeliverer.com/lokelton35269 gitea.goldendeliverer.com
https://skytube.skyinfo.in/@karolyntillery?page=about skytube.skyinfo.in
https://cloudtu.be/@mariecalwell93?page=about https://cloudtu.be
https://gitea.wuyuank.com/frederickalutw https://gitea.wuyuank.com/frederickalutw
https://sportsdungeon.com/@alinagood38417?page=about https://sportsdungeon.com
https://www.ohovideo.com/@tiffanyblanche?page=about https://www.ohovideo.com/
http://gitea.yiban.com.tw:3030/cedricholland gitea.yiban.com.tw
https://www.ohovideo.com/@jodyckx3738230?page=about ohovideo.com
https://platform.giftedsoulsent.com/danatoney46542 platform.giftedsoulsent.com
References:
https://git.apextoaster.com/allanbaader53
gitea.pnkx.top · April 18, 2026 at 4:49 am
tdu2 casino
https://crazyworksports.com/@staciekoertig8?page=about crazyworksports.com
https://simapodcast.co.ls/@geriwalls66936?page=about simapodcast.co.ls
https://rjlove.org/@cesarkrichauff https://rjlove.org/
https://learninghub.fulljam.com/@ritaves439876?page=about https://learninghub.fulljam.com
https://learninghub.fulljam.com/@ritaves439876?page=about learninghub.fulljam.com
https://gitlab-rock.freedomstate.idv.tw/kelliedennys88 gitlab-rock.freedomstate.idv.tw
https://gitea.yantootech.com/dietermileham4 https://gitea.yantootech.com/
https://gitea.diputadosalta.gob.ar/poerosella6250 https://gitea.diputadosalta.gob.ar
https://gitea.shizuka.icu/hectordoolan75 gitea.shizuka.icu
https://itimez.com/@jamilaspears46?page=about itimez.com
https://clipbeans.com/@anthonysteffen?page=about https://clipbeans.com
https://hellomusic.app/alvapaine1789 https://hellomusic.app/alvapaine1789
https://git.vsadygv.com/claudiokellehe git.vsadygv.com
https://vydiio.com/@edlshana617193?page=about https://vydiio.com/
https://clovyn.club/@elvinhampton65 https://clovyn.club/@elvinhampton65
https://gitea.waterworld.com.hk/deanap47911441 gitea.waterworld.com.hk
https://dev3.worldme.tv/@consuelowhatmo?page=about dev3.worldme.tv
https://itimez.com/@jamilaspears46?page=about https://itimez.com
References:
https://gbewaaplay.com/quyenmedford73
git.vezpi.com · April 18, 2026 at 5:22 am
winaday casino
https://gitea.mynas-lechner.de/adelacranswick gitea.mynas-lechner.de
https://git.chalypeng.xyz/colinnadel321 git.chalypeng.xyz
https://www.lizyum.com/@ioladuhig49961 https://www.lizyum.com/@ioladuhig49961
https://gitea.yantootech.com/dietermileham4 gitea.yantootech.com
https://lasigal.com/amyfloyd072285 lasigal.com
https://dotvdo.com/@earthadaplyn2?page=about dotvdo.com
https://myhealthypunjab.com/@ipkramiro8359?page=about https://myhealthypunjab.com/@ipkramiro8359?page=about
https://git.warze.org/rosalindcumpst git.warze.org
https://freshtube.net/@kristopherchow?page=about freshtube.net
https://www.herzog-it.de/fayedelargie09 http://www.herzog-it.de
https://loopplay.site/@franciscohaszl?page=about https://loopplay.site/
https://romatube.com/@elisturm975363?page=about romatube.com
https://tayartaw.kyaikkhami.com/elvabrehm2935 tayartaw.kyaikkhami.com
https://www.broutube.com/@galenhumphreys?page=about http://www.broutube.com
https://code.hpswk.com/jerrodcone7240 code.hpswk.com
https://645123.com/@wilfordchastai?page=about 645123.com
https://gitea.shizuka.icu/nadine50610805 gitea.shizuka.icu
https://git.daoyoucloud.com/danestorey0763 git.daoyoucloud.com
References:
https://qflirt.net/@danielariordan
gitea.nongnghiepso.com · April 18, 2026 at 6:08 am
majestic casino
https://demo.playtubescript.com/@holliesimpkins?page=about demo.playtubescript.com
https://dotvdo.com/@kindrahenschke?page=about dotvdo.com
https://myafritube.com/@chiquitademers?page=about myafritube.com
https://adufoshi.com/sanfordengland adufoshi.com
https://cameotv.cc/@mamiemickens71?page=about https://cameotv.cc/@mamiemickens71?page=about
https://ceedmusic.com/kristie32m858 ceedmusic.com
https://git.0935e.com/lemuelrittenho git.0935e.com
https://21pac.com/@alinadesmond7?page=about 21pac.com
https://www.kornerspot.com/@zach9417310512 http://www.kornerspot.com
https://adufoshi.com/alfiebarlow73 https://adufoshi.com/alfiebarlow73
https://pure.itsabouttimetv1.com/@rodgerlangler0?page=about https://pure.itsabouttimetv1.com/@rodgerlangler0?page=about
https://spice.blue/@lacygrigsby47?page=about https://spice.blue/@lacygrigsby47?page=about
https://mxtube.mimeld.com/@altoncolosimo8?page=about https://mxtube.mimeld.com/@altoncolosimo8?page=about
https://git.alderautomation.ca/ingeborgforema git.alderautomation.ca
https://code.hpswk.com/elyse20h704167 https://code.hpswk.com/
https://www.howeasynetwork.com/@kristophermoll?page=about https://www.howeasynetwork.com/@kristophermoll?page=about
https://liverights.org//@paulescobar853?page=about https://liverights.org//@paulescobar853?page=about
https://chenxil.top/estherrobinett chenxil.top
References:
https://git.0935e.com/senaida18e081
thewerffreport.com · April 18, 2026 at 6:08 am
crown europe casino
https://www.singuratate.ro/@marilynnweathe http://www.singuratate.ro
https://hlumi.com/@mohameddunham?page=about https://hlumi.com/@mohameddunham?page=about
https://git.wisder.net/annmariefriedm git.wisder.net
https://aladin.tube/@issacbarragan8?page=about https://aladin.tube/
https://git.hgbenjamin.com/vickiwalden28 https://git.hgbenjamin.com/vickiwalden28
https://hiwifi.denq.us:8418/linnieu8822313 hiwifi.denq.us
https://gitea.nongnghiepso.com/stevemceachern https://gitea.nongnghiepso.com
https://volts.howto.co.ug/@gaypqw9837172 volts.howto.co.ug
https://deltasongs.com/chautimmerman deltasongs.com
https://git.healthathome.com.np/tylercrandall0 git.healthathome.com.np
https://gitlab.iplusus.com/brandiestubbs7 gitlab.iplusus.com
https://lius.familyds.org:3000/alana375816079 lius.familyds.org
https://channel-u.tv/@ibcvirgilio68?page=about https://channel-u.tv/@ibcvirgilio68?page=about
https://gitlab-rock.freedomstate.idv.tw/francespethard gitlab-rock.freedomstate.idv.tw
https://gitea.dsmaster.myds.me/margaret155538 gitea.dsmaster.myds.me
http://gitea.jb1000.com:88/carrilapine079 http://gitea.jb1000.com:88/carrilapine079
https://gitea.coderpath.com/xokhelena86276 https://gitea.coderpath.com/xokhelena86276
https://kition.mhl.tuc.gr/demetriusi767 kition.mhl.tuc.gr
References:
https://wiibiplay.fun/@jasperfzf96485?page=about
git.zakum.cn · April 18, 2026 at 6:49 am
casino times
https://shamrick.us/torstenhause63 shamrick.us
https://git.vezpi.com/latanyafusco07 git.vezpi.com
https://gitea.biboer.cn/eloisewilliam1 https://gitea.biboer.cn/eloisewilliam1
http://rm.runfox.com/gitlab/allisonparas0 rm.runfox.com
https://dotvdo.com/@earthadaplyn2?page=about dotvdo.com
https://git.zakum.cn/samualbaylee8 https://git.zakum.cn/genevievecudmo
https://www.ituac.com/franciscojay38 ituac.com
https://git.autotion.net/juanbushby5500 git.autotion.net
https://truthtube.video/@florenciagarri?page=about https://truthtube.video/@florenciagarri?page=about
https://nelgit.nelpi.co.uk/melvakastner7 https://nelgit.nelpi.co.uk/melvakastner7
https://git.huwhy.cn/collettethaxto git.huwhy.cn
https://gitea.diputadosalta.gob.ar/poerosella6250 https://gitea.diputadosalta.gob.ar/
https://www.fepp.org.ec/sondran604348 https://www.fepp.org.ec/sondran604348
https://git.clickforadventure.co/norbertopennin git.clickforadventure.co
http://newchanpin.yuntangkeji.cn:33009/wolfgangmonett http://newchanpin.yuntangkeji.cn:33009/wolfgangmonett
https://git.adityagupta.dev/melindabown087 https://git.adityagupta.dev/
https://mxtube.mimeld.com/@altoncolosimo8?page=about mxtube.mimeld.com
https://www.lizyum.com/@ioladuhig49961 http://www.lizyum.com
actv.1tv.hk · April 18, 2026 at 6:55 am
roulette wheel numbers
https://music.1mm.hk/mpkhanna01008 https://music.1mm.hk
https://tcodpractice.com/angiegreig2638 tcodpractice.com
https://gitea.zczcfiles.com.cn/shellablackmon gitea.zczcfiles.com.cn
https://profmustafa.com/@laurenmtm73697?page=about profmustafa.com
https://git.yinbonet.cn/harveyandrade https://git.yinbonet.cn/
https://git.vsadygv.com/bettiemunday0 https://git.vsadygv.com
https://git.apextoaster.com/allanbaader53 git.apextoaster.com
https://watchnpray.life/@sharipeltier03?page=about https://watchnpray.life
https://k0ki-dev.com/keenanibr67348 https://k0ki-dev.com
https://myclassictv.com/@hassanjefferso?page=about myclassictv.com
https://git.flymiracle.com/emiliadelong36 https://git.flymiracle.com
https://digitalafterlife.org/@vernitas600123?page=about digitalafterlife.org
https://git.slegeir.com/darnellpriestl https://git.slegeir.com/
https://qdate.ru/@leonoreberkman qdate.ru
https://hlumi.com/@rhyssligo14406?page=about hlumi.com
http://git.zxkedu.com:33769/coygodfrey2046 http://git.zxkedu.com:33769/coygodfrey2046
https://channel-u.tv/@fletcherlauren?page=about channel-u.tv
https://xonnon.com/@vnwbenny215255?page=about xonnon.com
References:
https://vxtube.net/@rhealavallie7?page=about
iraqitube.com · April 18, 2026 at 7:40 am
References:
Hoyle casino
References:
https://lovcam.mydaddyonline.in/@donclaude63012
git.nulldirect.com · April 18, 2026 at 8:08 am
slots no download
https://git.lucas-michel.fr/broderickchill git.lucas-michel.fr
https://romatube.com/@charlesb660845?page=about https://romatube.com
https://seychelleslove.com/@christiebethun https://seychelleslove.com/@christiebethun
https://superocho.org/@zsfbrandi50319?page=about https://superocho.org/@zsfbrandi50319?page=about
https://git.gonethome.id/rockydecastell https://git.gonethome.id/rockydecastell
https://smartcampus-seskoal.id/streaming/@micheljasper31?page=about smartcampus-seskoal.id
https://dotvdo.com/@earthadaplyn2?page=about https://dotvdo.com/@earthadaplyn2?page=about
https://seychelleslove.com/@christiebethun https://seychelleslove.com/@christiebethun
https://git.louislabs.com/meistevens124 https://git.louislabs.com/
https://apyarx.com/@rileyprovost68?page=about https://apyarx.com/@rileyprovost68?page=about
https://git.hubhoo.com/josieprobert0 git.hubhoo.com
https://wopid.io/@latashiacaroth?page=about wopid.io
https://qpxy.cn/jadarayner9413 qpxy.cn
https://git.sskuaixiu.com/lisaoates91159 git.sskuaixiu.com
https://www.kornerspot.com/@zach9417310512 https://www.kornerspot.com/
https://music.crone.es/@muhammadleclai?page=about music.crone.es
https://aprileaton.net/carlton0348032 https://aprileaton.net/
https://www.hyzq123.com/@gabrielesidney?page=about https://www.hyzq123.com
References:
https://unitedmusicstreaming.com/roccorusso8388
repo.magicbane.com · April 18, 2026 at 8:12 am
cairns casino
https://gitea.dsmaster.myds.me/margaret155538 gitea.dsmaster.myds.me
https://camtalking.com/@valentinashley camtalking.com
https://gitea.personalsoftware.space/erika02e29722 gitea.personalsoftware.space
https://nildigitalco.com/@alejandrinawes?page=about nildigitalco.com
https://yaseen.tv/@wsdmathew13351?page=about https://yaseen.tv/
https://lishan148.synology.me:3014/doyleburks6440 lishan148.synology.me
http://dsmcase.com:2180/annbogen26183 dsmcase.com
https://skytube.skyinfo.in/@karolyntillery?page=about skytube.skyinfo.in
https://gitea.css-sistemas.com.br/lylefinnegan7 gitea.css-sistemas.com.br
https://loopplay.site/@georgiannalayc?page=about https://loopplay.site
https://play.ophirstudio.com//@merryesposito0?page=about https://play.ophirstudio.com//@merryesposito0?page=about
https://www.mein-bdsm.de/@nellyvalladare http://www.mein-bdsm.de
https://musiciansportal.ru/starlabryson77 https://musiciansportal.ru/
https://git.smart-tool.jp/princesswunder git.smart-tool.jp
https://dammsound.com/robin177090374 dammsound.com
https://cloveebiz.com.ng/@haimccomas7864?page=about cloveebiz.com.ng
https://play.eccentric.etc.br/@harrietthumphr?page=about https://play.eccentric.etc.br/
https://mmctube.com/@betsygibbs069?page=about https://mmctube.com/@betsygibbs069?page=about
References:
https://git.csi-kjsce.org/trishaa021835
https://niqnok.com/hannawoodall38 · April 18, 2026 at 8:19 am
References:
Woodbine casino
References:
https://isugar-dating.com/@garrettforsyth
https://44sex.com/@pilarecq753827?page=about · April 18, 2026 at 8:30 am
References:
Shreveport casinos
References:
https://naijasingles.net/@virginiaguinn
https://pure.itsabouttimetv1.com/@damariseldersh?page=about · April 18, 2026 at 8:39 am
puerto rico casinos
https://www.herzog-it.de/fayedelargie09 https://www.herzog-it.de/
https://date-duell.de/@rosellabeane7 date-duell.de
https://www.ituac.com/franciscojay38 https://www.ituac.com/franciscojay38
https://git.limework.net/williemaehytte https://git.limework.net/williemaehytte
https://asiannearby.com/@alexandraflagg asiannearby.com
https://git.yinbonet.cn/harveyandrade git.yinbonet.cn
https://git.gonethome.id/roxiemickens17 git.gonethome.id
https://truthtube.video/@pearlb23758629?page=about truthtube.video
https://streamifyr.com/@mahaliaconsidi?page=about streamifyr.com
https://playtube.com.pl/@brittlockhart?page=about https://playtube.com.pl/@brittlockhart?page=about
https://git.game-dev.space/aureliofosbery git.game-dev.space
https://git.navex.com.br/rolandotyree8 git.navex.com.br
https://114.242.31.6:3000/leonelthibodea https://114.242.31.6
https://www.shreegandha.com/@angeles10u6101?page=about https://www.shreegandha.com/@angeles10u6101?page=about
https://xonnon.com/@vnwbenny215255?page=about https://xonnon.com
https://gogolive.biz/@aidaq804598570?page=about gogolive.biz
https://naijasingles.net/@virginiaguinn naijasingles.net
https://music.crone.es/@demetrius68e34?page=about https://music.crone.es/@demetrius68e34?page=about
References:
https://beatsong.app/johniemckeon97
https://mygit.kikyps.com/elvissellheim · April 18, 2026 at 9:11 am
References:
Comanche nation casino
References:
https://git.game-dev.space/aureliofosbery
www.herzog-it.de · April 18, 2026 at 9:18 am
pocola casino
https://thefusionflix.com/@carmelasanborn?page=about thefusionflix.com
https://gitea.shizuka.icu/nadine50610805 https://gitea.shizuka.icu/nadine50610805
https://camtalking.com/@valentinashley https://camtalking.com/
https://tea.neuron.my/cheryl2598605 tea.neuron.my
http://gitea.mikarsoft.com/claudettevanwi gitea.mikarsoft.com
https://play.eccentric.etc.br/@arleneboland8?page=about https://play.eccentric.etc.br
https://apyarx.com/@rileyprovost68?page=about apyarx.com
https://superocho.org/@spencerjbz9667?page=about https://superocho.org/@spencerjbz9667?page=about
http://app.venusroyale.date/@freddybabbidge http://app.venusroyale.date
https://itimez.com/@noahchambliss5?page=about itimez.com
https://git.huwhy.cn/marcelofetty31 git.huwhy.cn
https://gitea.shizuka.icu/nadine50610805 https://gitea.shizuka.icu/
https://git.game-dev.space/aureliofosbery git.game-dev.space
https://www.oddmate.com/@karissa0446898 http://www.oddmate.com
https://clipbeans.com/@anthonysteffen?page=about clipbeans.com
https://gitea.biboer.cn/victorinaclaud gitea.biboer.cn
https://git.mana-web.com/bernardoscherf https://git.mana-web.com/
https://smartastream.com/@halleykaestner?page=about https://smartastream.com/@halleykaestner?page=about
References:
https://git.yinbonet.cn/harveyandrade
https://gitea.kdlsvps.top/maritamahoney7 · April 18, 2026 at 10:29 am
References:
William hill desktop site
References:
https://git.flymiracle.com/emiliadelong36
megastream.pl · April 18, 2026 at 10:31 am
silver oak casino
https://unired.zz.com.ve/@amie80s0849445 unired.zz.com.ve
http://git.yanei-iot.com:600/willard41a9606 git.yanei-iot.com
https://musiciansportal.ru/starlabryson77 https://musiciansportal.ru/starlabryson77
https://friztty.com/@codyfinnan9864 https://friztty.com
https://git.adityagupta.dev/melindabown087 git.adityagupta.dev
https://git.louislabs.com/davemeister954 git.louislabs.com
https://beatsong.app/johniemckeon97 https://beatsong.app/johniemckeon97
https://cloveebiz.com.ng/@valentinapelle?page=about https://cloveebiz.com.ng/@valentinapelle?page=about
https://www.bongmedia.tv/@kristianshilli?page=about https://www.bongmedia.tv
https://freehaitianmovies.com/@tessasmithson?page=about freehaitianmovies.com
https://gitea.yantootech.com/finnkiek471057 gitea.yantootech.com
https://streamifyr.com/@mahaliaconsidi?page=about streamifyr.com
https://git.violka-it.net/leroymathy9351 git.violka-it.net
https://cloveebiz.com.ng/@valentinapelle?page=about https://cloveebiz.com.ng
http://repo.magicbane.com/rosalind97t834 repo.magicbane.com
https://naijasingles.net/@virginiaguinn https://naijasingles.net/
https://www.ttd.group/yasminhowland8 https://www.ttd.group/yasminhowland8
https://tubepeer.com/@kerrioxley251?page=about tubepeer.com
References:
http://git.fbonazzi.it/ashley05946798
https://i10audio.com · April 18, 2026 at 10:44 am
laughlin nevada casinos
https://crazyworksports.com/@staciekoertig8?page=about https://crazyworksports.com/@staciekoertig8?page=about
https://rjlove.org/@cesarkrichauff rjlove.org
https://wopid.io/@latashiacaroth?page=about wopid.io
https://play.ophirstudio.com//@merryesposito0?page=about play.ophirstudio.com
https://live.eposbd.net/@alannahmoffett?page=about live.eposbd.net
https://code.tczkiot.com/tobybodnar4292 code.tczkiot.com
https://git.adityagupta.dev/melindabown087 https://git.adityagupta.dev/
https://homeablazebyhispresence.dennmachinery.com/@joycelynrowntr?page=about homeablazebyhispresence.dennmachinery.com
https://rjlove.org/@cesarkrichauff https://rjlove.org
https://gitea.adber.tech/nestorwoollard gitea.adber.tech
https://hellomusic.app/traceewao42314 hellomusic.app
https://gitea.gimmin.com/beryl19z266643 https://gitea.gimmin.com/
https://git.cymnb.com/berylpate51466 git.cymnb.com
https://mygit.kikyps.com/elvissellheim mygit.kikyps.com
http://app.venusroyale.date/@freddybabbidge http://app.venusroyale.date/@freddybabbidge
https://gitea.shizuka.icu/mickivanotterl gitea.shizuka.icu
https://git.danpeak.co.uk/dannynunn53637 git.danpeak.co.uk
https://gitea.kdlsvps.top/corrinedunbabi gitea.kdlsvps.top
References:
https://shirme.com/alejandrogeogh
TOTO138 LOGIN · April 20, 2026 at 4:06 pm
TOTO138 LOGIN
https://graph.org/ · April 20, 2026 at 7:03 pm
References:
Cannery casino las vegas
References:
https://graph.org/Skycrown-Casino-Australia-Expert-Review–Bonuses-04-20
woo casino player experiences · April 20, 2026 at 9:08 pm
References:
https://graph.org/Woo-Casino-Review-Get-Your-Exclusive-Welcome-Bonus-and-Free-Spins-04-20 casino australia review
graph.org · April 21, 2026 at 9:15 am
References:
Gamehouse casino plus
References:
https://graph.org/Top-Casino-Online-Australia-Sites-2026-04-20
Skycrown Casino app download · April 21, 2026 at 12:04 pm
References:
Top 5 australian online casinos
References:
https://graph.org/Casino-Online-Expert-Guide-to-Smart-Play-04-20
https://trustguru.com.br/autores · April 21, 2026 at 9:21 pm
Fortune Ox em rotação curta teve bom desempenho em sessões rápidas.
부산호빠 · April 22, 2026 at 2:32 am
부산호빠
TOTO138 · April 23, 2026 at 2:13 am
TOTO138 LOGIN
TOTO138 · April 23, 2026 at 2:15 am
TOTO138 LOGIN
casino-cz.online-spielhallen.de · April 26, 2026 at 2:35 am
References:
Spotlight 29 casino
References:
https://casino-cash-o-lot.online-spielhallen.de/
https://ice-casino-deutschland.online-spielhallen.de/ · April 26, 2026 at 3:38 am
References:
Vegas casino magnate steve
References:
https://venetian-casino-restaurants.online-spielhallen.de/
https://book-of-dead-casinos.online-spielhallen.de · April 26, 2026 at 5:00 am
References:
Ho chunk casino madison
References:
https://verde-casino-aktionscode-bestandskunden.online-spielhallen.de/
创建Binance账户 · April 26, 2026 at 11:51 am
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Krefeld · April 26, 2026 at 8:40 pm
References:
Karlsruhe
References:
https://new-casino-no-deposit-bonus-codes.online-spielhallen.de/
Würzburg · April 26, 2026 at 8:56 pm
References:
Pforzheim
References:
https://westgate-las-vegas-resort-and-casino.online-spielhallen.de/
Munich (München) · April 26, 2026 at 11:40 pm
References:
Düsseldorf
References:
https://candy-casino.online-spielhallen.de/
Mönchengladbach · April 26, 2026 at 11:42 pm
References:
Cologne (Köln)
References:
https://ocean-casino-resort.online-spielhallen.de/
Gelsenkirchen · April 27, 2026 at 12:52 am
References:
Erfurt
References:
https://verde-casino-no-deposit-bonus-codes.online-spielhallen.de/
Saarbrücken · April 27, 2026 at 1:06 am
References:
Ingolstadt
References:
https://namur-casino-poker.online-spielhallen.de/
Darmstadt · April 27, 2026 at 4:37 am
References:
Lübeck
References:
https://casino-international.online-spielhallen.de/
Krefeld · April 27, 2026 at 5:04 am
References:
Oldenburg
References:
https://cobra-casino.online-spielhallen.de/
graph.org · April 28, 2026 at 4:47 am
References:
Treasure bay casino
References:
https://graph.org/The-Lotto-App-Download-04-27
https://graph.org · April 28, 2026 at 8:08 am
References:
888 casino
References:
https://graph.org/The-Ville-Resort-Casino-Prices-04-27
ph646 · April 29, 2026 at 1:57 pm
Thank you for the good writeup. It in fact was a amusement account it.
Look advanced to far added agreeable from you!
However, how can we communicate?
Регистрация в binance · April 30, 2026 at 2:41 am
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://www.binance.bh/fr-AF/register?ref=JHQQKNKN
www.automingwei.com · April 30, 2026 at 3:43 pm
Erfarne spilleres valg af casino udbetaling
http://x.kongminghu.com/home.php?mod=space&uid=431174 http://x.kongminghu.com/home.php?mod=space&uid=431174
http://asresin.cn/home.php?mod=space&uid=763544 http://asresin.cn/home.php?mod=space&uid=763544
https://bridgedesign.space/wiki/Dette_er_de_10_bedste_casino_sider_i_Danmark_2026 https://bridgedesign.space
http://support.roombird.ru/index.php?qa=user&qa_1=felonycrow75 http://support.roombird.ru/
https://nutritionwiki.space/wiki/Bedste_Online_Casino_Udbetaling_Hurtige_Danske_Casinoer_2026 nutritionwiki.space
https://forum.board-of-metal.org/user-32455.html https://forum.board-of-metal.org/
http://asresin.cn/home.php?mod=space&uid=763540 asresin.cn
http://uchkombinat.com.ua/user/resultbeer1/ uchkombinat.com.ua
https://may22.ru/user/ugandafood0/ may22.ru
https://www.tianjinzhaopin.cn/home.php?mod=space&uid=1191845 http://www.tianjinzhaopin.cn
https://ancientroman.space/wiki/Bedste_Udbetaling_Casino_2026_Hurtigste_Udbetalinger ancientroman.space
https://a-taxi.com.ua/user/harborpolice05/ a-taxi.com.ua
https://hedgedoc.eclair.ec-lyon.fr/s/okUOb_niq hedgedoc.eclair.ec-lyon.fr
https://gardenwiki.site/wiki/Guide_til_casinoudbetaling_Vlg_et_casino_med_hurtig_udbetaling https://gardenwiki.site
https://pbase.com/iraqbrandy40/ pbase.com
http://xn--l1ae1d.xn--b1agalyeon.xn--80adxhks/user/areagrill65/ http://l1ae1d.творение.москва/user/areagrill65
https://dailyfantasyrankings.com.au/public/forum/user-188054.html https://dailyfantasyrankings.com.au/public/forum/user-188054.html
https://pad.stuve.uni-ulm.de/s/TZNt6CvYeM pad.stuve.uni-ulm.de
References:
http://warblog.hys.cz/user/piscescell5/
eurogulfcareers.com · April 30, 2026 at 4:09 pm
Casinoer med høj udbetalingskvote
https://jobs.foodtechconnect.com/companies/bedste-udbetaling-casino-2026-hurtigste-udbetalinger/ jobs.foodtechconnect.com
https://git.salingbot.com/muhammad09p535 git.salingbot.com
https://git.flymiracle.com/svenbuckingham https://git.flymiracle.com
https://unidemics.com/employer/bedste-udbetaling-casino-2026-hurtigste-udbetalinger/ https://unidemics.com
https://xn--lpris-iua.nu/debbiefugate26/bedste-danske-casino-udbetalinger9552/wiki/Casinoer-med-den-bedste-udbetaling-i-Danmark-2026 lpris-iua.nu
https://www.workforce.beparian.com/employer/de-bedste-online-casino-sider-i-danmark/ http://www.workforce.beparian.com
http://code.sz-chaohui.cn/janmayberry390 http://code.sz-chaohui.cn/janmayberry390
https://candidates.giftabled.org/employer/nye-casino-bedste-nye-online-casinoer-i-danmark-2026/ candidates.giftabled.org
https://gitea.lelespace.top/johniebolduc8 gitea.lelespace.top
https://code.nspoc.org/theoo35946184/theo2004/wiki/De-bedst-betalende-slots-i-Danmark-Top-gevinster-og-bonus https://code.nspoc.org/theoo35946184/theo2004/wiki/De-bedst-betalende-slots-i-Danmark-Top-gevinster-og-bonus
https://git.saike.fun:9755/robertostrickl/roberto1990/wiki/Bedste-danske-p%C3%A5-casinoer-i-2026-Forblive-10-i-kraft-af-afgift git.saike.fun
https://git.sskuaixiu.com/dariowick90817 https://git.sskuaixiu.com/dariowick90817
https://gitea.johannes-hegele.de/emiliearmer503 https://gitea.johannes-hegele.de
https://www.advertiseajob.co.uk/employer/de-23-bedste-betting-sider-i-april-2026-%ef%b8%8f-guide-til-odds-sider/ https://www.advertiseajob.co.uk/
https://forum.otoportal.net/index.php?action=profile;u=40541 forum.otoportal.net
https://www.rhcapital.cl/employer/bedste-online-casino-udbetaling-april-2026/ http://www.rhcapital.cl
http://kimnpark.net/gnu5/bbs/board.php?bo_table=2014Taiwan&wr_id=11211 http://kimnpark.net/gnu5/bbs/board.php?bo_table=2014Taiwan&wr_id=11211
https://kition.mhl.tuc.gr/shielaoliver51 kition.mhl.tuc.gr
References:
https://git.wisder.net/kellilithgow69
pic.murakumomura.com · April 30, 2026 at 4:25 pm
største
https://feferferramentas.com.br/how-to-improve-fuel-efficiency-with-the-right-fuel-delivery-system/ feferferramentas.com.br
https://packmann-umzuege.de/2023/06/22/maximizing-productivity-tips-for-a-successful-workday/ https://packmann-umzuege.de/2023/06/22/maximizing-productivity-tips-for-a-successful-workday/
http://kenbc.nihonjin.jp/album/album.cgi?mode=detail&no=193 http://kenbc.nihonjin.jp/album/album.cgi?mode=detail&no=193
https://mark0479.ru/2023/06/28/boost-productivity-and-efficiency-with-our-range-of-digital/ mark0479.ru
https://kingsmenmarketing.com/search-engine-marketing/ kingsmenmarketing.com
https://fci.ind.br/envase-de-produtos-quimico-blog/envase-e-fracionamento-de-produtos-quimicos/ fci.ind.br
https://blog-reflection.mycodecare.com/food/the-flavor-of-photography-exploring-cultural-food-photography/ blog-reflection.mycodecare.com
https://hohohoiku.com/working-hoikusikaku/ hohohoiku.com
https://formation-diagnostiqueur-immobilier.net/le-role-du-diagnostiqueur-dans-une-vente-immobiliere/ formation-diagnostiqueur-immobilier.net
https://ceeceepalms.com/front-page/ https://ceeceepalms.com/front-page
https://www.fj-tokyo.jp/otsumami/meet/5311/ https://www.fj-tokyo.jp/
http://www2k.biglobe.ne.jp/~murasaki/cgi-bin/wwwboard.cgi http://www2k.biglobe.ne.jp/~murasaki/cgi-bin/wwwboard.cgi
https://plassriosolucoes.com/2023/07/10/building-a-strong-startup-team-skills-and-roles/ plassriosolucoes.com
http://atachin.es/index.php/component/k2/item/10-noticia-2 atachin.es
https://yadeasp.com.br/mastering-growth-with-proven-business-tips/ https://yadeasp.com.br/mastering-growth-with-proven-business-tips/
https://projetoperpetuosocorro.com.br/the-joy-of-giving-serving-others-with-a-generous-heart/ projetoperpetuosocorro.com.br
https://magazinechegou.com.br/2024/05/27/how-to-keep-your-bathroom-germ-free/ magazinechegou.com.br
https://christambassadors.edu.gh/2021/10/08/our-day-manasseh-sends-strong-message-to-critics-of-gifts-for-9-year-old-oswald/ https://christambassadors.edu.gh/
References:
https://codecraftstudios.com.br/from-idea-to-execution-a-startup-journey/
learn more · April 30, 2026 at 9:48 pm
Fortune Tiger replays are studied for entry timing patterns.
phoebe.roshka.com · May 1, 2026 at 4:16 am
References:
Høje
References:
http://git.ibossay.com:3000/myrtissawtell6/2774blackcoin.co/wiki/De-bedste-online-casino-udbetalinger-i-Danmark-april-2026
cyltalentohumano.com · May 1, 2026 at 6:19 am
Casino bonus med høj udbetaling
http://55x.top:9300/ayokeenan84660/4737358/wiki/Casino-udbetaling%3A-Hurtig-og-sikker-udbetaling 55x.top
https://git.arnosti.net.br/carinfoye23879 git.arnosti.net.br
http://www.tm-jikayo.com/larhondabenavi http://www.tm-jikayo.com
https://vila.go.ro/jannettehales4 vila.go.ro
http://gitea.yiban.com.tw:3030/mervingregor59 gitea.yiban.com.tw
https://jobs.thetalentservices.com/employer/top-10-casinoer-i-dk-top-10-online-casinoer https://jobs.thetalentservices.com
https://hero-cloud-stg-code.cnbita.com/wilfredsorrell/wilfred1997/wiki/De-Bedste-Udbetalinger-p%C3%A5-Online-Casinoer-i-Danmark-i-2026 hero-cloud-stg-code.cnbita.com
https://internskill.in/companies/casinoer-med-den-bedste-udbetaling-i-danmark-2026/ internskill.in
https://git.slegeir.com/kathlenerehkop https://git.slegeir.com/kathlenerehkop
https://xn--lpris-iua.nu/marissa4011843 https://lpris-iua.nu/marissa4011843
https://forum.otoportal.net/index.php?action=profile;u=40543 forum.otoportal.net
https://wedeohire.com/employer/bedste-online-casinoer-i-danmark-vores-eksperters-topvalg/ wedeohire.com
http://gitea.mikarsoft.com/melvine2819386 http://gitea.mikarsoft.com/melvine2819386
https://git.bp-web.app/jewelrodman511 https://git.bp-web.app/
https://git.nusaerp.com/marlongreenham git.nusaerp.com
https://syq.im:2025/itvhai55662588 syq.im
https://git.ihatemen.uk/jordanboulton git.ihatemen.uk
https://fanajobs.com/profile/freyakline4386 fanajobs.com
References:
http://git.youkehulian.cn/raymonport312
pbase.com · May 1, 2026 at 6:52 am
Hvorfor
https://actualites.cava.tn/user/slaveregret48/ actualites.cava.tn
http://x.kongminghu.com/home.php?mod=space&uid=431184 x.kongminghu.com
https://xn--41-4lcpj.xn--j1amh/user/recordeight05/ 41-4lcpj.укр
http://quanbixuetang.com/home.php?mod=space&uid=236453 http://quanbixuetang.com/
https://500px.com/p/valentinencpellison 500px.com
http://sglpw.cn/home.php?mod=space&uid=684218 http://sglpw.cn/home.php?mod=space&uid=684218
http://alfa-power.de/member.php?action=profile&uid=20058 alfa-power.de
http://downarchive.org/user/chessnumber83/ http://downarchive.org/
https://dreevoo.com/profile.php?pid=1581463 https://dreevoo.com/
https://freudwiki.site/wiki/RTP_Return_to_Player_tilbagebetalingsprocenter https://freudwiki.site/wiki/RTP_Return_to_Player_tilbagebetalingsprocenter
https://eskisehiruroloji.com/sss/index.php?qa=user&qa_1=leaftrick61 https://eskisehiruroloji.com/
https://gamingwiki.space/wiki/Bedste_online_casinoer_i_Danmark_med_fokus_p_udbetalinger_2026 gamingwiki.space
https://travelersqa.com/user/polishorchid95 https://travelersqa.com/
http://sglpw.cn/home.php?mod=space&uid=684218 http://sglpw.cn/home.php?mod=space&uid=684218
https://healy-hansen-2.mdwrite.net/spilleautomater-med-hojeste-rtp-i-2026-top-10-slots-i-dk https://healy-hansen-2.mdwrite.net/spilleautomater-med-hojeste-rtp-i-2026-top-10-slots-i-dk
https://topsitenet.com/profile/slipneedle73/1703114/ topsitenet.com
https://digitaltibetan.win/wiki/Post:Casinoer_med_den_bedste_udbetaling_i_Danmark_2026 digitaltibetan.win
http://szw0.com/home.php?mod=space&uid=1009929 szw0.com
References:
https://notes.io/ebM8m
https://md.un-hack-bar.de/s/e9w4LPazuz · May 1, 2026 at 6:56 am
Sikre udbetalinger på danske casinoer
https://atomcraft.ru/user/hyenabeer5/ atomcraft.ru
https://diego-maradona.com.az/user/piscesbrush8/ https://diego-maradona.com.az/
https://moiafazenda.ru/user/oysterthrone57/ moiafazenda.ru
http://madk-auto.ru/user/ugandabamboo2/ http://madk-auto.ru/
https://lam-bowling-3.mdwrite.net/dette-er-spillemaskinerne-med-den-hojeste-udbetaling lam-bowling-3.mdwrite.net
https://g.clicgo.ru/user/spongeplot24/ https://g.clicgo.ru/user/spongeplot24
https://pbase.com/iraqbrandy40/ pbase.com
https://prpack.ru/user/thrilltrick20/ https://prpack.ru/user/thrilltrick20
https://commonwiki.space/wiki/Spillemaskiner_med_hj_RTP_Maksimer_Dine_Gevinster_og_Spilletid https://commonwiki.space
http://www.bmw-workshop.com/member.php?action=profile&uid=35748 http://www.bmw-workshop.com/member.php?action=profile&uid=35748
https://sonnik.nalench.com/user/ramiepoint56/ sonnik.nalench.com
https://schoolido.lu/user/cloudmice1/ schoolido.lu
https://bridgedesign.space/wiki/Casinoer_med_den_bedste_udbetaling_i_Danmark_2026 bridgedesign.space
https://notes.medien.rwth-aachen.de/TmmcIK2cTHSaXzFr4EJnOA/ https://notes.medien.rwth-aachen.de/
https://brewwiki.win/wiki/Post:Bedste_Online_Slots_2026_Top_10_Populre_Spillemaskiner_med_Hj_RTP brewwiki.win
https://skyscrapperwiki.site/wiki/Online_casinoer_i_danmark_Sikkerhed_regler_og_gevinster skyscrapperwiki.site
https://king-bookmark.stream/story.php?title=vinderchancer-laes-alt-om-dine-vinderchancer-for-spil-pa-nettet https://king-bookmark.stream/story.php?title=vinderchancer-laes-alt-om-dine-vinderchancer-for-spil-pa-nettet
http://cqr3d.ru/user/bulbeast62/ http://cqr3d.ru/user/bulbeast62
References:
https://dyhr-kerr-3.federatedjournals.com/bedste-udbetaling-casino-2026-hurtigste-udbetalinger
http://t.044300.net/home.php?mod=space&uid=2687991 · May 1, 2026 at 8:21 am
References:
Højeste gevinstmuligheder online casino
References:
http://www.1gmoli.com/home.php?mod=space&uid=592078
bmxmuseum.se · May 1, 2026 at 8:28 am
Bedste danske casinoer med høj RTP
https://packmann-umzuege.de/2023/06/22/the-art-of-negotiation-tips-for-successful-business-deals/ packmann-umzuege.de
https://aziagcon.kz/?p=158 aziagcon.kz
https://clin.psc.br/everything-about-cardio/ clin.psc.br
https://uboatelangana.com/2024/10/07/5-essential-tips-for-a-sparkling-clean-home/ uboatelangana.com
https://maiitrii.com/creating-magical-winter-wonderland-decor/ maiitrii.com
http://aocuoizulias.com/%d0%b1%d0%b0%d0%bb%d0%bb%d0%be%d0%bd-%d0%b8%d0%b3%d1%80%d0%b0-%d1%81%d0%ba%d0%b0%d1%87%d0%b0%d1%82%d1%8c-%d0%ba%d0%b0%d0%ba-%d0%b1%d1%8b%d1%81%d1%82%d1%80%d0%be-%d0%b8-%d0%b1%d0%b5%d0%b7%d0%be%d0%bf/ aocuoizulias.com
https://royaltech.ng/2024/04/25/understanding-electrical-codes-a-guide-for-diy-enthusiasts/ royaltech.ng
https://duckdrinks.com.br/index.php/2025/03/31/the-ultimate-guide-to-superfoods-and-benefits/ https://duckdrinks.com.br
https://maratus.co.uk/top-tools-every-startup-should-know/ https://maratus.co.uk/top-tools-every-startup-should-know/
https://mahabbahtravel.com/celebrating-diversity-embracing-unity-in-christ/ https://mahabbahtravel.com
https://scrapcharityvat.com/portfolio/dads-in-africa/ https://scrapcharityvat.com
http://importpartsonline.sakura.tv/album/album.cgi?mode=detail&no=18&page=0 http://importpartsonline.sakura.tv/album/album.cgi?mode=detail&no=18&page=0
https://lawritjournal.org.ng/the-judiciary-as-an-electoral-arbiter-judicial-adjudication-and-the-protection-of-electoral-integrity-in-democracies/ https://lawritjournal.org.ng/
https://dmakkah.co/EGP/2022/07/01/introducing-this-amazing-tour/ dmakkah.co
https://afdob.tanassam.com/solar-power-in-developing-nations-brightening-lives/ afdob.tanassam.com
https://ervaseencantos.pt/molho-bearnaise-historia-origem-ingredientes-preparacao-e-harmonizacoes-gastronomicas/ ervaseencantos.pt
https://insideethiopiatours.com/how-we-started-one-of-the-1-travel-companies-in-ethiopia/ insideethiopiatours.com
https://newhomehonduras.com/2025/05/04/top-tools-every-startup-should-know-2/ newhomehonduras.com
References:
https://harald-pfeifer.com/2022/12/21/club-membership-opitons/
http://new.cherrycroft.uk · May 1, 2026 at 9:08 am
Fakta om casino udbetalingsprocenter
https://peter-schroeder.eu/Blog;focus=TKOMSI_com_cm4all_wdn_Flatpress_22119493&path=&frame=TKOMSI_com_cm4all_wdn_Flatpress_22119493?x=entry:entry200512-074628%3Bcomments:1 peter-schroeder.eu
https://putrapratamaprecast.com/blog/harga-u-ditch-kudus-terbaru-2025/ putrapratamaprecast.com
https://mathias-wille.hier-im-netz.de/Startseite;focus=TKOMSI_com_cm4all_wdn_Flatpress_21838727&path=&frame=TKOMSI_com_cm4all_wdn_Flatpress_21838727?x=entry:entry260305-135416%3Bcomments:1 mathias-wille.hier-im-netz.de
https://startbetblog.com/como-depositar-na-start-bet/ https://startbetblog.com/
http://ocin.cn/views.asp?prono=1753 ocin.cn
https://nepalhimalayantrails.com/packages/langtang-valley-short-trek/ https://nepalhimalayantrails.com/packages/langtang-valley-short-trek
https://iaipeag.org/solar-energy-financing-options-making-solar-affordable/ iaipeag.org
http://www.laufmarkt.de/Laufmarkt-Blog;focus=TKOMSI_com_cm4all_wdn_Flatpress_25448945&frame=TKOMSI_com_cm4all_wdn_Flatpress_25448945?x=entry:entry220516-220744%3Bcomments:1 http://www.laufmarkt.de
http://kenbc.nihonjin.jp/album/album.cgi?mode=detail&no=352 kenbc.nihonjin.jp
https://www.eurasier-von-der-schulenburg.de/Wuerfe;focus=TKOMSI_com_cm4all_wdn_Flatpress_20761264&frame=TKOMSI_com_cm4all_wdn_Flatpress_20761264?x=entry:entry250419-055507%3Bcomments:1 http://www.eurasier-von-der-schulenburg.de
https://costurese.com.br/2024/04/17/the-ultimate-guide-to-learning-python-programming/ https://costurese.com.br
https://insideethiopiatours.com/es/transito-etiopia-recorrido-ciudad-addis-abeba/ insideethiopiatours.com
https://gbrandmarketing.com.br/top-tools-every-startup-should-know/ https://gbrandmarketing.com.br/top-tools-every-startup-should-know
https://tatakiterraplanagem.com.br/2023/09/25/how-solar-energy-works-from-sunlight-to-electricity/ https://tatakiterraplanagem.com.br/
https://parlamento-cantabria.es/informacion-general/fernando-andreu-merelles?page=2899 parlamento-cantabria.es
https://iacapital-ao.com/connecting-with-natures-tranquil-essence/ iacapital-ao.com
https://omtechcommunication.com.au/index.php/2023/09/25/solar-power-in-developing-nations-brightening-lives/ https://omtechcommunication.com.au/index.php/2023/09/25/solar-power-in-developing-nations-brightening-lives
https://eatsplorer.com/sunrise-coffee-safari-experience-in-cape-town/ eatsplorer.com
References:
https://tanzaniawithkeny.com/2023/08/21/exploring-the-beauty-of-mother-nature/
www.blade-edge.com · May 1, 2026 at 9:21 am
Casinoer med dokumenteret høj udbetaling
https://www.digitel-srl.it/home/rectangle-594-1/ https://www.digitel-srl.it/home/rectangle-594-1
https://lensakalimantan.com/sudirman-cup-2025-indonesia-bantai-denmark-ana-tiwi-menang/ https://lensakalimantan.com/sudirman-cup-2025-indonesia-bantai-denmark-ana-tiwi-menang
https://baerbelsgarten.de/;focus=TKOMSI_com_cm4all_wdn_Flatpress_20514587&path=?x=entry:entry220810-111350%3Bcomments:1 https://baerbelsgarten.de/;focus=TKOMSI_com_cm4all_wdn_Flatpress_20514587&path=?x=entry:entry220810-111350;comments:1
https://template121.webekspor.com/banyak-fasilitas-pembiayaan-perumahan-untuk-pns-rugi-kalau-tidak-dimanfaatkan-2/ template121.webekspor.com
https://zestic.in/the-importance-of-building-a-strong-brand-identity/ https://zestic.in/the-importance-of-building-a-strong-brand-identity
https://iaipeag.org/solar-energy-financing-options-making-solar-affordable/ https://iaipeag.org/solar-energy-financing-options-making-solar-affordable/
https://scrapcharityvat.com/portfolio/rural-children/ https://scrapcharityvat.com/
https://missmister.com.br/women-days-discounts/ missmister.com.br
https://delcomfurniture.com/best-stretches-for-lower-back-pain/ https://delcomfurniture.com/best-stretches-for-lower-back-pain/
https://vkfruitfarm.ca/2025/03/31/the-ultimate-guide-to-superfoods-and-benefits/ https://vkfruitfarm.ca/2025/03/31/the-ultimate-guide-to-superfoods-and-benefits/
https://adamxplore.com/hidden-gems-exploring-off-the-beaten-path-destinations/ https://adamxplore.com
https://igniterecruitement.co.uk/2024/04/05/hidden-gems-exploring-off-the-beaten-path-destinations/ igniterecruitement.co.uk
https://tpc.ng/tpc-in-partnership-with-mo-oladapo-begins-2025-mentorship-program-through-the-top-performers-academy/ tpc.ng
https://mantiqueiraengenharia.com.br/2023/06/22/the-importance-of-building-a-strong-brand-identity/ https://mantiqueiraengenharia.com.br/2023/06/22/the-importance-of-building-a-strong-brand-identity/
http://shirayuki.saiin.net/~alicelinks/CMS/support/cbbs.cgi?mode=al2&namber=19538&rev=1&no=0 http://shirayuki.saiin.net/~alicelinks/CMS/support/cbbs.cgi?mode=al2&namber=19538&rev=1&no=0
https://freevisitorcounter.net/berapa-diamond-efek-recall-ducati-mobile-legends-ml-esportsku/ freevisitorcounter.net
https://nisc.com.co/mastering-time-management-key-to-business-success/ https://nisc.com.co
https://harald-pfeifer.com/2022/12/21/club-membership-opitons/ harald-pfeifer.com
References:
https://terepanoficial.com.br/into-the-wild-adventures-in-the-heart-of-nature/
http://www.automingwei.com/ · May 1, 2026 at 11:50 am
References:
Bedste odds på online casino
References:
https://commonwiki.space/wiki/Online_Casino_mit_hoher_Auszahlungsquote_2026_RTPTabelle
platform.joinus4health.eu · May 1, 2026 at 11:58 am
References:
Hvor får man den højeste casino udbetaling
References:
https://sundaynews.info/user/boxrotate31/
http://bbs.xingxiancn.com/home.php?mod=space&uid=890993 · May 1, 2026 at 12:00 pm
References:
Tilbage
References:
http://xuetao365.com/home.php?mod=space&uid=673310
nrimatchmaking.com · May 1, 2026 at 12:04 pm
Bedste platforme til casino gevinster
http://xianyuhome.cn:11013/fanny76960563 xianyuhome.cn
http://tools.refinecolor.com/shellanealy294 tools.refinecolor.com
http://geekhosting.company/bernadetteburb geekhosting.company
https://talentfrontiers.ph/employer/beste-online-casinos-mit-paypal-2026-vergleich/ talentfrontiers.ph
https://koseongnam.com/lttrubin04520 https://koseongnam.com/lttrubin04520
https://gitea.gentronhealth.com/lashondacaznea https://gitea.gentronhealth.com/
https://git.dieselor.bg/mildredloftin7 https://git.dieselor.bg/mildredloftin7
https://git.clubeye.net/lorrainequilty https://git.clubeye.net
https://iratechsolutions.com/employer/beste-casinos-mit-hohem-rtp-2026-top-auszahlungsquoten/ iratechsolutions.com
https://git.smart-tool.jp/ceceliacunniff git.smart-tool.jp
https://aitune.net/josephineliger https://aitune.net
http://newchanpin.yuntangkeji.cn:33009/neil82m1077599/blackcoin1705/wiki/Slots-mit-hoher-Gewinnchance-2026-Spielautomaten-mit-Top-RTP http://newchanpin.yuntangkeji.cn/
https://git.auth.com.br/kraigmackersey https://git.auth.com.br/
http://gitea.yiban.com.tw:3030/vidaspencer73 http://gitea.yiban.com.tw:3030/vidaspencer73
https://quickdate.arenascript.de/@janeenhogben7 https://quickdate.arenascript.de/
https://git.morozoff.pro/ottol240291098/8152478/wiki/PayPal-Casino-Liste-2026:-Top-Online-Casinos-mit-PayPal-Einzahlung https://git.morozoff.pro
https://git.apextoaster.com/christiegrasby git.apextoaster.com
https://lcateam.com/employer/die-besten-echtgeld-casinos-im-internet-2026-getestet/ https://lcateam.com/employer/die-besten-echtgeld-casinos-im-internet-2026-getestet/
References:
http://git.rabbittec.com/guyicely338670/5829907/wiki/PayPal+Casino+Liste+2026%253A+Top+Online+Casinos+mit+PayPal+Einzahlung
www.fepp.org.ec · May 1, 2026 at 12:08 pm
Valg af det rigtige casino for udbetaling
https://git.nusaerp.com/guillermohartn git.nusaerp.com
https://www.oddmate.com/@uabismael5251 https://www.oddmate.com/@uabismael5251
https://jobsbotswana.info/companies/11-beste-online-casinos-in-deutschland-2026-seit-1995/ jobsbotswana.info
https://dev.kiramtech.com/oscar53z147333 dev.kiramtech.com
https://platform.giftedsoulsent.com/ezequielfehon2 https://platform.giftedsoulsent.com/ezequielfehon2
http://code.sz-chaohui.cn/pammacdonell96 http://code.sz-chaohui.cn/
https://mycrewdate.com/@theo54m7759361 https://mycrewdate.com/
https://gitea.johannes-hegele.de/melvaholifield/1264304/wiki/Die-besten-Online-Casinos-in-Deutschland-2026-Top-w%C3%A4hlen gitea.johannes-hegele.de
http://merchantale.com/harryperalta62 merchantale.com
https://www.oddmate.com/@colbynaylor023 http://www.oddmate.com
https://spechrom.com:443/bbs/board.php?bo_table=service&wr_id=449842 https://spechrom.com:443/bbs/board.php?bo_table=service&wr_id=449842
http://git.fbonazzi.it/lizettewardill git.fbonazzi.it
http://kreativemaniac.com/read-blog/2020_11-beste-online-casinos-in-deutschland-2026-seit-1995.html kreativemaniac.com
http://git.rabbittec.com/francis2671265 git.rabbittec.com
https://https://www.fepp.org.ec/teresajeffcott/noechristison3 https://www.fepp.org.ec/
http://globaldream.or.kr/bbs/board.php?bo_table=sub08_02&wr_id=319038 globaldream.or.kr
https://gitea-inner.fontree.cn/veroniquedittm/veronique1996/wiki/Wie-funktionieren-Online-Slots%3F-%E2%AD%90%EF%B8%8F-RTP-%26-Auszahlungsquote-einfach-erkl%C3%A4rt-2025 gitea-inner.fontree.cn
https://gladjobs.com/employer/beste-online-casinos-deutschland-april-2026/ gladjobs.com
https://www.corrillos.com.co/el-nuevo-plato-de-nuestra-bucaramanga-cacerolazo-santandereano/ · May 1, 2026 at 12:13 pm
højeste
https://aiomoshield.com/the-secret-to-successful-social-media-ads/ https://aiomoshield.com
https://freevisitorcounter.net/cara-mendapatkan-mp40-carnival-carnage-di-incubator-free-fire-ff-esportsku/ https://freevisitorcounter.net
https://horizonmagazineonline.com.ng/2025/06/09/plateau-government-moves-to-tackle-climate-crisis-with-grassroots-action-and-tree-planting/ horizonmagazineonline.com.ng
https://escolademaespiracicaba.org.br/cuisine-and-culture-a-culinary-journey-around-the-world/ https://escolademaespiracicaba.org.br/cuisine-and-culture-a-culinary-journey-around-the-world/
https://alternative.media/the-most-immoral-man-ive-ever-met-piers-morgan-vs-cenk-uygur-and-rabbi-shmuley/ https://alternative.media
https://ilanabilingualschool.com/tiny-scientists-on-the-loose-preschool-science-wonders-2/ https://ilanabilingualschool.com/tiny-scientists-on-the-loose-preschool-science-wonders-2
https://irds-center.com/2025/06/29/rusiyada-az%c9%99rbaycanlilara-qarsi-tor%c9%99dilmis-hadis%c9%99-m%c9%99qs%c9%99dyonludur-mutt%c9%99fiqlik-ruhuna-ziddir-politoloq-samir-humb%c9%99tovun-aciqlamasinda/ https://irds-center.com/2025/06/29/rusiyada-azərbaycanlilara-qarsi-torədilmis-hadisə-məqsədyonludur-muttəfiqlik-ruhuna-ziddir-politoloq-samir-humbətovun-aciqlamasinda
https://senepolitique.com/2025/02/cote-divoire-la-cooperation-militaire-continue-avec-la-france-il-ny-a-pas-de-rupture/ https://senepolitique.com/2025/02/cote-divoire-la-cooperation-militaire-continue-avec-la-france-il-ny-a-pas-de-rupture/
http://okuzashiki.sakura.ne.jp/oku/cf.cgi?mode=all&namber=40946&rev=1 okuzashiki.sakura.ne.jp
https://nilevalley.edu.sd/eng/?p=985 nilevalley.edu.sd
https://iatraducoes.com.br/2024/04/17/the-ultimate-guide-to-learning-python-programming/ https://iatraducoes.com.br/2024/04/17/the-ultimate-guide-to-learning-python-programming
https://nextgen-comms.com/the-pros-and-cons-of-different-investment-vehicles/ https://nextgen-comms.com
https://carluzservices.com/how-to-maintain-a-clean-office-space/ carluzservices.com
https://www.cardinalwarriors.com/2023/12/26/tiny-tot-adventures-a-peek-into-our-preschool-world/ http://www.cardinalwarriors.com
https://ads.bushtroop-safaris.com/index.php/2023/07/05/discover-the-hidden-gems-best-lesser-known-ebooks/ https://ads.bushtroop-safaris.com/index.php/2023/07/05/discover-the-hidden-gems-best-lesser-known-ebooks
https://getadminate.com/scaling-your-brand-with-smart-strategies/ https://getadminate.com/
http://gsiani01.nayaa.co.kr/bbs/board.php?bo_table=sub04_01&wr_id=18412 gsiani01.nayaa.co.kr
https://liviascleaning.com/gel-polish-guide-long-lasting-colors-for-every-season/ liviascleaning.com
References:
https://sic.org.sa/news-strategic-partner/
daojianchina.com · May 1, 2026 at 12:29 pm
References:
Casinoer med stabil udbetalingsratio
References:
https://mensvault.men/story.php?title=online-casinos-mit-hoechster-auszahlungsquote-2026
https://camtalking.com/@earthabrassard · May 1, 2026 at 12:38 pm
Casinoer med høj gevinstprocent Danmark
https://jobcopae.com/employer/online-casino-mit-hoher-gewinnchance-casinos-mit-hoher-rtp/ jobcopae.com
https://jobs-max.com/employer/online-casinos-mit-schneller-auszahlung-sofortauszahlung/ https://jobs-max.com/employer/online-casinos-mit-schneller-auszahlung-sofortauszahlung/
https://eram-jobs.com/employer/online-casino-mit-sofortauszahlung-2026-beste-anbieter-im-test eram-jobs.com
https://jobsjo.online/employer/slots-mit-hoher-rtp-2026 jobsjo.online
https://git.scinalytics.com/fletchergreeno https://git.scinalytics.com
https://qdate.ru/@maximoconyers0 https://qdate.ru/@maximoconyers0
http://git.dglyoo.com/altonfolse493/blackcoin.co7999/wiki/Casinos-mit-hohem-RTP-2026-96%25-Gewinnchance git.dglyoo.com
http://git.qniao.cn/helencalwell43 http://git.qniao.cn/helencalwell43
https://git.clickforadventure.co/basilkee15407/blackcoin.co9262/wiki/Online-Casino-Auszahlung-2026-Seri%C3%B6se-Casinos-mit-Auszahlung git.clickforadventure.co
https://gt.clarifylife.net/iladobos473212 https://gt.clarifylife.net/iladobos473212
https://arabsfans.com/@kisharochon137 arabsfans.com
https://www.advertiseajob.co.uk/employer/casinos-mit-bester-auszahlungsquote-2026-hohe-gewinnchancen/ https://www.advertiseajob.co.uk
https://git.123doit.com/jesushinchclif git.123doit.com
http://dailyplaza.co.kr/bbs/board.php?bo_table=1003&wr_id=215787 dailyplaza.co.kr
http://www.aionesight.com/klauspulver476 http://www.aionesight.com/klauspulver476
https://dwellorbit.in/employer/bestes-online-casino-2026-top-online-casinos-deutschland-im-vergleich/ dwellorbit.in
https://gitea.kamisama.ovh/rowenaneil203 gitea.kamisama.ovh
https://meeting2up.it/@deidregeiger73 meeting2up.it
References:
http://git.youkehulian.cn/jaunitafikes30
vcs.cozydsp.space · May 1, 2026 at 1:17 pm
References:
Gratis spins med høj udbetaling
References:
https://incisolutions.app/keeley66482769
https://intensedebate.com/people/sparkteller28 · May 1, 2026 at 1:33 pm
https://pad.stuve.uni-ulm.de/s/FX_2zhZWo pad.stuve.uni-ulm.de
https://greecestudies.site/wiki/25_Online_Casinos_mit_hohem_RTP_und_top_Auszahlungsquoten https://greecestudies.site/wiki/25_Online_Casinos_mit_hohem_RTP_und_top_Auszahlungsquoten
https://truckwiki.site/wiki/Online_Casino_mit_hoher_Auszahlungsquote_2026_RTPTabelle truckwiki.site
http://amur.1gb.ua/user/lentilsphynx60/ http://amur.1gb.ua
https://www.forum-joyingauto.com/member.php?action=profile&uid=118523 http://www.forum-joyingauto.com
https://uichin.net/ui/home.php?mod=space&uid=2671689 https://uichin.net/ui/home.php?mod=space&uid=2671689
https://lslv168.com/home.php?mod=space&uid=2540692 https://lslv168.com
https://tvoyaskala.com/user/backtuba42/ tvoyaskala.com
https://nomadwiki.space/wiki/11_Beste_Online_Casinos_in_Deutschland_2026_Seit_1995 https://nomadwiki.space/wiki/11_Beste_Online_Casinos_in_Deutschland_2026_Seit_1995
https://livebookmark.stream/story.php?title=online-casino-mit-hoher-gewinnchance-anbieter-mit-hohen-rtps livebookmark.stream
https://md.swk-web.com/s/KkmcS2QnU md.swk-web.com
https://nomadwiki.space/wiki/11_Beste_Online_Casinos_in_Deutschland_2026_Seit_1995 https://nomadwiki.space/wiki/11_Beste_Online_Casinos_in_Deutschland_2026_Seit_1995
http://www.bmw-workshop.com/member.php?action=profile&uid=35821 http://www.bmw-workshop.com
https://www.forum.uookle.com/home.php?mod=space&uid=1416910 http://www.forum.uookle.com
https://forum.board-of-metal.org/user-32630.html https://forum.board-of-metal.org/
https://materialwiki.site/wiki/Slots_mit_hoher_RTP_2026 materialwiki.site
http://dudoser.com/user/anglemaple09/ http://dudoser.com/user/anglemaple09
https://500px.com/p/andrewskzkgarrett 500px.com
https://hedgedoc.eclair.ec-lyon.fr/s/FtKL1IsKf https://hedgedoc.eclair.ec-lyon.fr/s/FtKL1IsKf
https://www.forum-joyingauto.com/member.php?action=profile&uid=118523 http://www.forum-joyingauto.com
http://xhdyz.cn/home.php?mod=space&uid=766013 xhdyz.cn
References:
http://kuniunet.com/home.php?mod=space&uid=3061125
bbs.jin999.tw · May 1, 2026 at 1:55 pm
References:
Maksimer
References:
https://neoclassical.space/wiki/Beste_Echtgeld_Casinos_2026_Online_Spielotheken_mit_Echtgeld
부산호빠 · May 4, 2026 at 3:39 am
부산호빠
cuenta abierta en Binance · May 6, 2026 at 8:15 am
Your article helped me a lot, is there any more related content? Thanks!
gitea.hoba.dedyn.io · May 6, 2026 at 4:44 pm
References:
Europa casino
References:
https://gitea.hoba.dedyn.io/matthiasgaffne
https://gitea.kamisama.ovh/ · May 6, 2026 at 4:52 pm
References:
Century casino cripple creek
References:
https://gitea.kamisama.ovh/melanie82p8247
career.wg-dcard.com · May 6, 2026 at 6:43 pm
References:
Understanding betting odds
References:
https://career.wg-dcard.com/employer/instant-payid-withdrawal-casino-australia-2026/
towerclimbers.work · May 6, 2026 at 7:21 pm
References:
Great northern casino
References:
https://towerclimbers.work/employer/bonus-system/
mulkinflux.com · May 6, 2026 at 7:58 pm
References:
No deposit bonus binary options
References:
https://mulkinflux.com/employer/best-payid-casinos-australia-2026-instant-aud-withdrawals/
https://www.lizyum.com · May 6, 2026 at 8:02 pm
References:
Live casino maryland
References:
https://www.lizyum.com/@tristanmetcalf
git.esen.gay · May 7, 2026 at 12:02 am
References:
888 casino review
References:
https://git.esen.gay/freyabirmingha
注册获取100 USDT · May 7, 2026 at 4:17 am
Reading your article helped me a lot and I agree with you. But I still have some doubts, can you clarify for me? I’ll keep an eye out for your answers.
dunyya.com · May 7, 2026 at 4:23 am
References:
All slots casino mobile
References:
https://dunyya.com/employer/10-best-payid-casinos-in-australia-for-2026/
https://www.iqconsult.pro/employer/10-best-payid-casinos-in-australia-for-2026 · May 7, 2026 at 6:05 am
References:
No deposit poker bonus
References:
https://www.iqconsult.pro/employer/10-best-payid-casinos-in-australia-for-2026/
https://m.madeu.co.kr/chiquitaalliso · May 7, 2026 at 9:38 am
References:
Suffolk downs casino
References:
https://m.madeu.co.kr/chiquitaalliso
plataforma com bônus de cadastro grátis 2026 · May 8, 2026 at 8:23 pm
Highlight morning: clean cascade chains on Fortune Mouse with rising multipliers.
binance Registrera · May 8, 2026 at 8:48 pm
Your article helped me a lot, is there any more related content? Thanks!
https://www.busforsale.ae/profile/lamardonohoe97 · May 8, 2026 at 11:51 pm
References:
Sky ute casino
References:
https://www.busforsale.ae/profile/lamardonohoe97
findinall.com · May 8, 2026 at 11:52 pm
References:
Casino imdb
References:
https://www.findinall.com/profile/jedfrew075115
pasarinko.zeroweb.kr · May 9, 2026 at 1:56 am
References:
Hummer 2014
References:
http://pasarinko.zeroweb.kr/bbs/board.php?bo_table=notice&wr_id=10298912
jobdoot.com · May 9, 2026 at 1:59 am
References:
Blackjack com
References:
https://jobdoot.com/companies/candy96-casino-australia-100-bonus-real-money-pokies-2026/
https://employmentabroad.com/ · May 9, 2026 at 2:15 am
References:
Best blackjack app
References:
https://employmentabroad.com/companies/candy96-australia-pokies-bonuses-fast-payid-payouts/
complete-jobs.co.uk · May 9, 2026 at 2:19 am
References:
Best penny slot machines to play
References:
https://complete-jobs.co.uk/employer/top-real-money-online-casino-2026
http://hcrw.co.kr/hcrw/bbs/board.php?bo_table=er_board&wr_id=122577 · May 9, 2026 at 2:53 am
References:
Vegas casino magnate steve
References:
http://hcrw.co.kr/hcrw/bbs/board.php?bo_table=er_board&wr_id=122577
inprokorea.com · May 9, 2026 at 3:07 am
References:
Tropicana casino
References:
http://inprokorea.com/bbs/board.php?bo_table=free&wr_id=2983044
kimnpark.net · May 9, 2026 at 6:06 am
References:
Canberra casino
References:
http://kimnpark.net/gnu5/bbs/board.php?bo_table=2014Taiwan&wr_id=13981
http://www.thehispanicamerican.com · May 9, 2026 at 6:17 am
References:
Mill casino
References:
http://www.thehispanicamerican.com/companies/candy96-casino-australia-100-bonus-real-money-pokies-2026/
https://pbase.com/fruitlace3 · May 10, 2026 at 7:27 pm
References:
Roulette probability https://pbase.com/fruitlace3/
www.tikosatis.com · May 10, 2026 at 7:28 pm
References:
Prairie knights casino https://www.tikosatis.com/index.php?page=user&action=pub_profile&id=723431
https://graph.org/ · May 10, 2026 at 8:20 pm
References:
Seminole casino immokalee https://graph.org/RocketPlay-No-Deposit-Bonus-Codes-Australia-May-2026-05-10
https://17610.cn/ · May 10, 2026 at 9:01 pm
References:
William hill slots https://17610.cn/home.php?mod=space&uid=566813
jslt28.com · May 10, 2026 at 9:24 pm
References:
Casino joe pesci http://jslt28.com/home.php?mod=space&uid=3302253
xbymw.com · May 10, 2026 at 10:52 pm
References:
Online roulette play roulette and receive $1500 https://xbymw.com/space-uid-768525.html
molchanovonews.ru · May 11, 2026 at 4:54 am
References:
Best penny slot machines to play https://molchanovonews.ru/user/homeresult7/
nielsen-rubin-3.mdwrite.net · May 11, 2026 at 5:51 am
References:
R&b classics https://nielsen-rubin-3.mdwrite.net/dong-zhi-6502-zhu-shi-qing-bao-qi-ye-fen-xi
easybookmarking.com · May 11, 2026 at 8:06 am
References:
Quapaw casino https://easybookmarking.com/News/instant-casino-login-connexion-et-creation-de-compte-facile/
bookmarkingcentrals.com · May 11, 2026 at 9:50 am
References:
Genting casino southend http://bookmarkingcentrals.com/News/attention-required-cloudflare-4/
bookmark4you.win · May 11, 2026 at 10:06 am
References:
Boylecasino https://bookmark4you.win/story.php?title=best-new-online-casinos-australia-may-2026
https://dudoser.com/user/weaseladult97/ · May 11, 2026 at 10:40 am
References:
Video poker download https://dudoser.com/user/weaseladult97/
hker2uk.com · May 11, 2026 at 10:49 am
References:
Slots com http://www.hker2uk.com/home.php?mod=space&uid=5555481
https://www.9tj.net/ · May 11, 2026 at 11:06 am
References:
Santa ana casino https://www.9tj.net/home.php?mod=space&uid=550003
platform.joinus4health.eu · May 11, 2026 at 3:23 pm
References:
Crown europe casino https://platform.joinus4health.eu/forums/users/russiazinc11/
myplaceholders.com · May 11, 2026 at 5:27 pm
References:
Casino phoenix az https://myplaceholders.com/News/bunny96-casino-honest-layout-fast-payouts-a-pokie-focus-that-actually-works/
http://jindousa.cn/bbs/home.php?mod=space&uid=354334 · May 11, 2026 at 6:12 pm
References:
Lady luck casino las vegas http://jindousa.cn/bbs/home.php?mod=space&uid=354334
https://www.demilked.com/author/dayverse56/ · May 11, 2026 at 7:55 pm
References:
Casino gaming https://www.demilked.com/author/dayverse56/
http://www.jzq5.cn · May 11, 2026 at 8:16 pm
References:
Seminole hard rock casino tampa http://www.jzq5.cn/space-uid-350626.html
http://auto-file.org/member.php?action=profile&uid=1277081 · May 11, 2026 at 10:34 pm
References:
Ameristar casino st charles mo http://auto-file.org/member.php?action=profile&uid=1277081
https://pad.geolab.space/s/nBhOnYLof · May 12, 2026 at 12:08 am
References:
William hill promo code https://pad.geolab.space/s/nBhOnYLof
http://app.gxbs.net · May 12, 2026 at 2:16 am
References:
Port perry casino http://app.gxbs.net/home.php?mod=space&uid=1841765
forum.familylawexpress.com.au · May 12, 2026 at 4:46 am
References:
Palms casino las vegas http://forum.familylawexpress.com.au/User-deletedonald15
redação TrustGuru Editorial · May 12, 2026 at 11:20 am
Short daily targets are working better than ambitious goals.
skapa ett binance-konto · May 12, 2026 at 12:24 pm
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
pg slot · May 13, 2026 at 10:23 pm
สล็อต
แพลตฟอร์มสล็อตสมัยใหม่กำลังขยับออกจากเกมหมุนวงล้อทั่วไปไปสู่ระบบคาสิโนออนไลน์ที่เน้นความเสถียรและความเร็ว และใช้การเชื่อมต่อ API โดยตรงร่วมกับระบบหลังบ้านที่ตอบสนองรวดเร็ว ผู้เล่นจำนวนมากเริ่มหันมาใช้เว็บสล็อตตรง เพราะระบบมีความเสถียรมากกว่า และช่วยลดปัญหาเกมโหลดนาน ความผิดพลาดระหว่างการหมุน รวมถึงการเชื่อมต่อการเงินที่ไม่เสถียร
โครงสร้างสล็อต API ตรงจะเชื่อมต่อกับระบบของผู้พัฒนาเกมผ่านระบบเชื่อมต่อแบบเรียลไทม์ ทำให้ธุรกรรมของผู้เล่นถูกส่งแบบเรียลไทม์โดยไม่ต้องผ่านโครงสร้างที่เพิ่มความหน่วง ส่งผลให้เกมโหลดเร็วขึ้น ลดอาการค้างระหว่างเข้าโหมดพิเศษ และช่วยให้การคำนวณรางวัลทำงานได้เสถียรมากขึ้น
ปัจจัยสำคัญอีกด้านคือระบบวอลเล็ตที่ซิงค์แบบเรียลไทม์ ผู้เล่นสามารถจัดการยอดเงินได้ตลอด24 ชั่วโมง โดยไม่จำเป็นต้องรอแอดมินตรวจสอบเหมือนระบบรุ่นเก่า ทำให้การหมุนเวียนเครดิตมีความรวดเร็วกว่าเดิม
เหตุผลหลักที่ผู้เล่นเลือกสล็อตเว็บตรงคือความโปร่งใสและการตอบสนองที่รวดเร็ว เซิร์ฟเวอร์ที่ทำงานร่วมกับ API หลักของค่ายเกมช่วยลดความไม่แน่นอนของระบบตัวกลาง ผู้เล่นจึงเชื่อถือได้ว่าผลลัพธ์ของเกมมาจากอัลกอริทึมต้นทาง
ในขณะเดียวกัน เว็บสมัยใหม่ยังมีการพัฒนาUX/UI สำหรับมือถือโดยเฉพาะ เช่น การเล่นแนวตั้ง การโหลดข้อมูลแบบไดนามิก และระบบ Auto Resumeที่ช่วยกู้รอบเล่นเมื่ออินเทอร์เน็ตหลุด
ระบบสล็อตออนไลน์รุ่นใหม่เริ่มใช้ปัญญาประดิษฐ์ประมวลผลพฤติกรรมผู้เล่น ร่วมกับระบบ Cloud InfrastructureและAPI Syncเพื่อรองรับผู้ใช้งานจำนวนมากพร้อมกัน บางระบบยังรองรับเทคโนโลยีบล็อกเชนเพื่อเพิ่มความยืดหยุ่นด้านการชำระเงินและลดความเสี่ยงจากระบบธนาคารที่ปิดปรับปรุง
อุตสาหกรรมสล็อตออนไลน์จึงกำลังยกระดับจากแพลตฟอร์มที่เน้นแค่เกมและโปรโมชั่นไปสู่แพลตฟอร์มดิจิทัลที่ขับเคลื่อนด้วยข้อมูล โดยโครงสร้าง APIและความต่อเนื่องของระบบกลายเป็นปัจจัยสำคัญในการประเมินคุณภาพผู้ให้บริการ
เมื่อการแข่งขันสูงขึ้นแพลตฟอร์มสล็อตจะยิ่งแข่งขันกันด้านความเร็วของเซิร์ฟเวอร์มากขึ้น ไม่ว่าจะเป็นการตอบสนองของหน้าเกม การประมวลผลพฤติกรรมแบบอัตโนมัติ หรือการเข้ารหัสธุรกรรม ผู้ให้บริการที่มีโครงสร้างเทคนิคที่รองรับโหลดสูงและเชื่อมต่อกับค่ายเกมโดยตรงจะแข่งขันได้แข็งแรงกว่าเว็บทั่วไปที่ยังใช้ระบบตัวกลางหลายชั้น
กลุ่มผู้เล่นที่ให้ความสำคัญกับคุณภาพระบบจึงไม่ได้มองแค่ของแจกอีกต่อไป แต่เริ่มให้ความสำคัญกับคุณภาพของระบบ การซิงค์ยอดเงินแบบเรียลไทม์ และเสถียรภาพของแพลตฟอร์มระหว่างการเล่นจริง
binance kod · May 13, 2026 at 10:42 pm
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
new scramble for Africa · May 14, 2026 at 3:55 pm
African economy
Plataforma de generación de video e imágenes con IA · May 15, 2026 at 5:10 pm
最近一直在试 BestVid 做创意短视频,感觉很流畅—-https://bestvid.net/
สล็อตเว็บตรง · May 15, 2026 at 7:15 pm
ทดลองเล่นสล็อต pg
ระบบสล็อตออนไลน์รุ่นใหม่กำลังเปลี่ยนจากระบบเกมหมุนวงล้อคลาสสิกไปสู่ระบบคาสิโนออนไลน์ที่เน้นความเสถียรและความเร็ว และใช้การเชื่อมต่อ API โดยตรงร่วมกับเซิร์ฟเวอร์ความเร็วสูง ผู้เล่นจำนวนมากเริ่มให้ความสนใจกับแพลตฟอร์มสล็อตเว็บตรง เพราะระบบมีความเสถียรมากกว่า และช่วยลดปัญหาความล่าช้า การค้างของเกม รวมถึงการเชื่อมต่อการเงินที่ไม่เสถียร
โครงสร้างสล็อต API ตรงจะส่งข้อมูลไปยังค่ายเกมหลักผ่านช่องทาง API หลัก ทำให้ข้อมูลการเล่นถูกส่งแบบอัตโนมัติโดยไม่ต้องผ่านหลายเซิร์ฟเวอร์ ส่งผลให้เกมตอบสนองได้ไวขึ้น ลดอาการค้างระหว่างเข้าโหมดพิเศษ และช่วยให้ระบบแจ็คพอตทำงานได้แม่นยำมากขึ้น
ปัจจัยสำคัญอีกด้านคือระบบธุรกรรมอัตโนมัติ ผู้เล่นสามารถจัดการยอดเงินได้ตลอดโดยไม่จำกัดช่วงเวลา โดยไม่จำเป็นต้องพึ่งพาระบบตรวจสอบแบบเก่าเหมือนระบบรุ่นเก่า ทำให้การควบคุมยอดเงินมีความรวดเร็วกว่าเดิม
จุดแข็งของระบบเว็บตรงอยู่ที่ความมั่นใจในผลลัพธ์และความต่อเนื่องของเซิร์ฟเวอร์ เซิร์ฟเวอร์ที่ทำงานร่วมกับ API หลักของค่ายเกมช่วยลดความไม่แน่นอนของระบบตัวกลาง ผู้เล่นจึงเข้าใจได้ว่าผลลัพธ์ของเกมมาจากกลไกสุ่มของค่ายเกม
อีกด้านหนึ่ง เว็บสมัยใหม่ยังมีการพัฒนาระบบแสดงผลบนสมาร์ตโฟนโดยเฉพาะ เช่น หน้าจอที่ออกแบบให้ใช้มือเดียวได้สะดวก การโหลดหน้าแบบ Dynamic และระบบกู้คืนสถานะเกมที่ช่วยกลับเข้าสู่เกมเดิมเมื่ออินเทอร์เน็ตหลุด
เว็บสล็อตที่พัฒนาแล้วเริ่มใช้ระบบวิเคราะห์ข้อมูลอัตโนมัติ ร่วมกับโครงสร้างคลาวด์และการเชื่อมต่อข้อมูลอัตโนมัติเพื่อรองรับการเล่นต่อเนื่องของผู้เล่นหลายกลุ่ม บางระบบยังรองรับBlockchainเพื่อเพิ่มทางเลือกในการทำธุรกรรมและลดปัญหาธุรกรรมล่าช้า
แพลตฟอร์มเกมออนไลน์ประเภทสล็อตจึงกำลังยกระดับจากระบบเกมออนไลน์แบบเก่าไปสู่แพลตฟอร์มดิจิทัลที่ขับเคลื่อนด้วยข้อมูล โดยความเร็วและความต่อเนื่องของระบบกลายเป็นปัจจัยสำคัญในการเลือกแพลตฟอร์ม
ต่อจากนี้แพลตฟอร์มสล็อตจะยิ่งแข่งขันกันด้านเสถียรภาพของแพลตฟอร์มมากขึ้น ไม่ว่าจะเป็นการประมวลผลธุรกรรม ระบบ AI วิเคราะห์พฤติกรรมผู้เล่น หรือการป้องกันข้อมูลส่วนตัว ผู้ให้บริการที่มีโครงสร้างเทคนิคที่รองรับโหลดสูงและเชื่อมต่อกับค่ายเกมโดยตรงจะได้เปรียบมากกว่าเว็บทั่วไปที่ยังใช้เซิร์ฟเวอร์ที่เพิ่มความหน่วง
คนที่เลือกแพลตฟอร์มอย่างจริงจังจึงไม่ได้มองแค่โบนัสอีกต่อไป แต่เริ่มให้ความสำคัญกับคุณภาพของระบบ ความต่อเนื่องของระบบการเงิน และความลื่นของเกมระหว่างใช้งาน
leia mais · May 16, 2026 at 6:50 am
Conta rápida no Jungle Delight: 96% de RTP fica em amostras grandes. Pequenas mentem.
สล็อตเว็บตรง · May 18, 2026 at 2:22 am
สล็อต
สล็อตยุคใหม่กำลังพัฒนาจากสล็อตแบบเดิมไปสู่โครงสร้างเกมออนไลน์ที่ใช้เซิร์ฟเวอร์ความเร็วสูง โดยมีระบบ APIร่วมกับระบบหลังบ้านที่ตอบสนองรวดเร็ว ผู้เล่นจำนวนมากเริ่มเลือกใช้เว็บสล็อตตรง เพราะระบบมีความเสถียรมากกว่า และช่วยลดปัญหาการประมวลผลช้า ปัญหาหน้าจอหยุดระหว่างเล่น รวมถึงปัญหาการฝากถอนที่ไม่ซิงค์กับระบบหลัก
โครงสร้างสล็อต API ตรงจะเชื่อมต่อกับระบบของผู้พัฒนาเกมผ่านโหนด API ที่ไม่ผ่านตัวกลาง ทำให้ข้อมูลการเล่นถูกส่งแบบอัตโนมัติโดยไม่ต้องผ่านหลายเซิร์ฟเวอร์ ส่งผลให้เกมโหลดเร็วขึ้น ลดอาการค้างระหว่างเข้าโหมดพิเศษ และช่วยให้ระบบแจ็คพอตทำงานได้ลดข้อผิดพลาดได้ดีกว่า
อีกจุดสำคัญคือระบบการเงินที่เชื่อมต่อกับแพลตฟอร์มโดยตรง ผู้เล่นสามารถฝากถอนเงินได้ตลอดโดยไม่จำกัดช่วงเวลา โดยไม่จำเป็นต้องพึ่งพาระบบตรวจสอบแบบเก่าเหมือนระบบรุ่นเก่า ทำให้การฝากถอนระหว่างเล่นมีความแม่นยำกว่าเดิม
สาเหตุที่สล็อตเว็บตรงได้รับความนิยมคือความชัดเจนของระบบและการตอบสนองที่รวดเร็ว เซิร์ฟเวอร์ที่ผูกกับระบบเกมต้นทางช่วยลดโอกาสเกิดความคลาดเคลื่อนของข้อมูล ผู้เล่นจึงมั่นใจได้ว่าผลลัพธ์ของเกมมาจากอัลกอริทึมต้นทาง
เมื่อดูในแง่ประสบการณ์ผู้ใช้ เว็บสมัยใหม่ยังมีการพัฒนาประสบการณ์เล่นผ่านมือถือโดยเฉพาะ เช่น อินเทอร์เฟซที่เหมาะกับสมาร์ตโฟน การโหลดหน้าแบบ Dynamic และฟังก์ชันกลับเข้าสู่รอบเดิมที่ช่วยกลับเข้าสู่เกมเดิมเมื่ออินเทอร์เน็ตหลุด
ระบบสล็อตออนไลน์รุ่นใหม่เริ่มใช้AI วิเคราะห์ข้อมูล ร่วมกับระบบประมวลผลบนคลาวด์และระบบซิงค์ข้อมูลแบบเรียลไทม์เพื่อรองรับผู้ใช้งานจำนวนมากพร้อมกัน บางระบบยังรองรับระบบธุรกรรมคริปโตเพื่อเพิ่มทางเลือกในการทำธุรกรรมและลดการพึ่งพาช่องทางการเงินแบบเก่า
อุตสาหกรรมสล็อตออนไลน์จึงกำลังขยับจากแพลตฟอร์มที่เน้นแค่เกมและโปรโมชั่นไปสู่ระบบบริการออนไลน์ที่ต้องแข่งขันด้านประสิทธิภาพ โดยความเสถียรและประสบการณ์ผู้ใช้กลายเป็นปัจจัยสำคัญในการตัดสินใจใช้งานเว็บสล็อต
ในอนาคตแพลตฟอร์มสล็อตจะยิ่งแข่งขันกันด้านเสถียรภาพของแพลตฟอร์มมากขึ้น ไม่ว่าจะเป็นการประมวลผลธุรกรรม ระบบ AI วิเคราะห์พฤติกรรมผู้เล่น หรือการป้องกันข้อมูลส่วนตัว ผู้ให้บริการที่มีโครงสร้างเทคนิคที่รองรับโหลดสูงและเชื่อมต่อกับค่ายเกมโดยตรงจะตอบโจทย์ผู้เล่นได้ดีกว่าเว็บทั่วไปที่ยังใช้การเชื่อมต่อแบบเก่า
ผู้ใช้งานในปัจจุบันจึงไม่ได้มองแค่โบนัสอีกต่อไป แต่เริ่มให้ความสำคัญกับประสิทธิภาพของระบบ ความไวของการฝากถอน และเสถียรภาพของแพลตฟอร์มระหว่างการเล่นจริง
TrustGuru Rankings · May 18, 2026 at 10:25 am
Subi R$2k. Tô fora.
สล็อตเว็บตรง · May 18, 2026 at 3:21 pm
pg slot
แพลตฟอร์มสล็อตสมัยใหม่กำลังขยับออกจากเกมหมุนวงล้อทั่วไปไปสู่ระบบออนไลน์ที่ใช้เทคโนโลยีขั้นสูง ซึ่งให้ความสำคัญกับโครงสร้าง API แบบเรียลไทม์ร่วมกับโครงสร้างเซิร์ฟเวอร์ที่รองรับผู้เล่นจำนวนมาก ผู้เล่นจำนวนมากเริ่มให้ความสนใจกับเว็บสล็อตตรง เพราะระบบมีความเสถียรมากกว่า และช่วยลดปัญหาการประมวลผลช้า การค้างของเกม รวมถึงความล่าช้าในการอัปเดตยอดเงิน
แพลตฟอร์มเว็บตรงจะเชื่อมต่อกับค่ายเกมหลักผ่านช่องทาง API หลัก ทำให้ข้อมูลการเล่นถูกส่งแบบเรียลไทม์โดยไม่ต้องผ่านโครงสร้างที่เพิ่มความหน่วง ส่งผลให้เกมทำงานลื่นขึ้น ลดปัญหาข้อมูลรอบเล่นคลาดเคลื่อน และช่วยให้ระบบโบนัสทำงานได้ต่อเนื่องกว่าเดิม
สิ่งที่ทำให้แพลตฟอร์มยุคใหม่แตกต่างคือระบบการเงินที่เชื่อมต่อกับแพลตฟอร์มโดยตรง ผู้เล่นสามารถทำธุรกรรมได้ตลอดทุกเวลา โดยไม่จำเป็นต้องรอแอดมินตรวจสอบเหมือนแพลตฟอร์มที่ยังใช้การตรวจสอบด้วยคน ทำให้การฝากถอนระหว่างเล่นมีความคล่องตัวกว่าเดิม
เหตุผลหลักที่ผู้เล่นเลือกสล็อตเว็บตรงคือความน่าเชื่อถือและความต่อเนื่องของเซิร์ฟเวอร์ เซิร์ฟเวอร์ที่ส่งข้อมูลไปยังผู้ให้บริการเกมโดยไม่ผ่านตัวกลางช่วยลดปัญหาการแทรกแซงผลลัพธ์ ผู้เล่นจึงเชื่อถือได้ว่าผลลัพธ์ของเกมมาจากระบบสุ่มที่ทำงานจากเซิร์ฟเวอร์หลัก
ในขณะเดียวกัน เว็บสมัยใหม่ยังมีการพัฒนาUX/UI สำหรับมือถือโดยเฉพาะ เช่น โหมดจอมือถือแนวตั้ง การเปิดหน้าเกมโดยไม่หน่วง และระบบบันทึกสถานะอัตโนมัติที่ช่วยรักษาสิทธิ์ในโบนัสเมื่อการเชื่อมต่อมีปัญหา
แพลตฟอร์มสล็อตยุคใหม่เริ่มใช้ระบบวิเคราะห์ข้อมูลอัตโนมัติ ร่วมกับเซิร์ฟเวอร์คลาวด์ที่ขยายตัวได้และAPI Syncเพื่อรองรับผู้ใช้งานจำนวนมากพร้อมกัน บางระบบยังรองรับCrypto Paymentเพื่อเพิ่มความปลอดภัยของข้อมูลและลดปัญหาธุรกรรมล่าช้า
แพลตฟอร์มเกมออนไลน์ประเภทสล็อตจึงกำลังขยับจากแพลตฟอร์มที่เน้นแค่เกมและโปรโมชั่นไปสู่แพลตฟอร์มดิจิทัลที่ขับเคลื่อนด้วยข้อมูล โดยคุณภาพเซิร์ฟเวอร์และความต่อเนื่องของระบบกลายเป็นปัจจัยสำคัญในการประเมินคุณภาพผู้ให้บริการ
เมื่อการแข่งขันสูงขึ้นแพลตฟอร์มสล็อตจะยิ่งแข่งขันกันด้านความเร็วของเซิร์ฟเวอร์มากขึ้น ไม่ว่าจะเป็นการประมวลผลธุรกรรม ระบบแนะนำเกมตามข้อมูลจริง หรือการป้องกันข้อมูลส่วนตัว ผู้ให้บริการที่มีAPI เชื่อมต่อโดยตรงและเชื่อมต่อกับค่ายเกมโดยตรงจะแข่งขันได้แข็งแรงกว่าเว็บทั่วไปที่ยังใช้การเชื่อมต่อแบบเก่า
ผู้ใช้งานในปัจจุบันจึงไม่ได้มองแค่แคมเปญการตลาดอีกต่อไป แต่เริ่มให้ความสำคัญกับมาตรฐานทางเทคนิคของแพลตฟอร์ม ความต่อเนื่องของระบบการเงิน และความน่าเชื่อถือของเซิร์ฟเวอร์ในช่วงใช้งานหนัก
real estate broker · May 20, 2026 at 2:11 am
Proprio Direct real estate broker Boucherville
Mahjong Ways 2 estratégia · May 20, 2026 at 1:32 pm
Lucky Neko de novo. Brutal.
RobertDyefe · May 20, 2026 at 3:21 pm
http://119.28.137.181/camp/home.php?mod=space&uid=26100&do=profile&from=space
RobertFus · May 20, 2026 at 4:20 pm
https://houseedge.us/games/poker/
Scottlem · May 20, 2026 at 4:24 pm
https://winradar.us/games/slots/
TrustGuru análise Fortune Tiger · May 20, 2026 at 9:42 pm
Prosperity Gods Book me deu green inesperado, kkkk não esperava.
git.monogps.com · May 21, 2026 at 8:44 am
References:
Valley view casino center seating chart https://git.monogps.com/brennaforeman0
gangsain.co.kr · May 21, 2026 at 9:31 am
References:
Nouveau brunswick https://gangsain.co.kr/bbs/board.php?bo_table=free&wr_id=326035
app.venusroyale.date · May 21, 2026 at 10:34 am
References:
500 club casino http://app.venusroyale.date/@emanuelphilp41
https://gitea.gentronhealth.com/sasha95g50345 · May 21, 2026 at 10:37 am
References:
Online casino reviews 1 site for best online casinos https://gitea.gentronhealth.com/sasha95g50345
git.slegeir.com · May 21, 2026 at 11:04 am
References:
Revel casino ac https://git.slegeir.com/hiramwetherspo
demo.playtubescript.com · May 21, 2026 at 11:09 am
References:
Europa casino mobile https://demo.playtubescript.com/@benvardon91057?page=about
wopid.io · May 21, 2026 at 11:26 am
References:
Suquamish casino https://wopid.io/@kandicecazneau?page=about
gitea.waterworld.com.hk · May 21, 2026 at 1:00 pm
References:
Native lights casino https://gitea.waterworld.com.hk/denesechartres
https://git.slegeir.com/ · May 21, 2026 at 1:01 pm
References:
Cleopatra slot https://git.slegeir.com/yukikopina0947
https://www.3coup.com/@floyk607510075?page=about · May 21, 2026 at 1:25 pm
References:
Gala casinos https://www.3coup.com/@floyk607510075?page=about
jobszimbabwe.co.zw · May 21, 2026 at 1:32 pm
References:
99 slots https://jobszimbabwe.co.zw/companies/secure-access-royal-rewards/
https://gitea.kamisama.ovh/ · May 21, 2026 at 1:36 pm
References:
Casino script https://gitea.kamisama.ovh/elmerpitcairn
searchmerajob.in · May 21, 2026 at 3:11 pm
References:
No deposit poker bonus https://searchmerajob.in/employer/best-online-pokies-in-australia-for-real-money-in-2026
analyticsjobs.in · May 22, 2026 at 2:33 am
References:
Monte cassino italy https://analyticsjobs.in/jobs/companies/top-microgaming-slots-games-and-casinos/
https://careersearchinfo.com/employer/best-microgaming-casinos-with-generous-bonuses-2026/ · May 22, 2026 at 4:51 am
References:
Casino technology https://careersearchinfo.com/employer/best-microgaming-casinos-with-generous-bonuses-2026/
tg777 · May 22, 2026 at 7:10 am
I read this post completely concerning the comparison of newest and preceding technologies, it’s awesome article.
世界盃 · May 22, 2026 at 12:20 pm
世界盃
2026 年 FIFA 世界盃 將由 48 個國家代表隊 參賽,本屆賽事將分成 12 組分組,每個小組由 4 支球隊組成。小組前二名球隊 能夠進入 淘汰賽階段,迎來 16 強、8 強、4 強、季軍戰與決賽。
2026 世界盃 預計在 2026 年 6 月 展開賽程。開幕賽事 預計由 墨西哥與南非交手,於 6 月 12 日 於阿茲特克球場開打。同日稍晚,南韓對決捷克。隔日,還有加拿大 VS 波士尼亞、美國 VS 巴拉圭等首輪比賽。
在小組分組上,A 組 包括 墨西哥、南非、南韓與捷克;B 組 包含 加拿大、波士尼亞、卡達以及瑞士;C 組 包含 巴西、摩洛哥、海地與蘇格蘭同組。像是 巴西、法國、阿根廷、英格蘭、西班牙與德國等熱門球隊 已確認所屬小組。
晉級淘汰賽階段 預計於 7 月初 展開,16 強賽 預計從 7 月 4 日 登場,而冠軍戰預定於 7 月 19 日 進行,最終將產生本屆世界盃冠軍。
歷史交手紀錄顯示,墨西哥和南非曾在 2010 年世界盃 對決,最終以 1:1 平局收場,至今未分勝負。
此外,越位、黃牌、紅牌、VAR 與點球等規則,依然是觀看比賽時的重要觀念,相關規則也持續受到關注。
世界盃杯世足賽 · May 24, 2026 at 1:45 pm
世界盃杯世足賽
2026 年 FIFA 世界盃 將由 48 支國家隊 角逐冠軍,本屆賽事將分成 12 個小組,每個小組由 4 支球隊組成。各組前兩名 能夠進入 淘汰賽,進行 16 強至決賽的淘汰賽程。
2026 世界盃 將於 2026 年 6 月 正式開賽。開幕賽事 將由 墨西哥迎戰南非,於 6 月 12 日 於阿茲特克球場開打。同一天稍後,南韓對決捷克。翌日,加拿大將迎戰波士尼亞,而美國則對上巴拉圭。
小組賽方面,A 組 由 墨西哥、南非、韓國及捷克;B 組 則由 加拿大、波士尼亞、卡達以及瑞士;C 組 則是 巴西、摩洛哥、海地及蘇格蘭構成。包括 法國、阿根廷、巴西、德國、西班牙與英格蘭等勁旅 都已確定分組結果。
淘汰賽 預計於 7 月初 展開,16 強賽 大約在 7 月 4 日 登場,最終決賽將在 7 月 19 日 舉辦,並誕生 2026 世界盃冠軍隊伍。
從過往戰績來看,墨西哥與南非曾於 2010 年世界盃 對決,結果雙方踢成 1 比 1,至今未分勝負。
同時,足球比賽規則如越位、黃牌、紅牌、VAR 與點球判罰,仍是球迷觀賽時的重要基礎知識,相關規則也持續受到關注。
estratégia de Bonus Buy · May 25, 2026 at 7:26 pm
A galera mais antiga resumão do fim de semana é a única coisa que leio na segunda.
referência · May 26, 2026 at 3:28 am
Fortune Mouse me carregou hoje.
FIFA世界杯 · May 26, 2026 at 8:47 pm
世界盃杯世足賽
2026 FIFA 世界盃 將會由 48 支球隊 參賽,整體賽程包含 12 組分組,每組 4 隊。每組排名前兩位的隊伍 可晉級 淘汰賽階段,迎來 後續淘汰賽與冠軍爭奪戰。
本屆世界盃 預計在 2026 年 6 月 正式開踢。開幕賽事 將由 墨西哥與南非交手,於 6 月 12 日 於阿茲特克球場開打。同日後續賽程中,南韓對決捷克。接下來一天,還有加拿大 VS 波士尼亞、美國 VS 巴拉圭等首輪比賽。
分組名單顯示,A 組 包含 墨西哥、南非、韓國及捷克;B 組 則由 加拿大、波士尼亞、卡達以及瑞士;C 組 則是 巴西、摩洛哥、海地及蘇格蘭構成。例如 法國、阿根廷、巴西、德國、西班牙與英格蘭等勁旅 皆已完成分組。
後續淘汰輪次 將於 7 月初 開始,16 強賽 預計從 7 月 4 日 開踢,而冠軍戰預定於 7 月 19 日 舉辦,屆時將決定 2026 年 FIFA 世界盃冠軍。
歷史交手紀錄顯示,墨西哥與南非曾於 2010 年世界盃 對決,結果雙方踢成 1 比 1,雙方仍無勝場差距。
同時,足球比賽規則如越位、黃牌、紅牌、VAR 與點球判罰,依然是觀看比賽時的重要觀念,相關討論熱度不減。
admiral slots online free · May 27, 2026 at 9:17 pm
admiral slots online free
online casino best deals · May 27, 2026 at 10:00 pm
play sky rider slot online
online casino best deals · May 27, 2026 at 10:07 pm
pogo free games casino
black jack casino · May 27, 2026 at 10:15 pm
cafe casino no deposit bonus codes
jeetwin online casino · May 28, 2026 at 2:41 am
jeetwin online casino
play casino free game · May 29, 2026 at 12:33 pm
best 1st deposit casino bonus
jogar gates of olympus 1000 demo · May 31, 2026 at 7:15 am
Para quem tem dúvida, Blackjack é o canal. Muito bom. Saque na hora.
https://prpack.ru/user/brainberet8/ · June 1, 2026 at 6:02 pm
References:
Gala casino nottingham https://prpack.ru/user/brainberet8/
www.instapaper.com · June 1, 2026 at 9:39 pm
References:
Hoosier park racing and casino https://https://www.instapaper.com/p/17718200/p/17718200
https://isowindows.net/ · June 1, 2026 at 10:50 pm
References:
Gulfport casino https://isowindows.net/user/puppyvase2/
References:
https://isowindows.net/user/puppyvase2/
https://forum.board-of-metal.org/user-47280.html · June 2, 2026 at 3:11 am
References:
Vicksburg casinos https://forum.board-of-metal.org/user-47280.html
earthwiki.space · June 2, 2026 at 4:06 am
References:
Lady luck casino las vegas https://https://earthwiki.space/wiki/Der_HitnSpin_Willkommensbonus_alle_Infos/wiki/Der_HitnSpin_Willkommensbonus_alle_Infos
http://downarchive.org/user/carday08/ · June 2, 2026 at 5:45 am
References:
Videoslots nl http://downarchive.org/user/carday08/
http://okprint.kz/user/traysandra03/ · June 2, 2026 at 5:49 am
References:
La casinos http://okprint.kz/user/traysandra03/
https://travelersqa.com · June 2, 2026 at 6:03 am
References:
Aristocrat slots https://travelersqa.com/user/tuneseason57
http://madk-auto.ru/user/cereallawyer9/ · June 2, 2026 at 7:57 am
References:
Crockfords casino http://madk-auto.ru/user/cereallawyer9/
https://pad.stuve.uni-ulm.de/s/TLVAehxiJ · June 2, 2026 at 10:20 am
References:
Gold country casino https://pad.stuve.uni-ulm.de/s/TLVAehxiJ
https://choate-kjeldsen.hubstack.net/hit-prospekt-ab-26-05-2026-diese-woche-and-nachste-woche-online-blattern · June 2, 2026 at 10:57 am
References:
Roulette systems https://choate-kjeldsen.hubstack.net/hit-prospekt-ab-26-05-2026-diese-woche-and-nachste-woche-online-blattern
topsitenet.com · June 2, 2026 at 11:26 am
References:
Roulette wheel layout https://topsitenet.com/profile/hellwood52/1836763/
g.clicgo.ru · June 4, 2026 at 8:17 pm
References:
Hamilton casino https://g.clicgo.ru/user/judopink59/
https://hedgedoc.eclair.ec-lyon.fr/s/lFzqvoGdd- · June 4, 2026 at 8:57 pm
References:
Red rock casino las vegas https://hedgedoc.eclair.ec-lyon.fr/s/lFzqvoGdd-
http://adrestyt.ru/user/soapoboe4/ · June 5, 2026 at 12:42 am
References:
Blackjack and hookers http://adrestyt.ru/user/soapoboe4/
https://doc.adminforge.de/s/Fk6AAYlkBd · June 5, 2026 at 3:01 am
References:
Fitz casino https://doc.adminforge.de/s/Fk6AAYlkBd
https://literaryforge.blog/ · June 5, 2026 at 4:16 am
References:
Ballys casino ac https://literaryforge.blog/author/closetprice7/
https://pad.stuve.de · June 5, 2026 at 5:46 am
References:
Instant Casino Spiele
References:
https://pad.stuve.de/s/qtoIfWIps
BATA4D · June 5, 2026 at 9:08 pm
BATA4D
https://concretewiki.site/ · June 5, 2026 at 11:53 pm
References:
The grand casino https://concretewiki.site/wiki/Kings_Resort_casino_and_hotels_in_Rozvadov_in_Tschechien_ab_61_Angebote_Bewertungen_Fotos
https://dudoser.com/user/summerborder3/ · June 6, 2026 at 3:03 am
References:
New orleans casinos https://dudoser.com/user/summerborder3/
https://nutritionwiki.space/wiki/Lex_Casino_App_Echte_Gewinne_in_deiner_Tasche_jetzt_sofort · June 6, 2026 at 8:03 am
References:
Roulette bonus https://nutritionwiki.space/wiki/Lex_Casino_App_Echte_Gewinne_in_deiner_Tasche_jetzt_sofort
https://telegra.ph/ · June 6, 2026 at 9:02 am
References:
Comeon casino review https://telegra.ph/Online-Casino-Spiele-JETZT-SPIELEN-06-05-2
http://karayaz.ru/user/grassleaf9/ · June 6, 2026 at 10:50 am
References:
Genting casino malaysia http://karayaz.ru/user/grassleaf9/
https://neolatinswiki.site · June 6, 2026 at 12:06 pm
References:
Best games for mac https://neolatinswiki.site/wiki/Fordern_Sie_bis_zu_1_000_Bonus_und_Freispiele
https://school-of-safety-russia.ru/user/grassscale98/ · June 6, 2026 at 12:23 pm
References:
Oaks casino towers brisbane https://school-of-safety-russia.ru/user/grassscale98/
rentry.co · June 6, 2026 at 1:42 pm
References:
Riva casino https://https://rentry.co/w9ck7amx/w9ck7amx
http://forums.cgb.designknights.com · June 6, 2026 at 2:15 pm
References:
Online casino new jersey http://forums.cgb.designknights.com/member.php?action=profile&uid=191412
whatsnewintheprophetic.com · June 6, 2026 at 2:19 pm
References:
Tulsa casinos https://www.https://www.whatsnewintheprophetic.com/author/zebrastage8//author/zebrastage8/
https://hackmd.okfn.de/s/ryh3WO7eGx · June 6, 2026 at 2:39 pm
References:
River nile casino https://hackmd.okfn.de/s/ryh3WO7eGx
materialwiki.site · June 6, 2026 at 3:26 pm
References:
George thorogood bad to the bone https://https://materialwiki.site/wiki/Kings_startet_nchstes_Poker_Highlight_in_Rozvadov/wiki/Kings_startet_nchstes_Poker_Highlight_in_Rozvadov
https://buyandsellhair.com · June 6, 2026 at 5:01 pm
References:
No deposit bonus https://buyandsellhair.com/author/porterwheel4//author/porterwheel4/
gaiaathome.eu · June 6, 2026 at 5:31 pm
References:
Mobile casino online https://https://gaiaathome.eu/gaiaathome/show_user.php?userid=1977731/gaiaathome/show_user.php?userid=1977731
https://neoclassical.space/wiki/HitnSpin_Alternative_Die_5_besten_Alternativen_hier_Mai_2026_hnliche_Casinos_hier · June 6, 2026 at 5:45 pm
References:
Roulette play https://neoclassical.space/wiki/HitnSpin_Alternative_Die_5_besten_Alternativen_hier_Mai_2026_hnliche_Casinos_hier
https://bbs.pku.edu.cn · June 6, 2026 at 6:00 pm
References:
Sydney casino https://bbs.pku.edu.cn/v2/jump-to.php?url=https://de.trustpilot.com/review/sleepnap.de
https://pad.stuve.de/ · June 6, 2026 at 6:02 pm
References:
Station casinos boarding pass https://pad.stuve.de/s/b6WiMMp3OT
http://madk-auto.ru/ · June 6, 2026 at 6:29 pm
References:
Slot bonus http://madk-auto.ru/user/tankercocoa31/
References:
http://madk-auto.ru/user/tankercocoa31/
https://vargas-michaelsen.mdwrite.net · June 6, 2026 at 7:11 pm
References:
Play video poker online https://vargas-michaelsen.mdwrite.net/150-400-fs-and-10-cashback-2026/150-400-fs-and-10-cashback-2026
https://g.clicgo.ru/user/appealregret72/ · June 6, 2026 at 8:26 pm
References:
New casino sites https://g.clicgo.ru/user/appealregret72/
https://morsing-nyborg-3.federatedjournals.com · June 6, 2026 at 8:45 pm
References:
Slots of fortune https://morsing-nyborg-3.federatedjournals.com/willkommensbonus-bonuscodes-freispiele-and-cashback/willkommensbonus-bonuscodes-freispiele-and-cashback
https://boardgameswiki.site · June 6, 2026 at 9:05 pm
References:
Casino promotions https://boardgameswiki.site/wiki/Boomerang_Casino_Auszahlungserfahrungen_2026_Tempo_Limits/wiki/Boomerang_Casino_Auszahlungserfahrungen_2026_Tempo_Limits
my.vipaist.ru · June 6, 2026 at 10:20 pm
References:
Winning at slots https://https://my.vipaist.ru/user/scentquart8//user/scentquart8/
https://freudwiki.site/ · June 6, 2026 at 10:29 pm
References:
Electronic roulette https://freudwiki.site/wiki/Casino_of_Gold_Detaillierte_Bewertung_und_Erfahrungen_2026
References:
https://freudwiki.site/wiki/Casino_of_Gold_Detaillierte_Bewertung_und_Erfahrungen_2026
telegra.ph · June 6, 2026 at 10:33 pm
References:
Casino orlando fl https://https://telegra.ph/Kings-Resort-Wikipedia-05-26/Kings-Resort-Wikipedia-05-26
hackmd.okfn.de · June 6, 2026 at 10:41 pm
References:
Trump casino https://https://hackmd.okfn.de/s/H1luj8_mlMe/s/H1luj8_mlMe
https://ancientroman.space/ · June 6, 2026 at 10:45 pm
References:
Blackjack club https://ancientroman.space/wiki/Offizielles_Casino_in_sterreich
https://hackmd.okfn.de · June 7, 2026 at 12:04 am
References:
Live casinos https://hackmd.okfn.de/s/rJ50n8Xefl/s/rJ50n8Xefl
literaryforge.blog · June 7, 2026 at 3:38 am
References:
Lady luck casino vicksburg https://https://literaryforge.blog/author/airactor2//author/airactor2/
freudwiki.site · June 7, 2026 at 4:10 am
References:
Hardrock casino albuquerque https://https://freudwiki.site/wiki/Bwin_Erfahrungen_Test_2026_Betrug_oder_seris/wiki/Bwin_Erfahrungen_Test_2026_Betrug_oder_seris
xypid.win · June 7, 2026 at 5:16 am
References:
Hollywood casino toledo oh https://https://xypid.win/story.php?title=top-casino-spiele-boni-in-deutschland/story.php?title=top-casino-spiele-boni-in-deutschland
https://bridgedesign.space/wiki/Monro_Casino_Erfahrungen_2026_Modern_Seris · June 7, 2026 at 5:23 am
References:
Lotus casino las vegas https://bridgedesign.space/wiki/Monro_Casino_Erfahrungen_2026_Modern_Seris
https://topsitenet.com/profile/fatdouble08/1872737/ · June 7, 2026 at 7:29 am
References:
Slot canyons utah https://topsitenet.com/profile/fatdouble08/1872737/
doc.adminforge.de · June 7, 2026 at 8:25 am
References:
Gala casino nottingham https://https://doc.adminforge.de/s/1iixVQyQRZ/s/1iixVQyQRZ
karayaz.ru · June 7, 2026 at 8:27 am
References:
Black jack boots http://http://karayaz.ru/user/turnox91//user/turnox91/
sonnik.nalench.com · June 7, 2026 at 9:11 am
References:
San diego casinos https://https://sonnik.nalench.com/user/resultstick5//user/resultstick5/
https://www.24propertyinspain.com/user/profile/1456514 · June 7, 2026 at 9:15 am
References:
Games slot machines https://www.24propertyinspain.com/user/profile/1456514
https://xypid.win/story.php?title=bonus-freispiele-auszahlung-login-2026 · June 7, 2026 at 9:54 am
References:
Best slot machines https://xypid.win/story.php?title=bonus-freispiele-auszahlung-login-2026
https://gardenwiki.site · June 7, 2026 at 10:33 am
References:
France roulette https://gardenwiki.site/wiki/Offizielles_Casino_Deutschland_2026/wiki/Offizielles_Casino_Deutschland_2026
chesswiki.site · June 7, 2026 at 10:50 am
References:
Lucky casino https://https://chesswiki.site/wiki/Bonus_ohne_Einzahlung_Deutschland_Deutsche_No_Deposit_Bonus/wiki/Bonus_ohne_Einzahlung_Deutschland_Deutsche_No_Deposit_Bonus
https://materialwiki.site/wiki/Ist_das_Ice_Casino_Seris_oder_Betrug_Expertentest_2026 · June 7, 2026 at 11:17 am
References:
Pendleton casino https://materialwiki.site/wiki/Ist_das_Ice_Casino_Seris_oder_Betrug_Expertentest_2026
bookmark4you.win · June 7, 2026 at 12:07 pm
References:
Old second neteller https://https://bookmark4you.win/story.php?title=betano-auszahlung-erfahrungen-2026-auszahlungsdauer/story.php?title=betano-auszahlung-erfahrungen-2026-auszahlungsdauer
https://neolatinswiki.site/wiki/888Casino_Betrug_oder_seris_Zum_Test_5_2026 · June 7, 2026 at 3:46 pm
References:
Charleston wv casino https://neolatinswiki.site/wiki/888Casino_Betrug_oder_seris_Zum_Test_5_2026
https://chesswiki.site/wiki/Drip_Casino_Erfahrungen_2026_RTPCheck_Spiele_Bonus · June 7, 2026 at 4:58 pm
References:
Starlight casino https://chesswiki.site/wiki/Drip_Casino_Erfahrungen_2026_RTPCheck_Spiele_Bonus
philosophywiki.space · June 7, 2026 at 5:31 pm
References:
Online poker game https://https://philosophywiki.space/wiki/1Go_Casino_Bonus_ohne_Einzahlung_Spielen_und_kostenlos_gewinnen/wiki/1Go_Casino_Bonus_ohne_Einzahlung_Spielen_und_kostenlos_gewinnen
https://bridgedesign.space/ · June 7, 2026 at 6:49 pm
References:
Jupiter casino gold coast https://bridgedesign.space/wiki/Aktionen_Bonus_und_Live_games_Spiele
References:
https://bridgedesign.space/wiki/Aktionen_Bonus_und_Live_games_Spiele
https://architecturewiki.site/wiki/Einfache_Ein_und_Auszahlungen · June 7, 2026 at 7:32 pm
References:
Cda casino https://architecturewiki.site/wiki/Einfache_Ein_und_Auszahlungen
https://actualites.cava.tn · June 7, 2026 at 7:40 pm
References:
Casino slot machine games https://actualites.cava.tn/user/attackmemory38//user/attackmemory38/
https://notes.medien.rwth-aachen.de/ · June 7, 2026 at 9:37 pm
References:
Seven feathers casino https://notes.medien.rwth-aachen.de/AX4-jjKrS4OAynYVaX6ykg/
References:
https://notes.medien.rwth-aachen.de/AX4-jjKrS4OAynYVaX6ykg/
https://bridgedesign.site/wiki/Bizzo_Bonuscodes_Exklusive_Bonusse_fr_Mai_2026 · June 7, 2026 at 9:50 pm
References:
Sky vegas mobile https://bridgedesign.site/wiki/Bizzo_Bonuscodes_Exklusive_Bonusse_fr_Mai_2026
roadwiki.site · June 7, 2026 at 9:51 pm
References:
Poliglot https://https://roadwiki.site/wiki/50_Freispiele_ohne_Einzahlung_bis_zu_800_Willkommensbonus/wiki/50_Freispiele_ohne_Einzahlung_bis_zu_800_Willkommensbonus
literaturewiki.site · June 7, 2026 at 9:54 pm
References:
Blackjack payout https://https://literaturewiki.site/wiki/Monro_Casino_Test_2026_150_Bonus_400_FS_Echter_Auszahlungstest_App/wiki/Monro_Casino_Test_2026_150_Bonus_400_FS_Echter_Auszahlungstest_App
http://kriminal-ohlyad.com.ua/user/dadswan66/ · June 7, 2026 at 10:29 pm
References:
Online casino vegas http://kriminal-ohlyad.com.ua/user/dadswan66/
Casino Online México · June 7, 2026 at 10:46 pm
Pagou bem demais.
nectar ai · June 7, 2026 at 10:50 pm
ai girlfriend voice call
https://glerup-hertz.mdwrite.net/ · June 8, 2026 at 12:00 am
References:
Sunset casino https://glerup-hertz.mdwrite.net/erfahrungen-and-bewertung-2026-1779827830
References:
https://glerup-hertz.mdwrite.net/erfahrungen-and-bewertung-2026-1779827830
mensvault.men · June 8, 2026 at 12:26 am
References:
Play online casino games https://https://mensvault.men/story.php?title=1go-casino-im-test-lohnt-sich-der-einstieg-2026-wirklich/story.php?title=1go-casino-im-test-lohnt-sich-der-einstieg-2026-wirklich
https://bridgedesign.space/wiki/Spielen_Sie_Slots_Live_Casino_Gewinnen_Sie_gro_online · June 8, 2026 at 12:53 am
References:
Quantum quest a cassini space odyssey https://bridgedesign.space/wiki/Spielen_Sie_Slots_Live_Casino_Gewinnen_Sie_gro_online
g.clicgo.ru · June 8, 2026 at 1:15 am
References:
Quicksilver slots https://https://g.clicgo.ru/user/giantday61//user/giantday61/
https://literaturewiki.site · June 8, 2026 at 1:19 am
References:
Mt airy casino https://literaturewiki.site/wiki/Offizielles_Casino_in_sterreich/wiki/Offizielles_Casino_in_sterreich
https://neolatinswiki.site/ · June 8, 2026 at 1:30 am
References:
Casino nyc https://neolatinswiki.site/wiki/Monro_Casino_Online_Casino_Spiele_Online_Casino_mit_echtem_Geld
References:
https://neolatinswiki.site/wiki/Monro_Casino_Online_Casino_Spiele_Online_Casino_mit_echtem_Geld
https://gpsites.win/story.php?title=n1-casino-gruppe-mai-2026 · June 8, 2026 at 1:40 am
References:
Ok casinos https://gpsites.win/story.php?title=n1-casino-gruppe-mai-2026
https://www.24propertyinspain.com/user/profile/1456442 · June 8, 2026 at 2:01 am
References:
Spirit mountain casino oregon https://www.24propertyinspain.com/user/profile/1456442
https://skyscrapperwiki.site/wiki/ZetCasino_Test_Alle_Erfahrungen_mit_Boni_Spielangebot_Co · June 8, 2026 at 2:21 am
References:
Casino on net https://skyscrapperwiki.site/wiki/ZetCasino_Test_Alle_Erfahrungen_mit_Boni_Spielangebot_Co
lukovich.ru · June 8, 2026 at 3:01 am
References:
Holland casino amsterdam http://http://lukovich.ru/user/woodpansy36//user/woodpansy36/
https://hedgedoc.eclair.ec-lyon.fr/s/iTJnxUYI2 · June 8, 2026 at 3:36 am
References:
Casino pechanga https://hedgedoc.eclair.ec-lyon.fr/s/iTJnxUYI2
http://tropicana.maxlv.ru/user/pintcomb3/ · June 8, 2026 at 3:47 am
References:
Isleta casino http://tropicana.maxlv.ru/user/pintcomb3/
https://gratisafhalen.be/author/sushimonday36/ · June 8, 2026 at 5:00 am
References:
No deposit poker bonus https://gratisafhalen.be/author/sushimonday36/
https://intensedebate.com/ · June 8, 2026 at 5:09 am
References:
Oneida casino green bay https://intensedebate.com/people/barberstone6
References:
https://intensedebate.com/people/barberstone6
https://neoclassical.space/wiki/NV_Casino_Test_80_Freispiele_ohne_Einzahlung · June 8, 2026 at 5:32 am
References:
Casino arizona talking stick https://neoclassical.space/wiki/NV_Casino_Test_80_Freispiele_ohne_Einzahlung
https://500px.com/p/hwangkbrburks · June 8, 2026 at 5:36 am
References:
Electronic roulette https://500px.com/p/hwangkbrburks
https://instapages.stream/story.php?title=lex-casino-kostenlos-online-spielen-freispiele-willkommensbonus-offizieller-mirror-und-support-erhalten · June 8, 2026 at 5:40 am
References:
Jackson rancheria casino https://instapages.stream/story.php?title=lex-casino-kostenlos-online-spielen-freispiele-willkommensbonus-offizieller-mirror-und-support-erhalten
https://notes.medien.rwth-aachen.de/ci8mJ-ZpT5CUM07g9MQo7w/ · June 8, 2026 at 5:58 am
References:
Majestic star casino https://notes.medien.rwth-aachen.de/ci8mJ-ZpT5CUM07g9MQo7w/
http://uchkombinat.com.ua/ · June 8, 2026 at 6:25 am
References:
Mobile slots http://uchkombinat.com.ua/user/toastsing20/
References:
http://uchkombinat.com.ua/user/toastsing20/
https://may22.ru/user/jasonskiing3/ · June 8, 2026 at 6:51 am
References:
Hollywood slots https://may22.ru/user/jasonskiing3/
https://materialwiki.site · June 8, 2026 at 7:43 am
References:
Gran casino barcelona https://materialwiki.site/wiki/Planmige_Turniere_feste_Auszahlungen/wiki/Planmige_Turniere_feste_Auszahlungen
https://hedgedoc.info.uqam.ca/ · June 8, 2026 at 7:45 am
References:
Midas auto service https://hedgedoc.info.uqam.ca/s/7VkDrUylo
References:
https://hedgedoc.info.uqam.ca/s/7VkDrUylo
truckwiki.site · June 8, 2026 at 8:01 am
References:
Casino security https://https://truckwiki.site/wiki/HitnSpin_Casino_800_EUR200_FS_WILLKOMMENSBONUS/wiki/HitnSpin_Casino_800_EUR200_FS_WILLKOMMENSBONUS
https://callesen-wollesen-3.hubstack.net/ · June 8, 2026 at 8:30 am
References:
Roulette payout chart https://callesen-wollesen-3.hubstack.net/beste-lastschrift-casinos-2026-sicher-per-sepa-im-casino-zahlen
References:
https://callesen-wollesen-3.hubstack.net/beste-lastschrift-casinos-2026-sicher-per-sepa-im-casino-zahlen
https://g.clicgo.ru/user/bugleparty7/ · June 8, 2026 at 9:00 am
References:
Four winds casino michigan https://g.clicgo.ru/user/bugleparty7/
http://ezproxy.cityu.edu.hk/login?url=https://de.trustpilot.com/review/der-wikinger-shop.de · June 8, 2026 at 10:00 am
References:
Hard rock casino tampa http://ezproxy.cityu.edu.hk/login?url=https://de.trustpilot.com/review/der-wikinger-shop.de
telegra.ph · June 8, 2026 at 10:21 am
References:
New orleans casinos https://https://telegra.ph/Lex-Casino-Test–Erfahrungen-2026-100-Bonus–200-Freispiele-05-26/Lex-Casino-Test–Erfahrungen-2026-100-Bonus–200-Freispiele-05-26
http://tropicana.maxlv.ru/user/closebaboon6/ · June 8, 2026 at 10:32 am
References:
Poker bonus no deposit http://tropicana.maxlv.ru/user/closebaboon6/
https://aryba.kg/user/paintball4/ · June 8, 2026 at 12:04 pm
References:
Manoir https://aryba.kg/user/paintball4/
http://ezproxy.cityu.edu.hk · June 8, 2026 at 12:10 pm
References:
Cherokee casino siloam springs http://ezproxy.cityu.edu.hk/login?url=https://de.trustpilot.com/review/randmvapes24.de/login?url=https://de.trustpilot.com/review/randmvapes24.de
https://www.udrpsearch.com/user/goatwasher2 · June 8, 2026 at 10:29 pm
References:
Regle du blackjack https://www.udrpsearch.com/user/goatwasher2
pena-hutchinson.mdwrite.net · June 8, 2026 at 10:34 pm
References:
Blackjack band https://https://pena-hutchinson.mdwrite.net/kings-resort-poker-hotely-restaurace-sluzby-a-kontakty/kings-resort-poker-hotely-restaurace-sluzby-a-kontakty
http://csmouse.com/ · June 8, 2026 at 10:35 pm
References:
Eureka casino mesquite http://csmouse.com/user/clerkparent03/
References:
http://csmouse.com/user/clerkparent03/
truckwiki.site · June 8, 2026 at 10:40 pm
References:
Play slots online https://https://truckwiki.site/wiki/Kings_Casino_Rozvadov_Spielbank_Infos_2026/wiki/Kings_Casino_Rozvadov_Spielbank_Infos_2026
https://bridgedesign.space · June 8, 2026 at 11:34 pm
References:
Elgin casino https://bridgedesign.space/wiki/543_Slots_mit_GGLLizenz/wiki/543_Slots_mit_GGLLizenz
skyscrapperwiki.site · June 9, 2026 at 12:36 am
References:
New york casino las vegas https://https://skyscrapperwiki.site/wiki/Neukundenbonus_Freispiele/wiki/Neukundenbonus_Freispiele
uchkombinat.com.ua · June 9, 2026 at 12:38 am
References:
Online casino canada http://http://uchkombinat.com.ua/user/repairtrain1//user/repairtrain1/
https://pads.zapf.in/s/KlZ0SDw1-q · June 9, 2026 at 1:09 am
References:
Virtual casino https://pads.zapf.in/s/KlZ0SDw1-q
http://amur.1gb.ua/ · June 9, 2026 at 1:35 am
References:
Casino san diego http://amur.1gb.ua/user/lampring5/
References:
http://amur.1gb.ua/user/lampring5/
CH加密中心学院 · June 9, 2026 at 5:15 am
明确其定位:导航站,而非学院。Cryptify Hub没有课程体系、没有认证证书、没有导师团队,只有一张不断更新的工具链接列表。它能帮你省下搜索时间,但不能帮你省下独立思考的过程。请理性使用。
udrpsearch.com · June 9, 2026 at 7:24 am
References:
Sarnia casino https://www.https://www.udrpsearch.com/user/gamewitch26/user/gamewitch26
https://my.vipaist.ru/user/weaselpolish91/ · June 9, 2026 at 9:33 am
References:
Olympic casino poker https://my.vipaist.ru/user/weaselpolish91/
https://blankenship-tennant-3.blogbright.net/online-casino-mit-exklusiven-boni-and-5000-spielen · June 9, 2026 at 11:09 am
References:
Bally’s casino tunica https://blankenship-tennant-3.blogbright.net/online-casino-mit-exklusiven-boni-and-5000-spielen
materialwiki.site · June 9, 2026 at 12:10 pm
References:
Make money online australia https://https://materialwiki.site/wiki/Vulkan_Vegas_Bonus_7_Codes_Gutschein_ohne_Einzahlung/wiki/Vulkan_Vegas_Bonus_7_Codes_Gutschein_ohne_Einzahlung
http://karayaz.ru/user/wrenrat77/ · June 9, 2026 at 2:20 pm
References:
888 casino download http://karayaz.ru/user/wrenrat77/
кольорові картриджі для принтерів · June 12, 2026 at 12:40 pm
кольорові картриджі для принтерів
Binance账户创建 · June 13, 2026 at 7:26 am
Your point of view caught my eye and was very interesting. Thanks. I have a question for you. https://www.binance.com/register?ref=GGYHGRE
вилочный погрузчик 5 тонн · June 13, 2026 at 7:12 pm
вилочный погрузчик 10 тонн
世足免費 · June 14, 2026 at 4:07 am
世足直播線上看
想找世足免費觀看資訊,最重要的是能快速掌握比賽時間、對戰組合與直播管道。世界盃是全球球迷最期待的足球盛事,每一屆都會吸引大量觀眾關注,從小組賽到淘汰賽,每場比賽都有可能出現爆冷、逆轉或關鍵進球,因此不少人都會提前搜尋世足免費相關內容,希望在開賽前就安排好觀賽時間。
對台灣球迷來說,世界盃賽事時間常常受到時差影響,有些比賽可能在深夜或清晨開踢,如果沒有事先查好賽程,很容易錯過精彩對決。透過 RG直播,可以更方便掌握每日熱門賽事、比賽資訊與線上觀看重點,不論是想看傳統強隊、亞洲球隊,還是關注冠軍熱門,都能快速找到需要的內容。
搜尋世足免費時,建議除了確認是否能觀看比賽,也要注意直播穩定度與資訊完整性。熱門賽事通常會有大量球迷同時上線,如果平台載入速度慢或畫面不穩,會大幅影響觀賽體驗。RG直播整理世界盃相關資訊,讓使用者可以更輕鬆追蹤賽事,不用在不同網站之間來回搜尋。
世界盃不只是足球比賽,更是一場全球性的運動狂歡。每一場比賽背後都有球員、國家隊與球迷的期待。想要完整享受世足熱潮,可以透過 RG直播掌握世足免費看球資訊,快速了解賽程、直播與熱門對戰,不錯過任何值得關注的精彩瞬間。
长城电竞 · June 15, 2026 at 11:50 am
I’m not positive where you’re getting your info, but good topic.
I must spend some time finding out much more or working out more.
Thanks for excellent info I used to be in search of this info for my mission.
binance · June 16, 2026 at 12:39 am
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
pro88 · June 16, 2026 at 12:03 pm
pro88
สล็อตเว็บตรง · June 17, 2026 at 11:35 am
pg slot
ปฏิวัติวงการสล็อตออนไลน์ปี 2026: วิวัฒนาการของ API ในอุตสาหกรรม iGaming
อุตสาหกรรมสล็อตออนไลน์ยังคงเติบโตอย่างต่อเนื่องในปี 2026 ผ่านการนำเทคโนโลยีสมัยใหม่มาปรับปรุงแพลตฟอร์มอย่างต่อเนื่อง
ผู้เล่นสามารถเข้าถึงเกมได้ตลอด 24 ชั่วโมงผ่านสมาร์ทโฟน แท็บเล็ต และคอมพิวเตอร์ โดยไม่มีข้อจำกัดด้านสถานที่ในการใช้งาน
สล็อตออนไลน์ยุคใหม่
เกมสล็อตสมัยใหม่มาพร้อมกราฟิก 3 มิติ ระบบเสียงที่สมจริง และโบนัสที่หลากหลายกว่าเดิม
เกมจำนวนมากมาพร้อมระบบแจ็คพอตสะสมและฟีเจอร์พิเศษต่าง ๆ ทำให้รูปแบบการเล่นมีความหลากหลายมากกว่าเดิม
Direct API มีความสำคัญอย่างไร
Direct API เป็นรูปแบบการเชื่อมต่อข้อมูลแบบตรงระหว่างผู้ให้บริการและเกม ซึ่งช่วยลด Latency และเพิ่มประสิทธิภาพในการทำงาน
ข้อดีของการเชื่อมต่อแบบ Direct API ได้แก่
เพิ่มความเร็วในการตอบสนอง
รองรับทราฟฟิกสูง
ประมวลผลข้อมูลแบบ Real-Time
เพิ่มความเสถียรในการให้บริการ
เพิ่มความยืดหยุ่นในการพัฒนา
เทคโนโลยีนี้มักทำงานร่วมกับ Cloud Infrastructure ที่สามารถขยายทรัพยากรได้ตามปริมาณผู้ใช้งาน
ระบบ RNG และความโปร่งใส
RNG เป็นระบบสุ่มผลลัพธ์ที่ใช้ในเกมสล็อต
แต่ละรอบการเล่นจึงเป็นอิสระจากกันและไม่สามารถคาดเดาผลลัพธ์ล่วงหน้าได้
RNG ที่มีคุณภาพจะได้รับการตรวจสอบจากหน่วยงานที่เกี่ยวข้อง เพื่อสร้างความเชื่อมั่นในด้านความโปร่งใสและความยุติธรรมของระบบ
fussballwetten-De.com · June 19, 2026 at 11:25 am
richtig tippen sportwetten
my site :: fussballwetten-De.com
https://madesocials.com/ · June 19, 2026 at 1:24 pm
References:
Habbo casino https://madesocials.com/story7114934/casino-of-gold-ihr-weg-zum-jackpot
hoki1881 · June 19, 2026 at 2:08 pm
hoki1881
Dennisesozy · June 19, 2026 at 2:14 pm
hoki1881
https://single-bookmark.com/story21574457/casino-of-gold-ihr-weg-zum-jackpot · June 19, 2026 at 4:14 pm
References:
Keno payouts https://single-bookmark.com/story21574457/casino-of-gold-ihr-weg-zum-jackpot
pg slot · June 19, 2026 at 10:30 pm
สล็อต
ก้าวสู่ยุคใหม่ของสล็อตออนไลน์ปี 2026: วิวัฒนาการของ API ในอุตสาหกรรม iGaming
ตลาดสล็อตออนไลน์ยังคงขยายตัวอย่างต่อเนื่องในปี 2026 ด้วยการพัฒนาเทคโนโลยีที่ช่วยยกระดับทั้งประสิทธิภาพ ความเสถียร และประสบการณ์ของผู้ใช้งาน
ผู้เล่นสามารถเข้าถึงเกมได้ตลอด 24 ชั่วโมงผ่านสมาร์ทโฟน แท็บเล็ต และคอมพิวเตอร์ โดยไม่ถูกจำกัดด้วยสถานที่หรือเวลา
สล็อตออนไลน์ยุคใหม่
สล็อตออนไลน์ยุคใหม่ถูกออกแบบให้มีภาพ เสียง และรูปแบบการเล่นที่ทันสมัยยิ่งขึ้น
หลายเกมใช้ระบบ Progressive Jackpot และกลไกพิเศษที่ช่วยเพิ่มความหลากหลายในการเล่น ช่วยเพิ่มความตื่นเต้นและความสนุกให้กับผู้เล่น
Direct API มีความสำคัญอย่างไร
Direct API เป็นรูปแบบการเชื่อมต่อข้อมูลแบบตรงระหว่างผู้ให้บริการและเกม ทำให้ระบบมีความรวดเร็วและมั่นคงมากขึ้น
ข้อดีของการเชื่อมต่อแบบ Direct API ได้แก่
ลด Latency
รองรับผู้ใช้งานจำนวนมากพร้อมกัน
ประมวลผลข้อมูลแบบ Real-Time
เพิ่มความเสถียรในการให้บริการ
รองรับการอัปเดตระบบได้รวดเร็ว
เทคโนโลยีนี้มักทำงานร่วมกับ Cloud Infrastructure ที่สามารถขยายทรัพยากรได้ตามปริมาณผู้ใช้งาน
ระบบ RNG และความโปร่งใส
Random Number Generator ทำหน้าที่กำหนดผลลัพธ์แต่ละรอบแบบสุ่ม
ทุกการหมุนเป็นอิสระและไม่สามารถทำนายผลลัพธ์ล่วงหน้าได้
ระบบ RNG มาตรฐานต้องผ่านการรับรองจากองค์กรภายนอก เพื่อสร้างความเชื่อมั่นในด้านความโปร่งใสและความยุติธรรมของระบบ
pera789 · June 20, 2026 at 5:20 am
I really love the interface here. The payouts are fast and the games are super smooth. Highly recommended for everyone! Check it out at pera789
jilibetcasino · June 20, 2026 at 5:21 am
Jili slots are the best and this site hosts them perfectly. Fast loading times and big wins. I am hooked. jilibetcasino
phlbest · June 20, 2026 at 5:21 am
This is hands down one of the best platforms I have tried so far. The games are exciting and the bonuses are generous. Try phlbest
Cheryle · June 20, 2026 at 8:00 pm
casino what does stake me mean in the gambler (Cheryle) british columbia united kingdom, australia casino
pokies and high roller pokies united states, or trusted uk casinos
https://altinbasaktohum.com.tr/playing-slots-tips-australia/ · June 20, 2026 at 8:27 pm
no wager no deposit bonus united states, how to win on pokie machines usa and do you have to pay tax on casino winnings
in canada, or online casino reviews united states
Here is my blog neon bingo; https://altinbasaktohum.com.tr/playing-slots-tips-australia/,
Sang · June 20, 2026 at 8:48 pm
united statesn slot machine emulator, united statesn bingo rules and new zealand bingo how to play, or
free united statesn slot machine games
My blog post; mr burns casino germs – Sang –
thesocialroi.com · June 20, 2026 at 10:58 pm
References:
Betclic casino https://thesocialroi.com/story11529327/casino-of-gold-ihr-weg-zum-jackpot
Latosha · June 21, 2026 at 12:59 am
latest online casinos canada, 5 dollar min deposit zorro casino game download for free;
Latosha,
united states and play yukon gold slot machine, or uk
gambling license conditions
https://bookmarklinx.com/story21627443/casino-of-gold-ihr-weg-zum-jackpot · June 21, 2026 at 1:11 am
References:
Vegas slots https://bookmarklinx.com/story21627443/casino-of-gold-ihr-weg-zum-jackpot
is zero even or odd in roulette · June 21, 2026 at 7:26 pm
poker stars sign up bonus uk, free spins no
deposit usa 888 and usa slot machines, is zero even or odd in roulette united statesn online no deposit pokies
How is Blackjack played in Vegas · June 21, 2026 at 8:14 pm
ladbrokes casino canada, popular pokie machines australia and best new
uk bingo sites, or poker with real money usa
Also visit my homepage How is Blackjack played in Vegas
Adrian · June 21, 2026 at 8:40 pm
can you play online pokies in united states for real money storm casino sign up (Adrian), online slots casino australia and united statesn no deposit casino bonus codes, or are poker machines legal in western canada
http://www.mama4mama.it · June 21, 2026 at 8:59 pm
new usa online casinos no deposit bonuses, golden tiger casino nights (http://www.mama4mama.it) uk and
is bingo gambling in canada, or united statesn casinos still accepting skrill
ทดลองเล่นสล็อต pg · June 22, 2026 at 12:38 am
pg slot
อนาคตของสล็อตออนไลน์ในปี 2026: เทคโนโลยี API และอนาคตของ iGaming
อุตสาหกรรมสล็อตออนไลน์ยังคงเติบโตอย่างต่อเนื่องในปี 2026 จากนวัตกรรมที่ช่วยเพิ่มประสิทธิภาพของระบบ ความเสถียร และคุณภาพการใช้งาน
การเข้าถึงเกมสามารถทำได้ตลอดเวลาผ่านอุปกรณ์หลากหลายประเภท โดยไม่มีข้อจำกัดด้านสถานที่ในการใช้งาน
สล็อตออนไลน์ยุคใหม่
สล็อตออนไลน์ยุคใหม่ถูกออกแบบให้มีภาพ เสียง และรูปแบบการเล่นที่ทันสมัยยิ่งขึ้น
ผู้พัฒนาเกมนิยมเพิ่มระบบรางวัลสะสมและโบนัสรูปแบบใหม่ ส่งผลให้ประสบการณ์โดยรวมมีความสมจริงและน่าสนใจยิ่งขึ้น
Direct API มีความสำคัญอย่างไร
Direct API ช่วยให้ข้อมูลถูกส่งระหว่างระบบต่าง ๆ ได้โดยตรง ซึ่งช่วยลด Latency และเพิ่มประสิทธิภาพในการทำงาน
ข้อดีของการเชื่อมต่อแบบ Direct API ได้แก่
ลดความหน่วงของระบบ
รองรับทราฟฟิกสูง
ส่งข้อมูลแบบเรียลไทม์
ลดโอกาสเกิดปัญหาระบบ
ช่วยให้การปรับปรุงระบบทำได้ง่ายขึ้น
เทคโนโลยีนี้มักทำงานร่วมกับ Cloud Infrastructure ที่สามารถขยายทรัพยากรได้ตามปริมาณผู้ใช้งาน
ระบบ RNG และความโปร่งใส
Random Number Generator ทำหน้าที่กำหนดผลลัพธ์แต่ละรอบแบบสุ่ม
ทุกการหมุนเป็นอิสระและไม่สามารถทำนายผลลัพธ์ล่วงหน้าได้
ระบบ RNG มาตรฐานต้องผ่านการรับรองจากองค์กรภายนอก เพื่อยืนยันความโปร่งใสและความเป็นธรรมของเกม
Www.Balegia.com · June 22, 2026 at 4:43 am
neue sportwetten seiten
Visit my blog: basketball wetten system (http://Www.Balegia.com)
https://www.Kita-diegrashuepfer.de/wie-man-mit-wettunterlagen-umgeht-und-sie-Sinnvoll-nutzt/ · June 22, 2026 at 4:59 am
was heißt handicap wette
Feel free to visit my web site – nba basketball wett tipps
(https://www.Kita-diegrashuepfer.de/wie-man-mit-wettunterlagen-umgeht-und-sie-Sinnvoll-nutzt/)
Jorg · June 22, 2026 at 8:55 am
online pokies crash gambling fake money (Jorg) australia, 888 poker app united kingdom and
usa casino news, or united states live casino
wetten basketball Nba · June 22, 2026 at 8:57 am
sportwetten neukundenbonus vergleich
Have a look at my web page … wetten basketball Nba
Layne · June 22, 2026 at 9:02 am
bouka spins no deposit bonus code, legal canadian online
pokies and no deposit bonus uk poker, or best australia pokies
my blog – casino in queens open today (Layne)
https://theconqueror.com.Mx/ · June 22, 2026 at 12:00 pm
legal gambling sites canada, best rated online pokies new zealand and free usa cash bingo, or online 400% casino Bonus – https://theconqueror.com.Mx/, no deposit bonus
keep what you win united states 2021
Jewell · June 22, 2026 at 12:47 pm
free pokies canada aristocrat, no deposit bonus on sign up
usa and black jack australia, or uk slot sites not on gamstop
My site … games apps to win real money philippines (Jewell)
Starla · June 22, 2026 at 1:54 pm
new zealandn no deposit bonus pokies, legitimate online pokies australia and new zealandn casino no deposit bonus codes, or latest free spins no deposit usa
Also visit my website – senior bus trips to casinos –
Starla –
Gambling College Basketball · June 22, 2026 at 2:54 pm
play online pokies for real money in canada, is there a casino
in sydney united states and poker run thousand islands
2021, or Gambling College Basketball bonuses
co usa
Elmo · June 22, 2026 at 3:30 pm
nj online casino blackjack (Elmo) pokies canada law, fishing freuky slot game and casino in connecticut usa, or canadian online gambling
best video Blackjack vegas · June 22, 2026 at 4:08 pm
united statesn roulette online fast, top paying online casinos canada and online australian pokies, or pokies online casino australia
Here is my website best video Blackjack vegas
Renaldo · June 22, 2026 at 4:50 pm
casino in phuket, do you have to pay taxes on gambling winnings in australia and odds of
winning pokies united states, or casino no deposit bonus codes 2021 united states
Take a look at my webpage free play blackjack rules (Renaldo)
real Casino game apps · June 22, 2026 at 7:24 pm
free chip no deposit real Casino game apps bonus united states, do you have to pay taxes on gambling winnings in australia
and casino in united states, or how to win on the pokies in united states
Punkte wetten basketball · June 22, 2026 at 7:40 pm
wett tipps wochenende
Also visit my web-site: Punkte wetten basketball
环亚官方平台 · June 22, 2026 at 8:17 pm
What’s up, I would like to subscribe for this
weblog to take most recent updates, so where can i do it
please help out.
base sur roulette pour plante · June 22, 2026 at 8:30 pm
online gambling laws in uk, vancouver united states casino and how
many gambling casinos are in the united states, or how to become
a casino dealer uk
My homepage: base sur roulette pour plante
Latrice · June 22, 2026 at 8:57 pm
how to come back from gambling debt (Latrice) much
top online pokies and casinos australian games, usa casino bonuses and bet365 united statesn roulette guide uk, or free spins casino no deposit bonus
united states
Carmela · June 22, 2026 at 9:06 pm
triple shot pokies united states, 888 poker login australia and new zealand
real money full tilt casino download (Carmela), or are there
pokies in new united states
blackjack evolutionary algorithm · June 22, 2026 at 9:58 pm
casino uk pay by phone bill, cash online poker canada and no deposit poker bonus
usa 2021, or win real money online free usa
Here is my blog post blackjack evolutionary algorithm
when did potawatomi casino open · June 22, 2026 at 10:47 pm
real money united statesn online casino, fastest paying when did potawatomi casino open
usa and usa accepted casino, or online roulette usa real
money review
Porfirio · June 22, 2026 at 11:27 pm
online casino usa bonus, united statesn roulette odds
can you bet on both black and red in roulette (Porfirio) best bingo sites uk 2021, or
free united statesn slot machine games
Olg first deposit Promo · June 23, 2026 at 12:29 am
online casino winners usa, rules of gambling usa and new zealandn online pokies for
real money, or canadian online gambling
Feel free to visit my website – Olg first deposit Promo
环亚彩票 · June 23, 2026 at 12:48 am
I’d like to find out more? I’d want to find out more details.
vip casino malaysia · June 23, 2026 at 2:05 am
best casino bonus new zealand, slot payback info united
states and australian vip casino malaysia free spins, or
uk poker forum
Blackjack bucket · June 23, 2026 at 2:11 am
free casino slots in united kingdom, top slot games uk and whats the largest casino in australia, or
new zealandn free chip casino
My web page: Blackjack bucket
what is the difference Between A place bet and a buy bet in craps · June 23, 2026 at 2:37 am
online casino united states that accept paysafe, semyon dusaach blackjack what is the difference Between A place bet and a buy bet in craps
usa casino free no deposit bonus, or united statesn online
casino best
Teresa · June 23, 2026 at 3:05 am
canadian poker stars, slot payback info united states
and free united statesn poker money, or top
ez baccarat online casino (Teresa) pokies and casinos canadian free games
Tammie · June 23, 2026 at 4:02 am
netent 100 casino moons; Tammie, list
usa, casino ratings canada and las vegas usa casino online no deposit bonus codes, or bingo no deposit bonus
win real money united states
Verla · June 23, 2026 at 4:18 am
famous united statesn poker, online slots usa fast withdrawal and best online casino united kingdom real
money, or online how to ban gambling on iphone (Verla) united states
banned
lowest minimum craps table vegas · June 23, 2026 at 4:30 am
best online casino bc australia, rules of gambling usa and no deposit free bonus spins usa aug,
28,2021, or starburst slots uk
Also visit my web site … lowest minimum craps table vegas
cassino online · June 23, 2026 at 4:53 am
Eae, pergunta séria sobre jogo do baccarat? procede?
Emmanuel · June 23, 2026 at 6:00 am
wetten prognose heute
Also visit my web blog :: nba basketball wett tipps (Emmanuel)
Camh Gambling · June 23, 2026 at 6:01 am
free $100 casino chip 2021 uk, no deposit bingo bonus uk and free spins new usa, or
are slot machines illegal in united kingdom
Visit my web-site – Camh Gambling
Kellee · June 23, 2026 at 6:07 am
wettanbieter vergleich paypal
Also visit my web-site basketball unentschieden wetten [Kellee]
blackjack Seed coverage · June 23, 2026 at 6:47 am
united kingdom pokies online real money, free money online casino
canada and new no deposit casino bonus uk, or united kingdom poker machine game
download
Feel free to surf to my web page – blackjack Seed coverage
https://www.kfz-Steinert.de/cs2-quoten-kalkulation-so-berechnest-du-deine-gewinne/ · June 23, 2026 at 8:24 am
online wetten ohne einzahlung
My web blog; ncaa basketball wett vorhersage üBer tore untertore (https://www.kfz-Steinert.de/cs2-quoten-kalkulation-so-berechnest-du-deine-gewinne/)
Indiana · June 23, 2026 at 8:31 am
safe online poker sites united states, is online slots legal in australia and new
casino online usa 2021, or betsoft no deposit bonus united states
Have a look at my blog :: how to play craps videos (Indiana)
Lasonya · June 23, 2026 at 10:51 am
gambling illegal usa, no deposit online australian casinos and gambling issues in australia, or
best online pokies new zealand casino
Here is my webpage – casinoeuro 35, Lasonya,
play live baccarat free · June 23, 2026 at 12:27 pm
new zealandn online casino minimum deposit $10,
united kingdom poker league ceo and australian casino play live baccarat free spins,
or new zealandn poker table
blackjack Lanza wrestler · June 23, 2026 at 1:05 pm
australian pm blackjack Lanza wrestler,
online casino united states 1 dollar deposit and usa casino fast withdrawal, or top 10 casino canada
http://bcnfusio.cat/uk-casino-Online-tax/ · June 23, 2026 at 1:10 pm
is online pokies banned in united states, united statesn roulette betting strategy and directions to
potawatomi casino in milwaukee, or live uk poker tournaments
Feel free to surf to my web site :: blackjack american Alligator boots (http://bcnfusio.cat/uk-casino-Online-tax/)
Yvette · June 23, 2026 at 1:19 pm
best online slot usa, auto poker dealer and casino
apps for real money australia, or free online
pokies no deposit united kingdom
Also visit my web blog – gambling legal in nj – Yvette –
d2 gambling worth it · June 23, 2026 at 1:43 pm
canadian casino guide blackjack chart, best australian online casinos and
united statesn online casinos 2021 real money, or is online d2 gambling worth it in canada legal
can you win real money on bovada · June 23, 2026 at 2:14 pm
auto wheel roulette play usa online, bet365 free casino usa
and uk casino 10 no deposit, or how to deposit cash into paypal canada
My blog post – can you win real money on bovada
basketball-wetten.com · June 23, 2026 at 2:36 pm
asiatische wetten erklärung
Visit my page: basketball-wetten.com
Tracey · June 23, 2026 at 3:56 pm
gambling statistics uk 2021, can you play poker online bonus code for online casinos – Tracey, real money in united kingdom and casinos in central united kingdom, or
bingo uk online
money glitch casino Heist · June 23, 2026 at 8:26 pm
online bingo games united statesn residents, new online money glitch casino Heist united states 2021 and united statesn pokies
companies, or bingo united kingdom on gsn
Randy · June 23, 2026 at 9:03 pm
when will pokies reopen south united states,
winner slots uk best and worst odds in casino (Randy) free $30 pokies united states, or bingo uk online
Lamont · June 23, 2026 at 10:16 pm
best rated payout online casino app for real money (Lamont) nz, free spins for registration usa 2021 and
slot machines are called in canada, or best payout online slots australia
Mack · June 23, 2026 at 10:41 pm
new uk casino no deposit free spins, online slot casino usa
and usa online in fast five who won in the casino – Mack – no deposit bonus codes,
or casinos for gambling for uk
Richie · June 24, 2026 at 12:31 am
canadian original free slots, best new zealandn online real
money pokies and windsor casino in united states, or internet gambling
uk
Also visit my homepage :: no deposit games (Richie)
hoki1881 · June 24, 2026 at 1:57 am
hoki1881
Grubhub Blackjack Pizza · June 24, 2026 at 2:05 am
casino in quebec canada, casino sites usa no deposit bonus and bet365 Grubhub Blackjack Pizza hints uk,
or fully cashable no deposit bonus australia
https://www.multisol-parquets.ch · June 24, 2026 at 2:10 am
crypto gambling sites uk, gambling stocks in united states
and new zealand real money pokies app, or australian How much to buy
a casino in vegas [https://www.multisol-parquets.ch] free chips
casino san carlos mendoza · June 24, 2026 at 2:58 am
united kingdom gambling online, latest no deposit casino san carlos mendoza bonuses usa and online casino united statesn legal real money no deposit
bonus, or northern lights casino uk
casino machine a sous gratuit demo · June 24, 2026 at 3:48 am
statistics of gambling in canada, play free slots united states and online pokies
australia no deposit signup bonus, or usa online casino machine a sous gratuit demo lists
apuestas bayern barcelona · June 24, 2026 at 4:23 am
mejores apuestas bayern barcelona formula 1
Steven · June 24, 2026 at 5:12 am
online gambling legal in united states, are there any legal online poker
sites in australia and free online gambling united states, or free spins on signup no deposit uk
My blog; spicy sauce roulette (Steven)
Apuestas Deportivas Con Puntos Virtuales · June 24, 2026 at 5:14 am
Apuestas Deportivas Con Puntos Virtuales sin deposito
Humberto · June 24, 2026 at 5:25 am
gambling costs in australia, online poker casino real money in usa and online poker with friends australia, or united kingdom roulette game wheel
my web blog where did casinos originate, Humberto,
Karolyn · June 24, 2026 at 5:25 am
umiejetnosci bukmacher – Karolyn, nhl
typy
casino battle royale aew 2022 · June 24, 2026 at 5:30 am
new no deposit uk casino battle royale aew 2022 2021,
golden tiger casino uk and big usa slot wins, or top online pokies nz
virgin casino Online app · June 24, 2026 at 5:35 am
how many native united statesn casinos are there, united statesn online
casino win real money and online gambling uk legal, or canadian online virgin casino Online app with $5 deposit
https://nl-betting.com/ · June 24, 2026 at 6:45 am
sportbeste hoe wedden op bookmaker 2026 (https://nl-betting.com/)
Gwendolyn · June 24, 2026 at 7:11 am
best live dealer roulette (Gwendolyn) online slots
payout percentage usa, 888 poker withdrawal united states and slot machines sale united
states, or new zealandn online casino no deposit bonus 2021
future of Online casinos · June 24, 2026 at 7:30 am
gaming club casino usa login, do casinos pay out in cash uk and canadian future of Online casinos casino free signup
bonus, or united statesn gambling regulations
what's a bust card in blackjack · June 24, 2026 at 8:55 am
united kingdom roulette rules, 888 casino nz and united statesn roulette strategy to win big, or best canada poker sites
My web-site … what’s a bust card in blackjack
Albert · June 24, 2026 at 9:46 am
pokies return rate canada, slot free spins no deposit uk and bet365 money blackjack usa,
or best no deposit top 10 european online casinos (Albert) aus
Toney · June 24, 2026 at 10:18 am
casino in british columbia united kingdom, united statesn roulette odds and
united statesn online slots real money, or usa super pala casino entertainment director [Toney]
Helen · June 24, 2026 at 10:34 am
united statesn online casinos real money, new zealandn online casino sign up no deposit bonus and
new zealandn free slots no download, or deposit 10 get usa
Here is my blog :: white sox gambling (Helen)
Autumn · June 24, 2026 at 10:41 am
bet365 united kingdom roulette layout, usa casino sign up bonus and free
spins no deposit united kingdom casino, or best australia pokies
Feel free to visit my website … montecasino spa (Autumn)
is commerce casino open now · June 24, 2026 at 10:48 am
the best online is commerce casino open now for usa, slot free spins no deposit uk and online bingo usa, or online
gambling united states banned
Kay · June 24, 2026 at 11:14 am
200 free spins no deposit usa casinos, online slots bonausaa
and play slots for real money usa, or top 10 casino no deposit bonus austria (Kay)
canada
how old do you have to Be to gamble at indian casinos · June 24, 2026 at 12:02 pm
united statesn roulette wheel play, free 10 no
deposit casino usa and online casino united statesn dollars, or highest payout online casino usa
My blog :: how old do you have to Be to gamble at indian casinos
Shelby · June 24, 2026 at 12:06 pm
prepaid visa for online gambling uk, best paying pokies united
kingdom and how old do you have to be to go in a big fish casino cheats for android (Shelby) usa,
or casinos in toronto united kingdom
shabar mantra for gambling · June 24, 2026 at 12:25 pm
aristocrat pokies real money united kingdom, vancouver
united states casino and buy pokie machine usa, or no deposit casino real money usa
Also visit my page :: shabar mantra for gambling
how old do you have to be to gamble at tachi Palace · June 24, 2026 at 12:41 pm
best australia casino no deposit bonus, poker usa artrix and no
deposit free bonus casinos usa, or casinos that accept neteller australia
my web site: how old do you have to be to gamble at tachi Palace
Layne · June 24, 2026 at 12:42 pm
bouka spins no deposit bonus code, united kingdom roulette free download
and top 10 online casinos pa – Layne, slots free
bonus no deposit uk, or native united statesn tribal casinos
fish casino app for android · June 24, 2026 at 2:23 pm
online gambling sites in the usa, $10 deposit bonus casino
nz and free online poker united states, or online fish casino app for android guide uk
Aundrea · June 24, 2026 at 4:08 pm
online casinos in ontario australia, australian online real money casino and
canadian best tips to play roulette; Aundrea, app, or casino usa bonus
wind creek casino age requirement · June 24, 2026 at 4:47 pm
an canadian casino, wind creek casino age requirement games canada and canadian casino
sign up no deposit bonus, or casino classic uk
Loreen · June 24, 2026 at 5:12 pm
united kingdom online casino minimum deposit dollar 10, no deposit
online casino voucher codes (Loreen) casino united states and united kingdom online pokies 2021, or canadian accepted online poker sites
online casino game win real money · June 24, 2026 at 5:36 pm
eur 20 free no deposit casino uk 2021, how to win on pokie machines usa and free no deposit australia casino, or united kingdom online casino game win real money real pokies
Play free roulette no download · June 24, 2026 at 5:45 pm
usa online casinos new, claiming gambling winnings in united kingdom and united kingdom online pokies 2021, or casino uk Play free roulette no download spins
betmgm Casino Bonus codes · June 24, 2026 at 6:38 pm
how many native united statesn casinos are there, 20 free spins on registration usa and free imatant
spins no deposit betmgm Casino Bonus codes united states, or how to play pokies in canada
gamble with google Play credit · June 24, 2026 at 6:50 pm
888 poker promotion code united states, free spins no deposit casinos usa and no deposit casino bonus usa august 2021, or paysafe casinos uk
Feel free to surf to my blog: gamble with google Play credit
5 pound No Deposit Casino · June 24, 2026 at 7:14 pm
5 pound No Deposit Casino euro uk login, new 2021
usa online casinos and poker for real money in usa, or united
kingdom civil war poker tables
Julianne · June 24, 2026 at 7:36 pm
paypal gambling sites canada, casino games canada
and good morning united states time slot, or online canadian can i do casino heist solo
(Julianne) real money
gambling games to play for free · June 24, 2026 at 7:44 pm
when are pokies opening in south united states,
betsoft no deposit bonus united kingdom and casino online jackpot usa
5f bonus, or usa poker app
Feel free to surf to my blog gambling games to play for free
Pferderennen wetten schweiz · June 24, 2026 at 9:01 pm
sportwetten anbieter gratiswette
my web page: Pferderennen wetten schweiz
Hai · June 24, 2026 at 9:23 pm
best online poker usa real money, canadian gambling statistics 2021
and canada online gambling laws, or new casino in stroudsburg pa (Hai) no deposit free spins uk 2021
Pat · June 24, 2026 at 9:51 pm
$1 min deposit casino australia, best poker online new zealand and free bingo games united states, or usa
$200 no deposit bonus 200 free spins
my web site … why was cousin blackjack so small in spongebob (Pat)
Https://Anhangafilmes.Com.Br/Tipp3-Wetten-Ergebnisse/ · June 24, 2026 at 10:25 pm
quotenvergleich wettbasis
Visit my blog post Sicher Wetten Sportwetten (https://Anhangafilmes.Com.Br/Tipp3-Wetten-Ergebnisse/)
Gia · June 24, 2026 at 11:23 pm
gambling advertising canada, bet365 play blackjack online uk and foxwoods casino open (Gia)
sarnia ontario australia, or united statesn online casino minimum
deposit $10
Where Is There Gambling In The Caribbean · June 25, 2026 at 12:25 am
best poker app usa, united kingdom casino documentary online and online casino united
statesn legal real money no deposit bonus, or casino uk free spins
Here is my web page; Where Is There Gambling In The Caribbean
Allan · June 25, 2026 at 12:50 am
the great united statesn casino everett,
win real money online instantly usa and age of gods
slots uk, or best united statesn using vpn for online casino
(Allan) gambling
Monroe · June 25, 2026 at 1:15 am
bet365 united kingdom roulette layout, real money pokies canada app and best online golden casino
review [Monroe] united kingdom fast payouts, or poker usa
tournaments
Shelly · June 25, 2026 at 1:23 am
bet365 roulette strategy usa, best non usa casino sites and roulette australia rules,
or bingo liner uk
Look into my webpage – online gambling in france (Shelly)
Grady · June 25, 2026 at 1:42 am
united statesn betstars casino (Grady) no deposit free spins, casino sites usa no deposit bonus
and best online casino united kingdom fast payouts, or new casinos no deposit bonus usa
Calvin · June 25, 2026 at 2:23 am
top online pokies and casinos australian deals, non gamstop casinos uk and online poker
canada two plus two, or trusted casino online usa
my blog post :: bingo matematik (Calvin)
Best casino Stocks to Buy right now · June 25, 2026 at 2:47 am
free spins Best casino Stocks to Buy right now no deposit usa, casino new south wales united states and new usa
casinos free spins, or gambling age in the usa
Lynda · June 25, 2026 at 3:21 am
80 free spins no deposit uk, best live blackjack sites usa cash and
casino chips (Lynda) td australia visa debit gambling, or new
uk based online casino
Richard · June 25, 2026 at 3:38 am
yusaon gold slots, united states online casino slots and uk latest online york pa mini casino – Richard -, or is online bingo legal in canada
Randy · June 25, 2026 at 3:44 am
best new casino sites usa, best gambling websites usa and what
poker sites are legal in australia, or pay by phone bill tips for the diamond casino heist (Randy) australia
what is a split hand in blackjack · June 25, 2026 at 4:04 am
free $100 casino chip 2021 uk, craps tutorial usa and run it once poker canada, or
big uk slot wins
Here is my blog; what is a split hand in blackjack
Mari · June 25, 2026 at 6:33 am
wett prognose
Also visit my homepage – mathematische wettstrategie, Mari,
https://Pt-betting.com/ · June 25, 2026 at 7:07 am
casas melhores sites de aposta online; https://Pt-betting.com/,
apostas limitam
bonus Kaufen Slots um geld spielen · June 25, 2026 at 7:28 am
casino mit auszahlung auf bitcoin wallet
my web site … bonus Kaufen Slots um geld spielen
casino 300 euro startguthaben · June 25, 2026 at 7:46 am
roulette online um geld spielen
Feel free to visit my blog; casino 300 euro startguthaben
online casino ohne umsatzbedingungen klarna · June 25, 2026 at 8:17 am
online casino ohne umsatzbedingungen klarna 5 euro einzahlung
revolut
handicap wette erklärt · June 25, 2026 at 8:43 am
quote bei wetten dass
my website; handicap wette erklärt
beste Casinos mit niedriger mindesteinzahlung · June 25, 2026 at 9:02 am
casino 15 euro bonus ohne einzahlung
Stop by my web page beste Casinos mit niedriger mindesteinzahlung
https://WWW.Lojadovinil.Com.br/Site/besten-buchmacher-2025/ · June 25, 2026 at 9:14 am
sportwette tipps
Look at my web blog – beste App sportwetten (https://WWW.Lojadovinil.Com.br/Site/besten-buchmacher-2025/)
casino 4 euro handyrechnung · June 25, 2026 at 9:18 am
echt geld casino 4 euro handyrechnung
app
roulette bis 5000 euro einsatz · June 25, 2026 at 9:56 am
online casino bonus ohne einzahlung aktuell
Here is my blog … roulette bis 5000 euro einsatz
Sportwetten In Der NäHe · June 25, 2026 at 10:01 am
wettbüro duisburg
My homepage; Sportwetten In Der NäHe
wetten Kostenlos · June 25, 2026 at 10:03 am
beste wettquoten
Also visit my web site; wetten Kostenlos
dryfruitcart.com · June 25, 2026 at 10:23 am
online roulette dogecoin, dryfruitcart.com, blackjack banküberweisung
Aplicativo De Apostas android · June 25, 2026 at 10:23 am
é aposta multipla
Stop by my page: Aplicativo De Apostas android
http://Www.Kabaty.4Fan.cz · June 25, 2026 at 10:25 am
casinos weltweit
my web blog :: online roulette Schnellspiel (http://Www.Kabaty.4Fan.cz)
wetten ohne einzahlung österreich · June 25, 2026 at 10:31 am
online wetten ohne einzahlung österreich mit startguthaben ohne einzahlung
Gemma · June 25, 2026 at 10:39 am
gratiswette bei anmeldung
my blog: back und lay wetten anbieter (Gemma)
wettanbieter ohne Lugas mit paypal · June 25, 2026 at 10:47 am
wettseiten einzahlungsbonus
Also visit my web blog wettanbieter ohne Lugas mit paypal
casino mit 250 euro einzahlung paysafecard · June 25, 2026 at 10:54 am
kenozahlen vom sonntag
Stop by my homepage – casino mit 250 euro einzahlung paysafecard
Online Wetten Beste Anbieter · June 25, 2026 at 11:15 am
sportwetten neukundenbonus vergleich
My blog: Online Wetten Beste Anbieter
Violette · June 25, 2026 at 11:21 am
beste live casino klarna
My webpage: scratch cards um echtes geld
(Violette)
Julianne · June 25, 2026 at 11:25 am
online casino für sachsen-anhalt (Julianne) casino bonus geld auszahlen
blackjack casino visa · June 25, 2026 at 11:44 am
persönliche permanenz roulette
Here is my web-site … blackjack casino visa
casino Ohne limit bremen · June 25, 2026 at 11:52 am
slots um echtgeld
Also visit my page – casino Ohne limit bremen
sapporo88 · June 25, 2026 at 11:56 am
sapporo88
Casino 5 Euro Einzahlung Cashlib · June 25, 2026 at 12:03 pm
online Casino 5 Euro Einzahlung Cashlib
ohne identitätsprüfung
Jan · June 25, 2026 at 12:07 pm
roulette schwarze zahlen
Also visit my web page – die besten online casinos paypal (Jan)
online casino 2 euro ethereum · June 25, 2026 at 1:23 pm
beste online casino 2 euro ethereum casinos mit giropay
echtes geld gewinnen ohne einzahlung · June 25, 2026 at 1:38 pm
online casino 15 euro neosurf
Check out my web page: echtes geld gewinnen ohne einzahlung
Annetta · June 25, 2026 at 2:01 pm
casino mit neteller
Feel free to surf to my web blog :: keno app um echtes
geld (Annetta)
casino deutsche welle · June 25, 2026 at 2:06 pm
bester casino deutsche welle reload
angebot
Sibyl · June 25, 2026 at 2:54 pm
online spielautomaten ethereum bezahlen
Here is my webpage: casino cashlib ab 30 euro [Sibyl]
lizenz wettbüro · June 25, 2026 at 3:04 pm
ohne einzahlung sportwetten
my website – lizenz wettbüro
online casino ab 1 Euro google pay · June 25, 2026 at 3:08 pm
roulette spielbank
my web blog … online casino ab 1 Euro google pay
spielplan füR Roulette · June 25, 2026 at 3:14 pm
beste live casino google pay
Review my web blog … spielplan füR Roulette
casino jeton ab 25 Euro · June 25, 2026 at 3:14 pm
slot spiele mit paypal
my web-site :: casino jeton ab 25 Euro
Slots mit 96 prozent rtp · June 25, 2026 at 4:13 pm
30 free spins ohne einzahlung
Visit my site … Slots mit 96 prozent rtp
https://spmb.Alqolam.ac.id/ · June 25, 2026 at 4:41 pm
deutsche Casino einsatzlimit; https://spmb.Alqolam.ac.id/,
bonus
Tina · June 25, 2026 at 4:49 pm
casino 100 euro litecoin (Tina) 20 einzahlen 50 bekommen
Maddison · June 25, 2026 at 7:36 pm
die besten wett strategien (Maddison) tipps für heute
https://Www.Ozident.com · June 25, 2026 at 7:48 pm
casino ehrliche casinos mit Paysafecard – https://Www.Ozident.com,
lizenz nrw
online casino 3 euro mastercard · June 25, 2026 at 8:36 pm
online casino 3 euro mastercard
casino mit handy guthaben aufladen
https://Excellentprowork.hu/traume-davon-geld-am-spielautomaten-zu-gewinnen-2026/ · June 25, 2026 at 10:07 pm
casino 20 euro einzahlung skrill, https://Excellentprowork.hu/traume-davon-geld-am-spielautomaten-zu-gewinnen-2026/, 100 euro litecoin
Spielautomaten ab 1 euro · June 25, 2026 at 10:12 pm
online casino 50 Spielautomaten ab 1 euro cashtocode
slots Casino astropay · June 25, 2026 at 10:16 pm
slots Casino astropay 5 euro neosurf
360 Casino bonus ohne Einzahlung · June 25, 2026 at 11:14 pm
mit wie vielen karten spielt man blackjack
Feel free to surf to my blog post … 360 Casino bonus ohne Einzahlung
Neue Slots Mit Bonus Kaufen · June 25, 2026 at 11:32 pm
classic blackjack um geld spielen
Feel free to surf to my web-site; Neue Slots Mit Bonus Kaufen
Myra · June 26, 2026 at 12:09 am
freispiele bei erster einzahlung
Have a look at my blog post; casino 2026 ludwigshafen (Myra)
Https://broderickmovers.com/ · June 26, 2026 at 12:48 am
online casino tether mindesteinzahlung (https://broderickmovers.com/) mit vpn spielen
Jeyddtiieu.cfolks.pl · June 26, 2026 at 2:02 am
slots neue casinos mit live dealer (Jeyddtiieu.cfolks.pl) tumbling reels
what is exacta box bet · June 26, 2026 at 6:51 am
how do you bet on horse racing online
Here is my website: what is exacta box bet
Ai governance · June 26, 2026 at 7:50 pm
Ai governance
ai testing and ai assurance · June 27, 2026 at 11:46 pm
Ai governance
Desmond · June 28, 2026 at 3:37 am
betting on the grand national
Feel free to surf to my blog post :: greyhound race track results (Desmond)
Casino ohne Verifizierung astropay · June 28, 2026 at 7:53 am
Casino ohne Verifizierung astropay roulette leipzig
https://www.sapivikimakeup.hu/ · June 28, 2026 at 8:28 am
casino spiele mit leiter
My web-site :: slots online freispiele ohne anzahlung (https://www.sapivikimakeup.hu/)
Leopoldo · June 28, 2026 at 9:02 am
online casinos ohne limits (Leopoldo) casino 4 euro
einzahlung paypal
Vernon · June 28, 2026 at 9:14 am
casino jeton ab 1 euro
Here is my page: neue sportwetten; Vernon,
online Casino cashlib Einzahlung ohne anmeldung · June 28, 2026 at 9:16 am
online Casino cashlib Einzahlung ohne anmeldung jeton ab 100 euro
https://Ngoinhavietgroup.Com.vn/2026/05/29/Kostenlos-ohne-anmeldung-casino-2026/ · June 28, 2026 at 9:47 am
online casino webmoney bezahlen (https://Ngoinhavietgroup.Com.vn/2026/05/29/Kostenlos-ohne-anmeldung-casino-2026/) 20 euro flexepin
Real Casino Apps That Pay Real Money · June 28, 2026 at 10:10 am
the top online pokies and casinos in united states legit, online Real Casino Apps That Pay Real Money no deposit bonus free spins usa and state gambling revenue australia,
or best united statesn online casino no deposit bonus
2021
Test.Hospodapraha.Cz · June 28, 2026 at 10:11 am
ladbrokes casino canada, big poker tournaments uk and casino in connecticut usa, or
canadian accepted online poker sites
my web page: No Deposit Bonus Codes Forum (Test.Hospodapraha.Cz)
https://www.Egorebel.it/2026/05/06/online-casino-bonus-erfahrungen-2026/ · June 28, 2026 at 11:56 am
online casino 30 euro lastschrift
Also visit my web page … bekannte casinos deutschland
(https://www.Egorebel.it/2026/05/06/online-casino-bonus-erfahrungen-2026/)
Rose · June 28, 2026 at 12:03 pm
how do casinos pump oxygen – Rose,
poker machines work in australia, best online casinos new
zealand and united statesn poker 95 download, or best payout
online slots australia
https://Fgcglass.com/ · June 28, 2026 at 12:08 pm
spielautomaten wattenscheid
Here is my site: bestes gammix Casino; https://Fgcglass.com/,
https://Cmhc.Techzenau.com · June 28, 2026 at 12:10 pm
casino echtgeld rheinland-pfalz; https://Cmhc.Techzenau.com, echtgeld bonus code
ohne einzahlung
Hiram · June 28, 2026 at 12:16 pm
usa bingo search pound, australian online real money
play casino holdem for free (Hiram) and
best bingo sites uk 2021, or new zealandn online casino pokies
Maribel · June 28, 2026 at 12:58 pm
blackjack switch um geld spielen
Check out my page … online spielautomaten mit muchbetter
[Maribel]
Luck Of The Irish Fortune Spins Demo · June 28, 2026 at 1:31 pm
usa casino providers, united kingdom gambling rules and las vegas
usa casino online no deposit bonus codes, or usa casino
no deposit bonus
Feel free to visit my website :: Luck Of The Irish Fortune Spins Demo
Blackjack Switch Casino · June 28, 2026 at 2:41 pm
Blackjack Switch Casino 50 euro jeton
Eugenia · June 28, 2026 at 3:08 pm
online neues casino turnier preisgeld (Eugenia) deutschland auszahlung erfahrungen
Woodrow · June 28, 2026 at 3:32 pm
cimarron casino app (Woodrow) online usa all sites, online gambling uk statistics and the largest casino in australia, or latest australian slot machines
Winnie · June 28, 2026 at 3:52 pm
neue baccarat
Look at my blog post … casino mit 2 euro einzahlung klarna (Winnie)
slots Mit multiplier · June 28, 2026 at 4:28 pm
bei welchem casino kann man 5 euro einzahlen
Feel free to surf to my web site: slots Mit multiplier
Jannette · June 28, 2026 at 5:43 pm
casino amusements united kingdom, united kingdom roulette payout calculator and
new zealandn eagle slot machine, or can i use td canada trust visa debit for online gambling
techniques (Jannette) gambling
royal caribbean explorer of the seas casino · June 28, 2026 at 7:13 pm
united kingdom roulette rules, spin royal caribbean explorer of the seas casino nz login and casino apps real money australia,
or canada online slots
Adalberto · June 28, 2026 at 7:56 pm
echtgeld bonus casino deutschland
Also visit my web blog – spielcasino frankfurt (Adalberto)
blackjack iphone app real money · June 28, 2026 at 8:21 pm
pokies return rate canada, united states free online slots and free spins no deposit uk low wagering, or new zealand star casino
Feel free to visit my webpage … blackjack iphone app real money
früchte Spielautomaten mit paypal · June 28, 2026 at 8:24 pm
freispiele kaufen slots online echtgeld
Take a look at my website früchte Spielautomaten mit paypal
why do you never split 10s in blackjack · June 28, 2026 at 9:09 pm
prepaid visa for online gambling uk, poker site usa and what poker sites are legal why do you never split 10s in blackjack
australia, or quatro casino united states
online roulette spielen mit echtgeld · June 28, 2026 at 9:21 pm
online roulette spielen mit echtgeld roulette mit paysafecard
no deposit bonus ohne maximalen gewinn · June 28, 2026 at 10:33 pm
online casino 150 euro einzahlung paypal
my page :: no deposit bonus ohne maximalen gewinn
Are There Casinos In Tulum Mexico · June 28, 2026 at 11:06 pm
slots bonuses uk, golden tiger casino uk and online slots australia ipad,
or setting up an online casino usa
my webpage – Are There Casinos In Tulum Mexico
Gamble for real Money on android · June 28, 2026 at 11:15 pm
legitimate canadian online casinos, australian currency poker
chips and $5 deposit online casino canada, or top 10 australian online casino
Here is my homepage – Gamble for real Money on android
Elke · June 28, 2026 at 11:42 pm
best online play casino game free (Elke) bc
australia, best gambling websites usa and online pokies paysafe canada, or poker with real money usa
https://ediltagliaro.pierrepubblicita.it/ · June 28, 2026 at 11:58 pm
roulette spiele 123
Also visit my blog; seriöses casino direkte Auszahlung; https://ediltagliaro.pierrepubblicita.it/,
Burton · June 29, 2026 at 12:17 am
how much is a gambling license in canada, new zealandn online real money poker sites and how to cheat pokie machines canada, or new uk paypal casino bonus 300 prozent – Burton –
echtgeld bonus mit einzahlung · June 29, 2026 at 12:54 am
casino echtgeld bonus mit einzahlung ersteinzahlung
https://Jannedoma.cz/ · June 29, 2026 at 1:15 am
online casino mit eps bezahlen
Feel free to surf to my blog post; an spielautomaten gewinnen (https://Jannedoma.cz/)
Lindsey · June 29, 2026 at 1:41 am
triple shot pokies united states, blackjack mulligan uk and ontario australia online gambling,
or usa fallsview casino spa reviews [Lindsey] no deposit bonus
Graton Casino Cabana · June 29, 2026 at 1:49 am
all united statesn bingo, gala bingo gift
vouchers uk and hausaos dojo slot online real money no deposit bonus, or online Graton Casino Cabana real money free spins canada
Saarland casino · June 29, 2026 at 2:11 am
echtgeld bonus sofort erhältlich
Also visit my site … Saarland casino
Ilene · June 29, 2026 at 2:46 am
are pokies open in new zealand, best online pokies in canada and free bingo australia, or
australian online casino no deposit signup bonus
My homepage blackjack hole card mirror (Ilene)
Grace · June 29, 2026 at 3:27 am
no deposit bonus codes usa, free top online casino australia 2021; Grace, pokies no
downloads usa and united statesn no deposit casino bonus codes, or free
50 pokies canada
spielcasinos Frankreich · June 29, 2026 at 6:22 am
willkommensbonus automatisch
my homepage :: spielcasinos Frankreich
Ruben · June 29, 2026 at 8:00 am
casino mit vpn [Ruben] mit 25 euro einzahlung
Louise · June 29, 2026 at 8:03 am
united statesn slot machine emulator, how much top online
pokies and casinos australian coins and united statesn real pokies online, or casino
no deposit bonus codes 2021 united states
Here is my blog post; journal of gambling studies abbreviation [Louise]
Online Slots Mit Paypal · June 29, 2026 at 8:34 am
tischspiele Online Slots Mit Paypal paypal
Corrine · June 29, 2026 at 9:21 am
the top online pokies and casinos in united states 60fps, difference between european roulette and united kingdom and roulette australia
rules, or casino pay by mobile usa
My webpage: gambling control authority, Corrine,
fire rock navajo casino gallup nm · June 29, 2026 at 10:12 am
united kingdom poker deluxe 2, united kingdom gambling
rules and is top online pokies and casinos in australia same, or fire rock navajo casino gallup nm united states age
Timmy · June 29, 2026 at 10:33 am
top australian online pokies, united statesn online casino win real money and casino frenzy 250 free spins, or free 10
no deposit casino uk
Look into my page; bingo games for kids- rules (Timmy)
binance referral · June 29, 2026 at 10:42 am
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
roulette Wheel android App · June 29, 2026 at 11:08 am
no deposit bonus casinos canada, casino coquitlam bc united
kingdom and online casino uk free bonus no deposit, or australian online casino no
deposit signup bonus
Also visit my blog post roulette Wheel android App
Brenton · June 29, 2026 at 11:35 am
bestes online casino mit geld spielen – Brenton – glücksspiel
casino paysafecard nrw · June 29, 2026 at 11:37 am
casino paysafecard nrw mit 1000 euro maximaleinsatz
Velva · June 29, 2026 at 11:43 am
casino winnings tax free in united states, win real money online instantly usa and td australia visa debit
gambling, or united kingdom no deposit casino cash pull tabs – Velva – bonuses
https://bostonspacattery.co.Uk · June 29, 2026 at 11:47 am
remote gambling usa license, usa new online casino and free
spins no deposit bonus codes canada, or free online poker machine games
united kingdom
my page – giant craps table [https://bostonspacattery.co.Uk]
https://grafikaweb.exone-web.pl/formularz/2026/05/18/free-spins-deposit-10-uk/ · June 29, 2026 at 2:40 pm
casino in british columbia united kingdom, free money online casino canada and australian problem gambling statistics, or online casino real money free spins canada
Check out my page … mackie onyx blackjack vs
focusrite scarlett 2i2 (https://grafikaweb.exone-web.pl/formularz/2026/05/18/free-spins-deposit-10-uk/)
how to earn Money online in india by playing games · June 29, 2026 at 3:08 pm
online gambling sites in the usa, real how to earn Money online in india by playing games united statesn pokies and
united statesn pokies companies, or online gambling websites usa
marge simpson gambling episode · June 29, 2026 at 3:58 pm
auto wheel roulette play usa online, new zealandn online casino sign up no deposit bonus and what is the most trusted
online casino in united states, or australian open marge simpson gambling episode
Quyen · June 29, 2026 at 4:18 pm
biggest usa gambling sites, free deposit casino uk and new zealandn free
slots no download, or united statesn casinos in california
Stop by my webpage – blackjack processing plant (Quyen)
seriöses online casino mecklenburg-vorpommern · June 29, 2026 at 4:22 pm
seriöses online casino mecklenburg-vorpommern
20 euro jeton
James · June 29, 2026 at 5:16 pm
online casino real money no deposit australia,
uptown pokies no deposit bonus 2021 united states and crusader lvl
1 gambling, or online uk casino woth 24 hours payout
Here is my web page: bingo love meter (James)
Lillie · June 29, 2026 at 6:08 pm
yukon gold pala casino entertainment director – Lillie, legit,
gousaos quest free spins no deposit and online casino australia free spins sign up, or
bet online casino uk
Jeramy · June 29, 2026 at 6:43 pm
casinos in windsor canada, slot machines united states for sale and united kingdom pokies no
deposit bonus, or united kingdom civil war poker tables
my web-site is 50 50 raffle gambling; Jeramy,
online live Casino kreditkarte Bezahlen · June 29, 2026 at 7:28 pm
beste roulette flexepin
Feel free to surf to my website online live Casino kreditkarte Bezahlen
inkspireinternationalpublishers.com · June 29, 2026 at 7:59 pm
Blackjack bis 500 euro einsatz (inkspireinternationalpublishers.com) mit echtgeld
roulette ohne Oasis · June 29, 2026 at 9:11 pm
casino mindesteinzahlung 1 euro handyrechnung
Here is my blog … roulette ohne Oasis
sport live Wetten · June 30, 2026 at 8:36 am
wettanbieter sport live Wetten wetten
neue sportwetten anbieter · June 30, 2026 at 8:38 am
besten wetten apps
Here is my web-site – neue sportwetten anbieter
beste wettseiten österreich · June 30, 2026 at 9:20 am
wetten quote berechnen
Here is my webpage: beste wettseiten österreich
https://Masstech.Aacook.co/2025/10/06/online-wetten-groter-bonus/ · June 30, 2026 at 10:55 am
wetten online paypal
Feel free to visit my page: wettbüro augsburg (https://Masstech.Aacook.co/2025/10/06/online-wetten-groter-bonus/)
casino mindesteinzahlung 1 euro cashtocode · June 30, 2026 at 11:16 am
casino mindesteinzahlung 1 euro cashtocode bonus geld auszahlen
casino ohne maximaleinsatz mit bonus · June 30, 2026 at 11:38 am
casino ohne maximaleinsatz mit bonus bonus ohne einzahlung nach registrierung gratis
Bester Wettanbieter mit Bonus · June 30, 2026 at 11:41 am
quoten rechner wetten
Also visit my web blog; Bester Wettanbieter mit Bonus
https://Timefreedomwithmel.com/bez-rubriki/buchmacher-software/ · June 30, 2026 at 11:41 am
wettprognosen heute
my website – lizenz sportwetten deutschland (https://Timefreedomwithmel.com/bez-rubriki/buchmacher-software/)
25 euro einzahlen 75 Euro Spielen · June 30, 2026 at 7:46 pm
20 25 euro einzahlen 75 Euro Spielen ohne einzahlung casino
beste Spielautomaten Paysafecard · June 30, 2026 at 7:47 pm
persönliche permanenz roulette
Review my web-site – beste Spielautomaten Paysafecard
online Roulette apple pay Bezahlen · June 30, 2026 at 10:17 pm
sicheres casinos mit hoher bonus
Take a look at my site … online Roulette apple pay Bezahlen
https://Yduochanoi.vn/Mobiles-casino-mit-10-bonus-ohne-einzahlung-Im-jahr-2026-Entdecken/ · June 30, 2026 at 11:37 pm
online casino 10 euro muchbetter
Also visit my page: slots mit flexepin bezahlen; https://Yduochanoi.vn/Mobiles-casino-mit-10-bonus-ohne-einzahlung-Im-jahr-2026-Entdecken/,
Meagan · June 30, 2026 at 11:44 pm
seriöses online live casino flexepin bezahlen (Meagan)
sachsen
spielotheken mecklenburg vorpommern · July 1, 2026 at 1:55 am
online casino klarna schnelle auszahlung
Review my website – spielotheken mecklenburg vorpommern
Anitra · July 1, 2026 at 1:55 am
sicheres casinos mit klarna
Feel free to surf to my blog – bester casino bonusgeld [Anitra]
glücksspielrechtliche erlaubnis Nrw · July 1, 2026 at 3:53 am
realtime casino bonus ohne einzahlung
my website :: glücksspielrechtliche erlaubnis Nrw
https://lightseagreen-rook-598408.hostingersite.com · July 1, 2026 at 4:01 am
casino 10 euro flexepin (https://lightseagreen-rook-598408.hostingersite.com) app mit
geringer einzahlung
Sofort rückzahlung online casino · July 1, 2026 at 6:06 am
Sofort rückzahlung online casino 15 euro einzahlen 75 euro spielen
wo kann man noch online live roulette spielen · July 1, 2026 at 6:53 am
bonus kaufen slots mit bonus
my homepage: wo kann man noch online live roulette spielen
online Sportwetten in deutschland · July 1, 2026 at 6:55 am
wetten online Sportwetten in deutschland
japan
Ayushpureherbs.Com · July 1, 2026 at 7:03 am
casino trustly ab 10 euro
My web blog Slots Mit Expanding Wilds [Ayushpureherbs.Com]
wettbasis gratiswetten Category · July 1, 2026 at 7:30 am
wetten in deutschland
my web page: wettbasis gratiswetten Category
welche sportwetten anbieter gibt es · July 1, 2026 at 8:07 am
welche sportwetten anbieter gibt es tipps kostenlos
die besten buchmacher · July 1, 2026 at 8:39 am
wetten bonus
Also visit my page; die besten buchmacher
Casino monatsbonus · July 1, 2026 at 9:19 am
Casino monatsbonus 2 euro einzahlung cashlib
wettquoten · July 1, 2026 at 9:23 am
online-wetten
my website wettquoten
Daryl · July 1, 2026 at 9:26 am
legales online casino hessen, Daryl,
casino mit 400 euro bonus
Jeannette · July 1, 2026 at 10:27 am
live dealer spiele freispiele
my webpage online casino 175% willkommensbonus – Jeannette,
Jacinto · July 1, 2026 at 10:34 am
casino bonus per handyrechnung
my homepage … online progressive jackpots echtgeld (Jacinto)
https://Www.Catalocatering.com · July 1, 2026 at 10:51 am
slots ventura login ohne anzahlung bonuscodes
Here is my web-site :: willkommensbonus mit einzahlung (https://Www.Catalocatering.com)
eurovision wetten deutschland · July 1, 2026 at 11:22 am
was bedeutet handicap beim eurovision wetten deutschland
mediumslateblue-skunk-300497.hostingersite.com · July 1, 2026 at 1:15 pm
virtuelles casino 20 euro höChster bonus casino deutschland (mediumslateblue-skunk-300497.hostingersite.com) ohne einzahlung
https://poucomais.com/casino-gewinne-Auf-Deutsch-erklart-2026/ · July 1, 2026 at 1:53 pm
online casino ab 30 euro skrill (https://poucomais.com/casino-gewinne-Auf-Deutsch-erklart-2026/) live
casino schnelle auszahlung
https://enigma.ci/zertifiziertes-slots-ohne-anmeldung-spielen-2026/ · July 1, 2026 at 2:32 pm
online casino neue casinos mit ohne verifizierung (https://enigma.ci/zertifiziertes-slots-ohne-anmeldung-spielen-2026/) automaten
casino freispiele Sofortüberweisung · July 1, 2026 at 2:52 pm
online casino freispiele Sofortüberweisung ab 300
euro einzahlung
Brodie · July 1, 2026 at 4:29 pm
live casino 30 euro einzahlung cashtocode (Brodie) neosurf
Online Casino Ohne Umsatzbedingungen Klarna · July 1, 2026 at 5:02 pm
Online Casino Ohne Umsatzbedingungen Klarna casino 1 euro trustly
wie oft gewinnt man im casino · July 1, 2026 at 5:30 pm
realtime wie oft gewinnt man im casino bonus ohne einzahlung
Kostenlose Casino spiele spielen · July 1, 2026 at 5:45 pm
die spielbank online Kostenlose Casino spiele spielen no deposit bonus
online live casino Mastercard bezahlen · July 1, 2026 at 6:04 pm
deutsche online live casino Mastercard bezahlen casinos mit roulette
online casino ab 4 Euro giropay · July 1, 2026 at 6:39 pm
roulette gewinn möglichkeiten
my web blog online casino ab 4 Euro giropay
online casino 1 Euro Flexepin · July 1, 2026 at 7:48 pm
online casino 1 Euro Flexepin mit 150 prozent bonus
casino 250% Einzahlungsbonus · July 1, 2026 at 10:19 pm
live casino 250% Einzahlungsbonus eps auszahlung
seriöse roulette online casinos · July 1, 2026 at 10:54 pm
casino mindesteinzahlung 50 euro google pay
My webpage: seriöse roulette online casinos
casino ohne wartezeit echtgeld · July 2, 2026 at 12:17 am
crash casino ohne wartezeit echtgeld echtgeld
Beliebte Slots · July 2, 2026 at 12:19 am
online casino bonuscodes
Feel free to visit my blog; Beliebte Slots
casino 100 euro neosurf · July 2, 2026 at 12:24 am
beste online slot spiele
Look at my homepage … casino 100 euro neosurf
online casino mit telefon auszahlung · July 2, 2026 at 12:33 am
online casino mit telefon auszahlung
50 euro lastschrift
Astrid · July 2, 2026 at 2:51 am
175 bonus casino mindesteinzahlung 10 euro revolut (Astrid)
casino 125% Einzahlungsbonus · July 2, 2026 at 2:58 am
casino 125% Einzahlungsbonus
50 einzahlen 100 spielen
roulette App ohne geld · July 2, 2026 at 3:07 am
roulette App ohne geld gewinnen strategie
casinos ohne 1 Euro limit · July 2, 2026 at 3:58 am
blackjack echtgeld klarna
Feel free to visit my web blog … casinos ohne 1 Euro limit
ubytovanikv.cz · July 2, 2026 at 4:05 am
crash legales casino seiten (ubytovanikv.cz) hohe gewinne
Lowell · July 2, 2026 at 4:16 am
online casino mit crash spiele – Lowell – freispiele ohne
maximalgewinn
Live Dealer Online Echtgeld · July 2, 2026 at 4:23 am
romme Live Dealer Online Echtgeld spielen
Thomas · July 2, 2026 at 5:48 am
wow vegas online casino ohne anzahlung bonuscodes – Thomas
– casino 30 euro handyrechnung
casino mit 100 euro Einsatz · July 2, 2026 at 7:22 am
online spielothek casino mit 100 euro Einsatz
handy bezahlen
https://Residencialcossis.com · July 2, 2026 at 7:33 am
5 walzen slots online Blackjack mit ethereum; https://Residencialcossis.com,
April · July 2, 2026 at 7:34 am
online bester casino treue bonus (April) ohne verifizierung
mit paysafecard
online casino 500 euro einzahlung bitcoin · July 2, 2026 at 8:47 am
früchte spielautomaten um geld spielen
Also visit my web site … online casino 500 euro einzahlung bitcoin
seriöse casinos ohne mindesteinsatz · July 2, 2026 at 8:56 am
online spielautomaten sofortüberweisung bezahlen
my web site … seriöse casinos ohne mindesteinsatz
casino höhr grenzhausen · July 2, 2026 at 9:35 am
casino höhr grenzhausen 2 euro einzahlung giropay
casino ohne verifizierung jeton · July 2, 2026 at 9:37 am
online slots ab 20 cent einsatz
My blog post: casino ohne verifizierung jeton
Online Casino Mit Jeton · July 2, 2026 at 9:56 am
Online Casino Mit Jeton
casino ab 4 euro cashtocode
wettbüro bonn · July 2, 2026 at 10:15 am
beste quoten sportwetten
Look at my website … wettbüro bonn
casino bonus per Neteller · July 2, 2026 at 10:56 am
online casino bonus per Neteller skrill einzahlung
ohne anmeldung
Melina · July 2, 2026 at 11:18 am
online casino 100 euro giropay (Melina) slots ohne 5
sekunden
Aristocrat Spielautomaten · July 2, 2026 at 12:17 pm
online casino ohne ausweis paypal
Visit my web blog … Aristocrat Spielautomaten
online casino trustly einzahlung ohne anmeldung · July 2, 2026 at 12:19 pm
bestes slot spiel android
My blog post – online casino trustly einzahlung ohne anmeldung
online casinos die paypal akzeptieren · July 2, 2026 at 12:46 pm
slots mit jeton bezahlen
Here is my web site online casinos die paypal akzeptieren
survey.Ceoguard.de · July 2, 2026 at 1:06 pm
casino bonus rheinland-pfalz
Here is my blog post; blackjack ohne einzahlung (survey.Ceoguard.de)
https://Visitanzi.it/online-casino-mit-besten-bonus-ohne-einzahlung-2026/ · July 2, 2026 at 1:19 pm
online casino auszahlung auf giropay (https://Visitanzi.it/online-casino-mit-besten-bonus-ohne-einzahlung-2026/)
ab 2 euro eps
blackjack bis 20 Euro einsatz · July 2, 2026 at 1:22 pm
blackjack bis 20 Euro einsatz bank vorteil
Casino Spiele Lernen · July 2, 2026 at 1:24 pm
Casino Spiele Lernen sofort spielen ohne warten
casino mit 300 Euro einzahlung handyrechnung · July 2, 2026 at 2:15 pm
online casino mit 300 Euro einzahlung handyrechnung
ohne spinstopp
beste slots über 98 prozent rtp · July 2, 2026 at 2:37 pm
beste slots über 98 prozent rtp casino bonus ohne einzahlung
casino mit 25 Euro einzahlung · July 2, 2026 at 3:12 pm
online spielautomaten beste auszahlungsquote
Also visit my web-site: casino mit 25 Euro einzahlung
Slots Mit Freispiele Kaufen · July 2, 2026 at 4:54 pm
casino ohne verifizierung kreditkarte
Feel free to visit my web blog … Slots Mit Freispiele Kaufen
casino mit Trustly · July 2, 2026 at 6:10 pm
freespins aktuell
Feel free to surf to my web site :: casino mit Trustly
Claire · July 2, 2026 at 6:13 pm
online casino 50 euro google pay (Claire) mit video spielautomaten
Iona · July 2, 2026 at 7:22 pm
muchbetter casino seriös (Iona) ohne autoplay
sperre erfahrungen
http://shop2.chuukr.cafe24.com/member/login.html?noMemberOrder=&returnUrl=https://de.trustpilot.com/review/truehustlerz.de · July 2, 2026 at 7:43 pm
References:
Classy coin casino http://shop2.chuukr.cafe24.com/member/login.html?noMemberOrder=&returnUrl=https%3a%2f%2fde.trustpilot.com%2Freview%2Ftruehustlerz.de
References:
http://shop2.chuukr.cafe24.com/member/login.html?noMemberOrder=&returnUrl=https%3a%2f%2fde.trustpilot.com%2Freview%2Ftruehustlerz.de
https://legal-dictionary.thefreedictionary.com/ · July 2, 2026 at 8:43 pm
References:
Victoria casino london https://legal-dictionary.thefreedictionary.com/_/cite.aspx?url=https%3A%2F%2Fde.trustpilot.com%2Freview%2Ftruehustlerz.de&word=consent&sources=weal,law,hcLaw,bouvier_/cite.aspx?url=https%3A%2F%2Fde.trustpilot.com%2Freview%2Ftruehustlerz.de&word=consent&sources=weal,law,hcLaw,bouvier
https://4gameforum.com/proxy.php?link=https://de.trustpilot.com/review/truehustlerz.de · July 2, 2026 at 9:23 pm
References:
Canadian gaming summit https://4gameforum.com/proxy.php?link=https://de.trustpilot.com/review/truehustlerz.de
https://www.michael-smirnov.ru · July 3, 2026 at 2:16 am
References:
Casino circus https://www.michael-smirnov.ru/Get_RSS.php?pRSSurl=http%3a%2f%2fde.trustpilot.com%2Freview%2Ftruehustlerz.de/Get_RSS.php?pRSSurl=http%3a%2f%2fde.trustpilot.com%2Freview%2Ftruehustlerz.de
neue online casinos Nrw · July 3, 2026 at 12:51 pm
casino 30 euro einzahlen bonus
My blog post … neue online casinos Nrw
Online Casino Ab 25 Euro Cashlib · July 3, 2026 at 12:53 pm
Online Casino Ab 25 Euro Cashlib casino ab 25 euro paysafecard
Hohe VolatilitäT Casino · July 3, 2026 at 1:40 pm
seriöses online blackjack
My web site :: Hohe VolatilitäT Casino
Spielautomaten giropay Auszahlung · July 3, 2026 at 3:18 pm
richtiges casino deutschland
Review my page … Spielautomaten giropay Auszahlung
casino 30 euro mastercard · July 3, 2026 at 6:23 pm
online casino 30 euro mastercard
bonus geld auszahlen
https://www.arnal-Sofocev.fr/2026/06/04/wie-Kann-man-ein-eu-konto-in-spielbanken-loschen/ · July 3, 2026 at 6:24 pm
roulette varianten
My blog post … ehrliche online slots (https://www.arnal-Sofocev.fr/2026/06/04/wie-Kann-man-ein-eu-konto-in-spielbanken-loschen/)
Www.Jordaoadvogados.com.br · July 3, 2026 at 8:22 pm
gewinne beim roulette
Check out my blog post – casino 10 einzahlen 50 spielen (http://Www.Jordaoadvogados.com.br)
beste blackjack Trustly · July 3, 2026 at 8:56 pm
sofortgewinn spiele mit paypal
My web-site beste blackjack Trustly
online Casino für Baden-württemberg · July 4, 2026 at 12:33 am
online Casino für Baden-württemberg 4 euro einzahlen 8 euro spielen
casino Mit Echtgeld bonus Ohne einzahlung · July 4, 2026 at 12:38 am
online roulette telefon
My web site casino Mit Echtgeld bonus Ohne einzahlung
https://Parejaslatin.Csbnews.org/gibt-es-im-jahr-2026-spielbanken-die-paypal-lastschrift-anbieten/ · July 4, 2026 at 1:56 am
online casino mit vodafone bezahlen
Also visit my web site :: klassische slots echtgeld – https://Parejaslatin.Csbnews.org/gibt-es-im-jahr-2026-spielbanken-die-paypal-lastschrift-anbieten/ –
casino auszahlung auf cashtocode · July 4, 2026 at 2:06 am
50 freispiele online ohne einzahlung
My web page casino auszahlung auf cashtocode
Casino 5 Euro Einzahlen 100 Freispiele · July 4, 2026 at 3:35 am
android blackjack app deutsch
Stop by my website: Casino 5 Euro Einzahlen 100 Freispiele
Http://Www.Groupmg.Cl/Zertifiziertes-Slots-Verantwortliches-Spielen/ · July 4, 2026 at 3:42 am
Online Casino Mit 3 Euro Startguthaben – http://Www.Groupmg.Cl/Zertifiziertes-Slots-Verantwortliches-Spielen/, mit 50 prozent bonus
https://repolis.bg.polsl.pl/ · July 4, 2026 at 4:54 am
References:
List of las vegas casinos https://repolis.bg.polsl.pl/dlibra/login?refUrl=aHR0cHM6Ly9hcGkuZm9sbG93Lml0L3JlZGlyZWN0LXRvLXVybD9xPWh0dHBzJTNBJTJGJTJGZGUudHJ1c3RwaWxvdC5jb20vcmV2aWV3L293b3dlYXIuZGU
References:
https://repolis.bg.polsl.pl/dlibra/login?refUrl=aHR0cHM6Ly9hcGkuZm9sbG93Lml0L3JlZGlyZWN0LXRvLXVybD9xPWh0dHBzJTNBJTJGJTJGZGUudHJ1c3RwaWxvdC5jb20vcmV2aWV3L293b3dlYXIuZGU
Lonna · July 4, 2026 at 5:28 am
casino top 20 deutschland
Also visit my homepage bingo um echtes geld spielen (Lonna)
online casino ab 30 euro cashlib · July 4, 2026 at 5:48 am
online casino ab 30 euro cashlib 5 euro einzahlung
cashtocode
Gute Online Casino Slots · July 4, 2026 at 6:18 am
Gute Online Casino Slots
30 euro einzahlung litecoin
Casino 20 Euro Einzahlen 30 freispiele · July 4, 2026 at 7:03 am
online Casino 20 Euro Einzahlen 30 freispiele mit niedrigem einsatz ab 2 cent
https://thermosolar.hu · July 4, 2026 at 9:01 am
casino mit 50 prozent bonus
Feel free to surf to my web site … spielautomaten ethereum auszahlung (https://thermosolar.hu)
casino automat gewinnen · July 4, 2026 at 9:10 am
höchster bonus casino automat gewinnen deutschland
Die Spielbank Casino · July 4, 2026 at 10:39 am
online Die Spielbank Casino 4 euro einzahlung
paypal
Online spielautomaten hamburg · July 4, 2026 at 10:39 am
keno mit hoher auszahlung
Feel free to surf to my webpage: Online spielautomaten hamburg
casino strategie · July 4, 2026 at 10:51 am
online casino strategie perfect money
bezahlen
Casino 3 Euro Giropay · July 4, 2026 at 11:27 am
online slots bester rtp
Here is my page … Casino 3 Euro Giropay
Lelia · July 4, 2026 at 11:32 am
eps casino seriös (Lelia) handyrechnung ab 20
euro
https://Precisionfs.com/ · July 4, 2026 at 2:06 pm
casino ohne verifizierung cashtocode
Here is my web page: xxxtreme lightning roulette
bonus (https://Precisionfs.com/)
die 10 besten online casinos · July 4, 2026 at 2:25 pm
bester casino freitagsbonus
Here is my webpage … die 10 besten online casinos
Scratch Cards Mit Hoher Auszahlung · July 4, 2026 at 2:41 pm
online casino 1 euro einzahlung sofortüberweisung
Here is my web page – Scratch Cards Mit Hoher Auszahlung
avtomobilistam.ru · July 4, 2026 at 2:42 pm
References:
Casino classic https://www.https://www.avtomobilistam.ru:443/redir.php?go=https://bbs.pku.edu.cn/v2/jump-to.php?url=https://de.trustpilot.com/review/owowear.de:443/redir.php?go=https://bbs.pku.edu.cn/v2/jump-to.php?url=https://de.trustpilot.com/review/owowear.de
https://30.cholteth.com/index/d1?diff=0&utm_source=ogdd&utm_campaign=26607&utm_content=&utm_clickid=g00w000go8sgcg0k&aurl=https://www.google.com.sg/url?q=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 3:18 pm
References:
Slot machines online https://30.cholteth.com/index/d1?diff=0&utm_source=ogdd&utm_campaign=26607&utm_content=&utm_clickid=g00w000go8sgcg0k&aurl=https://www.google.com.sg/url?q=https://de.trustpilot.com/review/owowear.de
https://www2.hu-berlin.de/hu/collaboration/project-contact.php?ref=http://shop2.parisyang.cafe24.com/member/login.html?returnUrl=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 3:23 pm
References:
Play slot machine https://www2.hu-berlin.de/hu/collaboration/project-contact.php?ref=http://shop2.parisyang.cafe24.com/member/login.html?returnUrl=https://de.trustpilot.com/review/owowear.de
come.ac · July 4, 2026 at 3:33 pm
References:
Schecter blackjack atx c 7 https://https://come.ac/new-york-casino-las-vegas-89007/new-york-casino-las-vegas-89007
https://syclub24.ru · July 4, 2026 at 4:08 pm
References:
Century casino cripple creek https://syclub24.ru/proxy.php?link=https://empyriononline.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de/proxy.php?link=https://empyriononline.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de
https://szsa.ru · July 4, 2026 at 4:20 pm
References:
Blackjack clothing https://szsa.ru/bitrix/rk.php?goto=https://www.allods.net/redirect/de.trustpilot.com%2Freview%2Fowowear.de//bitrix/rk.php?goto=https://www.allods.net/redirect/de.trustpilot.com%2Freview%2Fowowear.de/
online Casino ab 50 euro mastercard · July 4, 2026 at 5:03 pm
crypto online Casino ab 50 euro mastercard einzahlungsbonus
http://shop2.chuukr.cafe24.com/member/login.html?noMemberOrder=&returnUrl=https://scienceplus.abes.fr/describe/?url=http://de.trustpilot.com/review/owowear.de · July 4, 2026 at 5:12 pm
References:
Hollywood casino toledo ohio http://shop2.chuukr.cafe24.com/member/login.html?noMemberOrder=&returnUrl=https%3a%2f%2fscienceplus.abes.fr%2Fdescribe%2F%3Furl%3Dhttp%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
http://shop2.chuukr.cafe24.com/member/login.html?noMemberOrder=&returnUrl=https%3a%2f%2fscienceplus.abes.fr%2Fdescribe%2F%3Furl%3Dhttp%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
https://bios-fix.com/proxy.php?link=https://alumni.skema.edu/global/redirect.php?url=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 5:19 pm
References:
Saratoga springs casino https://bios-fix.com/proxy.php?link=https://alumni.skema.edu/global/redirect.php?url=https://de.trustpilot.com/review/owowear.de
tulum.ru · July 4, 2026 at 6:31 pm
References:
Craps system https://https://tulum.ru/catalog/view/theme/quick-view.php?product_id=2702&product_href=http%3a%2f%2ftoolbarqueries.google.gp%2Furl%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/catalog/view/theme/quick-view.php?product_id=2702&product_href=http%3a%2f%2ftoolbarqueries.google.gp%2Furl%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
http://proxy.nowhereincoming.net · July 4, 2026 at 6:44 pm
References:
Casino listing http://proxy.nowhereincoming.net/index.php?q=aHR0cHM6Ly9lbXB5cmlvbm9ubGluZS5jb20vcHJveHkucGhwP2xpbms9aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ/index.php?q=aHR0cHM6Ly9lbXB5cmlvbm9ubGluZS5jb20vcHJveHkucGhwP2xpbms9aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ
http://ville.montreal.qc.ca/ · July 4, 2026 at 6:50 pm
References:
Vegas palms casino http://ville.montreal.qc.ca/portal/page?_dad=portal&_pageid=5798%2C43481603&_schema=PORTAL&id=9191&ret=http://forum.cmsheaven.org/proxy.php?link=https://de.trustpilot.com/review/owowear.de
References:
http://ville.montreal.qc.ca/portal/page?_dad=portal&_pageid=5798%2C43481603&_schema=PORTAL&id=9191&ret=http://forum.cmsheaven.org/proxy.php?link=https://de.trustpilot.com/review/owowear.de
https://freerepublic.com/ · July 4, 2026 at 6:57 pm
References:
Amelia belle casino https://freerepublic.com/~voyagesechellesluxe/index?U=https://jguitar.com/tabmap?url=https%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de~voyagesechellesluxe/index?U=https://jguitar.com/tabmap?url=https%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
https://truckymods.io · July 4, 2026 at 7:09 pm
References:
Vegas online casino https://truckymods.io/external-link?url=https://uz.goodinternet.org/uz/external-link/?next=https://de.trustpilot.com/review/owowear.de/external-link?url=https://uz.goodinternet.org/uz/external-link/?next=https://de.trustpilot.com/review/owowear.de
http://optimize.viglink.com/ · July 4, 2026 at 7:16 pm
References:
Crown europe casino http://optimize.viglink.com/page/pmv?url=https%3A//forumsad.ru%2Fproxy.php%3Flink%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
http://optimize.viglink.com/page/pmv?url=https%3A//forumsad.ru%2Fproxy.php%3Flink%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
gewinnstrategie roulette · July 4, 2026 at 7:22 pm
sector 777 casino ohne anzahlung bonus
Also visit my web site … gewinnstrategie roulette
longurl.eti.pw · July 4, 2026 at 7:40 pm
References:
Best casino games http://www.http://www.longurl.eti.pw/?url=https%3A%2F%2Fwww.google.ms%2Furl%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de</a/?url=https%3A%2F%2Fwww.google.ms%2Furl%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de</a
http://alt1.toolbarqueries.google.tk/ · July 4, 2026 at 7:54 pm
References:
Betfair casino http://alt1.toolbarqueries.google.tk/url?q=http://s2.xvatit.com/api.php?action=https://de.trustpilot.com/review/owowear.de
References:
http://alt1.toolbarqueries.google.tk/url?q=http://s2.xvatit.com/api.php?action=https://de.trustpilot.com/review/owowear.de
http://clients1.google.com.ai · July 4, 2026 at 8:10 pm
References:
Gulfstream casino http://clients1.google.com.ai/url?sa=t&url=http%3A%2F%2Futmagazine.ru%2Fr%3Furl%3Dhttp%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/url?sa=t&url=http%3A%2F%2Futmagazine.ru%2Fr%3Furl%3Dhttp%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
fishki.net · July 4, 2026 at 8:12 pm
References:
Best online game sites https://https://fishki.net/go/?url=https://www.google.ng/url?q=http%3A//de.trustpilot.com%2Freview%2Fowowear.de//go/?url=https://www.google.ng/url?q=http%3A//de.trustpilot.com%2Freview%2Fowowear.de/
hairyvaginapics.com · July 4, 2026 at 8:20 pm
References:
Casino 365 http://http://hairyvaginapics.com/fcj/out.php?s=50&url=http%3A%2F%2Fgrch37.ensembl.org%2FHelp%2FPermalink%3Furl%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/fcj/out.php?s=50&url=http%3A%2F%2Fgrch37.ensembl.org%2FHelp%2FPermalink%3Furl%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
skin-skin11--shop2.jjukbbang1.cafe24.com · July 4, 2026 at 8:29 pm
References:
San manuel casino http://http://skin-skin11–shop2.jjukbbang1.cafe24.com/member/login.html?returnUrl=https://empyriononline.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de/member/login.html?returnUrl=https://empyriononline.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de
Poker hoher Einsatz · July 4, 2026 at 8:35 pm
casino mit geld bonus ohne einzahlung
my site – Poker hoher Einsatz
http://saab.one/ · July 4, 2026 at 8:39 pm
References:
Sands casino bethlehem pa http://saab.one/proxy.php?link=http://vebiradoworid.school2100.com/bitrix/redirect.php?goto=https%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
http://saab.one/proxy.php?link=http://vebiradoworid.school2100.com/bitrix/redirect.php?goto=https%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
Mei · July 4, 2026 at 8:48 pm
online casino ab 4 euro klarna
Feel free to surf to my web blog – freispiele ohne einzahlung gamble (Mei)
http://images.google.com.om/url?q=https://www.gitaristam.ru/redir.php?go=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 8:56 pm
References:
Maryland casinos http://images.google.com.om/url?q=https://www.gitaristam.ru/redir.php?go=https://de.trustpilot.com/review/owowear.de
https://www.ironhidegames.com/ · July 4, 2026 at 9:04 pm
References:
Coconut creek casino https://www.ironhidegames.com/external?url=https://forum.reizastudios.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de
References:
https://www.ironhidegames.com/external?url=https://forum.reizastudios.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de
http://www.rojadirecta.eu/goto/forumsad.ru/proxy.php?link=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 9:07 pm
References:
Boulevard casino poker http://www.rojadirecta.eu/goto/forumsad.ru/proxy.php%3Flink%3Dhttps%3A//de.trustpilot.com/review/owowear.de
References:
http://www.rojadirecta.eu/goto/forumsad.ru/proxy.php%3Flink%3Dhttps%3A//de.trustpilot.com/review/owowear.de
Pestcontrolservicesnearme.ca · July 4, 2026 at 9:10 pm
sportwetten casino bonus
Feel free to visit my homepage … glücksspiel mit paypal
(Pestcontrolservicesnearme.ca)
Houseofgroovesblueridge.Com · July 4, 2026 at 9:12 pm
casino mit 1000 euro einzahlung paypal
My blog … Roulette Ohne Limit, Houseofgroovesblueridge.Com,
wiki.holzheizer-forum.de · July 4, 2026 at 9:19 pm
References:
Jupiter casino gold coast https://https://wiki.holzheizer-forum.de/api.php?action=https://www.eshko.by/redirect.php?url=https://de.trustpilot.com/review/owowear.de/api.php?action=https://www.eshko.by/redirect.php?url=https://de.trustpilot.com/review/owowear.de
http://marketplace.salisburypost.com/ · July 4, 2026 at 9:37 pm
References:
Harrah’s rincon casino http://marketplace.salisburypost.com/adhunter/salisburypost/home/emailfriend?url=http://www.degeneratov.net/proxy.php?link=https://de.trustpilot.com/review/owowear.de
References:
http://marketplace.salisburypost.com/adhunter/salisburypost/home/emailfriend?url=http://www.degeneratov.net/proxy.php?link=https://de.trustpilot.com/review/owowear.de
top 10 live casino seiten · July 4, 2026 at 9:52 pm
online top 10 live casino seiten 15 euro einzahlung kreditkarte
Charolette · July 4, 2026 at 9:53 pm
blackjack regels splitsen
My web page :: lightning box casino liste [Charolette]
https://forum-msk.info:443/proxy.php?link=http://images.google.de/url?q=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 10:07 pm
References:
Island casino https://forum-msk.info:443/proxy.php?link=http://images.google.de/url?q=https://de.trustpilot.com/review/owowear.de
darf man beim roulette auf die Null setzen · July 4, 2026 at 10:11 pm
jackpot slots app echtgeld
my homepage darf man beim roulette auf die Null setzen
https://www.web-pra.com/ · July 4, 2026 at 10:12 pm
References:
Harrah’s casino new orleans https://www.web-pra.com/home/externallink?url=https%3A%2F%2Fclients1.google.ms%2Furl%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/
References:
https://www.web-pra.com/home/externallink?url=https%3A%2F%2Fclients1.google.ms%2Furl%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/
Auto Roulette Casino · July 4, 2026 at 10:12 pm
Auto Roulette Casino neugablonz
http://cn.bing.com · July 4, 2026 at 10:19 pm
References:
Treasure bay casino http://cn.bing.com/news/apiclick.aspx?ref=FexRss&aid=&url=http://s0565755c.fastvps-server.com/api.php?action=https://de.trustpilot.com/review/owowear.de/news/apiclick.aspx?ref=FexRss&aid=&url=http://s0565755c.fastvps-server.com/api.php?action=https://de.trustpilot.com/review/owowear.de
live Casino casino bonus ohne einzahlung · July 4, 2026 at 10:20 pm
online spielautomaten kreditkarte bezahlen
Also visit my blog … live Casino casino bonus ohne einzahlung
https://mk.cs.msu.ru · July 4, 2026 at 10:31 pm
References:
Harrah’s casino new orleans https://mk.cs.msu.ru/api.php?action=http://it.rojadirecta.eu/goto/de.trustpilot.com/review/owowear.de/api.php?action=http://it.rojadirecta.eu/goto/de.trustpilot.com/review/owowear.de
http://images.google.co.in · July 4, 2026 at 10:32 pm
References:
No deposit required http://images.google.co.in/url?sa=t&url=http%3A%2F%2Fapi.follow.it%2Fredirect-to-url%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/url?sa=t&url=http%3A%2F%2Fapi.follow.it%2Fredirect-to-url%3Fq%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
http://rlu.ru/ · July 4, 2026 at 10:44 pm
References:
Cliff castle casino http://rlu.ru/5bdeE
References:
http://rlu.ru/5bdeE
http://www.google.com.nf/url?sa=t&url=https://chaturbate.com/external_link/?url=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 10:55 pm
References:
21 black jack online subtitulada http://www.google.com.nf/url?sa=t&url=https://chaturbate.com/external_link/?url=https://de.trustpilot.com/review/owowear.de
https://www.webmath.ru/forum/go.php?url=aHR0cDovL3NoZWxsLmNuZm9sLmNvbS9hZHNlbmNlL2dldF9pcC5waHA/dXJsPWh0dHBzOi8vZGUudHJ1c3RwaWxvdC5jb20vcmV2aWV3L293b3dlYXIuZGU · July 4, 2026 at 11:10 pm
References:
Latest casino bonus https://www.webmath.ru/forum/go.php?url=aHR0cDovL3NoZWxsLmNuZm9sLmNvbS9hZHNlbmNlL2dldF9pcC5waHA/dXJsPWh0dHBzOi8vZGUudHJ1c3RwaWxvdC5jb20vcmV2aWV3L293b3dlYXIuZGU
online casino ohne 5 sekunden Pause klarna · July 4, 2026 at 11:19 pm
online casino ohne 5 sekunden Pause klarna echtgeld hamburg
https://forums.techarp.com/ · July 4, 2026 at 11:25 pm
References:
Craps system https://forums.techarp.com/proxy.php?link=https://delta.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de
References:
https://forums.techarp.com/proxy.php?link=https://delta.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de
http://aintedles.yoo7.com/go/aHR0cDovL25hc2hpLXByb2d1bGtpLnJ1L2JpdHJpeC9yay5waHA/Z290bz1odHRwczovL2RlLnRydXN0cGlsb3QuY29tL3Jldmlldy9vd293ZWFyLmRl · July 4, 2026 at 11:36 pm
References:
Mobile slots http://aintedles.yoo7.com/go/aHR0cDovL25hc2hpLXByb2d1bGtpLnJ1L2JpdHJpeC9yay5waHA/Z290bz1odHRwczovL2RlLnRydXN0cGlsb3QuY29tL3Jldmlldy9vd293ZWFyLmRl
https://wiki.hetzner.de/api.php?action=http://images.google.by/url?q=https://de.trustpilot.com/review/owowear.de · July 4, 2026 at 11:36 pm
References:
Celine dion in las vegas https://wiki.hetzner.de/api.php?action=http://images.google.by/url?q=https://de.trustpilot.com/review/owowear.de
https://old.urso.ru/action.redirect/url/aHR0cDovL21hcHMuZ29vZ2xlLnJ1L3VybD9xPWh0dHBzOi8vZGUudHJ1c3RwaWxvdC5jb20vcmV2aWV3L293b3dlYXIuZGU · July 4, 2026 at 11:38 pm
References:
Lucky emperor casino https://old.urso.ru/action.redirect/url/aHR0cDovL21hcHMuZ29vZ2xlLnJ1L3VybD9xPWh0dHBzOi8vZGUudHJ1c3RwaWxvdC5jb20vcmV2aWV3L293b3dlYXIuZGU
tinhte.vn · July 4, 2026 at 11:41 pm
References:
3d roulette https://https://tinhte.vn/proxy.php?link=http://maps.google.vg/url?q=https://de.trustpilot.com/review/owowear.de/proxy.php?link=http://maps.google.vg/url?q=https://de.trustpilot.com/review/owowear.de
http://www.xcnews.ru/go.php?go=www.newhydro.ru/action.redirect/url/aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ · July 4, 2026 at 11:44 pm
References:
Cannery casino http://www.xcnews.ru/go.php?go=www.newhydro.ru/action.redirect/url/aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ
https://szsa.ru · July 4, 2026 at 11:53 pm
References:
Le st laurent portage https://szsa.ru/bitrix/rk.php?goto=https://ocprof.ru/action.redirect/url/aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ/bitrix/rk.php?goto=https://ocprof.ru/action.redirect/url/aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ
https://aktsh.ru · July 4, 2026 at 11:54 pm
References:
Oceans 11 casino https://aktsh.ru/go.php?url=http://www.dftgroupsvn.uniroma2.it/search?q=https://de.trustpilot.com/review/owowear.de/go.php?url=http://www.dftgroupsvn.uniroma2.it/search?q=https://de.trustpilot.com/review/owowear.de
https://metager.de/meta/settings?fokus=web&url=https://wiki.wargaming.net/api.php?action=https://de.trustpilot.com/review/owowear.de&* · July 5, 2026 at 12:02 am
References:
Valley view casino center seating chart https://metager.de/meta/settings?fokus=web&url=https%3A%2F%2Fwiki.wargaming.net%2Fapi.php%3Faction%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de%26%2A
References:
https://metager.de/meta/settings?fokus=web&url=https%3A%2F%2Fwiki.wargaming.net%2Fapi.php%3Faction%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de%26%2A
http://images.google.md · July 5, 2026 at 12:04 am
References:
Casino tropez mobile http://images.google.md/url?q=http://image.google.ge/url?q=https://de.trustpilot.com/review/owowear.de/url?q=http://image.google.ge/url?q=https://de.trustpilot.com/review/owowear.de
http://maps.google.tk/url?sa=t&url=https://digiex.net/proxy.php?link=https://de.trustpilot.com/review/owowear.de · July 5, 2026 at 12:09 am
References:
Wrest point casino http://maps.google.tk/url?sa=t&url=https://digiex.net/proxy.php?link=https://de.trustpilot.com/review/owowear.de
http://electrik.org/forum/redirect.php?url=https://login.littlejoys.ru/?redir=//de.trustpilot.com/review/owowear.de · July 5, 2026 at 12:11 am
References:
L’auberge casino baton rouge http://electrik.org/forum/redirect.php?url=https://login.littlejoys.ru/?redir=%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
http://electrik.org/forum/redirect.php?url=https://login.littlejoys.ru/?redir=%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
https://www.textise.net/ · July 5, 2026 at 12:13 am
References:
Real casino slots https://www.textise.net/showtext.aspx?strurl=http://skin-skin11–shop2.jjukbbang1.cafe24.com/member/login.html?returnUrl=https://de.trustpilot.com/review/owowear.de
References:
https://www.textise.net/showtext.aspx?strurl=http://skin-skin11–shop2.jjukbbang1.cafe24.com/member/login.html?returnUrl=https://de.trustpilot.com/review/owowear.de
https://tulum.ru/ · July 5, 2026 at 12:17 am
References:
Soaring eagle casino coupons https://tulum.ru/catalog/view/theme/quick-view.php?product_id=2702&product_href=http%3a%2f%2fnashi-progulki.ru%2Fbitrix%2Frk.php%3Fgoto%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
https://tulum.ru/catalog/view/theme/quick-view.php?product_id=2702&product_href=http%3a%2f%2fnashi-progulki.ru%2Fbitrix%2Frk.php%3Fgoto%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
preserve.lib.unb.ca · July 5, 2026 at 12:42 am
References:
King of prussia casino https://https://preserve.lib.unb.ca/wayback/20141205151334mp_/kakaku.com%2Fjump%2F%3Furl%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de//wayback/20141205151334mp_/kakaku.com%2Fjump%2F%3Furl%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/
https://web.gavekal.com · July 5, 2026 at 12:47 am
References:
Casino titan https://web.gavekal.com/redirection-disclaimer/?next=http://toolbarqueries.google.ms/url?q=https://de.trustpilot.com/review/owowear.de/redirection-disclaimer/?next=http://toolbarqueries.google.ms/url?q=https://de.trustpilot.com/review/owowear.de
live.warthunder.com · July 5, 2026 at 12:51 am
References:
Slot machine manufacturers https://https://live.warthunder.com/away/?to=https%3A%2F%2Fvideoregforum.ru%2Fproxy.php%3Flink%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de</a/away/?to=https%3A%2F%2Fvideoregforum.ru%2Fproxy.php%3Flink%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de</a
http://images.google.ms/ · July 5, 2026 at 1:25 am
References:
Slot games for pc http://images.google.ms/url?q=https://lynx.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de
References:
http://images.google.ms/url?q=https://lynx.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de
Https://Trc-Solutions.10Xwebsolutions.Com/Casino-Neukundenbonus-Ohne-Einzahlung-2026/ · July 5, 2026 at 1:26 am
casino mit 40 euro einzahlung handyrechnung
My web-site – Slot Machine Spielen, https://Trc-Solutions.10Xwebsolutions.Com/Casino-Neukundenbonus-Ohne-Einzahlung-2026/,
board-es.seafight.com · July 5, 2026 at 1:28 am
References:
Video poker online https://https://board-es.seafight.com/proxy.php?link=https://board-pl.seafight.com:443/proxy.php?link=https://de.trustpilot.com/review/owowear.de/proxy.php?link=https://board-pl.seafight.com:443/proxy.php?link=https://de.trustpilot.com/review/owowear.de
online slots muchbetter bezahlen · July 5, 2026 at 1:32 am
online slots muchbetter bezahlen casino
mit 50 euro startguthaben ohne einzahlung
board-pl.seafight.com · July 5, 2026 at 1:37 am
References:
Inter casino https://https://board-pl.seafight.com:443/proxy.php?link=http://cse.google.vg/url?q=https://de.trustpilot.com/review/owowear.de:443/proxy.php?link=http://cse.google.vg/url?q=https://de.trustpilot.com/review/owowear.de
alt1.toolbarqueries.google.com.nf · July 5, 2026 at 2:14 am
References:
Don johnson blackjack http://http://alt1.toolbarqueries.google.com.nf/url?q=https://www.boxingforum24.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de/url?q=https://www.boxingforum24.com/proxy.php?link=https://de.trustpilot.com/review/owowear.de
https://forum.xnxx.com/proxy.php?link=http://www.sinp.msu.ru/ru/ext_link?url=http://de.trustpilot.com/review/owowear.de · July 5, 2026 at 2:32 am
References:
Nostalgia casino https://forum.xnxx.com/proxy.php?link=http://www.sinp.msu.ru/ru/ext_link?url=http%3A%2F%2Fde.trustpilot.com/review/owowear.de
References:
https://forum.xnxx.com/proxy.php?link=http://www.sinp.msu.ru/ru/ext_link?url=http%3A%2F%2Fde.trustpilot.com/review/owowear.de
https://auth.acog.org/createaccount?returnUrl=https://wapcenter.yn.lt/load/index?url=de.trustpilot.com/review/owowear.de&authRequestId=7375b828-4944-4c92-9556-472b6c2cba85 · July 5, 2026 at 2:37 am
References:
Real vegas online casino https://auth.acog.org/createaccount?returnUrl=https%3A%2F%2Fwapcenter.yn.lt%2Fload%2Findex%3Furl%3Dde.trustpilot.com%2Freview%2Fowowear.de&authRequestId=7375b828-4944-4c92-9556-472b6c2cba85
References:
https://auth.acog.org/createaccount?returnUrl=https%3A%2F%2Fwapcenter.yn.lt%2Fload%2Findex%3Furl%3Dde.trustpilot.com%2Freview%2Fowowear.de&authRequestId=7375b828-4944-4c92-9556-472b6c2cba85
https://almanach.pte.hu/oktato/273?from=https://hydra.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de · July 5, 2026 at 2:43 am
References:
The lodge casino https://almanach.pte.hu/oktato/273?from=https://hydra.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de
1 euro einzahlen 40 freispiele · July 5, 2026 at 2:47 am
online casino mit 10 1 euro einzahlen 40 freispiele bonus
casino Online spielen bonus ohne einzahlung · July 5, 2026 at 2:48 am
blackjack casino Online spielen bonus ohne einzahlung einschränkung
http://maps.google.com.bh/url?q=https://israelbusinessguide.com/away.php?url=https://de.trustpilot.com/review/owowear.de · July 5, 2026 at 2:50 am
References:
Slot play http://maps.google.com.bh/url?q=https://israelbusinessguide.com/away.php?url=https://de.trustpilot.com/review/owowear.de
shopvuikhoe.vn · July 5, 2026 at 3:25 am
casino 2 euro einzahlung giropay
Look at my page – roulette auf Farbe setzen gewinn – shopvuikhoe.vn,
http://maps.google.ms/url?q=https://ore.spongepowered.org/linkout?remoteUrl=https://de.trustpilot.com/review/owowear.de · July 5, 2026 at 3:45 am
References:
Gila river casinos http://maps.google.ms/url?q=https://ore.spongepowered.org/linkout?remoteUrl=https://de.trustpilot.com/review/owowear.de
casino mit 25 euro einzahlung bitcoin · July 5, 2026 at 3:45 am
casino mit 25 euro einzahlung bitcoin bonus per bitcoin
https://board-en.piratestorm.com/proxy.php?link=https://ar.paltalk.com/linkcheck?url=https://de.trustpilot.com/review/owowear.de · July 5, 2026 at 3:48 am
References:
Sun vegas casino https://board-en.piratestorm.com/proxy.php?link=https://ar.paltalk.com/linkcheck?url=https://de.trustpilot.com/review/owowear.de
postjung.com · July 5, 2026 at 3:51 am
References:
Pci slots https://https://postjung.com/paycc/paypal-cancel.php?go=https%3A%2F%2Fwww.pixiv.net%2Fjump.php%3Fhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de</a/paycc/paypal-cancel.php?go=https%3A%2F%2Fwww.pixiv.net%2Fjump.php%3Fhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de</a
Slots Handyrechnung einzahlung · July 5, 2026 at 3:52 am
neue casinos mit startguthaben
Have a look at my web-site :: Slots Handyrechnung einzahlung
https://geodesist.ru/proxy.php?link=https://www.google.com.sg/url?q=http://de.trustpilot.com/review/owowear.de · July 5, 2026 at 4:27 am
References:
Blackjack guide https://geodesist.ru/proxy.php?link=https://www.google.com.sg/url?q=http%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
https://geodesist.ru/proxy.php?link=https://www.google.com.sg/url?q=http%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
casino Mindesteinzahlung 100 euro neosurf · July 5, 2026 at 4:30 am
wo ist das größte casino Mindesteinzahlung 100 euro neosurf der welt
Roulette mit klarna · July 5, 2026 at 4:53 am
casino bonus umsetzen
Feel free to visit my web page – Roulette mit klarna
WWW.Crystallinegaia.Com · July 5, 2026 at 7:27 am
Casino Sieger Auszahlung (http://WWW.Crystallinegaia.Com) mit 1 euro mindesteinzahlung
Casino Vellberg · July 5, 2026 at 10:15 am
online Casino Vellberg einsatzlimit
https://autospa.vijayantech.com · July 5, 2026 at 11:17 am
roulette farben zahlen
my web-site online casino mit startguthaben Ohne download (https://autospa.vijayantech.com)
Casino in memmingen · July 5, 2026 at 11:30 am
online Casino in memmingen 1 euro trustly
Casino 4 euro einzahlung neteller · July 5, 2026 at 2:55 pm
beste online casinos mit cashlib
Take a look at my blog post: Casino 4 euro einzahlung neteller
iharosgarage.hu · July 5, 2026 at 3:01 pm
live blackjack erfahrungen – iharosgarage.hu,
gewinnauszahlung
Tanisha · July 5, 2026 at 4:26 pm
spiele in einem casino
Here is my page spielbank mindesteinsatz
(Tanisha)
Casino Das Klarna Akzeptiert · July 5, 2026 at 4:33 pm
roulette brettspill
Feel free to surf to my blog post; Casino Das Klarna Akzeptiert
Jacelyn · July 5, 2026 at 5:16 pm
online casino ab 2 euro flexepin (Jacelyn)
casino ab 20 euro apple pay
online casino bonus Vergleich · July 5, 2026 at 5:18 pm
beste slots litecoin
my blog post … online casino bonus Vergleich
Roulette spielen lernen · July 5, 2026 at 5:23 pm
seriöses casino mecklenburg-vorpommern
My page: Roulette spielen lernen
Registrier bonus casino · July 5, 2026 at 7:49 pm
25 € registrierungsbonus Registrier bonus casino
Beste Blackjack App Iphone · July 5, 2026 at 8:12 pm
casino 10 euro einzahlen 20 euro bekommen
Take a look at my website; Beste Blackjack App Iphone
https://maweld.hu/gibt-es-eine-deutsche-auszahlungsmethode-beim-spielbanken-roulette/ · July 5, 2026 at 8:12 pm
neteller online casino deutschland (https://maweld.hu/gibt-es-eine-deutsche-auszahlungsmethode-beim-spielbanken-roulette/) ohne limit mit lastschrift
arc.Upgradelabs.pt · July 5, 2026 at 8:14 pm
bestes auszahlungscasino 2026
my web site Roulette spielen München (arc.Upgradelabs.pt)
АВА терапия · July 5, 2026 at 8:22 pm
ai testing and ai assurance
casino freispiele banküberweisung · July 5, 2026 at 9:14 pm
casino freispiele banküberweisung
80 freispiele bei anmeldung
Online Casino Mit Ohne Lugas · July 5, 2026 at 9:37 pm
slots ab 2 cent einsatz
Also visit my site … Online Casino Mit Ohne Lugas
Luciana · July 5, 2026 at 9:38 pm
automatenspiele casino banküberweisung schnelle auszahlung
(Luciana)
Margarette · July 5, 2026 at 10:11 pm
geld mit roulette 1 zahl gewinn [Margarette]
casino ohne Oasis Trustly · July 5, 2026 at 10:17 pm
legales online casino ohne Oasis Trustly brandenburg
Casino App nrw · July 5, 2026 at 11:12 pm
wie setze ich beim roulette richtig
my blog; Casino App nrw
Online casino einzahlungslimit · July 5, 2026 at 11:20 pm
Online casino einzahlungslimit
casino ab 300 euro
online slots Brandenburg · July 5, 2026 at 11:44 pm
online slots Brandenburg casino 4 euro cashtocode
Shantae · July 6, 2026 at 12:23 am
online casino ab 20 euro kreditkarte
Review my blog post: seriöse casinos mit ohne wartezeit (Shantae)
online casino 25 euro giropay · July 6, 2026 at 12:24 am
online casino 25 euro giropay ab 400 euro einzahlung
Online roulette mit revolut · July 6, 2026 at 1:27 am
echtgeld casino astropay
Here is my site :: Online roulette mit revolut
Connie · July 6, 2026 at 2:33 am
neue online casino bonus mit einzahlung – Connie – 777 willkommensbonus
Roulette Casino Freispiele · July 6, 2026 at 3:28 am
neue slots mit respin feature
Here is my site … Roulette Casino Freispiele
casino ohne 5 Sekunden Kryptowährung · July 6, 2026 at 4:15 am
rubbellose mit freispielen
Feel free to visit my homepage – casino ohne 5 Sekunden Kryptowährung
Live casino ohne 5 Sekunden · July 6, 2026 at 5:03 am
online spielautomaten mit revolut
Also visit my web page … Live casino ohne 5 Sekunden
live poker echtgeld · July 6, 2026 at 5:59 am
150 euro startguthaben ohne einzahlung
Feel free to visit my page :: live poker echtgeld
crash games app um echtes geld · July 6, 2026 at 7:12 am
professionelle roulette spieler
Also visit my site … crash games app um echtes geld
Online Blackjack Paypal Bezahlen · July 6, 2026 at 7:32 am
Online Blackjack Paypal Bezahlen live dealer um
geld
casino 1 euro einzahlen 3 euro spielen · July 6, 2026 at 7:50 am
casino 1 euro einzahlen 3 euro spielen mit handyrechnung deutschland
blackjack Zu zweit · July 6, 2026 at 8:24 am
50 freispiele bei anmeldung ohne einzahlung
Feel free to visit my site: blackjack Zu zweit
Jetta · July 6, 2026 at 8:39 am
casino bonus per neteller
My web page; neue casinos ohne mindesteinzahlung (Jetta)
https://Webshop.professionalcsali.hu · July 6, 2026 at 8:41 am
bestes casino erlebnis (https://Webshop.professionalcsali.hu) freispiele geschenkt
Slots Casino Paypal · July 6, 2026 at 9:17 am
beste mobile Slots Casino Paypal
ehrliche echtgeld casinos · July 6, 2026 at 9:36 am
wöchentlicher casino bonus
Feel free to surf to my web page; ehrliche echtgeld casinos
Online casino spiele schleswig holstein · July 6, 2026 at 9:41 am
automaten ohne einzahlung
Here is my homepage :: Online casino spiele schleswig holstein
Casino 4 euro Einzahlung Ethereum · July 6, 2026 at 10:42 am
neue online casinos mit apple pay
My web-site – Casino 4 euro Einzahlung Ethereum
Gray-Hyena-877620.Hostingersite.Com · July 6, 2026 at 11:24 am
Online Casino Ohne Maximaleinsatz Paypal, Gray-Hyena-877620.Hostingersite.Com, einzahlung per sofortüberweisung
Www.polocasrozpadu.Hys.cz · July 6, 2026 at 11:26 am
blackjack nach split
Also visit my web page … casino 20 Freispiele bei anmeldung [http://Www.polocasrozpadu.Hys.cz]
Casino mit einzahlungsbonus · July 6, 2026 at 11:35 am
bei welchem automatenspiel gewinnt man am meisten
My site … Casino mit einzahlungsbonus
https://Explorerboattrips.com/spielbanken-echtgeld-kostenlos-2026/ · July 6, 2026 at 12:14 pm
online double ball roulette casino [https://Explorerboattrips.com/spielbanken-echtgeld-kostenlos-2026/] mit crash spiele
20 free spins bei registrierung · July 6, 2026 at 12:38 pm
online live casino apple pay bezahlen
Feel free to surf to my site … 20 free spins bei registrierung
http://granillohq.Seedup.la/ · July 6, 2026 at 1:48 pm
online casino mit auszahlung ohne verifizierung
Also visit my page: blackjack auf Deutsch (http://granillohq.Seedup.la/)
online casino Geld wiederholen · July 6, 2026 at 5:40 pm
roulette online casino Geld wiederholen eps
https://innovativewidget.Com/ · July 6, 2026 at 5:58 pm
neue casinos mit sofort spielen
Check out my webpage … Online casino ab 1 euro einzahlung Sofortüberweisung (https://innovativewidget.Com/)
Casino paysafecard mindesteinzahlung · July 6, 2026 at 6:30 pm
beste casinos stuttgart
Here is my webpage – Casino paysafecard mindesteinzahlung
Major · July 6, 2026 at 8:17 pm
beim roulette immer gewinnen (Major) gewinn
maximieren
Rochelle · July 6, 2026 at 8:37 pm
casino apps mit paypal
Feel free to surf to my blog post :: neue fruit slots
– Rochelle,
VertrauenswüRdiges Online Casino · July 6, 2026 at 8:51 pm
beste tischspiele VertrauenswüRdiges Online Casino casinos
Https://nwscholarships.hu/beste-spielautomaten-ohne-mindestumsatz-2026/ · July 7, 2026 at 3:06 am
online casino 1 euro handyrechnung
my web page; jackpot slots mit paypal [https://nwscholarships.hu/beste-spielautomaten-ohne-mindestumsatz-2026/]
Eli · July 7, 2026 at 4:19 am
blackjack casino eps
Look into my homepage: online slots kryptowährung; Eli,
online casino ab 50 euro sofortüberweisung · July 7, 2026 at 5:01 am
online casino ab 50 euro sofortüberweisung casino auszahlung über muchbetter
https://Store.Alanatura.Co.id · July 7, 2026 at 5:13 am
das erste mal im casino – https://Store.Alanatura.Co.id – ethereum ab 3 euro
400 Casino Bonus Deutschland · July 7, 2026 at 7:04 am
400 Casino Bonus Deutschland paysafecard niedersachsen
blackjack bank muss ziehen · July 7, 2026 at 7:50 am
casino mindesteinzahlung 50 euro paypal
Review my web blog – blackjack bank muss ziehen
Neue Blackjack · July 7, 2026 at 8:58 am
casino cashtocode ab 10 euro
my web page – Neue Blackjack
https://scienceplus.abes.fr · July 7, 2026 at 11:42 am
References:
Stations casinos https://scienceplus.abes.fr/describe/?url=http%3A%2F%2Fforum.xnxx.com%2Fproxy.php%3Flink%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de/describe/?url=http%3A%2F%2Fforum.xnxx.com%2Fproxy.php%3Flink%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
Gretchen · July 7, 2026 at 11:55 am
mobile automaten casino mindesteinzahlung 4 euro ethereum – Gretchen –
Live Roulette Strategie · July 7, 2026 at 12:02 pm
online casino gewonnen
Feel free to surf to my page – Live Roulette Strategie
Alex · July 7, 2026 at 12:33 pm
casino torremar
my web blog – casinos en san sebastian el grande (Alex)
Quiero juegos de casinos · July 7, 2026 at 12:37 pm
asociación casino Quiero juegos de casinos tiana
https://zerocoolpro.biz/ · July 7, 2026 at 2:13 pm
References:
Ballys casino https://zerocoolpro.biz/forum/proxy.php?link=http://eng.stove.ru/action.redirect/url/aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ==
References:
https://zerocoolpro.biz/forum/proxy.php?link=http://eng.stove.ru/action.redirect/url/aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ==
casino 20 euros gratis sin depósito 2026 · July 7, 2026 at 3:00 pm
100 tiradas gratis casino 20 euros gratis sin depósito 2026
10 casinos Famosos · July 7, 2026 at 4:46 pm
casino talavera carta
My web site; 10 casinos Famosos
Sunny · July 7, 2026 at 4:53 pm
juegos de casino de palermo (Sunny) gratis de casino spartacus
online casino belgie 10 euro gratis · July 7, 2026 at 5:49 pm
online casino belgie 10 euro gratis dinero paypal
premios de La ruleta casino · July 7, 2026 at 6:04 pm
jugar a las tragamonedas premios de La ruleta casino casino
https://www.ukgovgrants.org/ · July 7, 2026 at 6:20 pm
bajar casino gratis tragamonedas, https://www.ukgovgrants.org/, roquetas de mar
https://metodoinfaliveldoano.Shop · July 7, 2026 at 7:00 pm
mejores maquinitas gratis casinos las mas
nuevas – https://metodoinfaliveldoano.Shop – online
en español
https://traflinks.com · July 7, 2026 at 7:23 pm
References:
Casino dice https://traflinks.com/panel/page_analizer/page_wordlib.php?morfology&url=https://chanceforward.chatovod.ru/away/?to=https://de.trustpilot.com/review/owowear.de/panel/page_analizer/page_wordlib.php?morfology&url=https://chanceforward.chatovod.ru/away/?to=https://de.trustpilot.com/review/owowear.de
m.animal.memozee.com · July 7, 2026 at 8:13 pm
References:
George thorogood http://http://m.animal.memozee.com/m.list.php?q=%3Ca%20href=%22https://frontier.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de/m.list.php?q=%3Ca%20href=%22https://frontier.astroempires.com/redirect.aspx?https://de.trustpilot.com/review/owowear.de
truckymods.io · July 7, 2026 at 9:32 pm
References:
Cherokee casino siloam springs https://https://truckymods.io/external-link?url=http://www.google.com.ai/url?q=https://de.trustpilot.com/review/owowear.de/external-link?url=http://www.google.com.ai/url?q=https://de.trustpilot.com/review/owowear.de
https://www.adminer.org/redirect/?sa=t&url=http://cmbe-console.worldoftanks.com/frame/?language=en&login_url=https://de.trustpilot.com/review/owowear.de · July 7, 2026 at 9:38 pm
References:
Aspinalls casino https://www.adminer.org/redirect/?sa=t&url=http%3A%2F%2Fcmbe-console.worldoftanks.com%2Fframe%2F%3Flanguage%3Den%26login_url%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
https://www.adminer.org/redirect/?sa=t&url=http%3A%2F%2Fcmbe-console.worldoftanks.com%2Fframe%2F%3Flanguage%3Den%26login_url%3Dhttps%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
https://da.gd/ · July 7, 2026 at 9:39 pm
References:
Fortune teller blackjack https://da.gd/riviera296
References:
https://da.gd/riviera296
Casino en villa dolores · July 7, 2026 at 9:44 pm
el faraon juego de Casino en villa dolores
Listado de casinos online en españa · July 7, 2026 at 10:08 pm
casino Listado de casinos online en españa apuesta real
Garland · July 7, 2026 at 10:30 pm
casinos descargar juego de ruleta de casino – Garland, apuestas
en bilbao
https://mt-travel.ru/ · July 7, 2026 at 11:55 pm
References:
Casino drive lagny https://mt-travel.ru/bitrix/rk.php?goto=https://soundingames.dei.uc.pt/api.php?action=https://de.trustpilot.com/review/owowear.de
References:
https://mt-travel.ru/bitrix/rk.php?goto=https://soundingames.dei.uc.pt/api.php?action=https://de.trustpilot.com/review/owowear.de
https://www.apkmirror.com/wp-content/themes/APKMirror/ap_resize/ap_resize.php?src=https://wbc1.wbc.poznan.pl/dlibra/login?refUrl=aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ · July 8, 2026 at 12:17 am
References:
River spirit casino https://www.apkmirror.com/wp-content/themes/APKMirror/ap_resize/ap_resize.php?src=https://wbc1.wbc.poznan.pl/dlibra/login?refUrl=aHR0cHM6Ly9kZS50cnVzdHBpbG90LmNvbS9yZXZpZXcvb3dvd2Vhci5kZQ
economyscientist.Com · July 8, 2026 at 12:41 am
casino Ventajas (economyscientist.Com) en ourense
bajar Casino gratis tragamonedas · July 8, 2026 at 1:13 am
pago ruleta bajar Casino gratis tragamonedas
https://viblo.asia/ · July 8, 2026 at 2:08 am
References:
Gala casino nottingham https://viblo.asia/embed?url=http://parrots.ru/proxy.php?link=https://de.trustpilot.com/review/owowear.de
References:
https://viblo.asia/embed?url=http://parrots.ru/proxy.php?link=https://de.trustpilot.com/review/owowear.de
programok.andaba.hu · July 8, 2026 at 2:13 am
nombre casino de juegos (programok.andaba.hu) de aviles asturias
http://mercedes-club.ru/proxy.php?link=https://invent.kde.org/-/external_redirect?url=https://de.trustpilot.com/review/owowear.de · July 8, 2026 at 2:59 am
References:
Casino las vegas http://mercedes-club.ru/proxy.php?link=https://invent.kde.org/-/external_redirect?url=https%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
References:
http://mercedes-club.ru/proxy.php?link=https://invent.kde.org/-/external_redirect?url=https%3A%2F%2Fde.trustpilot.com%2Freview%2Fowowear.de
Casie · July 8, 2026 at 3:09 am
casinos para ganar dinero gratis
My website casino de juego melilla, Casie,
http://cm-us.wargaming.net/frame/?service=frm&project=wot&realm=us&language=en&login_url=https://m.kaskus.co.id/redirect?url=https://de.trustpilot.com/review/owowear.de · July 8, 2026 at 3:17 am
References:
Casino enjoy santiago http://cm-us.wargaming.net/frame/?service=frm&project=wot&realm=us&language=en&login_url=https://m.kaskus.co.id/redirect?url=https://de.trustpilot.com/review/owowear.de
casino En Pergamino · July 8, 2026 at 3:25 am
casino En Pergamino bono de bienvenida sin depósito
dinero real
https://come.ac/california-indian-casinos-19348 · July 8, 2026 at 4:00 am
References:
The star casino sydney https://come.ac/california-indian-casinos-19348
http://k.scandwap.xtgem.com/?id=irenon&url=de.trustpilot.com/review/owowear.de · July 8, 2026 at 5:15 am
References:
Legiano Casino No Deposit Bonus http://k.scandwap.xtgem.com/?id=irenon&url=de.trustpilot.com%2Freview%2Fowowear.de
startsiden.abcnyheter.no · July 8, 2026 at 5:18 am
References:
Legiano Casino Live Casino https://startsiden.abcnyheter.no/sok/nyheter/?q=%2Fde.trustpilot.com%2Freview%2Fowowear.de
sadiajaveed.webmarketingsol.com · July 8, 2026 at 7:01 am
casinos con tiradas gratis por registro
my site; Gano 4 millones en el Casino (sadiajaveed.webmarketingsol.com)
juegos de casinos Gratis 2026 · July 8, 2026 at 5:47 pm
casino en pachuca
My website: juegos de casinos Gratis 2026
Createplacemedia.Com · July 8, 2026 at 6:26 pm
casino casinos en españa Requisitos, Createplacemedia.Com, oropesa del
mar
https://Www.Soins-Chinois.fr · July 8, 2026 at 6:43 pm
jugar online juegos de casino gratis cinco tambores (https://Www.Soins-Chinois.fr)
tragamonedas
casinos que Dan bonos Sin deposito · July 8, 2026 at 6:52 pm
apuestas online casino gratis
My site: casinos que Dan bonos Sin deposito
Casinos en Toledo · July 8, 2026 at 8:24 pm
los Casinos en Toledo
mas lindos de españa
casinos that accept neteller australia · July 9, 2026 at 12:35 am
payid australia casino
Reina · July 9, 2026 at 1:40 am
spielothek in frankfurt am main
Feel free to surf to my webpage: beste obst slots; Reina,
Suzette · July 9, 2026 at 9:18 am
juegos valor de la ruleta casino (Suzette) casino blackjack online
bono 10 euros casino · July 9, 2026 at 9:35 am
bono 10 euros casino mas grande de españa
todo sobre juegos de casino · July 9, 2026 at 12:03 pm
casinos online que regalan un deposito inicial para jugar
Here is my website todo sobre juegos de casino
casinos online con bonus de registro · July 9, 2026 at 6:49 pm
juegos casinos online con bonus de registro gratis para jugar sin descargar
Http://www.eacsolucionsjuridiques.com · July 9, 2026 at 7:05 pm
aplicacion de Jugar casino dinero Real sin deposito (http://www.eacsolucionsjuridiques.com) del canelo
alvarez
Andre · July 9, 2026 at 11:14 pm
bonos gratis apuestas casino casinos reales online, Andre,
casino pagar Con paypal · July 10, 2026 at 1:06 am
jugar juegos casino pagar Con paypal gratis online sin descargar
juegos para jugar con Cartas de Casino · July 10, 2026 at 1:20 am
juegos para jugar con Cartas de Casino villajoyosa reapertura
Margie · July 10, 2026 at 2:32 am
casinos en vivo online
Feel free to visit my site; casino sabiñanigo (Margie)
Casino VillamañAn · July 10, 2026 at 7:54 am
como retirar dinero del Casino VillamañAn
Eugenio · July 10, 2026 at 10:30 am
es casino petra carta (Eugenio) de palmas del mar
Jugar Juegos De Cartas Gratis Casino Online · July 10, 2026 at 10:38 am
dinero Jugar Juegos De Cartas Gratis Casino Online para
casino
casino palermo maquinas tragamonedas · July 10, 2026 at 10:45 am
juegos de casino palermo maquinas tragamonedas
gratis para celular
Chong · July 10, 2026 at 10:47 am
aplicaciones para juegos de dónde jackpot casino online (Chong)
https://Jetbistro.Gastroopinie.pl/tragaperras-en-linea-Para-espanoles/ · July 10, 2026 at 11:00 am
declarar premios Casino (https://Jetbistro.Gastroopinie.pl/tragaperras-en-linea-Para-espanoles/) santa pola
casinos online en españa en bolívares · July 10, 2026 at 3:00 pm
software de ruleta de casino
Have a look at my homepage casinos online en españa en bolívares
descargar juegos de azar gratis casino · July 10, 2026 at 3:31 pm
descargar juegos de azar gratis casino torrelodones actuaciones
benson hedges gold · July 12, 2026 at 7:46 pm
double happiness cigar
AUS CIG SHOP online store is an online cigarette store serving customers across Australia. The website provides a selection of cigarettes and roll-your-own (RYO) tobacco, giving customers a convenient way to purchase tobacco products online.
One of the key benefits of the store is free delivery Australia wide with no minimum order requirement. Customers can place both small and large orders without extra shipping charges.
Orders paid before 5:00 am (GMT+11) are processed and dispatched on the same day, allowing for faster delivery throughout Australia. The store emphasizes secure and dependable shipping to ensure customer privacy.
The website supports several payment methods, including Wise, PayPal, bank transfer, and USDT, giving customers multiple payment options.
The website stocks a wide selection of cigarette brands, including Dunhill, Marlboro, Manchester, Double Happiness, Benson & Hedges, Mevius, Esse, Mac Super Slim, and Oscar Super Slim.
Some of the most popular products are Dunhill Red, Benson & Hedges Gold, Double Happiness, Mevius Option Purple, Esse Change, Mac Super Slim Ice Cool Blast, Oscar Super Slim Ice Cool, and Manchester Royal Red. These products are commonly available in cartons containing 10 packs of 20 cigarettes, often available at sale prices.
The company states that all products are obtained from trusted suppliers and are presented as 100% original products. The store limits sales to customers aged 18+ and emphasizes fair pricing and quality customer service.
The store also includes a blog together with an FAQ section, covering topics such as shipping times, international shipping, payment methods, parcel tracking, shipping costs, order cancellation, and customer support.
vape delivery singapore · July 12, 2026 at 9:23 pm
sg vape
The Singapore Vape Delivery Shop website is an online vape store serving customers across Singapore with online vape products. The company focuses on dependable service, premium products, and quick delivery.
Customer reviews mention the consistency of the delivery service and the overall shopping experience. Reviews commonly note that orders arrive on schedule, the product quality is excellent, and the seller provides professional customer service.
The website offers a broad selection of vaping products, allowing customers to choose from different devices and accessories through a simple online ordering system. Fast delivery and convenient purchasing are presented as key advantages of the service.
The store also supports bulk purchasing options for individuals planning to become vape resellers. Wholesale pricing is available for qualifying orders, with MOQ starting from 50 items.
The platform features a blog section covering topics related to vaping products and general information for consumers. Recent articles discuss legal information, nicotine levels, and vape product ingredients.
An customer FAQ answers common customer questions, including ordering procedures, payment options, minimum order quantities, delivery schedules, and buying vape products in Singapore.
Based on customer reviews the website is appreciated for fast delivery, responsive service, and wholesale availability, serving customers throughout Singapore.
Casinos Legales En EspañA · July 13, 2026 at 4:07 pm
juegos de casino multijuegos
Also visit my web-site :: Casinos Legales En EspañA
Los Meores Casinos Onlain · July 13, 2026 at 6:12 pm
Los Meores Casinos Onlain que aceptan paypal españa
https://mainichi-kenko.info/el-truco-de-Las-slots-en-es-2026/ · July 13, 2026 at 6:49 pm
nuevos casinos sin depósito 2026
Feel free to visit my web blog :: casino de aviles asturias (https://mainichi-kenko.info/el-truco-de-Las-slots-en-es-2026/)
Bert · July 13, 2026 at 8:33 pm
que casino sant cugat (Bert) es mejor
casinos gratis jugar por Diversion · July 13, 2026 at 9:00 pm
de donde proviene la palabra casino
Feel free to surf to my web blog casinos gratis jugar por Diversion
buscar casinos gratis tragamonedas · July 13, 2026 at 10:18 pm
buscar casinos gratis tragamonedas online desde españa
formatos de un casino · July 14, 2026 at 1:03 am
bono para formatos de un casino gran madrid
https://wantu.sfuhost.com · July 14, 2026 at 10:15 am
casino resepsiyon
Review my homepage :: Casinos online en españa en bolívares; https://wantu.sfuhost.com,
Orderedspaces.Co · July 14, 2026 at 10:24 am
Casino Enjoy En Linea (Orderedspaces.Co) cartas online
Gale · July 14, 2026 at 12:17 pm
juegos de casino 100 gratis (Gale) del ayuntamiento
Kassandra · July 14, 2026 at 1:13 pm
bono 5 euros gratis casino – Kassandra, nuevo de san roque
páginas apuestas · July 14, 2026 at 1:35 pm
nba pronosticos páginas apuestas deportivas
Lois · July 14, 2026 at 3:05 pm
casino gratis para celulares
Feel free to surf to my web blog; casinos nuevos sin deposito (Lois)
juegos de casino gratis para jugar en la computadora · July 14, 2026 at 3:28 pm
todos los casinos que den bonos juegos de casino gratis para jugar en la computadora bienvenida
Live wedden · July 14, 2026 at 3:32 pm
weddenschappen boksen 2026
my blog :: Live wedden
Casinos Online Que Te Dan Dinero Por Registrarte · July 14, 2026 at 3:51 pm
descargar juegos de casino jackpot
Here is my blog post … Casinos Online Que Te Dan Dinero Por Registrarte
Hyper Casino canet en roussillon · July 14, 2026 at 4:05 pm
Hyper Casino canet en roussillon
en tehuacan
Https://Imiinstitute.com/ · July 14, 2026 at 4:14 pm
dinero gratis para juegos casino online mercadopago [https://Imiinstitute.com/] sin deposito
juegos multiplicadores casino · July 14, 2026 at 4:36 pm
quiero juegos multiplicadores casino de casinos gratis
Adriana · July 14, 2026 at 5:05 pm
apuestas en casinos en españa – Adriana, con bonus gratis sin deposito
Gracie · July 14, 2026 at 5:05 pm
cuál es el mejor día para jugar en el casino en villa mercedes (Gracie)
mejores juegos de tragamonedas casino · July 14, 2026 at 5:53 pm
mejores juegos de tragamonedas casino la arrabassada
curso apuestas deportivas gratis · July 14, 2026 at 6:26 pm
predicciones curso apuestas deportivas gratis nba
bonos de bienvenida sin deposito casino online · July 14, 2026 at 7:20 pm
black jack 21 juego online bonos de bienvenida sin deposito casino online
Como ganhar apostas multiplas · July 14, 2026 at 7:20 pm
Como ganhar apostas multiplas grátis online
mejores juegos para ganar en casino online · July 14, 2026 at 7:22 pm
mejores juegos para ganar en casino online
de casino tragaperrasgratis
site de aposta esportiva · July 14, 2026 at 8:13 pm
site de aposta esportiva online
Latashia · July 14, 2026 at 9:24 pm
casino online por dinero real (Latashia)
online con tarjeta de crédito visa
mejores casinos en valencia · July 14, 2026 at 10:10 pm
jugar descargar juegos de casino gratis tragamonedas
Here is my page: mejores casinos en valencia
casino online bono de bienvenida · July 15, 2026 at 12:50 am
casino online bono de bienvenida pres
de romans
manchester cigarettes · July 15, 2026 at 1:14 am
manchester cigarettes
Australia Cig Delivery online store is an online tobacco shop providing nationwide service across Australia. Launched in 2024, the business is dedicated to delivering genuine tobacco products with reliable shipping and competitive prices for customers aged 18 and over.
The store offers reliable nationwide shipping, with orders dispatched the same day available for payments received before 5:00 am (GMT+11). All orders are packed in discreet packaging to ensure confidential delivery.
Customers can pay, including PayPal, Wise, bank transfer, and USDT. The store offers secure ordering and reliable delivery, making it easy to purchase tobacco products online.
Australia Cig Delivery offers a wide selection of well-known cigarette brands, including Dunhill, Marlboro, Manchester, Double Happiness, Benson & Hedges, Mevius, Seven Star, and Mac. The catalog includes various cigarette styles and tobacco blends to meet different customer tastes.
The Marlboro brand is known around the world for its authentic flavor and premium tobacco blend. The range features Red, Gold, and Menthol editions, providing different taste options.
Manchester cigarettes are recognized for their clean finish and enjoyable smoking experience. The collection includes different styles for adult smokers.
Double Happiness has become well known for its traditional character, rich aroma, and full-bodied tobacco blend. Originally developed in Asia, the brand is appreciated by customers who enjoy its distinctive taste.
Benson & Hedges is recognized for premium tobacco blends and refined craftsmanship. The brand has developed an international reputation for quality and reliability.
The Dunhill brand belongs to the premium cigarette category, offering carefully selected tobacco and smooth taste. The brand has long been recognized for premium standards and craftsmanship.
According to the company all products are supplied by reliable distributors and are described as 100% authentic. Australia Cig Delivery states that sales are intended exclusively for adults aged 18 years and over while providing secure ordering, reliable delivery, and customer-focused service.
sg vape · July 15, 2026 at 1:44 am
vape sg
Singapore Vape Delivery is an online vape retailer serving customers across Singapore with online vape products. The website is committed to quality products, reliable customer service, and convenient delivery.
Many customers mention the consistency of the delivery service and the overall shopping experience. Reviews commonly note that products are delivered promptly, the products are of good quality, and the seller provides professional customer service.
The website offers an extensive vape catalog, including various vape devices and accessories through an easy-to-use online store. Fast delivery and convenient purchasing are among the main benefits of the service.
Singapore Vape Delivery Shop also offers bulk purchasing options for customers interested in becoming vape resellers or sales agents in Singapore. Bulk order discounts are available, with a minimum order quantity of 50 items.
The website features an informational blog covering articles about vaping. Recent articles discuss Singapore vaping laws, nicotine strength comparisons, and vape ingredients.
An Frequently Asked Questions page answers common customer questions, including how to place an order, available payment methods, minimum order requirements, delivery timeframes, and general information about purchasing vape products in Singapore.
According to customer feedback the store is recognized for dependable delivery, quality products, competitive wholesale options, and an easy online ordering process, serving customers throughout Singapore.
casino en líNea online · July 15, 2026 at 6:03 am
casino en líNea online
online con tarjeta de crédito
Lauri · July 15, 2026 at 8:36 am
casinos españoles con bono sin deposito
my web blog :: juegos de casino gratis tragamonedas slots –
Lauri,
Casinos Extranjeros · July 15, 2026 at 10:07 am
juega a las cartas con los invitados del casino
my page Casinos Extranjeros
casino puerto Real · July 15, 2026 at 10:13 am
el mejor juego de casinos para android
My webpage :: casino puerto Real
https://charlesrhodesportfolio.com/ · July 15, 2026 at 10:21 am
apuesta minima en un casino online españa legal, https://charlesrhodesportfolio.com/,
Juegos De Casino Classic · July 15, 2026 at 11:09 am
jugar gratis tragamonedas Juegos De Casino Classic casino puerto banus
Myles · July 15, 2026 at 11:14 am
ganar en el casino tragamonedas
my blog post: top 20 online casinos – Myles,
significado stake en apuestas · July 15, 2026 at 11:25 am
mejores cuotas casas de significado stake en apuestas
Maurine · July 15, 2026 at 12:25 pm
combinada apuestas en perú (Maurine)
juegos online casino del rio · July 15, 2026 at 12:38 pm
juegos online casino del rio san remo tel aviv
mejores casinos crypto · July 15, 2026 at 12:43 pm
casino ciudad rodrigo
Here is my blog post: mejores casinos crypto
Yolanda · July 15, 2026 at 12:58 pm
jogos melhores apostas esportivas para hoje (Yolanda) online
jugar juegos de casino gratis tragamonedas con bonos · July 15, 2026 at 12:58 pm
casinos en navarra
Feel free to surf to my blog; jugar juegos de casino gratis tragamonedas con bonos
gran Casino los ángeles españA · July 15, 2026 at 1:14 pm
casinos online que mejor pagan
My web site :: gran Casino los ángeles españA
Julian · July 15, 2026 at 1:24 pm
casino en bristol (Julian) con bonus
gratis
que impuestos pagan los casinos y tragamonedas · July 15, 2026 at 1:25 pm
casino taormina sicily
Look at my site … que impuestos pagan los casinos y tragamonedas
Zoloft and gambling · July 15, 2026 at 1:39 pm
slot machines ontario united states, usa friendly casino no deposit free spins
2021 Zoloft and gambling no deposit
bonus codes australia casino, or top 20 online casinos usa no
deposit
Jerald · July 15, 2026 at 1:49 pm
favoritos nba impuestos sobre apuestas [Jerald]
Apuestas Mlb Pronosticos · July 15, 2026 at 2:10 pm
Apuestas Mlb Pronosticos copa europa
Bonos Apuestas · July 15, 2026 at 2:29 pm
curso Bonos Apuestas deportivas
gratis
juegos para ganar dinero real Sin depósito casino online · July 15, 2026 at 2:51 pm
casinos con juegos para ganar dinero real Sin depósito casino online
Apuestas Online Gratis Sin Deposito · July 15, 2026 at 2:55 pm
Apuestas Online Gratis Sin Deposito athletic sevilla
juegos de casino que tengan bonus · July 15, 2026 at 3:03 pm
juegos de casino que tengan bonus curacao online
apuestas deportivas libres de impuestos · July 15, 2026 at 3:10 pm
app de apuestas deportivas libres de impuestos gratis
Teena · July 15, 2026 at 3:18 pm
apuestas quien ganara el mundial (Teena) futbol en directo
Https://Www.Fotografiafede.Es/El-Futuro-De-Las-Apuestas-En-Ufc-Tendencias-Para-Los-Proximos-Anos/ · July 15, 2026 at 3:49 pm
mejor casa Celta Alaves Apuestas, https://Www.Fotografiafede.Es/El-Futuro-De-Las-Apuestas-En-Ufc-Tendencias-Para-Los-Proximos-Anos/, deportivas españa
Golf odds sammenligning · July 15, 2026 at 3:51 pm
alle spiludbydere
My page – Golf odds sammenligning
Sammy · July 15, 2026 at 4:11 pm
ayr gold cup betting 2026
my site … how to place a bet on horse racing
uk (Sammy)
http://Www.sonrisoterapia.com/de-rol-van-nft-s-in-de-bitcoin-markt/ · July 15, 2026 at 4:11 pm
sports top bitcoin beste wedden (http://Www.sonrisoterapia.com/de-rol-van-nft-s-in-de-bitcoin-markt/) promo 2026
British Horse Racing Not On Gamstop · July 15, 2026 at 4:13 pm
today’s British Horse Racing Not On Gamstop racing results at lingfield
rabona scommesse app download · July 15, 2026 at 4:19 pm
pronostico napoli atalanta coppa italia
Feel free to visit my blog post; rabona scommesse app download
free horse racing Betting Games · July 15, 2026 at 4:22 pm
free horse racing Betting Games
results for wolverhampton
http://www.Tenamotors.Com/ · July 15, 2026 at 4:31 pm
bonus sammenligning betting
Feel free to surf to my blog: odds med visa (http://www.Tenamotors.Com/)
apuestas juegos olímpicos · July 15, 2026 at 4:35 pm
casa de apuestas juegos olímpicos
de futbol
Wedden Sport Spelletjes Tips · July 15, 2026 at 4:35 pm
ajax benfica Wedden Sport Spelletjes Tips
Corinne · July 15, 2026 at 4:46 pm
online sporte-wedden hockey – Corinne,
sporte-wedden snooker
descargar juegos de casino Sin internet · July 15, 2026 at 5:03 pm
descargar juegos de casino Sin internet de casino para pc gratis en español
Stake Apuestas Deportivas · July 15, 2026 at 5:19 pm
que significa 1×2 en Stake Apuestas Deportivas deportivas
Frank · July 15, 2026 at 5:38 pm
apuestas betis girona – Frank, deportivas simulador eurocopa
apuestas f1 bahrein · July 15, 2026 at 5:50 pm
ofertas apuestas f1 bahrein deportivas
Half time full time Strategy · July 15, 2026 at 5:52 pm
total shots betting
Feel free to surf to my webpage Half time full time Strategy
Casino roulette Juego · July 15, 2026 at 5:56 pm
juegos casinos gratis para jugar sin descargar
Have a look at my site … Casino roulette Juego
gratis fodboldtips · July 15, 2026 at 5:58 pm
fodbold odds sammenligning
my page … gratis fodboldtips
https://www.Greencoopeu.eu · July 15, 2026 at 6:08 pm
tiradas gratis por registro sin deposito bono 10 euros
casino (https://www.Greencoopeu.eu)
cuanto se paga de Impuestos por apuestas · July 15, 2026 at 6:14 pm
cuotas cuanto se paga de Impuestos por apuestas final champions
Leigh · July 15, 2026 at 6:34 pm
how many online casinos in usa, online casinos free
spins no deposit usa approved and how much top progressive
jackpots online casino (Leigh) pokies
and casinos united statesn coins, or milwausaee casino entertainment
https://vcode.pro/como-elegir-el-mejor-casino-en-linea-espana/ · July 15, 2026 at 6:41 pm
maquinas app máquinas tragamonedas de casino (https://vcode.pro/como-elegir-el-mejor-casino-en-linea-espana/) casinos gratis sin descargar
https://poolqualityservices.com/das-glucksspielverhalten-der-deutschen-im-jahr-2026/ · July 15, 2026 at 6:56 pm
1 euro einzahlen 100 freispiele
my web-site wo ist das größte Casino der Welt (https://poolqualityservices.com/das-glucksspielverhalten-der-deutschen-im-jahr-2026/)
Betting Odds Explained · July 15, 2026 at 7:00 pm
best mobile Betting Odds Explained signup offers
vip betting tips apk · July 15, 2026 at 7:06 pm
value vip betting tips apk
Inter barcelona apuestas · July 15, 2026 at 7:16 pm
paginas de Inter barcelona apuestas esports
http://www.celestialcaringent.com · July 15, 2026 at 7:18 pm
online casino ohne wartezeit kreditkarte (http://www.celestialcaringent.com)
60 freispiele bei anmeldung
Casa Apuestas Chile · July 15, 2026 at 7:21 pm
Casa Apuestas Chile galgos online
apuestas bono sin Deposito · July 15, 2026 at 7:23 pm
apuestas bono sin Deposito
futbol hoy
casino loyalitätsbonus 2026 · July 15, 2026 at 7:24 pm
casino loyalitätsbonus 2026
20 euro cashtocode
Larry · July 15, 2026 at 7:39 pm
glücksspiele mit karten
My blog – online casino ab 15 euro visa (Larry)
Nannie · July 15, 2026 at 7:55 pm
online gambling bet sportsbook (Nannie)
https://www.sominformatics.com/ · July 15, 2026 at 7:59 pm
casas de apuestas en argentina (https://www.sominformatics.com/) argentina polonia
Spencer · July 15, 2026 at 8:00 pm
casinos con tragamonedas gratis para descargar
Take a look at my web blog casino en munro,
Spencer,
http://www.futursun.mx/2026/06/29/Bono-de-casino-sin-Deposito-10-Euros-en-es-2026/ · July 15, 2026 at 8:04 pm
juegos de casinos gratis para descargar
Also visit my web site :: app casino dinero real iphone (http://www.futursun.mx/2026/06/29/Bono-de-casino-sin-Deposito-10-Euros-en-es-2026/)
who to bet on at cheltenham today · July 15, 2026 at 8:05 pm
horse racing non runners for who to bet on at cheltenham today
Rudolph · July 15, 2026 at 8:15 pm
software predicción apuestas ganar mundial – Rudolph, deportivas
mejor sitio de apuestas de futbol · July 15, 2026 at 8:20 pm
prediccion mejor sitio de apuestas de futbol deportivas gratis
Angus · July 15, 2026 at 8:29 pm
promo sportweddenschappen
My web blog; golf weddenschappen tips 2026 (Angus)
casino gratis sin descargar ni registrarse · July 15, 2026 at 8:33 pm
casino gratis sin descargar ni registrarse en buta ranquil
Https://Homeeffect.pl · July 15, 2026 at 8:36 pm
horse racing results from wolverhampton yesterday
my homepage: best aintree betting odds (https://Homeeffect.pl)
Normand · July 15, 2026 at 8:37 pm
casino bonus one einzahlung (Normand) mit sofort bonus ohne einzahlung
basketball wetten anbieter aus bewertungskriterien? · July 15, 2026 at 9:23 pm
quote bei basketball wetten anbieter aus bewertungskriterien? dass
Casinos con bonos de bienvenida Sin Depósitos · July 15, 2026 at 9:31 pm
buscar juegos Casinos con bonos de bienvenida Sin Depósitos
maquinas de casino gratis
Betting Cheltenham Tomorrow · July 15, 2026 at 9:41 pm
daily Betting Cheltenham Tomorrow tips 1×2
basketball wetten Ab punktevorsprung sieg tippen · July 15, 2026 at 9:55 pm
heute basketball wetten Ab punktevorsprung sieg tippen
handicap Apuestas Baloncesto · July 15, 2026 at 10:09 pm
handicap Apuestas Baloncesto draft nfl
Beste bookmaker online wedden · July 15, 2026 at 10:18 pm
virtuele Beste bookmaker online wedden voor geld
Apuestas Gratis · July 15, 2026 at 10:31 pm
Apuestas Gratis chelsea
barcelona
über unter wetten basketball · July 15, 2026 at 10:39 pm
sportwetten verdoppler strategie
my blog post – über unter wetten basketball
Chiquita · July 15, 2026 at 10:49 pm
new zealandn poker 2 free game, is gambling illegal in the uk and casino in united
states near detroit, or what does big casino mean (Chiquita) the usa
have casinos
Apostas Over e under · July 15, 2026 at 10:51 pm
Apostas Over e under
prontas para hoje
buscador cuotas Apuestas · July 15, 2026 at 11:00 pm
casas buscador cuotas Apuestas deportivas españa
clinicallumpons.es · July 15, 2026 at 11:02 pm
casino madrid mejores paginas de apuestas (clinicallumpons.es) deportivas
https://Www.seaic.es · July 15, 2026 at 11:20 pm
tipos de apuestas deportivas online peru (https://Www.seaic.es)
WWW.Hernandezcano.es · July 15, 2026 at 11:32 pm
spread que es 1×2 en apuestas deportivas (http://WWW.Hernandezcano.es) español apuestas
Tandy · July 15, 2026 at 11:36 pm
cuantas apuestas hacer al dia – Tandy
– combinadas hoy
casino san Roque · July 15, 2026 at 11:55 pm
casinos online con licencia en españa
Take a look at my blog casino san Roque
Casimira · July 16, 2026 at 12:08 am
juegos paginas de apuestas con paypal (Casimira) apuestas deportivas gratis
Https://Www.Entresoles.Es/ · July 16, 2026 at 12:20 am
Apuestas Favoritos Eurocopa (https://Www.Entresoles.Es/) deportivas para hoy
Apuestas real madrid champions · July 16, 2026 at 12:22 am
Apuestas real madrid champions
carreras de caballos en directo
Freispiele bonus casino deutschland · July 16, 2026 at 12:36 am
neues casino bester Freispiele bonus casino deutschland
Apuestas Futbol Americano Nfl · July 16, 2026 at 1:06 am
casas de Apuestas Futbol Americano Nfl deportivas
https://WWW.Poceriaromero.es · July 16, 2026 at 1:08 am
sitios de deportes Apuestas en Vivo (https://WWW.Poceriaromero.es)
deportivas argentina
jugar 21 en casino · July 16, 2026 at 1:33 am
apuesta dados jugar 21 en casino
online blackjack google pay bezahlen · July 16, 2026 at 2:52 am
top casino apps
Feel free to visit my site – online blackjack google pay bezahlen
https://Middle-aisle.com/ · July 16, 2026 at 3:00 am
høje odds tips
Stop by my site: populære oddsudbydere (https://Middle-aisle.com/)
basketball wm wett Tipps · July 16, 2026 at 3:28 am
sportwetten bonus schweiz
Here is my page … basketball wm wett Tipps
Autorecambiosbastida.Com · July 16, 2026 at 3:30 am
plataformas de Final Copa Del Rey Apuestas (Autorecambiosbastida.Com)
ruleta De casino online gratis · July 16, 2026 at 3:31 am
ruleta De casino online gratis en cruceros
poucomais.com · July 16, 2026 at 3:51 am
profi sportwetten vorhersagen
my web-site; basketball wett tipps heute (poucomais.com)
apuestas de futbol mundial · July 16, 2026 at 3:57 am
apuestas de futbol mundial deportivas estrategias
College Basketball wetten · July 16, 2026 at 4:05 am
wettquoten
my web-site – College Basketball wetten
Susie · July 16, 2026 at 4:06 am
dantoto aalborg
Also visit my web page … oddssammenligning ski; Susie,
online slots mecklenburg-vorpommern · July 16, 2026 at 4:15 am
online slots mecklenburg-vorpommern slots saarland
app de apuestas En españa · July 16, 2026 at 4:15 am
mejores casas app de apuestas En españa apuestas en mexico
Apuestas Deportivas Ufc · July 16, 2026 at 4:28 am
casas de Apuestas Deportivas Ufc españa alemania
Juegos de casino gratis modo demo · July 16, 2026 at 4:35 am
casino Juegos de casino gratis modo demo tlalpan
www.Mrclickeventos.com · July 16, 2026 at 4:41 am
staatliches casino Ohne maximaleinsatz deutschland (http://www.Mrclickeventos.com)
bono Sin deposito casino español · July 16, 2026 at 4:42 am
pagos de la ruleta bono Sin deposito casino español
Black Jack Online Apuestas Casino · July 16, 2026 at 4:51 am
Black Jack Online Apuestas Casino depósito
mínimo 2 euro
Antoinette · July 16, 2026 at 5:04 am
oddssammenligning tennis
Visit my page: betting med mobilepay (Antoinette)
lopesan casino meloneras · July 16, 2026 at 5:07 am
buscar juegos de maquinas de lopesan casino meloneras gratis
Golf tips i Dag · July 16, 2026 at 5:12 am
odds med kort
Feel free to surf to my web site :: Golf tips i Dag
spiltips esport · July 16, 2026 at 5:14 am
betting bonus vilkår
Also visit my page; spiltips esport
Azucena · July 16, 2026 at 5:20 am
seriöse online basketball wetten heute, Azucena,
Kelly · July 16, 2026 at 5:57 am
oddssammenligning ishockey
Also visit my web site … spille på sport med mobilepay (Kelly)
las Mejores app de apuestas · July 16, 2026 at 6:03 am
las Mejores app de apuestas nfl
Https://Michaelenglish.Es/2026/06/06/Como-Activar-Bizum-En-Tu-Banco-Y-Jugar-En-Casinos-Sin-Complicaciones/ · July 16, 2026 at 6:04 am
Gran Casino Puerto Del Carmen – https://Michaelenglish.Es/2026/06/06/Como-Activar-Bizum-En-Tu-Banco-Y-Jugar-En-Casinos-Sin-Complicaciones/,
de tomares
massage-sensuel-Couple.com · July 16, 2026 at 6:13 am
omsætningskrav betting bonus
My web page; bedste danske bettingsider (massage-sensuel-Couple.com)
basketball Wm wett tipps · July 16, 2026 at 6:15 am
esport wettseiten
Review my page; basketball Wm wett tipps
beneficios de casinos Online · July 16, 2026 at 6:24 am
casino beneficios de casinos Online
sueca
jugar ruleta casino gratis español · July 16, 2026 at 6:28 am
blackjack jugar ruleta casino gratis español bonuses
Plinko spiel mit paypal · July 16, 2026 at 6:39 am
online casino 200 euro gratis
Feel free to surf to my page; Plinko spiel mit paypal
https://Simplexhealth.com/ · July 16, 2026 at 6:43 am
live odds badminton
Here is my web site … bettingtips proffstips (https://Simplexhealth.com/)
Apuestas juegos · July 16, 2026 at 6:50 am
Apuestas juegos en la champions league
Apuestas pronosticos nba · July 16, 2026 at 6:57 am
apps de Apuestas pronosticos nba mexico
Online casino mit 3 euro einzahlung · July 16, 2026 at 7:01 am
Online casino mit 3 euro einzahlung mindesteinzahlung 30 euro giropay
apuestas betplay Hoy colombia · July 16, 2026 at 7:34 am
apuestas betplay Hoy colombia regalo de bienvenida
Temeka · July 16, 2026 at 7:38 am
beste app zum handicap basketball wetten (Temeka)
maquinas nuevas De casino para Jugar Gratis · July 16, 2026 at 7:48 am
juegos maquinas nuevas De casino para Jugar Gratis casinos
que pagan dinero real
bono de apuestas gratis sin deposito · July 16, 2026 at 7:52 am
impuestos a las bono de apuestas gratis sin deposito deportivas
Frederick · July 16, 2026 at 8:16 am
poker od 10 groszy
My site sloty online tether (Frederick)
matematyka w kasynie · July 16, 2026 at 8:24 am
legalne kasyno online toruń
my blog – matematyka w kasynie
Spiludbydere · July 16, 2026 at 8:33 am
betting uden indbetalingsgrænse
Here is my webpage … Spiludbydere
Impuestos De Apuestas · July 16, 2026 at 8:49 am
Impuestos De Apuestas deportivas para hoy pronosticos
Casino playa chiquita · July 16, 2026 at 9:03 am
juegos de Casino playa chiquita
sin descargar
https://Truck-Food.de/?p=4705 · July 16, 2026 at 9:05 am
sportwetten anbieter
Also visit my web site; euroleague basketball wetten (https://Truck-Food.de/?p=4705)
ishockey tips i dag · July 16, 2026 at 9:12 am
betting tennis
Also visit my webpage ishockey tips i dag
casino De adrogue · July 16, 2026 at 9:17 am
casino De adrogue villanueva de la cañada
Https://Ashok-COM.Stackstaging.com · July 16, 2026 at 9:17 am
neue sportwetten seiten
Visit my website: sichere basketball wetten (https://Ashok-COM.Stackstaging.com)
oddset live · July 16, 2026 at 9:27 am
oddset live forhandler kolding
apuestas real Madrid Vs atletico · July 16, 2026 at 9:37 am
estadísticas apuestas real Madrid Vs atletico
WWW.Rentacanaria.com · July 16, 2026 at 9:40 am
danske spil betting, http://WWW.Rentacanaria.com, på heste online
beste live casino neosurf · July 16, 2026 at 9:55 am
online beste live casino neosurf echtgeld
roulette
Odds badminton · July 16, 2026 at 9:57 am
udenlandske spiludbydere mobilepay
My page; Odds badminton
mit basketball wetten Geld verdienen · July 16, 2026 at 10:23 am
wette deutschland dänemark
Feel free to surf to my webpage; mit basketball wetten Geld verdienen
Tawanna · July 16, 2026 at 10:36 am
jackpot slots mit freispielen
my web page :: legales casino apps, Tawanna,
significado 1x2 apuestas · July 16, 2026 at 10:39 am
avisador de cuotas significado 1×2 apuestas
casino ein und auszahlung · July 16, 2026 at 10:39 am
casino ein und auszahlung mit 3 euro einzahlung klarna
Amorphosistudio.Com · July 16, 2026 at 10:46 am
craps niskie stawki online
Here is my blog post :: Kasyno Bez Licencji Bitcoin – Amorphosistudio.Com,
Hildegarde · July 16, 2026 at 12:39 pm
mejores pronosticos apuestas deportivas – Hildegarde – quien gana eurocopa
pronosticos apuestas formula 1 · July 16, 2026 at 12:55 pm
casa de pronosticos apuestas formula 1 bono
Casino De San Javier · July 16, 2026 at 1:28 pm
premier Casino De San Javier tragaperras
Marlboro Menthol · July 16, 2026 at 1:37 pm
Marlboro Menthol
AUS CIG SHOP is an online tobacco shop serving customers across Australia. The website offers cigarettes and roll-your-own (RYO) tobacco products, giving customers an easy way to order tobacco products online.
A major feature of the website is Australia-wide free shipping with no minimum purchase. Customers can place both small and large orders without extra shipping charges.
Orders completed before 5:00 am (GMT+11) are sent out the same day, allowing for faster delivery throughout Australia. The company highlights reliable and discreet delivery throughout Australia.
AUS CIG SHOP accepts several payment methods, including bank transfer, Wise, PayPal, and USDT, giving customers multiple payment options.
The shop stocks many popular cigarette brands, including Dunhill, Marlboro, Manchester, Double Happiness, Benson & Hedges, Mevius, Esse, Mac Super Slim, and Oscar Super Slim.
Among the best-selling products are Manchester Royal Red, Dunhill Red, Benson & Hedges Gold, Double Happiness, Mevius Option Purple, Esse Change, Mac Super Slim Ice Cool Blast, and Oscar Super Slim Ice Cool. These cigarettes are usually offered as 10 packs of 20 cigarettes, often available at sale prices.
According to information on the website all products are obtained from trusted suppliers and are described as 100% original. The business serves adult customers aged 18 and over and emphasizes fair pricing and quality customer service.
The website also includes a blog and a frequently asked questions section, covering topics such as shipping times, international shipping, payment methods, parcel tracking, shipping costs, order cancellation, and customer support.
singapore vape shop · July 16, 2026 at 1:40 pm
vape delivery singapore
Singapore Vape Delivery is a Singapore-based vape shop focused on providing customers in Singapore with a convenient ordering experience. The company emphasizes dependable service, premium products, and quick delivery.
Feedback from customers mention the consistency of the delivery service and the overall shopping experience. Reviews often state that orders arrive on schedule, the product quality is excellent, and the seller provides professional customer service.
The store features a wide range of vape products, including various vape devices and accessories through a simple online ordering system. Fast delivery and convenient purchasing are among the main benefits of the service.
Singapore Vape Delivery Shop also supports bulk purchasing options for customers interested in becoming vape resellers or sales agents in Singapore. Bulk order discounts are available, with minimum wholesale orders of 50 products.
The store includes an informational blog covering topics related to vaping products and general information for consumers. Recent articles discuss legal information, nicotine levels, and vape product ingredients.
An Frequently Asked Questions page answers common customer questions, including online ordering, payments, shipping times, minimum purchases, and customer support.
Based on customer reviews the store is known for reliable shipping, quality vape products, and convenient ordering, serving customers throughout Singapore.
juegos de maquinitas de casinos gratis · July 16, 2026 at 1:41 pm
casino palermo tragamonedas juegos de maquinitas de casinos gratis
best cheap smoke online australia · July 16, 2026 at 1:42 pm
buy cigarettes online australia The Australia Tobacconist Hub website is an online cigarette retailer offering a wide selection of cigarettes and tobacco products throughout Australia. The website focuses on competitive pricing, convenient ordering, and reliable delivery, providing a convenient online shopping experience.
The store accepts orders using various payment methods, including PayPal, Wise, Bank Transfer, USDT, and more. Orders are accepted through WhatsApp and email, while the service team provides help with product questions and delivery tracking.
The store provides fast and discreet tobacco delivery throughout Australia. Fast order processing is available, with an emphasis on dependable shipping and customer convenience.
Australia Tobacconist Hub stocks a wide variety of tobacco brands, including Marlboro, Manchester, Double Happiness, Bossku, Zhongnanhai, Dunhill, and Benson & Hedges. The catalog includes premium as well as affordable products for a variety of smoking preferences.
Some of the top-selling products are Double Happiness Nanyang Soft Pack, Manchester Sapphire Blue Dubai Edition, Manchester Special Edition Flow Red Dubai Version, Manchester Blue Crush Dubai Version, Dunhill Blue UK Version, Dunhill Red UK Version, Benson & Hedges Gold, and Zhongnanhai. Selected products are supplied in 10-pack cartons.
The website focuses on quality tobacco products at reasonable prices. Customers looking for inexpensive tobacco and recognized international cigarette brands have access to a wide product selection.
The platform also features a section discussing smoking cessation. It explains that stopping smoking can improve health over time, highlighting the positive effects of reducing tobacco consumption.
Que es momio en Apuestas · July 16, 2026 at 1:47 pm
combinadas Que es momio en Apuestas deportivas
casino Gran madrid Apuestas · July 16, 2026 at 1:49 pm
casino Gran madrid Apuestas celta barcelona
https://www.alperroverde.es/Como-gestionar-tus-ganancias-y-perdidas-en-apuestas/ · July 16, 2026 at 1:50 pm
que son las apuestas barcelona atletico de madrid (https://www.alperroverde.es/Como-gestionar-tus-ganancias-y-perdidas-en-apuestas/) multiples
Apuestas De Blackjack En Linea · July 16, 2026 at 1:53 pm
Apuestas De Blackjack En Linea final champions league
najlepsze kasyno online dla początkujących · July 16, 2026 at 2:05 pm
gry automaty zagraj
Also visit my page – najlepsze kasyno online dla początkujących
manchester sapphire blue · July 16, 2026 at 2:28 pm
manchester cigarettes
Australia Cig Delivery is an online tobacco shop providing nationwide service across Australia. Launched in 2024, the company is dedicated to delivering genuine tobacco products with reliable shipping and competitive prices for customers aged 18 and over.
The company provides Australia-wide fast delivery, with orders dispatched the same day available for payments received before 5:00 am (GMT+11). Every order is shipped in discreet packaging to ensure confidential delivery.
Several payment methods are available, including USDT, Wise, PayPal, and bank transfer. The website offers secure ordering and reliable delivery, making it easy to purchase tobacco products online.
The store offers numerous popular tobacco brands, including Marlboro, Manchester, Double Happiness, Benson & Hedges, Dunhill, Mevius, Seven Star, and Mac. The selection includes various cigarette styles and tobacco blends to meet different customer tastes.
Marlboro is known around the world for its authentic flavor and premium tobacco blend. Popular options include Red, Gold, and Menthol editions, providing different taste options.
Manchester cigarettes are known for their smooth taste and balanced smoking experience. The range includes classic and menthol varieties.
The Double Happiness brand has built a reputation for its traditional character, rich aroma, and full-bodied tobacco blend. Originating in Asia, the brand remains popular among adult smokers who value its long-standing heritage.
Benson & Hedges is known for its premium quality and smooth smoking experience. The brand has built a strong global reputation for its refined tobacco blends and craftsmanship.
The Dunhill brand belongs to a premium tobacco brand, offering carefully selected tobacco and smooth taste. The brand has become known for quality, consistency, and traditional craftsmanship.
According to information on the website all products are obtained from reputable suppliers and are described as 100% authentic. The store states that orders are accepted only from adults over 18 while focusing on affordable prices, dependable service, and Australia-wide shipping.
https://Proscenioteatro.com · July 16, 2026 at 2:39 pm
sistema 2/4 apuestas portugal uruguay (https://Proscenioteatro.com)
Nam · July 16, 2026 at 2:44 pm
apuestas baloncesto juegos olimpicos (Nam) casino online argentina
casino y mujeres · July 16, 2026 at 2:45 pm
casino y mujeres online blackjack live
handicap asiatico en apuestas · July 16, 2026 at 2:48 pm
consejos de handicap asiatico en apuestas
Futsal Betting Online · July 16, 2026 at 2:50 pm
online Futsal Betting Online
site
Aprire Centro Scommesse · July 16, 2026 at 3:01 pm
offerte bookmakers italiani
Here is my web site: Aprire Centro Scommesse
Shaunte · July 16, 2026 at 3:01 pm
tipos de apuestas de futbol – Shaunte,
esports colombia
el mejor juego de casinos para android · July 16, 2026 at 3:03 pm
juegos de cartas el mejor juego de casinos para android casino gratis
Apuestas Momios · July 16, 2026 at 3:05 pm
Apuestas Momios deportivas.com foro
Nhl apuestas · July 16, 2026 at 3:10 pm
Nhl apuestas deportivas golf
Kenneth · July 16, 2026 at 3:12 pm
real madrid vs real sociedad apuestas (Kenneth)
altas y bajas
App Casa de apuestas · July 16, 2026 at 3:12 pm
apuestas App Casa de apuestas caballos
entresoles.es · July 16, 2026 at 3:18 pm
tipos de betis chelsea apuestas (entresoles.es) betplay
casino minimální vklad 1 kč paypal · July 16, 2026 at 3:23 pm
casino minimální vklad 1 kč paypal hrací automaty online
old.Brilianto.com · July 16, 2026 at 3:28 pm
ethereum casino pro české hráče (old.Brilianto.com) skrill bonus
kde hrát online casino Ústí nad Labem · July 16, 2026 at 3:52 pm
mobilní kde hrát online casino Ústí nad Labem ecopayz
nejlepší casino do mobilu · July 16, 2026 at 3:55 pm
online nejlepší casino do mobilu s paysafecard
best horse Race betting sites · July 16, 2026 at 4:20 pm
wolverhampton best horse Race betting sites racing betting odds
české casino s reload bonusem · July 16, 2026 at 4:36 pm
online české casino s reload bonusem vklad 5 kč
neteller
čEské Casino VýBěR Na Ecopayz · July 16, 2026 at 4:39 pm
klarna casino pro čEské Casino VýBěR Na Ecopayz hráče
Antje · July 16, 2026 at 5:15 pm
juegos maquinitas de casino online (Antje) casino ruleta electronica
ZahraničNí Casino Mobil · July 16, 2026 at 5:30 pm
nejlepší ZahraničNí Casino Mobil
Brno
gestpointnig.com · July 16, 2026 at 5:42 pm
české casino free Spin bez vkladu (gestpointnig.com) seznam
pronostici scommesse coppa italia · July 16, 2026 at 5:45 pm
verticale pronostici scommesse coppa italia sportive
casas Nuevas apuestas · July 16, 2026 at 5:53 pm
casas Nuevas apuestas valladolid valencia
Apuestas celta real madrid · July 16, 2026 at 5:56 pm
impuesto a las Apuestas celta real madrid
ofertas recurrentes casas de apuestas · July 16, 2026 at 5:58 pm
ofertas recurrentes casas de apuestas holanda vs argentina
Scommessa italia belgio · July 16, 2026 at 6:06 pm
scommesse digitali italiano español
Have a look at my blog: Scommessa italia belgio
Oddstips Ki · July 16, 2026 at 6:08 pm
värdespel premier league
Also visit my blog; Oddstips Ki
Jamel · July 16, 2026 at 6:29 pm
el mejor sitio de apuestas deportivas sin dinero (Jamel)
online Casino Vklad 1 Kč sms · July 16, 2026 at 6:46 pm
české online Casino Vklad 1 Kč sms s licenci
abetterratetoday.com · July 16, 2026 at 6:48 pm
difference between expert betting (abetterratetoday.com) exchange and bookmaker
Best Sports betting system · July 16, 2026 at 7:01 pm
which bookmaker is the Best Sports betting system
Tyrell · July 16, 2026 at 7:16 pm
online deposit bonus betting; Tyrell, sport
capitalhumanogf.com · July 16, 2026 at 7:19 pm
best betting odds for The eurovision song contest [capitalhumanogf.com]
agents
celtic Betting · July 16, 2026 at 7:24 pm
celtic Betting site
live streaming
Lingfield Horse Racing Results Today Live · July 16, 2026 at 7:28 pm
yesterday s Lingfield Horse Racing Results Today Live results wolverhampton
casino 25 free spinů bez vkladu · July 16, 2026 at 7:32 pm
online casino 25 free spinů bez vkladu
free spiny dnes
Ken · July 16, 2026 at 7:40 pm
apuestas en vivo ufc (Ken) nfl
pronósticos
Myflightime.Com · July 16, 2026 at 7:47 pm
todays Betting Sites With Early Payout – Myflightime.Com, tip
apuestas campeon motogp 2025 · July 16, 2026 at 7:48 pm
que significa 3.5 goles en apuestas campeon motogp 2025
betting and predictions · July 16, 2026 at 7:49 pm
ecopayz betting and predictions sites
Bruce · July 16, 2026 at 7:51 pm
kombspel tips allsvenskan
Feel free to surf to my blog post … v64 system (Bruce)
i migliori scommesse italiani · July 16, 2026 at 8:00 pm
i migliori scommesse italiani previsioni
oddssidor utan omsättningskrav · July 16, 2026 at 8:26 pm
esport odds
Also visit my site; oddssidor utan omsättningskrav
casino Bez regulace · July 16, 2026 at 8:45 pm
live casino Bez regulace s bonusem bez vkladu
Charmain · July 16, 2026 at 8:49 pm
good betting apps for sports (Charmain) results today
Maybell · July 16, 2026 at 8:53 pm
oddssidor utan svensk licens 2026
my web site :: odds sidor (Maybell)
apuestas 3 Division · July 16, 2026 at 8:55 pm
pronostico apuestas 3 Division tenis
Cheryl · July 16, 2026 at 8:56 pm
české peníze zdarma za založení účtu casino (Cheryl) platba klarna
casino registrace bank id · July 16, 2026 at 9:05 pm
nová casina bez vkladu 2026
Here is my web blog casino registrace bank id
Frederic · July 16, 2026 at 9:17 pm
valencia vs real madrid apuestas (Frederic) deportivas copa libertadores
Oddssidor Utan Spelpaus Nya · July 16, 2026 at 9:32 pm
bettingsidor Oddssidor Utan Spelpaus Nya licens swish
Betting Sites Top · July 16, 2026 at 9:44 pm
cheltenham festival Betting Sites Top tips
apuestas altas y bajas nfl · July 16, 2026 at 9:45 pm
app de apuestas altas y bajas nfl ecuador
scommesse cavalli virtuali · July 16, 2026 at 9:47 pm
lista ios scommesse cavalli virtuali italiani
speltips Ki · July 16, 2026 at 9:53 pm
betting tips flashback
Here is my site speltips Ki
casino con promociones casino · July 16, 2026 at 10:11 pm
cargar fichas casino con promociones casino online
casino real con bono sin depósito · July 16, 2026 at 10:13 pm
el casino real con bono sin depósito vallirana
casinos que regalan bonos 2026 · July 16, 2026 at 10:14 pm
casinos que regalan bonos 2026 de rio hondo
Don · July 16, 2026 at 10:18 pm
match betting guide
Here is my blog; online sportsbooks reviews (Don)
Sandra · July 16, 2026 at 10:19 pm
que casino paga mas rapido (Sandra) barcelona 15 euros gratis
scommesse italiani Aams · July 16, 2026 at 10:21 pm
scommesse italiani Aams italia avellino
Demo1.Fenixwebdesign.Click · July 16, 2026 at 10:26 pm
250 free spinů bonus čEské Casino 50 Kč Za Registraci (Demo1.Fenixwebdesign.Click)
Automaty za peníZe Přes google Pay · July 16, 2026 at 10:35 pm
casino Automaty za peníZe Přes google Pay pay minimální vklad
Www.odelot.es · July 16, 2026 at 10:45 pm
prediccion apuestas – http://Www.odelot.es – ruleta seguras
Skapa personligt konto · July 16, 2026 at 11:04 pm
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
score betting · July 16, 2026 at 11:10 pm
online score betting comparison
http://Www.Tanisdesign.com/the-best-online-platforms-for-rugby-world-cup-betting/ · July 17, 2026 at 12:04 am
cheltenham festival betting tips (http://Www.Tanisdesign.com/the-best-online-platforms-for-rugby-world-cup-betting/) expert review
https://Gympeniscola.com/ · July 17, 2026 at 12:05 am
best crypto sports statistic betting (https://Gympeniscola.com/) reddit
Casino En Pergamino · July 17, 2026 at 12:09 am
mejor jugada ruleta Casino En Pergamino
https://mediumaquamarine-dotterel-916337.hostingersite.com · July 17, 2026 at 12:39 am
online české casino výběr na mobil (https://mediumaquamarine-dotterel-916337.hostingersite.com) bonusový kód
isarals.bangalorebrandbuilders.com · July 17, 2026 at 12:53 am
casino vklad od 50 kč – isarals.bangalorebrandbuilders.com, Pardubice bonus bez vkladu
Salibandy Vinkit tänääN · July 17, 2026 at 2:01 am
veikkaus pori
My homepage :: Salibandy Vinkit tänääN
top betting sites offers · July 17, 2026 at 2:03 am
best top betting sites offers system for sports
is casino nb open yet · July 17, 2026 at 2:04 am
5dollar deposit casino united states, gambling statistics australia 202 and casino no deposit bonus codes canada 2021, or new is casino nb open yet no deposit bonus 2021 uk
Lawanna · July 17, 2026 at 2:33 am
horse racing results southwell yesterday (Lawanna)
racing betting sites online
Dulcie · July 17, 2026 at 2:44 am
mejor plataforma de apuestas; Dulcie, barcelona villarreal
https://Businessanalysisportal.com/vorteile-und-nachteile-von-progressiven-jackpots/ · July 17, 2026 at 3:37 am
online casino 25 euro kreditkarte (https://Businessanalysisportal.com/vorteile-und-nachteile-von-progressiven-jackpots/) casino 3 euro
mastercard
Margene · July 17, 2026 at 4:17 am
app de tips apuestas nfl (Margene) deportivas en españa
Shani · July 17, 2026 at 4:41 am
que es el stake en apuestas deportivas (Shani) campeon nba
que es 1x2 en apuestas · July 17, 2026 at 4:55 am
asiatico que es 1×2 en apuestas
Trav klampenborg i dag · July 17, 2026 at 4:58 am
sportsbetting strategi
my web-site; Trav klampenborg i dag
paginas estadisticas Apuestas deportivas · July 17, 2026 at 5:32 am
ofertas paginas estadisticas Apuestas deportivas online
pronosticos apuestas europa league · July 17, 2026 at 5:39 am
app para llevar control de pronosticos apuestas europa league
apuestas roma sevilla · July 17, 2026 at 5:44 am
casas de apuestas roma sevilla 5 euros
Jorge · July 17, 2026 at 6:00 am
300 free spinů bonus casino
my blog post :: kde hrát automaty za peníze Olomouc (Jorge)
trucos ganar Apuestas Deportivas · July 17, 2026 at 6:15 am
trucos ganar Apuestas Deportivas mlb
basketball over under wetten system · July 17, 2026 at 6:27 am
besten sportwetten anbieter
Here is my page – basketball over under wetten system
azaceramica.es · July 17, 2026 at 6:34 am
impuesto apuestas fútbol en directo, azaceramica.es, online
basketball wetten heute · July 17, 2026 at 6:37 am
beste wettanbieter ohne steuer
My web blog :: basketball wetten heute
Ascsystemy.pl · July 17, 2026 at 6:49 am
kurs bukmacher nba
my website – kwalifikacje f1 dzisiaj wyniki (Ascsystemy.pl)
Online glücksspiel schleswig-Holstein · July 17, 2026 at 6:52 am
vegas mobile casino ohne anzahlung bonus
Look at my blog :: Online glücksspiel schleswig-Holstein
https://www.intervitrine.es/estadisticas-intrigantes-en-la-historia-de-la-Nba-para-apostar/ · July 17, 2026 at 7:08 am
mejores ofertas casas casa de apuestas f1 – https://www.intervitrine.es/estadisticas-intrigantes-en-la-historia-de-la-Nba-para-apostar/, apuestas
nba basketball wett tipps · July 17, 2026 at 7:24 am
willkommensbonus ohne einzahlung wetten
Feel free to visit my site – nba basketball wett tipps
aplicaciones de apuestas online · July 17, 2026 at 7:25 am
aplicaciones de apuestas online madrid betis
https://WWW.Implantoprotesi.com/mlb-vedonlyonnin-psykologia-tunteiden-haltuun/ · July 17, 2026 at 7:25 am
veikkaus lahti
Here is my website :: vedonlyöntibonus ilman talletusta, https://WWW.Implantoprotesi.com/mlb-vedonlyonnin-psykologia-tunteiden-haltuun/,
casino 2 Euro litecoin · July 17, 2026 at 7:33 am
casino 2 Euro litecoin 25 euro
flexepin
Starcraft Live Odds · July 17, 2026 at 7:51 am
over under strategi
my blog post Starcraft Live Odds
casino na telefon bonus za registraci · July 17, 2026 at 7:57 am
mobilní casino na telefon bonus za registraci revolut
Dedra · July 17, 2026 at 8:14 am
kaikki suomalaiset vedonvälittäjä
Feel free to visit my site ravivihjeet ilmaiset –
Dedra –
Lauri · July 17, 2026 at 8:26 am
casino 5 euro kreditkarte
My webpage … no deposit bonus ohne maximalen gewinn – Lauri,
apuestas Deportivas app · July 17, 2026 at 8:30 am
pronosticos de apuestas Deportivas app
para hoy
apuestas seguras en la ruleta · July 17, 2026 at 8:32 am
linea de dinero apuestas seguras en la ruleta
Brasil Peru Apuestas · July 17, 2026 at 8:45 am
mejores canales de Brasil Peru Apuestas
telegram
shop.techswitchcf.com · July 17, 2026 at 8:50 am
mathematische wettstrategie
Feel free to visit my web site; basketball wetten [shop.techswitchcf.com]
Wett Tipps Basketball Nba · July 17, 2026 at 8:56 am
sportwetten forum strategie
My website – Wett Tipps Basketball Nba
Ocell.Es · July 17, 2026 at 9:14 am
qué es un momio en las Casas De Apuestas Deportivas En Sevilla
(Ocell.Es)
ravikertoimet pori · July 17, 2026 at 9:37 am
ravivihjeet oulu
Feel free to surf to my blog post: ravikertoimet pori
Sportodds FöRklaring · July 17, 2026 at 9:41 am
spela på allsvenskan
Here is my web blog; Sportodds FöRklaring
casino s vklad 100 Kč · July 17, 2026 at 9:49 am
casino s vklad 100 Kč blackjack
s nízkým vkladem
Brenna · July 17, 2026 at 10:09 am
consejos cuotas de apuestas deportivas – Brenna, apuestas de futbol
para hoy
Jefferey · July 17, 2026 at 10:14 am
foro de apuestas de tenis (Jefferey) liverpool barcelona
casino apple pay ab 4 Euro · July 17, 2026 at 10:18 am
wahrscheinlichkeiten black jack
my homepage … casino apple pay ab 4 Euro
online casino ab 100 euro kreditkarte · July 17, 2026 at 10:29 am
online casino ab 100 euro kreditkarte 10 euro einzahlen 200 euro bonus
Basketball VerläNgerung Wetten · July 17, 2026 at 10:31 am
neue sportwetten seiten
My blog post; Basketball VerläNgerung Wetten
WWW.Obradordesabores.es · July 17, 2026 at 10:44 am
apuestas Combinadas mundial (http://WWW.Obradordesabores.es) deportivas
bonos de bienvenida
casino Girocard schnelle Auszahlung · July 17, 2026 at 10:47 am
casino Girocard schnelle Auszahlung zweiteinzahlungsbonus 2026
Casino Gratis Por Registro · July 17, 2026 at 10:48 am
apostar al rojo y al negro Casino Gratis Por Registro
casino Ab 18 dortmund · July 17, 2026 at 11:13 am
sicherstes online casino Ab 18 dortmund
tunnetut urheiluvedonlyönti sivustot · July 17, 2026 at 11:17 am
vedonlyönti pienellä talletuksella
Feel free to visit my web page – tunnetut urheiluvedonlyönti sivustot
Trent · July 17, 2026 at 11:27 am
apuestas promociones en casa de apuestas (Trent) futbol
sin dinero
software predicción apuestas deportivas · July 17, 2026 at 11:37 am
software predicción apuestas deportivas argentina campeon del mundo
Live Resultater Sport · July 17, 2026 at 12:01 pm
spille på Live Resultater Sport med trustly
matched Betting website · July 17, 2026 at 12:01 pm
what does handicap mean in matched Betting website
Lino · July 17, 2026 at 12:19 pm
que es tipster en apuestas (Lino) puntos tarjetas
https://www.artesanadelavida.com/como-gestionar-tus-apuestas-con-disciplina/ · July 17, 2026 at 12:26 pm
nuevas casas casa de apuestas españa (https://www.artesanadelavida.com/como-gestionar-tus-apuestas-con-disciplina/) apuestas 2025
Badminton tips I dag · July 17, 2026 at 12:29 pm
største bettingsider
Also visit my web site :: Badminton tips I dag
tenis wyniki na żywo live · July 17, 2026 at 12:29 pm
bukmacher bez depoztyu
my site … tenis wyniki na żywo live
Marco · July 17, 2026 at 12:40 pm
casino online sin dinero – Marco, en bugambilias
Amanda · July 17, 2026 at 12:41 pm
sportwetten österreich anbieter
My blog post basketball wetten erklärung (Amanda)
Iesalpujarra.es · July 17, 2026 at 1:14 pm
real madrid vs sevilla estrategia tenis de mesa
apuestas – Iesalpujarra.es –
Pagina apuestas gratis · July 17, 2026 at 1:26 pm
Pagina apuestas gratis de sistema
dagens Odds · July 17, 2026 at 2:24 pm
underholdning dagens Odds
betting Bankroll strategi · July 17, 2026 at 2:25 pm
indbetalingsbonus betting Bankroll strategi
Oliva · July 17, 2026 at 2:49 pm
ufc bonos bienvenida apuestas – Oliva
–
Pagina apuestas Futbol · July 17, 2026 at 3:15 pm
Pagina apuestas Futbol
sevilla gana la liga
Lourdes · July 17, 2026 at 3:24 pm
live score for betting
Feel free to surf to my web blog: free bet (Lourdes)
calcular Apuestas sistema · July 17, 2026 at 3:48 pm
juegos de calcular Apuestas sistema online
Marylou · July 17, 2026 at 3:56 pm
guide to matched betting company offers, Marylou,
Jonas · July 17, 2026 at 4:11 pm
vinder odds håndbold em i dag
Also visit my web page – betting uden rofus (Jonas)
Que es asiático en apuestas · July 17, 2026 at 4:14 pm
calculadora stake Que es asiático en apuestas
Bitcoin wedden Platformen · July 17, 2026 at 4:16 pm
nieuwe Bitcoin wedden Platformen eu
Apuestas En Linea Argentina · July 17, 2026 at 4:22 pm
combinadas Apuestas En Linea Argentina hoy
Http://Medicalelessi-COM.Stackstaging.Com/2025/02/11/Betydningen-Af-At-Have-Kvindelige-Rollemodeller-I-Sporten/ · July 17, 2026 at 4:33 pm
spil danmark kroatien
My blog; Betting Uden Registrering – http://Medicalelessi-COM.Stackstaging.Com/2025/02/11/Betydningen-Af-At-Have-Kvindelige-Rollemodeller-I-Sporten/,
Plinko Mit Hoher auszahlung · July 17, 2026 at 4:45 pm
online casino Plinko Mit Hoher auszahlung klarna bezahlen
top 100 sportsbook · July 17, 2026 at 4:54 pm
betting on line
my web site; top 100 sportsbook
Waldo · July 17, 2026 at 4:54 pm
casas de apuestas en españa online (Waldo) en mexico
online
Tips deportivos Apuestas · July 17, 2026 at 5:01 pm
Tips deportivos Apuestas deportivas app
Http://Www.Trazadainvisible.Es/ · July 17, 2026 at 5:51 pm
Casino Rojas Keszitese (http://Www.Trazadainvisible.Es/) san nicolás de los
arroyos
casinos que te dan dinero sin deposito · July 17, 2026 at 5:52 pm
casino en un crucero
Here is my blog post – casinos que te dan dinero sin deposito
Marcella · July 17, 2026 at 6:07 pm
best betting on fouls, Marcella, tips apps android
Casas De Apuestas En Sevilla · July 17, 2026 at 6:22 pm
Casas De Apuestas En Sevilla girona
casas de apuestas venezuela · July 17, 2026 at 6:49 pm
bonos casas de apuestas venezuela deportivas
Https://Www.Graffipictures.Com · July 17, 2026 at 6:52 pm
Cash Out Betting Strategy (https://Www.Graffipictures.Com) sites you can use credit
card
cz Casino OvěřEné · July 17, 2026 at 6:53 pm
cz Casino OvěřEné poker za peníze
https://lindsayscarpello.com · July 17, 2026 at 7:03 pm
weddenschap trucs 2026
my webpage: aanbieders Online wedden (https://lindsayscarpello.com)
Apuestas Futbol Sala · July 17, 2026 at 8:08 pm
Apuestas Futbol Sala nfl semana 4
que es handicap 0 en apuestas · July 17, 2026 at 8:51 pm
comparador que es handicap 0 en apuestas
deportivas
Merrill · July 17, 2026 at 9:12 pm
bookmaker job
Check out my webpage – sure bets today (Merrill)
donde hacer apuestas de futbol · July 17, 2026 at 9:41 pm
donde hacer apuestas de futbol estadisticas
Https://Vpiseguridad.Com/ · July 17, 2026 at 10:03 pm
hedge Professional Betting Advice (https://Vpiseguridad.Com/) system
Atlasinsulationfl.com · July 17, 2026 at 10:16 pm
kombi gevinst beregner
Also visit my homepage … vinder odds Superligaen (Atlasinsulationfl.com)
Mejores Apuestas para hoy · July 17, 2026 at 10:46 pm
que es handicap en Mejores Apuestas para hoy baloncesto
Nan · July 17, 2026 at 11:00 pm
que significa cash out en app casas de apuestas (Nan)
Binance注册奖金 · July 17, 2026 at 11:08 pm
Your article helped me a lot, is there any more related content? Thanks! https://www.binance.com/register?ref=IXBIAFVY
apuestas Del mundial · July 17, 2026 at 11:12 pm
comparador de apuestas Del mundial deportivas
betting Explained Each way · July 17, 2026 at 11:15 pm
betting Explained Each way exchange explained
consejos para hacer apuestas deportivas · July 17, 2026 at 11:22 pm
donde consejos para hacer apuestas deportivas
apuestas deportivas
pronosticos y Apuestas deportivas · July 17, 2026 at 11:28 pm
pronosticos y Apuestas deportivas la liga santander
sg vape · July 18, 2026 at 12:01 am
sg vape hub
SGVape Hub: Pure Nicotine Vapes with Fast Same Day Delivery in Singapore
At SGVape Hub, we make it easy to enjoy premium SGVape products with speed and convenience across Singapore. We offer pure nicotine vapes, offering same day delivery and easy cash on delivery, making it simple to get your products fast.
Our collection offers trusted brands such as Lana, RELX, Vapetape, Elfbar, Snowwolf, SP2, and ONEM. Every product is carefully selected to deliver a premium vaping experience with dependable performance.
Customers can receive exclusive savings with every order. Get $5 OFF when purchasing six or more pieces, $10 OFF on 11 pieces or more, and free delivery for orders above $300.
Premium SGVape Devices
Discover some of Singapore’s best-selling vape devices available for same day delivery.
Our collection includes Vapetape Engage, Vapetape Offgrid, Vapetape Offgrid Reload, ONEM Reload Cartridge, Lana Ultra II 16,000 Puffs, Lana Touch 32,000 Puffs, Lana Pen Plus 9,000 Puffs, RELX Infinity 2, RELX Creator 22,000 Puffs, Elfbar Ice King 40,000 Puffs, and Snowwolf 16,000 Puffs.
Whether you prefer disposable vape devices, open pod systems, or compatible cartridges, SGVape Hub provides a wide range of products to match your vaping style.
Clean, Legal, and Pure Vape Products
Your safety is always our priority. SGVape Hub sells only clean, legal, and pure nicotine vape products.
We never sell K pods or products containing illegal substances. Every vape device in our collection is carefully chosen to meet our quality standards, providing peace of mind when choosing their preferred device.
Featured Product: Vapetape Engage
The Vapetape Engage is created for vapers who want customizable vaping in one device.
Key features include a powerful 2600mAh battery, adjustable wattage up to 50W, a refillable open pod system, dual cartridge compatibility, a 0.4? cartridge for bigger vapor production, and a 0.6? cartridge for a smoother draw with enhanced flavor.
Simply refill with your preferred e-liquid and fine-tune the device to match your vaping style.
Why Choose SGVape Hub
SGVape Hub combines premium products with fast local service to create a simple shopping experience.
Benefits include fast same day delivery across Singapore, cash on delivery, pure nicotine vape products only, trusted vape brands, competitive pricing, bulk order discounts, and fast, reliable customer service.
Whether you’re replacing your favorite disposable vape or upgrading to a refillable pod system, SGVape Hub supplies authentic SGVape products quickly, safely, and hassle-free throughout Singapore.
oddset Forhandler aalborg · July 18, 2026 at 2:13 am
vinder odds serie a i dag
Also visit my homepage; oddset Forhandler aalborg
velkomstbonus odds · July 18, 2026 at 2:37 am
oddset horsens
Feel free to surf to my web page – velkomstbonus odds
Timmy · July 18, 2026 at 2:40 am
online nové casino otočky zdarma za registraci (Timmy)
750 kč bonus
app para aposta Esportiva · July 18, 2026 at 2:53 am
apostas online com bonus
my page :: app para aposta Esportiva
wedden Trucs Bundesliga · July 18, 2026 at 2:58 am
hoe werkt wedden Trucs Bundesliga op sport
Nederlandse E-wedden · July 18, 2026 at 3:16 am
online sportwedden
Also visit my web blog :: Nederlandse E-wedden
Free Bets For Cheltenham Today · July 18, 2026 at 3:36 am
how does a wheel bet work in horse racing
Feel free to surf to my site Free Bets For Cheltenham Today
gratis csgo Wedden sites 2026 · July 18, 2026 at 3:42 am
top 5 online sports gratis csgo Wedden sites 2026
aanbieder Van virtuele wedden · July 18, 2026 at 3:44 am
betrouwbare online aanbieder Van virtuele wedden
Tilly · July 18, 2026 at 4:03 am
bonos gratis apuestas deportivas de tenis – Tilly,
apuestas argentina vs Australia · July 18, 2026 at 4:05 am
apuestas argentina vs Australia atlético de madrid real madrid
Online Sportweddenschappen · July 18, 2026 at 4:06 am
golf wedden registratie
Here is my blog post – Online Sportweddenschappen
Www.Hpvdiagnostics.Com · July 18, 2026 at 4:10 am
baixa casas de EstratéGia E MéTodo Apostas Tempo
[http://Www.Hpvdiagnostics.Com]
what casino chips are worth money · July 18, 2026 at 4:30 am
how much is a gambling license in canada, united statesn poker and win real money online what casino chips are worth money usa, or top online pokies nz
how To make Money playing games in South Africa · July 18, 2026 at 4:32 am
10 free spins no deposit casino uk, where can i play poker online how To make Money playing games in South Africa australia and online casino australia free spins sign up, or deposit 10 get
usa
horse racing lay betting explained · July 18, 2026 at 4:34 am
what is a boxed bet in horse racing lay betting explained racing
casino minimální vklad 50 kč bitcoin · July 18, 2026 at 5:15 am
nejlepší evropská ruleta casino minimální vklad 50 kč bitcoin
Top spread betting Brokers · July 18, 2026 at 5:19 am
Top spread betting Brokers sites that offer
cash out
apuestas Online Opiniones · July 18, 2026 at 5:23 am
consejos apuestas Online Opiniones deportivas combinadas
https://Goodquestionashtabula.com/het-kiezen-van-je-trouwringen-trends-en-stijlen/ · July 18, 2026 at 5:29 am
advies beste wedden, https://Goodquestionashtabula.com/het-kiezen-van-je-trouwringen-trends-en-stijlen/, voor geld vandaag net
Planilha Apostas Esportivas Odds · July 18, 2026 at 5:29 am
Planilha Apostas Esportivas Odds desportivas analise
https://Www.ambarquitectura.es · July 18, 2026 at 5:36 am
codigo promocional de marca apuestas deportivas dinero ficticio (https://Www.ambarquitectura.es)
Apuestas Tenis itf · July 18, 2026 at 5:36 am
ofertas Apuestas Tenis itf online
goalscorer betting tips · July 18, 2026 at 5:38 am
top 10 goalscorer betting tips sites
apuestas final libertadores · July 18, 2026 at 5:39 am
que es la linea de gol en apuestas final libertadores
Licencas apostas · July 18, 2026 at 5:47 am
Licencas apostas online como fazer
goede sportweddenschappen · July 18, 2026 at 5:57 am
virtuele wedden paypal
My web blog … goede sportweddenschappen
Maurine · July 18, 2026 at 5:59 am
online poker that takes united statesn express, blackjack online casino
australia and arcade slot machines for sale uk, or 21 dukes casino login
Feel free to surf to my web blog … what is the return on roulette (Maurine)
casa de apuestas que regalan Dinero · July 18, 2026 at 6:07 am
pronóstico casa de apuestas que regalan Dinero apuestas para hoy
da pra viver so de apostas esportivas · July 18, 2026 at 6:27 am
em quem apostar hoje
My blog post da pra viver so de apostas esportivas
http://www.u146774p138629.web0149.zxcs-klant.nl · July 18, 2026 at 6:49 am
bookmaker wedden de beste [http://www.u146774p138629.web0149.zxcs-klant.nl] wedden promotiecode
Wedden Sites Paypal · July 18, 2026 at 7:08 am
advies e-Wedden Sites Paypal
Carin · July 18, 2026 at 7:20 am
mejores paginas de apuestas csgo – Carin, ofertas casas apuestas
onde Apostar Esports · July 18, 2026 at 7:23 am
todos sites de apostas
My website :: onde Apostar Esports
site de apostas Com paysafecard · July 18, 2026 at 7:46 am
site de apostas Com paysafecard ténis hoje
Lindsay · July 18, 2026 at 7:54 am
gratis wedden voor geld 2026 (Lindsay) geld wedden
Waar Wedden Op Bookmaker · July 18, 2026 at 8:03 am
Waar Wedden Op Bookmaker tips sportcompetities
Roulette Cake · July 18, 2026 at 8:27 am
usa usd 200 no deposit bonus 200 free spins 2021, play free australian poker machines and bonausaa slot volatility, or united kingdom no deposit casino
bonuses
my web site – Roulette Cake
Shella · July 18, 2026 at 8:31 am
barcelona vs sevilla pronósticos apuestas deportivas tenis (Shella)
Apuestas Beisbol · July 18, 2026 at 8:33 am
calculo de Apuestas Beisbol deportivas
Ingrid · July 18, 2026 at 8:37 am
dicas de apostas quando apostar em empate – Ingrid, cavalos
handicap apuestas futbol explicacion · July 18, 2026 at 8:41 am
estadisticas de futbol handicap apuestas futbol explicacion
estrategias para Apuestas de futbol · July 18, 2026 at 8:48 am
las mejores apuestas deportivas estrategias para Apuestas de futbol hoy
casas De Apuestas deportivas con paypal · July 18, 2026 at 8:53 am
como funciona handicap casas De Apuestas deportivas con paypal
Garden.Wpfreebuild.Com · July 18, 2026 at 8:59 am
Apuestas De Futbol En Vivo (Garden.Wpfreebuild.Com) online net
Shalanda · July 18, 2026 at 9:23 am
goede wedden app
Stop by my web blog nfl online weddenschappen; Shalanda,
Estrategias De Apostas Esportivas · July 18, 2026 at 9:28 am
apostas para o dia Estrategias De Apostas Esportivas hoje
Gwen · July 18, 2026 at 9:46 am
goede wedden trucs 2026 (Gwen)
bookmaker trucs 2026
esse cigarettes · July 18, 2026 at 10:11 am
esse cigarettes
The Australia Cig Delivery website is an online tobacco shop operating throughout Australia. Launched in 2024, the store is dedicated to offering dependable service, affordable prices, and Australia-wide delivery for customers aged 18 and over.
The website offers reliable nationwide shipping, with orders dispatched the same day available for orders completed before 5:00 am (GMT+11). The company uses 100% discreet packaging for customer privacy.
Several payment methods are available, including Wise, PayPal, bank transfer, and USDT. The website provides secure payment and dependable shipping, allowing customers to order online with confidence.
The store stocks a wide selection of well-known cigarette brands, including Dunhill, Marlboro, Manchester, Double Happiness, Benson & Hedges, Mevius, Seven Star, and Mac. The product range includes various cigarette styles and tobacco blends for different smoking preferences.
The Marlboro brand is known around the world for its authentic flavor and premium tobacco blend. The range features Marlboro Red, Gold, and Menthol, providing different taste options.
Manchester are appreciated for their clean finish and enjoyable smoking experience. The collection includes multiple blends and menthol options.
The Double Happiness brand has earned recognition for its distinctive flavor and authentic heritage. With Asian origins, the brand remains popular among adult smokers who prefer its traditional tobacco flavor.
The Benson & Hedges brand is recognized for its premium quality and smooth smoking experience. The brand has built a strong global reputation for carefully selected tobaccos and consistent quality.
Dunhill is considered a premium tobacco brand, combining carefully selected tobacco with a refined flavor profile. The brand has long been recognized for premium standards and craftsmanship.
According to information on the website all products are sourced from trusted suppliers and are described as 100% authentic. The store states that products are sold only to customers aged 18+ while providing secure ordering, reliable delivery, and customer-focused service.
Apuestas Campeon Copa America · July 18, 2026 at 10:16 am
Apuestas Campeon Copa America en stake
are there casinos in gulf shores · July 18, 2026 at 10:34 am
best paying poker machines united states, emu casino united kingdom
and bet uk casino, or no deposit mobile casino australia
Also visit my web page – are there casinos in gulf shores
Https://alltravelsenergy-backup.Techzenau.com/apuestas-en-la-formacion-de-equipos-Analisis-y-perspectivas/ · July 18, 2026 at 11:07 am
mlb apuestas (https://alltravelsenergy-backup.Techzenau.com/apuestas-en-la-formacion-de-equipos-Analisis-y-perspectivas/) sin dinero
Bonos En Casa De Apuestas · July 18, 2026 at 11:12 am
Bonos En Casa De Apuestas nfl pronosticos
apuestas Beisbol Venezolano · July 18, 2026 at 11:24 am
comparativa apuestas Beisbol Venezolano deportivas
I9Desk.Com · July 18, 2026 at 11:38 am
bookmakers casas Qual O Melhor Mercado De Apostas (I9Desk.Com) apostas
https://www.Avignongourmetours.com/boatos-e-verdades-sobre-a-mega-sena/ · July 18, 2026 at 11:53 am
esporte online apostas esportivas vip (https://www.Avignongourmetours.com/boatos-e-verdades-sobre-a-mega-sena/)
Madeline · July 18, 2026 at 11:57 am
united statesn gambling news, bet365 new zealandn roulette
instructions and online pokies canada jokaroom, or what online gambling is legal in united states
Review my web site – epiphone casino worn review (Madeline)
Jorja · July 18, 2026 at 11:57 am
united statesn roulette wheel play, on line graton casino benefits
[Jorja] canada and bonausaa slot volatility, or registration bonus
casino usa
Https://Pensionteima.Es/ · July 18, 2026 at 1:40 pm
App Pronosticos Apuestas Deportivas – https://Pensionteima.Es/ – online
bono bienvenida
legal gambling nyc · July 18, 2026 at 1:45 pm
android casino united kingdom, canadian online pokies free spins and new casino site uk 2021, or top paying online casinos united states
Feel free to visit my webpage :: legal gambling nyc
Asa · July 18, 2026 at 1:53 pm
casinos in windsor canada, casino online free spins no deposit uk and poker for
real money in usa, or how to almost always win at roulette (Asa)
to play pokies in canada
Laverne · July 18, 2026 at 1:54 pm
bono bienvenida calculadora de cuotas de apuestas (Laverne)
casinos en mallorca · July 18, 2026 at 1:57 pm
casino bono tiradas gratis
Also visit my web blog: casinos en mallorca
que significa over en las Apuestas · July 18, 2026 at 1:58 pm
consejos para que significa over en las Apuestas de futbol
apuestas Liverpool Barcelona · July 18, 2026 at 2:01 pm
significado de stake en apuestas Liverpool Barcelona
associaciobonsaidecastello.Es · July 18, 2026 at 2:08 pm
tipster de apuestas Online Nuevas (associaciobonsaidecastello.Es)
listado apuestas deportivas prediccion · July 18, 2026 at 2:15 pm
listado apuestas deportivas prediccion nba hoy jugadores
https://leyvavendingmadrid.es/sin-categoria/importancia-del-analisis-de-la-racha-de-los-equipos-en-apuestas/ · July 18, 2026 at 2:36 pm
casa de casino apuestas en linea, https://leyvavendingmadrid.es/sin-categoria/importancia-del-analisis-de-la-racha-de-los-equipos-en-apuestas/, de futbol
www.metalfarm.es · July 18, 2026 at 2:38 pm
que es linea de dinero en apuestas deportivas España [http://www.metalfarm.es]
Stake 10 Apuestas · July 18, 2026 at 2:51 pm
sitios de Stake 10 Apuestas mexico
Pronosticos apuestas deportivas nba · July 18, 2026 at 2:56 pm
pronosticador de Pronosticos apuestas deportivas nba
Apuestas playoff Ascenso · July 18, 2026 at 3:09 pm
argentina vs chile Apuestas playoff Ascenso
https://Papyruss.Jtaborbroker.Com/ · July 18, 2026 at 3:19 pm
online betting sites new (https://Papyruss.Jtaborbroker.Com/) sites that accept paypal
mejores paginas de apuestas deportivas · July 18, 2026 at 3:35 pm
que es una combinada en mejores paginas de apuestas deportivas
Tisha · July 18, 2026 at 3:37 pm
online casinos licensed in usa, united statesn poker and does united kingdom have a gambling problem,
or european roulette layout usa
my web-site; 7red casino inloggen – Tisha,
Avmontmar.Es · July 18, 2026 at 3:43 pm
pronostico real madrid vs real sociedad apuestas [Avmontmar.Es] nba
Que Significa El En Las Apuestas · July 18, 2026 at 3:47 pm
consejos Que Significa El En Las Apuestas
Https://Www.Caip-Eeb.Es/2026/07/13/Los-Errores-Mas-Comunes-En-Las-Apuestas-De-Futbol-Y-Como-Evitarlos/ · July 18, 2026 at 3:55 pm
casa de Calculadora Stake Apuestas (https://Www.Caip-Eeb.Es/2026/07/13/Los-Errores-Mas-Comunes-En-Las-Apuestas-De-Futbol-Y-Como-Evitarlos/) colombia
Anderson · July 18, 2026 at 4:03 pm
estrategia bonos apuestas sin deposito (Anderson) baloncesto
apuestas paises bajos ecuador · July 18, 2026 at 4:04 pm
como ganar en apuestas paises bajos ecuador deportivas
tipos de apuestas hipodromo · July 18, 2026 at 4:07 pm
tipos de apuestas hipodromo futbol
apuestas athletic · July 18, 2026 at 4:10 pm
copa libertadores apuestas athletic deportivas
Apuestas Uruguay · July 18, 2026 at 4:13 pm
marca Apuestas Uruguay 20 euros gratis
apuestas Deportivas Mlb Hoy · July 18, 2026 at 4:23 pm
apuestas Deportivas Mlb Hoy tercera division
predicciones apuestas deportivas gratis · July 18, 2026 at 4:25 pm
casas de predicciones apuestas deportivas gratis en colombia
Lesli · July 18, 2026 at 4:37 pm
nba prorroga baloncesto apuestas – Lesli – deportivas
app de Apuestas Android · July 18, 2026 at 4:42 pm
programa para hacer app de Apuestas Android deportivas
Sheldon · July 18, 2026 at 5:02 pm
casa de casas apuestas bono sin deposito (Sheldon) baloncesto
apuestas mvp Nfl · July 18, 2026 at 5:04 pm
que significa 4.5 goles en apuestas mvp Nfl
Horace · July 18, 2026 at 5:10 pm
juegos de apuestas (Horace) deportivas y casino online
apuestas argentina francia mundial · July 18, 2026 at 5:32 pm
apuestas argentina francia mundial futbol peru
Dedra · July 18, 2026 at 5:37 pm
calculadora de apuestas seguras (Dedra)
nfl semana 4
juegos de casinos gratis sin descargar maquinas nuevas · July 18, 2026 at 5:41 pm
casino internacional online
Check out my blog :: juegos de casinos gratis sin descargar maquinas nuevas
apuestas handicap nfl · July 18, 2026 at 5:44 pm
argentina vs colombia apuestas handicap nfl
http://Apuestasf1.com · July 18, 2026 at 5:51 pm
mejor casa de apuestas barca girona; http://Apuestasf1.com, online mexico
apuestas multiples futbol · July 18, 2026 at 5:56 pm
mejores casas de apuestas multiples futbol españa
casa de apuestas en perú · July 18, 2026 at 6:08 pm
estadisticas casa de apuestas en perú apuestas
Velma · July 18, 2026 at 6:11 pm
online české casino výběr na bitcoin – Velma, deposit revolut
Https://mybalance.es/ · July 18, 2026 at 6:14 pm
copa del rey betis Madrid apuestas, https://mybalance.es/,
Gregg · July 18, 2026 at 6:16 pm
que significa stake 100 en apuestas (Gregg) liga de campeones
apuestas brasil vs Colombia · July 18, 2026 at 6:19 pm
mejores paginas para apuestas brasil vs Colombia deportivas
https://www.behumanleadership.es/2025/10/02/aspectos-legales-De-Apuestas-en-futbol-En-diferentes-paises/ · July 18, 2026 at 6:27 pm
apuestas sistema; https://www.behumanleadership.es/2025/10/02/aspectos-legales-De-Apuestas-en-futbol-En-diferentes-paises/, deportivas argentina
Que Es Doble Oportunidad En Las Apuestas · July 18, 2026 at 6:28 pm
casa Que Es Doble Oportunidad En Las Apuestas mundial
https://effectorx.Com/ · July 18, 2026 at 6:46 pm
hrát automaty přes trustly
Check out my website :: online casino minimální vklad (https://effectorx.Com/)
canales De apuestas gratis · July 18, 2026 at 6:54 pm
canales De apuestas gratis golf
pagina de apuestas gratis · July 18, 2026 at 6:55 pm
pronostico pagina de apuestas gratis apuestas
casas De apuestas españa licencia · July 18, 2026 at 7:00 pm
casa casas De apuestas españa licencia apuestas
eurocopa
Apuestas Del Dia · July 18, 2026 at 7:01 pm
Apuestas Del Dia mundial favoritos
Mejores Paginas Apuestas De Futbol · July 18, 2026 at 7:08 pm
favorito Mejores Paginas Apuestas De Futbol champions
Jake · July 18, 2026 at 7:13 pm
apuestas plataforma – Jake – handicap nba
pagina de Apuestas · July 18, 2026 at 7:14 pm
mejores casas pagina de Apuestas apuestas superdeporte
Apuestas Carrera De Galgos Nocturnas · July 18, 2026 at 7:17 pm
linea de Apuestas Carrera De Galgos Nocturnas
mlb
Puntos Tarjetas apuestas · July 18, 2026 at 7:33 pm
paginas Puntos Tarjetas apuestas gratis
predicciones de futbol para apuestas · July 18, 2026 at 7:51 pm
plataforma predicciones de futbol para apuestas deportivas
Kendrick · July 18, 2026 at 8:11 pm
nové casino vklad sms
Feel free to visit my page … hrát živá ruleta za
peníze (Kendrick)
Arleen · July 18, 2026 at 8:12 pm
favorito champions apuestas (Arleen) nba gratis
Apuestas f1 las vegas · July 18, 2026 at 8:35 pm
que es el handicap en Apuestas f1 las vegas
como funciona el handicap en apuestas · July 18, 2026 at 8:35 pm
que es stake 30 como funciona el handicap en apuestas apuestas
https://www.Agricolaportera.com/ · July 18, 2026 at 8:40 pm
aplicaciones de bonos gratis apuestas (https://www.Agricolaportera.com/) de fútbol
Https://www.corteyperforacionesladama.Com/ · July 18, 2026 at 9:05 pm
100 200 free spinů za registraci 2026 (https://www.corteyperforacionesladama.Com/)
spinů bez vkladu 2026
Apuestas Argentina Holanda · July 18, 2026 at 9:20 pm
Apuestas Argentina Holanda villarreal barcelona
Hannah · July 18, 2026 at 9:31 pm
apuestas nfl pronosticos – Hannah – dobles y triples
https://www.carroceriasperianes.es/2021/09/15/cuando-apostar-en-la-europa-league-mejores-momentos/ · July 18, 2026 at 10:17 pm
trucos apuestas deportivas Futbol, https://www.carroceriasperianes.es/2021/09/15/cuando-apostar-en-la-europa-league-mejores-momentos/, super bowl favorito
Casas de apuestas ofertas · July 18, 2026 at 10:35 pm
como hacer Casas de apuestas ofertas combinadas
apuestas Seguras tenis · July 18, 2026 at 11:19 pm
mejor estrategia apuestas Seguras tenis futbol
juegos Olimpicos Apuestas · July 18, 2026 at 11:36 pm
aplicaciones para hacer juegos Olimpicos Apuestas
pronostico apuestas deportivas Hoy · July 18, 2026 at 11:41 pm
pronostico apuestas deportivas Hoy sevilla madrid
online casino 500 free spinů · July 18, 2026 at 11:44 pm
online casino 500 free spinů platba trustly
zahraniční casino vklad mobil · July 19, 2026 at 1:20 am
zahraniční casino vklad mobil nízký
vklad
mejor aplicacion apuestas deportivas · July 19, 2026 at 1:51 am
mejor aplicacion apuestas deportivas playoff nba
apuestas william hill partidos de hoy · July 19, 2026 at 2:36 am
apuestas william hill partidos de hoy deportivas online peru
Franchesca · July 19, 2026 at 3:02 am
was ist kombiwette
Also visit my web page: basketball über unter wetten overtime (Franchesca)
bono bienvenida apuestas deportivas · July 19, 2026 at 3:08 am
estrategias para bono bienvenida apuestas deportivas deportivas
casas de Apuestas real madrid · July 19, 2026 at 3:11 am
casas de Apuestas real madrid deportivas partido
suspendido
mejores sitios de apuestas deportivas · July 19, 2026 at 3:16 am
mejores sitios de apuestas deportivas partidos
futbol
https://www.eavisiona.es/2026/07/13/como-las-fusiones-de-equipos-sacuden-la-j-league-y-alteran-el-Panorama-de-apuestas/ · July 19, 2026 at 3:25 am
bonos gratis apuestas (https://www.eavisiona.es/2026/07/13/como-las-fusiones-de-equipos-sacuden-la-j-league-y-alteran-el-Panorama-de-apuestas/)
carrera de galgos fin de semana
Maik · July 19, 2026 at 3:27 am
carrera de caballos apuestas (Maik) sin deposito
minimo
basketball Wetten overtime · July 19, 2026 at 3:32 am
tipps basketball Wetten overtime heute
Marcela · July 19, 2026 at 3:33 am
basketball wetten overtime (Marcela) bonus
ohne einzahlung
Linea De Dinero apuestas · July 19, 2026 at 3:35 am
Linea De Dinero apuestas caballos colocado
Https://Comerensitges.Com/ · July 19, 2026 at 3:46 am
Apuestas Para Ganar La Eurocopa (https://Comerensitges.Com/) gratis regalos
Nida · July 19, 2026 at 4:03 am
apuestas casa de apuestas cerca de mi – Nida, golf
Estelle · July 19, 2026 at 4:11 am
juegos de casino gratis slots (Estelle)
de casino ganar dinero real
Larae · July 19, 2026 at 4:12 am
mejor app stake apuestas app (Larae)
https://Hocksengmarine.Com.sg/die-besten-buchmacher-fur-direktes-einzahlen-per-bank/ · July 19, 2026 at 4:15 am
sportwetten prognosen heute
Review my webpage was heißt hc 0 7 5 2 bei basketball wetten [https://Hocksengmarine.Com.sg/die-besten-buchmacher-fur-direktes-einzahlen-per-bank/]
Basketball-Wetten · July 19, 2026 at 4:25 am
wetten spiele
my site – Basketball-Wetten
basketball wetten erkläRung · July 19, 2026 at 4:27 am
basketball wetten erkläRung halbzeit
endstand
apuestas Real madrid atletico de madrid · July 19, 2026 at 4:30 am
cuotas apuestas Real madrid atletico de madrid nba
basketball Pro B Wetten · July 19, 2026 at 4:40 am
wettquoten bielefeld stuttgart
Here is my web page basketball Pro B Wetten
Basketball Punkte Wetten · July 19, 2026 at 4:44 am
sportwetten tipps strategien
Feel free to visit my page – Basketball Punkte Wetten
basketball wetten besser als fußBall · July 19, 2026 at 4:46 am
beste sportwetten tipps
Visit my blog post … basketball wetten besser als fußBall
como hacer apuestas de futbol seguras · July 19, 2026 at 4:57 am
nuevas como hacer apuestas de futbol seguras
mejores sitios apuestas · July 19, 2026 at 4:58 am
bono sin deposito mejores sitios apuestas deportivas
Quincy · July 19, 2026 at 5:09 am
echtgeld slots progressive jackpots
Here is my blog post :: casino 75 euro einzahlen 225 euro spielen [Quincy]
apuestas para hoy futbol · July 19, 2026 at 5:09 am
apuestas para hoy futbol deportivas en linea
Enrique · July 19, 2026 at 5:17 am
tips de pronosticos apuestas deportivas foro; Enrique, de futbol
https://www.Gabaldo.Com/ · July 19, 2026 at 5:20 am
wettbüro bielefeld
My web-site :: basketball wetten Tips – https://www.Gabaldo.Com/,
software predicción apuestas deportivas · July 19, 2026 at 5:20 am
que es linea de gol software predicción apuestas deportivas
Homer · July 19, 2026 at 5:26 am
apuestas caballos sanlucar de barrameda – Homer – francia
argentina
mejores casas de apuestas México · July 19, 2026 at 5:37 am
betis sevilla mejores casas de apuestas México
juegos de apuestas para ganar dinero real casino · July 19, 2026 at 5:37 am
juegos de apuestas para ganar dinero real casino en buta ranquil
mejor pagina apuestas futbol · July 19, 2026 at 5:40 am
mejor pagina apuestas futbol caballos madrid
Online Casino Einzahlungsbonus Paysafe · July 19, 2026 at 5:42 am
slots eps einzahlung
Also visit my blog; Online Casino Einzahlungsbonus Paysafe
casas de Apuestas ingreso minimo · July 19, 2026 at 5:50 am
mejor casa casas de Apuestas ingreso minimo apuestas para tenis
wett Tipps basketball · July 19, 2026 at 6:00 am
sicher wetten
Visit my page … wett Tipps basketball
online casino Mit mifinity einzahlen · July 19, 2026 at 6:02 am
beste online casino Mit mifinity einzahlen automatenspiele casinos
juegos para ganar dinero en españa sin invertir casino online · July 19, 2026 at 6:04 am
juegos para ganar dinero en españa sin invertir casino online de casino online gratis en español
tragamonedas
Paginas de apuestas que aceptan paypal · July 19, 2026 at 6:05 am
mejor casa Paginas de apuestas que aceptan paypal apuestas en méxico
Http://For-Your-Soul.Tibwluulju-Wg96Gwxgm4Oy.P.Temp-Site.Link/ · July 19, 2026 at 6:07 am
nové Casino Platba Mobil (http://For-Your-Soul.Tibwluulju-Wg96Gwxgm4Oy.P.Temp-Site.Link/) s
licencí
casinos sin deposito requerido · July 19, 2026 at 6:14 am
juegos de casinos sin deposito requerido gratis sin deposito ni
registro
Kelle · July 19, 2026 at 6:48 am
wettbüro hannover
Also visit my site basketball wetten strategien, Kelle,
Clinton · July 19, 2026 at 6:49 am
online casino výběr na neosurf
Take a look at my web page … hrací automaty nízký vklad [Clinton]
casa de Apuestas beisbol · July 19, 2026 at 6:56 am
casa de Apuestas beisbol caballos
españa
An Zwei spielautomaten gleichzeitig spielen · July 19, 2026 at 7:05 am
casino mindesteinzahlung 2 euro kreditkarte
Stop by my blog post; An Zwei spielautomaten gleichzeitig spielen
apuestas en la liga · July 19, 2026 at 7:10 am
trucos de apuestas en la liga deportivas
Nba Basketball Wett-tipps · July 19, 2026 at 7:25 am
wetten doppelte chance erklärung
Also visit my web blog Nba Basketball Wett-tipps
casinos bono bienvenida gratis sin deposito españa · July 19, 2026 at 7:30 am
de donde viene la palabra casino
my page: casinos bono bienvenida gratis sin deposito españa
nové online casino 2025 · July 19, 2026 at 7:32 am
české nové online casino 2025 casino
reload bonus
Phillip · July 19, 2026 at 7:37 am
ganar apuestas deportivas barcelona (Phillip) deportivas seguras
Jacquetta · July 19, 2026 at 7:42 am
gekaufte spiele wetten
Here is my site :: basketball handicap-wetten; Jacquetta,
CóDigo Promocional Apuestas · July 19, 2026 at 7:46 am
CóDigo Promocional Apuestas de caballos
medicalelessi-com.stackstaging.Com · July 19, 2026 at 7:46 am
esc gewinner Basketball wetten online (medicalelessi-com.stackstaging.Com)
best Horse racing betting online · July 19, 2026 at 7:56 am
free cheltenham bet no deposit required
Take a look at my blog post – best Horse racing betting online
was heißt hc 0 7 5 2 Bei basketball wetten · July 19, 2026 at 7:57 am
wettanbieter
my page :: was heißt hc 0 7 5 2 Bei basketball wetten
apuestas deportivas sin registro · July 19, 2026 at 8:01 am
apuestas deportivas sin registro de caballos juegos
casas de apuestas con esports · July 19, 2026 at 8:14 am
nfl casas de apuestas con esports
Matthias · July 19, 2026 at 8:53 am
casino bonos sin depozit – Matthias,
palermo tragamonedas gratis
https://Www.Asesoriamjmallorca.es/ · July 19, 2026 at 9:04 am
como funcionan las estadisticas apuestas deportivas
futbol – https://Www.Asesoriamjmallorca.es/ – combinadas
Apuestas Real Madrid Campeon Champions · July 19, 2026 at 9:09 am
Apuestas Real Madrid Campeon Champions argentina francia
Alfred · July 19, 2026 at 10:33 am
hacer apuestas listado casas de apuestas españa – Alfred, futbol
apuestas deportivas tips · July 19, 2026 at 10:35 am
apuestas deportivas tips f1 cuotas
conductores.dinamicagestion.Es · July 19, 2026 at 10:52 am
juegos de casino tragamonedas reales descarga
gratis de casino [conductores.dinamicagestion.Es]
Basketball wm 2023 Wetten · July 19, 2026 at 11:15 am
Basketball wm 2023 Wetten
com bonus bedingungen
Cierra · July 19, 2026 at 12:11 pm
offshore online casino bez poplatků – Cierra – cz
how to bet horse racing online in the uk · July 19, 2026 at 1:23 pm
boxing a how to bet horse racing online in the uk in horse racing
tipico live Wetten basketball · July 19, 2026 at 2:55 pm
wettbüro amberg
Feel free to visit my webpage tipico live Wetten basketball
Mike · July 19, 2026 at 3:05 pm
online wettanbieter bonus
Also visit my web page; auf basketball wetten (Mike)
horse racing results from Wolverhampton · July 19, 2026 at 3:39 pm
how to bet exacta box on fanduel
My web blog horse racing results from Wolverhampton
Basketball Wetten Tipps Nba · July 19, 2026 at 3:44 pm
buchmacher in deutschland
my blog post … Basketball Wetten Tipps Nba
Penni · July 19, 2026 at 3:48 pm
beste sportwetten quoten
Have a look at my blog post: spread wetten basketball – Penni,
Free Bet Offers Cheltenham · July 19, 2026 at 4:34 pm
Free Bet Offers Cheltenham bets on cheltenham today
Wolverhampton Horse Racing Today Results And Payouts · July 19, 2026 at 4:36 pm
bet Wolverhampton Horse Racing Today Results And Payouts racing
online uk
zahraničNí casino bonusový kód · July 19, 2026 at 4:52 pm
zahraničNí casino bonusový kód do mobilu
http://hometownservicesusa.com/ · July 19, 2026 at 5:05 pm
how does betting on horse racing betting free horse racing tips the betting site (http://hometownservicesusa.com/) racing work
WWW.Transportesservicat.es · July 19, 2026 at 5:26 pm
curso de apuestas deportivas gratis (http://WWW.Transportesservicat.es) deportivas es pronosticos
Apuestas City Real Madrid · July 19, 2026 at 5:29 pm
ganar Apuestas City Real Madrid en vivo
basketball-wetten · July 19, 2026 at 5:35 pm
gratis bonus sportwetten
My blog post; basketball-wetten
Basketball Bundesliga Wetten · July 19, 2026 at 5:36 pm
was bedeutet kombiwette
Feel free to visit my site – Basketball Bundesliga Wetten
Alextrejo.Com · July 19, 2026 at 5:37 pm
die besten sportwetten anbieter
Also visit my homepage :: Basketball Bundesliga Wetten (Alextrejo.Com)
Olympia basketball Wetten · July 19, 2026 at 5:40 pm
sportwetten strategien ihren wetterfolg
Here is my homepage: Olympia basketball Wetten
Paysafecard Bookmaker Wedden · July 19, 2026 at 6:21 pm
poker Paysafecard Bookmaker Wedden
2026
donpachuco.com · July 19, 2026 at 6:29 pm
nové paysafecard casino bonus za registraci (donpachuco.com) platba sms
apuestas copa del rey final · July 19, 2026 at 6:35 pm
estadisticas para apuestas copa del rey final futbol
cheltenham Festival ante Post betting · July 19, 2026 at 6:41 pm
free grand national bets no deposit
Have a look at my blog – cheltenham Festival ante Post betting
Https://Www.Villaslaurotorre.Com/ · July 19, 2026 at 6:50 pm
mejor casa de Impuestos En Apuestas (https://Www.Villaslaurotorre.Com/) deportivas foro
Kari · July 19, 2026 at 6:50 pm
marca apuestas app android (Kari) copa mundial de hockey
sports beste wedden nederland · July 19, 2026 at 6:52 pm
paardenkoers virtuele sports beste wedden nederland
Spread Wetten Basketball · July 19, 2026 at 7:00 pm
Spread Wetten Basketball quote berechnen
wedden feyenoord · July 19, 2026 at 7:02 pm
wedden feyenoord op paarden
Elwood · July 19, 2026 at 7:06 pm
wettseiten schweiz
My webpage: wett tipps heute basketball [Elwood]
Bob · July 19, 2026 at 7:07 pm
wie funktionieren kombiwetten
Also visit my web-site; basketball nba wetten (Bob)
https://julakim.de/hindernisrennen-tipps-und-tricks-fur-wettende/ · July 19, 2026 at 7:11 pm
free bets on the grand national
Feel free to visit my web-site – southwell racing results tonight (https://julakim.de/hindernisrennen-tipps-und-tricks-fur-wettende/)
What Is A Round Robin Bet In Horse Racing · July 19, 2026 at 7:13 pm
What Is A Round Robin Bet In Horse Racing racing
results newcastle today
Hallie · July 19, 2026 at 7:33 pm
best wettanbieter
Here is my blog post :: basketball wetten (Hallie)
Https://Web.Devamediapreneur.Com · July 19, 2026 at 7:41 pm
kombiwetten
my web site Basketball Wm 2023 Wetten [https://Web.Devamediapreneur.Com]
Monroe · July 19, 2026 at 7:49 pm
sportwetten verdoppler strategie
Here is my website; olympia basketball wetten – Monroe –
Hilda · July 19, 2026 at 8:02 pm
today’s horse racing explained betting [Hilda] non runners
Casino 100Kc Za Registraci · July 19, 2026 at 8:12 pm
Casino 100Kc Za Registraci pro
iphone
https://Www.Tovarganes.es/ · July 19, 2026 at 8:14 pm
nueva ley Casas de apuestas (https://Www.Tovarganes.es/) ufc topuria
Ungecombo.partydessert.de · July 19, 2026 at 8:23 pm
gratiswetten für bestandskunden
Feel free to visit my web-site – basketball wetten tipps nba (Ungecombo.partydessert.de)
wett tipps Heute basketball · July 19, 2026 at 8:25 pm
wetten ohne einzahlung geizkragen
Also visit my page :: wett tipps Heute basketball
Margarito · July 19, 2026 at 8:30 pm
sport bild basketball spieler wetten, Margarito,
handicap wetten Basketball · July 19, 2026 at 8:38 pm
sichere wettstrategie
Here is my website :: handicap wetten Basketball
leadergie.com · July 19, 2026 at 8:57 pm
was bedeutet quote bei wetten
Feel free to surf to my homepage; wett Tipps basketball heute (leadergie.com)
online sportwetten und live-wetten für fussball tennis basketball eishockey · July 19, 2026 at 8:58 pm
wetten bonus ohne einzahlung
Feel free to visit my homepage: online sportwetten und live-wetten für fussball tennis basketball eishockey
basketball wetten Prognosen · July 19, 2026 at 9:02 pm
basketball wetten Prognosen gewinnen tipps
voor geld wedden op snooker · July 19, 2026 at 9:06 pm
voor geld wedden op snooker geld en tops 5 wedden
https://www.elregalomusical.com/die-neuesten-trends-in-der-pferdezucht-und-ihr-einfluss-auf-wetten/ · July 19, 2026 at 9:10 pm
who to bet on at ascot today
my web-site betting tips cheltenham day 2 (https://www.elregalomusical.com/die-neuesten-trends-in-der-pferdezucht-und-ihr-einfluss-auf-wetten/)
Koby · July 19, 2026 at 9:23 pm
casas de apuestas liverpool barcelona (Koby) online usa
Https://londrinavolei.com.br/ · July 19, 2026 at 9:28 pm
nové casino s rychlou výplatou
Stop by my website; hrát jackpot za Peníze (https://londrinavolei.com.br/)
olympia Basketball wetten · July 19, 2026 at 9:31 pm
sportwetten online neu
My webpage – olympia Basketball wetten
casino Vklad Od 500 kč · July 19, 2026 at 9:36 pm
casino Vklad Od 500 kč
přístupné z čr
online basketball Wetten · July 19, 2026 at 9:49 pm
gratiswette für neukunden
Also visit my web site … online basketball Wetten
Betting Sites With Live Horse Racing · July 19, 2026 at 9:54 pm
Betting Sites With Live Horse Racing racing non runners yesterday
mejores casas de apuestas colombia · July 19, 2026 at 10:00 pm
mejor casa mejores casas de apuestas colombia apuestas
deportivas foro
wetten basketball em · July 19, 2026 at 10:01 pm
wettbüro bielefeld
Feel free to visit my blog – wetten basketball em
Kacey · July 19, 2026 at 10:09 pm
sportwetten bonus bedingungen
My homepage :: euroleague basketball wett tipps
(Kacey)
casino Vklad 200 kč Bitcoin · July 19, 2026 at 10:15 pm
online casino Vklad 200 kč Bitcoin s trustly
https://Www.avcc.Es/ · July 19, 2026 at 10:31 pm
handicap en apuestas celta real madrid (https://Www.avcc.Es/)
Jerold · July 19, 2026 at 10:32 pm
wetten österreich türkei
Also visit my webpage; euroleague basketball wett tipps (Jerold)
apuestas mlb hoy · July 19, 2026 at 10:55 pm
casas de apuestas mlb hoy
deportivas mexico
Josefa · July 19, 2026 at 11:15 pm
online basketball wetten gerade ungerade (Josefa)
sgvape · July 19, 2026 at 11:34 pm
sg vape hub
SGVape Hub: Quality Nicotine Vapes with Fast Same Day Delivery in Singapore
At SGVape Hub, we make it easy to enjoy premium SGVape products with speed and convenience across Singapore. We offer pure nicotine vapes, offering same day delivery and convenient cash on delivery, so you can receive your order quickly.
Our collection features trusted brands such as Lana, RELX, Vapetape, Elfbar, Snowwolf, SP2, and ONEM. Every product is handpicked to offer a premium vaping experience with quality you can trust.
Customers can also enjoy exclusive savings with every order. Enjoy $5 OFF when purchasing six or more pieces, $10 OFF on eleven or more pieces, and free delivery for orders above $300.
Premium SGVape Devices
Explore some of Singapore’s best-selling vape devices available for same day delivery.
Our collection includes Vapetape Engage, Vapetape Offgrid, Vapetape Offgrid Reload, ONEM Reload Cartridge, Lana Ultra II 16,000 Puffs, Lana Touch 32,000 Puffs, Lana Pen Plus 9,000 Puffs, RELX Infinity 2, RELX Creator 22,000 Puffs, Elfbar Ice King 40,000 Puffs, and Snowwolf 16,000 Puffs.
Whether you prefer disposable vapes, refillable pod systems, or compatible cartridges, SGVape Hub stocks a wide range of products to match your vaping style.
Clean, Legal, and Pure Vape Products
Your safety remains our priority. SGVape Hub only supplies clean, legal, and pure nicotine vape products.
We do not sell K pods or products containing illegal substances. Every vape device in our collection is handpicked to meet our quality standards, ensuring dependable quality when choosing their preferred device.
Featured Product: Vapetape Engage
The Vapetape Engage is designed for vapers who want excellent performance and flexibility in one device.
Key features include a powerful 2600mAh battery, adjustable wattage up to 50W, a refillable open pod system, dual cartridge compatibility, a 0.4? cartridge for bigger vapor production, and a 0.6? cartridge for a smooth inhale with richer flavor.
Simply refill with your preferred e-liquid and adjust the settings to match your vaping style.
Why Choose SGVape Hub
SGVape Hub offers premium products with fast local service to create a smooth shopping experience.
Benefits include same day delivery across Singapore, cash on delivery, pure nicotine vape products only, trusted vape brands, competitive pricing, bulk order discounts, and fast, reliable customer service.
Whether you’re buying your favorite disposable vape or upgrading to a refillable pod system, SGVape Hub supplies authentic SGVape products with speed and reliability throughout Singapore.
sg vape delivery · July 19, 2026 at 11:41 pm
sgvape
SGVape Hub: Pure Nicotine Vapes with Same Day Delivery in Singapore
At SGVape Hub, we make it easy to enjoy premium SGVape products with quick and dependable delivery across Singapore. We focus on pure nicotine vapes, providing same day delivery and convenient cash on delivery, making it simple to get your products fast.
Our collection includes trusted brands including Lana, RELX, Vapetape, Elfbar, Snowwolf, SP2, and ONEM. Every product is carefully selected to provide a reliable vaping experience with dependable performance.
Customers can also enjoy exclusive savings with every order. Get $5 OFF when purchasing six or more pieces, $10 OFF on eleven or more pieces, and complimentary delivery for orders above $300.
Premium SGVape Devices
Explore some of Singapore’s most popular vape devices available for same day delivery.
Our collection features Vapetape Engage, Vapetape Offgrid, Vapetape Offgrid Reload, ONEM Reload Cartridge, Lana Ultra II 16,000 Puffs, Lana Touch 32,000 Puffs, Lana Pen Plus 9,000 Puffs, RELX Infinity 2, RELX Creator 22,000 Puffs, Elfbar Ice King 40,000 Puffs, and Snowwolf 16,000 Puffs.
Whether you prefer disposable vapes, open pod systems, or replacement cartridges, SGVape Hub stocks a wide range of products to suit different vaping preferences.
Clean, Legal, and Pure Vape Products
Your safety continues to be our priority. SGVape Hub offers only clean, legal, and pure nicotine vape products.
We never sell K pods or products containing illegal substances. Every vape device in our collection is carefully chosen to meet our quality standards, giving customers confidence when choosing their preferred device.
Featured Product: Vapetape Engage
The Vapetape Engage is designed for vapers who want customizable vaping in one device.
Key features include a powerful 2600mAh battery, adjustable wattage up to 50W, a refillable open pod system, dual cartridge compatibility, a 0.4? cartridge for bigger vapor production, and a 0.6? cartridge for a smoother draw with richer flavor.
Simply refill with your preferred e-liquid and adjust the settings to match your vaping style.
Why Choose SGVape Hub
SGVape Hub brings together premium products with fast local service to create a smooth shopping experience.
Benefits include fast same day delivery across Singapore, cash on delivery, pure nicotine vape products only, trusted vape brands, competitive pricing, bulk order discounts, and fast, reliable customer service.
Whether you’re replacing your favorite disposable vape or upgrading to a refillable pod system, SGVape Hub provides authentic SGVape products quickly, safely, and hassle-free throughout Singapore.
Vicki · July 20, 2026 at 12:07 am
como ganar sistema de apuestas de futbol – Vicki – combinadas
paginas de apuestas bono sin deposito · July 20, 2026 at 12:50 am
paginas de apuestas bono sin deposito deportivas licencia españa
Dell · July 20, 2026 at 1:16 am
apuestas app de apuestas gratis – Dell,
futbol peru
Amelie · July 20, 2026 at 1:53 am
wette deutschland dänemark
Feel free to visit my web blog … auf basketball wetten (Amelie)
comerciobenidorm.es · July 20, 2026 at 2:21 am
casas que es la linea de Gol en Las apuestas (comerciobenidorm.es) apuestas bono sin ingreso
Computingteachers.com · July 20, 2026 at 2:30 am
české online casino vklad přes giropay (Computingteachers.com) reload bonus
Wetten basketball nba · July 20, 2026 at 3:06 am
Wetten basketball nba steuer österreich
Maynard · July 20, 2026 at 3:12 am
wettanbieter deutschland ohne oasis
my web-site … basketball wetten online (Maynard)
Basketball-wetten · July 20, 2026 at 3:47 am
asiatische handicap wette
My blog Basketball-wetten
Devon · July 20, 2026 at 3:51 am
wett tipps vorhersagen
Check out my blog post basketball punkte wetten [Devon]
college Basketball wetten strategie · July 20, 2026 at 4:07 am
college Basketball wetten strategie ist unser sport
Kyle · July 20, 2026 at 4:13 am
sportwettem
Also visit my blog … basketball wett tipps heute,
Kyle,
Darell · July 20, 2026 at 4:18 am
top 10 casino in canada, what online when does pa casinos open (Darell) are legal in australia and free bingo
games united states, or best usa poker apps
Basketball wetten besser Als fußBall · July 20, 2026 at 4:22 am
em spiele Basketball wetten besser Als fußBall
betting Tips Eurovision · July 20, 2026 at 4:31 am
paypal betting Tips Eurovision websites
Kerrie · July 20, 2026 at 4:40 am
nejlepší cardano nové casino 200 kč bonus (Kerrie)
protouchautoservices.com · July 20, 2026 at 4:53 am
sicher auf basketball wetten (protouchautoservices.com) gewinnen
online sports betting best · July 20, 2026 at 5:10 am
online sports betting best vegas sportsbooks
https://Plumbandlevelsc.com · July 20, 2026 at 5:13 am
betting on the grand national (https://Plumbandlevelsc.com) tips
for tomorrow horse racing
ante post betting for the derby · July 20, 2026 at 5:22 am
what are odds in ante post betting for the derby
horse racing
sites Apostas zodiac · July 20, 2026 at 5:34 am
sites Apostas zodiac online dinheiro
euroleague basketball wetten · July 20, 2026 at 5:56 am
profitable wettstrategie
my blog post euroleague basketball wetten
Shelli · July 20, 2026 at 6:10 am
slots no wagering uk, grand dusae casino no deposit bonus and best australian online gambling stoke on trent [Shelli] casino bonuses, or
united kingdom roulette betting strategy
https://vellorebiblecollege.com/jake-herni-trendy-nas-cekaji-v-nasledujicich-letech/ · July 20, 2026 at 6:11 am
české Casino reload bonus (https://vellorebiblecollege.com/jake-herni-trendy-nas-cekaji-v-nasledujicich-letech/) minimální vklad 10
kč sms
how to work out betting odds horse racing · July 20, 2026 at 6:21 am
how to work out betting odds horse racing tips cheltenham friday
https://Hotel.Phratashaitsolution.com/horse-racing-betting-understanding-terms-and-jargon/ · July 20, 2026 at 6:27 am
racing results from wolverhampton yesterday
Also visit my page – bet on ayr (https://Hotel.Phratashaitsolution.com/horse-racing-betting-understanding-terms-and-jargon/)
sites apostas desportivas · July 20, 2026 at 6:43 am
como apostar em cavalos
Feel free to surf to my website … sites apostas desportivas
sichere basketball wetten · July 20, 2026 at 6:44 am
verkaufte spiele sichere basketball wetten
https://n4umobiles.com/2026/07/07/expected-points-vs-actual-points-what-matters/ · July 20, 2026 at 6:46 am
nottingham forest betting tips and predictions
– https://n4umobiles.com/2026/07/07/expected-points-vs-actual-points-what-matters/, tips
Devullu.Com · July 20, 2026 at 6:59 am
beste wettanbieter bonus
Visit my website Basketball üBer Unter Wetten Overtime (Devullu.Com)
Onde Casas De Apostas Profissionais · July 20, 2026 at 7:05 am
academia do apostador
Also visit my webpage … Onde Casas De Apostas Profissionais
basketball nba wett tipps · July 20, 2026 at 7:06 am
handicap wetten bedeutung
Have a look at my webpage – basketball nba wett tipps
Finley · July 20, 2026 at 7:10 am
buchmacher ohne steuer
my blog :: basketball spieler wetten (Finley)
auf basketball wetten · July 20, 2026 at 7:17 am
beste sportwetten seiten
my homepage; auf basketball wetten
http://tarobacontabilidade.com.br/ · July 20, 2026 at 7:21 am
aposta esportiva com bonus
Look into my web-site: casas de apostas limite que aceitam pix (http://tarobacontabilidade.com.br/)
Serena · July 20, 2026 at 7:29 am
best casino app in usa, gambling statistics australia 202 and australian free pokies games, or
$5 min deposit new zealandn casinos
my web blog :: craps press (Serena)
https://expose.Studio-Merlin.com/ · July 20, 2026 at 7:36 am
Betting apps with cash out (https://expose.Studio-Merlin.com/)
odds euros
https://slapp.com.br/ · July 20, 2026 at 7:41 am
aposta legal
Look into my web-site :: é planilha apostas esportivas online (https://slapp.com.br/)
Manuel · July 20, 2026 at 7:49 am
esports college basketball wetten – Manuel – deutschland verboten
bookie betting sheets · July 20, 2026 at 7:53 am
top 100 bookie betting sheets websites
extra Place matched betting · July 20, 2026 at 8:04 am
what is a handicap bet
Here is my site; extra Place matched betting
Gertrude · July 20, 2026 at 8:12 am
5dollar deposit casino united states, fast payout
chukchansi casino bus trips (Gertrude) nz and fun casino australia, or spin palace withdrawal canada
who owns blue Lake casino · July 20, 2026 at 8:16 am
new no deposit casino canada, best paying online pokies united kingdom and who owns blue Lake casino chip values usa, or 5 dollar deposit casino united kingdom
glorious goodwood betting · July 20, 2026 at 8:23 am
derby ante post glorious goodwood betting
betting System · July 20, 2026 at 8:31 am
free betting System tips
online casina S Licencí 2026 · July 20, 2026 at 8:35 am
nové casino uvítací bonus
Here is my blog: online casina S Licencí 2026
Melhores Casa de Apostas · July 20, 2026 at 8:43 am
sistema kelly Melhores Casa de Apostas
Linette · July 20, 2026 at 8:44 am
poker tournaments 2021 united states, free spins no deposit usa 888 and all slots flash plaza casino
comps – Linette, australia, or online casino australia best payout
casino med Bankid snabba uttag · July 20, 2026 at 8:48 am
free spins no deposit casino med Bankid snabba uttag united kingdom
2021, new zealandn roulette book and new usa casinos free spins, or
bet365 united statesn roulette betting
https://Ha.log.br/como-as-analises-de-odds-podem-transformar-sua-estrategia-de-apostas/ · July 20, 2026 at 8:55 am
Esporte aposta online (https://Ha.log.br/como-as-analises-de-odds-podem-transformar-sua-estrategia-de-apostas/) esportiva confiavel
Bet365 Basketball Spieler Wetten · July 20, 2026 at 8:55 am
sportwetten vorhersagen app
Also visit my web-site: Bet365 Basketball Spieler Wetten
Sergio · July 20, 2026 at 8:56 am
usa casino games, new rm77 online casino (Sergio) casino united states 2021
and best casinos in central united states, or wwf blackjack lanza
Marcy · July 20, 2026 at 9:06 am
betting apps for android
Take a look at my webpage: online sportsbooks ny (Marcy)
projeto.skilldev.com.br · July 20, 2026 at 9:12 am
aposta ganha libertadores
Feel free to visit my webpage :: Bookmaker Apostas (projeto.skilldev.com.br)
how to bet a exacta box · July 20, 2026 at 9:17 am
betting the wheel in horse racing
Feel free to surf to my blog; how to bet a exacta box
betting cheltenham offers · July 20, 2026 at 9:20 am
best mi sportsbook app
Feel free to visit my web blog :: betting cheltenham offers
wolverhampton race results last night · July 20, 2026 at 9:29 am
horse wolverhampton race results last night betting calculator
basketball pro a wetten · July 20, 2026 at 9:43 am
buchmacher angebote
Also visit my web site; basketball pro a wetten
https://13Shine.com/2024/09/22/wie-live-daten-die-wettlandschaft-revolutionieren/ · July 20, 2026 at 9:46 am
esc wetten österreich
Feel free to visit my page: wett tipps basketball (https://13Shine.com/2024/09/22/wie-live-daten-die-wettlandschaft-revolutionieren/)
Arleen · July 20, 2026 at 9:55 am
betting tips cheltenham friday
Also visit my blog southwell racing results yesterday and
payouts today – Arleen,
basketball wettart wetten · July 20, 2026 at 9:58 am
esports wettanbieter
Here is my blog post: basketball wettart wetten
brighterspublishing.com · July 20, 2026 at 10:03 am
chelsea brighton betting tips
Here is my web blog: non gamstop free bet no deposit, brighterspublishing.com,
fazer apostas online · July 20, 2026 at 10:07 am
forum fazer apostas online online
como fazer uma aposta online · July 20, 2026 at 10:08 am
calculadora apostas como fazer uma aposta online
Mayra · July 20, 2026 at 10:09 am
bet on epsom derby
Feel free to surf to my web-site aintree free bets
existing customers (Mayra)
unentschieden basketball wetten · July 20, 2026 at 10:15 am
kombiwetten erklärt
Here is my web site unentschieden basketball wetten
Ai betting tips · July 20, 2026 at 10:40 am
Ai betting tips tips apps for android
Bingo clash game reviews · July 20, 2026 at 10:45 am
casino chains uk, native united statesn casino issues and best
online poker sites for united kingdoms, or how to win on the pokies
in united states
My site – Bingo clash game reviews
Ruleta Casino Klarna · July 20, 2026 at 11:00 am
nové cz Ruleta Casino Klarna bonus bez vkladu
casino gran Canaria maspalomas · July 20, 2026 at 11:16 am
when will pokies reopen south united states, united statesn biggest pokies
operator and betway poker australia, or casinos for gambling for uk
my web site … casino gran Canaria maspalomas
500% Bonus Za Depozyt Kasyno · July 20, 2026 at 12:09 pm
500% Bonus Za Depozyt Kasyno z depozytem 2
zł
české casino bonus bez vkladu 2025 · July 20, 2026 at 12:42 pm
online české casino bonus bez vkladu 2025 výběr skrill
Automaty Na Telefon Najlepsze · July 20, 2026 at 1:09 pm
kasyno vpn polska
My blog: Automaty Na Telefon Najlepsze
Rachele · July 20, 2026 at 1:16 pm
tipsport sázky
My blog fotbal výsledky krajský přebor (Rachele)
casino Met free bet · July 20, 2026 at 1:18 pm
gokken dit weekend
My homepage – casino Met free bet
https://vital1010.ro · July 20, 2026 at 1:44 pm
campionatul european echipa națională de fotbal a Tunisiei (https://vital1010.ro)
fotbal in romania
casino mindesteinzahlung 4 euro bitcoin · July 20, 2026 at 1:46 pm
keno gewinn
Stop by my web site :: casino mindesteinzahlung 4 euro bitcoin
apuestas de Caballos Juegos · July 20, 2026 at 1:58 pm
bono bienvenida apuestas de Caballos Juegos sin deposito
Pago Impuestos apuestas deportivas · July 20, 2026 at 2:03 pm
sistemas de Pago Impuestos apuestas deportivas
carrera de galgos apuestas · July 20, 2026 at 2:17 pm
doble oportunidad carrera de galgos apuestas significado
usa německo hokej žIvě · July 20, 2026 at 2:17 pm
tenis čtyřhra ženy
My site: usa německo hokej žIvě
https://www.Ewaosinska.com/waarom-kiezen-veel-spelers-voor-gokken-zonder-vergunning/ · July 20, 2026 at 2:19 pm
casino blankenberge roulette (https://www.Ewaosinska.com/waarom-kiezen-veel-spelers-voor-gokken-zonder-vergunning/) storten met kbc
https://www.Sarazamora.es/ · July 20, 2026 at 2:32 pm
las casas de apuestas deportivas mexico, https://www.Sarazamora.es/, pagan impuestos
fotbal românia liechtenstein · July 20, 2026 at 2:41 pm
clasament echipe fotbal românia liechtenstein
Kristofer · July 20, 2026 at 2:46 pm
clasamentul liga 1 fotbal romania
Feel free to visit my homepage :: verificare bilet casa pariurilor 2021,
Kristofer,
https://www.coposervicios.com/ · July 20, 2026 at 2:46 pm
beste spielautomaten sofortüberweisung
Also visit my page; risiko spiel automat; https://www.coposervicios.com/,
Oferta sky bet · July 20, 2026 at 2:47 pm
live Oferta sky bet verificare
bilet
české casino 1000 kč za registraci · July 20, 2026 at 2:50 pm
casina bezpečná 2026
Here is my blog post: české casino 1000 kč za registraci
Apuestas Arsenal Real Madrid · July 20, 2026 at 2:50 pm
Apuestas Arsenal Real Madrid
de blackjack en linea
zahraniční sázkové kanceláře s licencí v čr · July 20, 2026 at 3:01 pm
anglické zahraniční sázkové kanceláře s licencí v čr kanceláře
https://Neracompany.com/top-5-mituri-despre-Pariurile-pe-formula-1-demontate/ · July 20, 2026 at 3:06 pm
verificare bilet super bets
Also visit my blog post; pariuri biletul zilei fotbal [https://Neracompany.com/top-5-mituri-despre-Pariurile-pe-formula-1-demontate/]
SystéMová SáZka Tabulka · July 20, 2026 at 3:09 pm
monopoly vs dostihy a sazky
Here is my page: SystéMová SáZka Tabulka
camwoodfarm.com · July 20, 2026 at 3:23 pm
casino in spanbroek
my blog; belgische goksites 2026 (camwoodfarm.com)
http://www.testwordpress.9e.cz · July 20, 2026 at 3:30 pm
mobilní online casino bonus 1500 kč, http://www.testwordpress.9e.cz, bank wire transfer
Muhammad · July 20, 2026 at 3:33 pm
nejlepší casino poker online casino vklad 10 kč revolut – Muhammad,
casino met bonus 2026 · July 20, 2026 at 3:35 pm
beste goksite prepaid kaart
Look into my web page … casino met bonus 2026
Michal · July 20, 2026 at 3:35 pm
mejor casa marca apuestas 20 euros gratis (Michal) deportivas
Nilda · July 20, 2026 at 3:36 pm
single hand blackjack spelen
Feel free to surf to my site – 90 ball bingo mobiel (Nilda)
Https://Oksut.Obizizdns.Com/ · July 20, 2026 at 3:40 pm
Basketball Unentschieden Wetten (https://Oksut.Obizizdns.Com/) esc gewinner
Www.Livora.Cz · July 20, 2026 at 3:41 pm
čtvrtfinále extraligy ledního hokeje
Feel free to visit my web-site – dostihy a sáZky Heureka; http://Www.Livora.Cz,
Marilyn · July 20, 2026 at 3:49 pm
csgo sazeni
Here is my homepage: český národní hokejový tým – Marilyn –
Deandre · July 20, 2026 at 4:07 pm
zahraniční casino minimální vklad 5 kč sms – Deandre – vklad
neosurf
innovativewidget.com · July 20, 2026 at 4:17 pm
live casino betalen met visa
Here is my page: amusementshal Zaandam (innovativewidget.com)
https://www.admeco.es/apuestas-a-La-clasificacion-como-funciona-el-nuevo-Formato · July 20, 2026 at 4:18 pm
sitio futbolista Sevilla apuestas (https://www.admeco.es/apuestas-a-La-clasificacion-como-funciona-el-nuevo-Formato) deportivas
http://www.evagilart.com/hoe-verandert-de-technologie-de-manier-van-gokken-zonder-cruks/ · July 20, 2026 at 4:21 pm
low volatility gokkasten casino Maldegem (http://www.evagilart.com/hoe-verandert-de-technologie-de-manier-van-gokken-zonder-cruks/)
Neracompany.com · July 20, 2026 at 4:48 pm
Campionatul spaniei fotbal (Neracompany.com) judetean de fotbal timis
premiergaragedoormd.com · July 20, 2026 at 4:55 pm
unde sa joci poker pe bani
my blog post – Keno cu Jackpot (premiergaragedoormd.com)
fotbal cupa africii pe națiuni · July 20, 2026 at 4:56 pm
casa pariurilor ro rezultate
my webpage … fotbal cupa africii pe națiuni
Emily · July 20, 2026 at 5:08 pm
besten casinos mit klarna
Feel free to surf to my webpage: online casino ab 100 euro einzahlung; Emily,
Marissa · July 20, 2026 at 5:12 pm
horario casas de apuestas madrid (Marissa) deportivas
francia argentina
Hokej Online PřEnos Cesko Nemecko · July 20, 2026 at 5:15 pm
ms v hokeji vysledky
Here is my homepage – Hokej Online PřEnos Cesko Nemecko
SáZení Sportky · July 20, 2026 at 5:17 pm
sazka korunka výsledky
Feel free to surf to my page SáZení Sportky
drabiiiq.4fan.cz · July 20, 2026 at 5:29 pm
casino zatočení zdarma – drabiiiq.4fan.cz, s bonusem 200%
casino met startgeld nederland · July 20, 2026 at 5:43 pm
bingo snelle registratie
Look at my homepage; casino met startgeld nederland
licee sportive bucuresti fotbal · July 20, 2026 at 5:50 pm
oferta winner bet
my web site – licee sportive bucuresti fotbal
revolut kasino 1€ minimitalletus · July 20, 2026 at 6:01 pm
suomen parhaat mga kasinot
my web blog: revolut kasino 1€ minimitalletus
Nida · July 20, 2026 at 6:02 pm
beste bingo lage inzet
Here is my website … casino brugge met bancontact (Nida)
Bradly · July 20, 2026 at 6:04 pm
dostihy a sázky seznam koní
my web blog; česko ukrajina fotbal vstupenky (Bradly)
Katharina · July 20, 2026 at 6:07 pm
apuestas bonos gratis casas de apuestas
(Katharina) caballo
casino beverwijk · July 20, 2026 at 6:18 pm
gratis slots met bonus zonder storting
Also visit my web page casino beverwijk
150 euro Startguthaben ohne einzahlung · July 20, 2026 at 6:48 pm
online casino anmelde bonus
Have a look at my page 150 euro Startguthaben ohne einzahlung
https://effectorx.com/ · July 20, 2026 at 7:04 pm
meciuri live campionatul european de fotbal sub 19 ani [https://effectorx.com/] fotbal
https://gullyroad.com/m/tien-Dingen-die-je-moet-controleren-voordat-je-je-registreert/ · July 20, 2026 at 7:14 pm
gokhal peer
Look at my web blog :: casino laag huisvoordeel (https://gullyroad.com/m/tien-Dingen-die-je-moet-controleren-voordat-je-je-registreert/)
Beste kansspelen · July 20, 2026 at 7:15 pm
gokkasten mobiele
my homepage: Beste kansspelen
beste eerste storting Bonus Casino · July 20, 2026 at 7:19 pm
roulette toernooi
Feel free to visit my page … beste eerste storting Bonus Casino
Shavonne · July 20, 2026 at 8:01 pm
live meciuri fotbal
Also visit my page: casa pariurilor apk download (Shavonne)
https://arrjomcareersolutions.com/Faq-over-casino-S-zonder-cruks/ · July 20, 2026 at 8:12 pm
beste goud gokkasten
Also visit my blog; 50 euro gratis speelgeld
online casino (https://arrjomcareersolutions.com/Faq-over-casino-S-zonder-cruks/)
https://www.cambiumrestaurant.com/en/2026/06/25/hoe-evolueert-de-technologie-in-het-online-gokken/ · July 20, 2026 at 8:19 pm
gokautomaten engels
Also visit my website: casino holdem nederland (https://www.cambiumrestaurant.com/en/2026/06/25/hoe-evolueert-de-technologie-in-het-online-gokken/)
Basketball Wm 2023 Wetten · July 20, 2026 at 8:21 pm
sportwetten experten tipps
Here is my web page; Basketball Wm 2023 Wetten
cele mai bune bingo pe Samsung · July 20, 2026 at 8:35 pm
recomandare casino online
Also visit my web blog: cele mai bune bingo pe Samsung
Beste Casino Wetteren · July 20, 2026 at 8:38 pm
poker storten met prepaid kaart
Look into my web page; Beste Casino Wetteren
mistrovství svěTa v Hokeji v česku · July 20, 2026 at 9:10 pm
nejlepší fotbalové ligy mistrovství svěTa v Hokeji v česku
Leticia · July 20, 2026 at 9:28 pm
blackjack weesp
Stop by my homepage beste goksite belgie lage inzet (Leticia)
Luotettavat Kasinot Ilman Pelirajoja · July 20, 2026 at 9:31 pm
turvalliset nettikasinot suomi
Also visit my homepage – Luotettavat Kasinot Ilman Pelirajoja
betrouwbaar Game shows online · July 20, 2026 at 9:46 pm
blackjack mastercard
my site – betrouwbaar Game shows online
Thurman · July 20, 2026 at 9:48 pm
animal slots nederland
Feel free to visit my webpage … casino app met litecoin (Thurman)
sazka sportka dnešní tah · July 20, 2026 at 9:55 pm
vysledky tenis dnes
my webpage; sazka sportka dnešní tah
binance anm"alningsbonus · July 20, 2026 at 10:00 pm
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
cele mai bogate echipe de fotbal · July 20, 2026 at 10:20 pm
verificare bilet casa pariurilor ro
Also visit my web blog: cele mai bogate echipe de fotbal
http://Www.Bajt.Hys.cz · July 20, 2026 at 10:38 pm
tenis dnes program televize
Also visit my page :: muj fotbal okresní přebor – http://Www.Bajt.Hys.cz,
cat alearga Un jucator de fotbal · July 20, 2026 at 10:57 pm
gets bets verificare bilet
My web blog; cat alearga Un jucator de fotbal
https://pzbusov.hys.cz · July 20, 2026 at 11:15 pm
pravidla dostihy a sázky rychlá dráha pravidla (https://pzbusov.hys.cz) a sázky junior
Uwe · July 20, 2026 at 11:20 pm
sázky a dostihy (Uwe) junior
https://Www.Argiluze.Com/2026/03/29/wat-gebeurt-er-met-je-gegevens-bij-illegale-Goksites/ · July 20, 2026 at 11:24 pm
joop van ham gokkasten
Also visit my homepage … beste casino snelle uitbetaling (https://Www.Argiluze.Com/2026/03/29/wat-gebeurt-er-met-je-gegevens-bij-illegale-Goksites/)
bonuscode nederland casino · July 20, 2026 at 11:36 pm
pay n play bonuscode nederland casino ervaringen
Casino Ninove · July 21, 2026 at 12:15 am
baccarat vanaf 10 euro
Here is my web page – Casino Ninove
české Casino platba ecopayz · July 21, 2026 at 2:42 am
české Casino platba ecopayz 300 free spinů aktuálně
casino lier · July 21, 2026 at 4:00 am
blackjack surrender casino lier nederland
Casino actie dit weekend · July 21, 2026 at 4:45 am
populairste krasloten Casino actie dit weekend nederland
basketball wetten tipps Heute · July 21, 2026 at 5:23 am
österreich türkei basketball wetten tipps Heute
was heisst online Slots · July 21, 2026 at 5:30 am
live roulette deutschland
My website :: was heisst online Slots
https://Winstoneberlin.de/wie-man-sich-auf-ein-futsal-match-vorbereitet/ · July 21, 2026 at 5:31 am
wettquoten europameister
Look at my page … basketball wetten ab punktevorsprung sieg tippen (https://Winstoneberlin.de/wie-man-sich-auf-ein-futsal-match-vorbereitet/)
Casino Jeton Ab 30 Euro · July 21, 2026 at 5:38 am
online Casino Jeton Ab 30 Euro mit banküberweisung auszahlung
welche Automatenspiele sind die besten · July 21, 2026 at 5:43 am
online casino beste chancen
Check out my website: welche Automatenspiele sind die besten
turvalliset vedonvälittäjät · July 21, 2026 at 5:47 am
live-kertoimet mma
Here is my web blog – turvalliset vedonvälittäjät
Basketball tipps wetten · July 21, 2026 at 5:59 am
sichere wett Basketball tipps wetten heute
basketball wetten über unter · July 21, 2026 at 6:06 am
buchmacher app
My page: basketball wetten über unter
Candice · July 21, 2026 at 6:11 am
französisches roulette bingo online spielen (Candice) spielen
https://stpaulsearlyedcenter.com/ein-leitfaden-fur-krypto-casinos-ohne-lizenz/ · July 21, 2026 at 6:28 am
online casino mit vcreditos einzahlen (https://stpaulsearlyedcenter.com/ein-leitfaden-fur-krypto-casinos-ohne-lizenz/)
50 euro einzahlung cashtocode
scommesse risultato Esatto · July 21, 2026 at 6:44 am
statistiche per scommesse risultato Esatto
https://kentbaths.com/2026/07/09/bonus-di-benvenuto-come-massimizzarli/ · July 21, 2026 at 7:12 am
nuovo sito scommesse on-line (https://kentbaths.com/2026/07/09/bonus-di-benvenuto-come-massimizzarli/)
Bryon · July 21, 2026 at 7:13 am
online roulette ohne limit (Bryon) casino 3 euro mindesteinzahlung
https://effectorx.Com · July 21, 2026 at 7:14 am
über unter basketball Bundesliga wetten (https://effectorx.Com) erklärung
chi pronostici Scommesse Sportive · July 21, 2026 at 7:22 am
chi pronostici Scommesse Sportive sportive italia
Kelvin · July 21, 2026 at 7:24 am
app sportwetten
my web blog – basketball wetten ab punktevorsprung sieg tippen (Kelvin)
Basketball Wm 2023 wetten · July 21, 2026 at 7:27 am
wett app mit paypal
Feel free to visit my webpage; Basketball Wm 2023 wetten
Philomena · July 21, 2026 at 7:29 am
sport live wedden bookmaker; Philomena,
Larue · July 21, 2026 at 7:32 am
pferderennen leipzig wetten basketball tipps – Larue –
Lettie · July 21, 2026 at 7:36 am
fotbal evropská liga slavia, Lettie, zápasy dnes
https://abetterratetoday.com/strategii-pentru-a-evita-capcanele-comisioanelor-neteller/ · July 21, 2026 at 7:41 am
ponturi predictii fotbal
Feel free to surf to my homepage … oferta totală Casa pariurilor (https://abetterratetoday.com/strategii-pentru-a-evita-capcanele-comisioanelor-neteller/)
Saicharan-com.Stackstaging.com · July 21, 2026 at 7:50 am
bonus scommesse migliori (Saicharan-com.Stackstaging.com) coppa davis
Amos · July 21, 2026 at 7:56 am
tiki taka bonus benvenuto siti scommesse (Amos)
GlüCksspiel App Echtes Geld · July 21, 2026 at 7:59 am
online casino ab 10 euro paypal
my web-site GlüCksspiel App Echtes Geld
Melodee · July 21, 2026 at 8:51 am
blackjack online od 20 kasyno 50 zł depozyt bonus [Melodee]
https://Isowhey.COM.Vn · July 21, 2026 at 8:55 am
kasyno szczecin ranking – https://Isowhey.COM.Vn, online pl
gg significato scommesse · July 21, 2026 at 9:01 am
sito gg significato scommesse online
Migliori Siti Scommesse Inglesi · July 21, 2026 at 9:11 am
Migliori Siti Scommesse Inglesi
formula 1 pronostici
Kasyno 30 Euro Na Start · July 21, 2026 at 9:21 am
Kasyno 30 Euro Na Start gry na maszynach
Jestine · July 21, 2026 at 9:22 am
cosa significa handicap nelle scommesse elettroniche italia spagna – Jestine
–
nopein kotiutus vedonvälittäjä · July 21, 2026 at 9:23 am
vedonlyönti ulkomaille
Also visit my blog post; nopein kotiutus vedonvälittäjä
https://torrecaim.cat/dinero-de-bonificacion-en-linea-de-blackjack-sin-deposito-en-espanol/ · July 21, 2026 at 9:36 am
casinos nuevos con bono sin deposito
Have a look at my web page :: casino las leñas (https://torrecaim.cat/dinero-de-bonificacion-en-linea-de-blackjack-sin-deposito-en-espanol/)
mobilní casino bez nutnosti vkladu 2026 · July 21, 2026 at 9:44 am
online mobilní casino bez nutnosti vkladu 2026 výběr na skrill
Wett tipps basketball · July 21, 2026 at 9:44 am
wettbüro erfurt
Also visit my page – Wett tipps basketball
http://stampingdiecomponents.com/ · July 21, 2026 at 9:56 am
české casino otočky zdarma [http://stampingdiecomponents.com/]
bez blokace cz
Elton · July 21, 2026 at 9:56 am
lista slotów z bonusem
Also visit my page … kasyno sofort bonus za rejestrację (Elton)
Classic Blackjack um Geld spielen · July 21, 2026 at 10:38 am
10 euro einzahlen 200 euro bekommen
Also visit my site Classic Blackjack um Geld spielen
Tenis dnes Program televize · July 21, 2026 at 10:48 am
online výsledky hokej krajský přebor
My blog: Tenis dnes Program televize
https://Reformashercules.com/die-rolle-der-medien-in-der-wm-vorbereitung-ein-vergleich/ · July 21, 2026 at 11:01 am
online sport-wetten
Feel free to surf to my webpage; basketball wett tipps forum (https://Reformashercules.com/die-rolle-der-medien-in-der-wm-vorbereitung-ein-vergleich/)
basketball Pro b wetten · July 21, 2026 at 11:13 am
basketball Pro b wetten vorhersage heute
Jaimie · July 21, 2026 at 11:19 am
wedden eredivisie
my blog post e-wedden aanbieders, Jaimie,
scommesse napoli · July 21, 2026 at 11:28 am
siti scommesse napoli curacao
Pgb-abogados.com · July 21, 2026 at 11:36 am
online casino 100 euro revolut
Also visit my homepage: blackjack mit freispielen (Pgb-abogados.com)
https://cerealentertainment.com/2026/06/09/l-evoluzione-tecnologica-nelle-scommesse-sportive/ · July 21, 2026 at 11:39 am
scommessa Scommesse pronostici italia spagna (https://cerealentertainment.com/2026/06/09/l-evoluzione-tecnologica-nelle-scommesse-sportive/) svezia
Betrouwbaar Casino Site Nederland Echt Geld · July 21, 2026 at 11:45 am
beste goksite crypto Betrouwbaar Casino Site Nederland Echt Geld
blackjack raalte · July 21, 2026 at 11:50 am
beste online casino nederland ideal
Feel free to surf to my blog :: blackjack raalte
Bart · July 21, 2026 at 11:55 am
pronosticatore bonus registrazione scommesse (Bart)
Casino Kein Einsatzlimit · July 21, 2026 at 11:59 am
progressive jackpots app um echtes geld
Here is my webpage … Casino Kein Einsatzlimit
blackjack leuven · July 21, 2026 at 12:06 pm
live bingo echt geld
my homepage: blackjack leuven
App Scommesse Pronostici · July 21, 2026 at 12:19 pm
risultati partite di oggi coppa italia
Also visit my site App Scommesse Pronostici
Rebecca · July 21, 2026 at 12:27 pm
glücksspiel app deutschland
Feel free to surf to my homepage … casino mindesteinzahlung 30 euro paypal (Rebecca)
Carol · July 21, 2026 at 12:29 pm
todos los casinos que den bonos ruleta de casino americana (Carol)
bienvenida
Karissa · July 21, 2026 at 12:30 pm
sito di pronostici scommesse [Karissa] in italiano senza acconto
Evan · July 21, 2026 at 12:50 pm
tippen sportwetten
Here is my blog basketball over under wetten (Evan)
Fotbal supercupa romaniei · July 21, 2026 at 1:11 pm
jucatori de tenis romani
My web blog Fotbal supercupa romaniei
online casino 10 euro Giropay · July 21, 2026 at 1:21 pm
beste blackjack jeton
My homepage online casino 10 euro Giropay
Basketball wetten ab punktevorsprung sieg tippen · July 21, 2026 at 1:47 pm
quoten von Basketball wetten ab punktevorsprung sieg tippen dass
vape delivery singapore · July 21, 2026 at 1:55 pm
sg vape Trusted Vape Shop in Singapore
SGVapeDeliveryShop is a reliable vape supplier in Singapore, offering genuine vape products for every type of user. Our shop strictly excludes K Pods, selling only high-quality vape products.
Shop an extensive range of disposable vapes from well-known brands including Lana, Vapetape, RELX, Elf Bar, and ONEM. Each device is tested for long-lasting satisfaction.
Customer favorites include Lana Ultra 2 16000 Puffs, RELX Infinity Pod, Elf Bar Ice King Pro 45000 Puffs, Lana Pen Plus 9000 Puffs, and ONEM Pod 15000 Puffs. These vape devices deliver high performance and premium vaping experiences.
New products include Lana Pix 20000 Puffs, Vapetape Engage, RELX Creator 22000 Puffs, Elf Bar Raya S1 15000 Puffs, ONEM Pod 15000 Puffs, and Elf Bar Ice King Pro 45000 Puffs. Selected products are available with promotional prices.
Vapetape Engage offers advanced vaping performance. Ideal for daily vaping, it combines consistent vapor production with user-friendly operation.
Customer testimonials consistently mention quick shipping and authentic vape products. Satisfied buyers choose Singapore Vape Delivery Shop because of its quality products and reliable delivery.
Wholesale opportunities are also supported. Businesses, retailers, and agents can purchase large orders at competitive reseller rates. Wholesale pricing help businesses to start selling vape products.
The online store also features educational blog articles covering topics such as vaping laws in Singapore, nicotine strength comparisons, and vape ingredients. Educational content answer common vaping questions.
Shopping online is simple, secure, and convenient. Select your favorite vape products and receive prompt delivery. Singapore Vape Delivery Shop continues to provide quality vaping solutions with reliable delivery and trusted products.
Sloturi Cu Scatter · July 21, 2026 at 2:11 pm
păcănele volatilitate mica pe bani reali
Take a look at my blog … Sloturi Cu Scatter
Argentina peru apuestas · July 21, 2026 at 2:11 pm
Argentina peru apuestas favorito champions
Edward · July 21, 2026 at 2:13 pm
beste sportwetten strategie
My website; basketball wetten über unter (Edward)
https://hogarok.es/ · July 21, 2026 at 2:42 pm
ofertas apuestas predicciones (https://hogarok.es/) deportivas
Kenton · July 21, 2026 at 3:10 pm
pronostici mobili passione scommessa
Here is my blog; scommesse di domani, Kenton,
https://Neracompany.com/Sazeni-na-navrh-a-pripravu-sportu/ · July 21, 2026 at 3:14 pm
výsledky čr dostihy a sazky na mobil (https://Neracompany.com/Sazeni-na-navrh-a-pripravu-sportu/) ms v hokeji
pronostici Scommesse sportive domani · July 21, 2026 at 3:23 pm
pubblicità pronostici Scommesse sportive domani
Betting strategi lave odds · July 21, 2026 at 3:29 pm
boksning tips i dag
My site: Betting strategi lave odds
accumulator one leg lost · July 21, 2026 at 3:51 pm
greyhound betting
Look at my webpage … accumulator one leg lost
Antwan · July 21, 2026 at 4:00 pm
dětská hokejka na lední hokej
My website – kurzové sázení tipy (Antwan)
10€ neosurf talletusbonus kasino · July 21, 2026 at 4:03 pm
parhaat kasinobonukset ilman talletusta
Feel free to surf to my webpage 10€ neosurf talletusbonus kasino
Bettingsider Med Visa · July 21, 2026 at 4:07 pm
odds på tennis
Look into my site; Bettingsider Med Visa
Nettikasino Turnausbonus · July 21, 2026 at 4:15 pm
nettikasinoiden tarjoukset
Feel free to visit my blog post: Nettikasino Turnausbonus
elessidesign-Com.stackstaging.com · July 21, 2026 at 4:25 pm
fulham betting shop nottingham – elessidesign-Com.stackstaging.com –
odds
https://Roditecnia.com/jaakiekon-alykkaat-tilastot-Miten-kayttaa-dataa-hyvaksi/ · July 21, 2026 at 4:28 pm
turvalliset urheiluvedonlyönti sivustot
Visit my homepage :: valioliiga voittaja kertoimet (https://Roditecnia.com/jaakiekon-alykkaat-tilastot-Miten-kayttaa-dataa-hyvaksi/)
Jared · July 21, 2026 at 4:33 pm
juego de ruleta de casino para pc
My web-site :: casinos nuevos en españa bono sin depósito (Jared)
basketball wetten Tips · July 21, 2026 at 4:38 pm
wettquoten papst
Also visit my blog post: basketball wetten Tips
Rafaela · July 21, 2026 at 4:59 pm
apuestas octavos eurocopa [Rafaela] under over
casino apuestas · July 21, 2026 at 5:10 pm
tips gratis casino apuestas
peru Chile apuestas · July 21, 2026 at 5:11 pm
real madrid arsenal peru Chile apuestas
http://hriste.skaut-Ub.cz/ · July 21, 2026 at 5:21 pm
dnes fotbal cesko
my homepage … historické tabulky Fotbalové ligy [http://hriste.skaut-Ub.cz/]
Apuestas la liga española · July 21, 2026 at 5:24 pm
mejores casa de Apuestas la liga española
Nejlepší fotbalové ligy Světa · July 21, 2026 at 5:45 pm
mistrovství Nejlepší fotbalové ligy Světa hokej u20
http://Www.Johnpedroza.com/blog/kasinopelaamisen-sosiaaliset-vaikutukset/ · July 21, 2026 at 5:55 pm
klarna 10€ talletus kasino
Feel free to surf to my web page – suomalainen nettikasinot ilmaiskierrokset (http://Www.Johnpedroza.com/blog/kasinopelaamisen-sosiaaliset-vaikutukset/)
Bingo online kasino bonus · July 21, 2026 at 6:12 pm
pankkisiirto kasinot ilman rekisteröitymistä
my web site … Bingo online kasino bonus
Ak Profitovat Live SáZky · July 21, 2026 at 6:16 pm
mistrovství evropy fotbal
Feel free to surf to my page … Ak Profitovat Live SáZky
En iyi bet escort hit botu · July 21, 2026 at 6:16 pm
Türkiye’nin en iyi req bet, escort hit botu. alanında bir numara. Rakipsiz, dünyanın en iyi escort ve bet hit botu. kafaya alan ücretsiz bet escort hit botu. https://www.r10hitbotu.com/ https://www.r10hitbotu.com/ https://www.r10hitbotu.com/ https://www.r10hitbotu.com/ [sjdixwcrnykzxpfrqw]
Tenis výsledky davis cup · July 21, 2026 at 7:04 pm
sazka kontrola výsledků
Also visit my web-site – Tenis výsledky davis cup
prenota Scommesse · July 21, 2026 at 7:10 pm
migliori bookmaker italia
Also visit my website: prenota Scommesse
casinos online sin descarga · July 21, 2026 at 7:14 pm
juegos de maquinas de casino casinos online sin descarga gratis
čEský Hokej Rozhodčí · July 21, 2026 at 7:24 pm
sazka výsledky kontrola
my page čEský Hokej Rozhodčí
Kimberly · July 21, 2026 at 7:46 pm
casino zahraniční casina s bonusem bez vkladu [Kimberly] dogecoin
Dollie · July 21, 2026 at 7:50 pm
hokej česko německo dnes (Dollie) zápasy
fotbal
Susanna · July 21, 2026 at 8:04 pm
top chelsea palace betting (Susanna) app
herní automaty free spiny za registraci · July 21, 2026 at 8:13 pm
online casino vklad 5 kč sms
my website herní automaty free spiny za registraci
https://www.colinhoisingtonart.com/vorausschau-2026-die-heissesten-f1-wettenrunden/ · July 21, 2026 at 8:47 pm
wettbüro landshut
My site … basketball wettarten wetten (https://www.colinhoisingtonart.com/vorausschau-2026-die-heissesten-f1-wettenrunden/)
Juegos De Casino Gratis Sin Interrupciones · July 21, 2026 at 9:22 pm
casinos online Juegos De Casino Gratis Sin Interrupciones descarga
https://Fabioypilar.webdetuboda.com · July 21, 2026 at 10:13 pm
pronostico scommessa oggi
Also visit my homepage migliori siti scommesse aams (https://Fabioypilar.webdetuboda.com)
es.thefreedictionary.com · July 21, 2026 at 10:49 pm
%random_anchor_text%
References:
http://es.thefreedictionary.com/_/cite.aspx?url=http%3A%2F%2Flollybet.com.de&word=apostata&sources=vox_manual,vox1,kdict,vox_thes,open_thes,hc_Es_En
web bookmaker traduzione italiano · July 21, 2026 at 10:52 pm
scommettere vittoria italia
Feel free to surf to my blog; web bookmaker traduzione italiano
scommesse Fortnite · July 21, 2026 at 11:02 pm
dove scommettere su italia inghilterra
Feel free to surf to my website scommesse Fortnite
http://www.google.mw/url?sa=t&url=https://lollybet.com.de/ · July 21, 2026 at 11:37 pm
%random_anchor_text%
References:
http://www.google.mw/url?sa=t&url=https://lollybet.com.de/
Opificiopavone.melectronics.it · July 22, 2026 at 1:27 am
migliore app per migliori siti Di pronostici Scommesse (Opificiopavone.melectronics.it)
http://images.google.ge/url?q=https://lollybet.com.de/ · July 22, 2026 at 1:36 am
%random_anchor_text%
References:
http://images.google.ge/url?q=https://lollybet.com.de/
výsledky evropské ligy ve fotbale · July 22, 2026 at 1:54 am
ms výsledky evropské ligy ve fotbale fotbale kvalifikace
vedonlyöntivinkit korkeat kertoimet · July 22, 2026 at 2:27 am
rovaniemi ravivihjeet tänään
My webpage; vedonlyöntivinkit korkeat kertoimet
suurimmat tervetuliaisbonus kasino · July 22, 2026 at 3:14 am
suurimmat tervetuliaisbonus kasino 100€ minimitalletus
Nba Kertoimet · July 22, 2026 at 4:19 am
pelipiste nokia
My web page :: Nba Kertoimet
Nora · July 22, 2026 at 4:29 am
online casino otočky zdarma za registraci (Nora) platba přes trustly
wetten Basketball tipps · July 22, 2026 at 4:36 am
top sportwetten quoten
Look at my web blog; wetten Basketball tipps
kaikki Suomalaiset vedonlyöntisivustot · July 22, 2026 at 4:49 am
vedonlyönti trustly suomi
Feel free to surf to my website – kaikki Suomalaiset vedonlyöntisivustot
Uk bookmakers · July 22, 2026 at 4:50 am
crypto sports betting exchange
my web blog … Uk bookmakers
best betting exchange · July 22, 2026 at 4:52 am
draw best betting exchange system
Dakota · July 22, 2026 at 4:53 am
juniorské mistrovství světa v hokeji
Take a look at my webpage: co je systémová
sázka (Dakota)
tenis us open výsledky · July 22, 2026 at 4:57 am
internetové sázkové kanceláře
Have a look at my web blog: tenis us open výsledky
Mobile Betting Shop · July 22, 2026 at 5:09 am
sure bets odds comparison
My web page Mobile Betting Shop
Mitchell · July 22, 2026 at 5:19 am
horse dog racing odds explained (Mitchell) winner
nba2k20 gambling · July 22, 2026 at 5:20 am
gala bingo usa, free spins australia and new nba2k20 gambling sites australia, or new
zealandn online pokies min $5 deposit
Julieta · July 22, 2026 at 5:24 am
valorant vedonlyönti
Review my website … paras live-vedonlyönti (Julieta)
Dee · July 22, 2026 at 5:52 am
veloci siti scommesse straniere – Dee, italia
empresas Apuestas · July 22, 2026 at 5:53 am
empresas Apuestas con handicap baloncesto
https://lynx.astroempires.com · July 22, 2026 at 6:03 am
%random_anchor_text%
References:
https://lynx.astroempires.com/redirect.aspx?https://lollybet.com.de/
volejbola derīBu padomi · July 22, 2026 at 6:09 am
uzvaroša likmju stratēģija
Feel free to visit my blog :: volejbola derīBu padomi
Eirolīga Tiešraides Likmes · July 22, 2026 at 6:09 am
e-sporta derību padomi
Here is my web-site … Eirolīga Tiešraides Likmes
binance sign up · July 22, 2026 at 6:22 am
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
https://thechicagoroundtable.com/2026/07/21/jaky-vliv-ma-pocasi-na-vysledky-sportovnich-udalosti/ · July 22, 2026 at 6:33 am
cesko mistrovstvi sveta fotbal
Here is my blog post – www ctsport cz Tenis (https://thechicagoroundtable.com/2026/07/21/jaky-vliv-ma-pocasi-na-vysledky-sportovnich-udalosti/)
Roulette wheel Ipad · July 22, 2026 at 6:40 am
top bingo site usa, uk casino sites with no wagering requirements
and slot machines are called in canada, or top 10 casino canada
Feel free to surf to my homepage: Roulette wheel Ipad
75.cholteth.com · July 22, 2026 at 6:43 am
%random_anchor_text%
References:
https://75.cholteth.com/index/d1?diff=0&utm_source=ogdd&utm_campaign=26607&utm_content=&utm_clickid=g00w000go8sgcg0k&aurl=https://lollybet.com.de/
Vijoca.Com · July 22, 2026 at 6:50 am
vetovinkit asiantuntija
Feel free to visit my web blog; toto75 äimärautio – Vijoca.Com,
england France Betting · July 22, 2026 at 7:12 am
corner england France Betting
google.com.ph · July 22, 2026 at 7:13 am
%random_anchor_text%
References:
http://www.google.com.ph/url?sa=t&url=https://lollybet.com.de/
pronostici scommesse Gratuiti · July 22, 2026 at 7:51 am
palinsesto pronostici scommesse Gratuiti italia
https://www.fapcam.org · July 22, 2026 at 7:56 am
%random_anchor_text%
References:
https://www.fapcam.org/external_link/?url=https://lollybet.com.de/
biatlona tiešraides Likmes · July 22, 2026 at 8:03 am
latvija spānija biatlona tiešraides Likmes
Tania · July 22, 2026 at 8:13 am
derby winners horse racing
Here is my website :: cheltenham free bets existing customers
– Tania,
Tamika · July 22, 2026 at 8:21 am
how do you bet an exacta box
Here is my page :: horse racing results southwell yesterday (Tamika)
Scommesse italia Belgio · July 22, 2026 at 8:35 am
siti di Scommesse italia Belgio online non aams
Jak HráT Dostihy A SáZky · July 22, 2026 at 8:36 am
hokej mistrovství světa tabulky
my site Jak HráT Dostihy A SáZky
http://gamer.kg/proxy.php?link=https://lollybet.com.de/ · July 22, 2026 at 8:56 am
%random_anchor_text%
References:
http://gamer.kg/proxy.php?link=https://lollybet.com.de/
nejdelší hokejový zápas extraligy · July 22, 2026 at 8:58 am
hokej živě slovensko
My blog; nejdelší hokejový zápas extraligy
Ulrich · July 22, 2026 at 8:58 am
captain cooks casino united kingdom review, best canadian no deposit casinos and
free no deposit spins usa, or northern lights casino uk
Take a look at my web-site; anti gambling campaign (Ulrich)
http://Www.Computerarchaeologie.de/ · July 22, 2026 at 8:59 am
sportwetten bonus trick
Here is my web-site … nba basketball wett-tipps (http://Www.Computerarchaeologie.de/)
betting Guides · July 22, 2026 at 9:05 am
top sportsbook apps
Take a look at my homepage; betting Guides
Https://www.beatrizlora.es/ · July 22, 2026 at 9:09 am
predicciones apuestas impuestos; https://www.beatrizlora.es/, de futbol
tennis Kerroinvihjeet · July 22, 2026 at 9:11 am
korkean kertoimen vihjeet
Here is my web-site – tennis Kerroinvihjeet
betsson Tu sitio de Apuestas online · July 22, 2026 at 9:25 am
casas betsson Tu sitio de Apuestas online
apuestas eurocopa
http://x-ray.ucsd.edu · July 22, 2026 at 9:43 am
%random_anchor_text%
References:
http://x-ray.ucsd.edu/mediawiki/api.php?action=https://lollybet.com.de/
romford greyhound racing results · July 22, 2026 at 9:47 am
best cheltenham betting offers
my blog: romford greyhound racing results
Internet Wedden hockey · July 22, 2026 at 9:51 am
sportcompetities Internet Wedden hockey 2026
cse.google.co.ve · July 22, 2026 at 10:05 am
%random_anchor_text%
References:
http://cse.google.co.ve/url?q=https://lollybet.com.de/
https://priuschat.com · July 22, 2026 at 10:18 am
%random_anchor_text%
References:
https://priuschat.com/proxy.php?link=https://lollybet.com.de/
Bukmeikeris Jaunjelgava · July 22, 2026 at 10:26 am
likmes uz asv vēlēšanas
Check out my website :: Bukmeikeris Jaunjelgava
webpage · July 22, 2026 at 10:35 am
play online poker united states, where can i play poker online in australia and 500 poker chips united kingdom,
or best slot sites for winning usa
My blog: webpage
Karina · July 22, 2026 at 10:39 am
all today’s horse racing results (Karina)
horseracing results
Https://Aspedals.Com/El-Impacto-De-Las-Selecciones-No-Favoritas-En-El-Torneo/ · July 22, 2026 at 10:48 am
asiaticos Apuestas Brasil Uruguay – https://Aspedals.Com/El-Impacto-De-Las-Selecciones-No-Favoritas-En-El-Torneo/ –
betting for ayr gold cup · July 22, 2026 at 10:49 am
how to calculate payouts betting for ayr gold cup win place show bets
Riley · July 22, 2026 at 10:57 am
pronostici mobili passione scommessa
My web site: scommesse vittoria campionato italiano (Riley)
live wedden Trucs · July 22, 2026 at 10:57 am
nieuwe wedden live wedden Trucs
2026
apuestas Copa de Europa · July 22, 2026 at 11:06 am
como ganar dinero apuestas Copa de Europa
https://andysassurance.com/uncategorized/a-beginner-s-guide-to-Cricket-betting-terminology/ · July 22, 2026 at 11:12 am
tottenham chelsea best sports betting Analysis; https://andysassurance.com/uncategorized/a-beginner-s-guide-to-Cricket-betting-terminology/, tips
Marcus · July 22, 2026 at 11:17 am
mejores tipster de apuestas deportivas (Marcus) villarreal betis
bet on Grand national 2026 · July 22, 2026 at 11:49 am
aintree marsiac horse racing betting tips
Feel free to visit my web-site bet on Grand national 2026
sgvape · July 22, 2026 at 11:51 am
sgvape
SGVape Hub is a reliable online store for pure nicotine vape products in Singapore. The store offers fast same day delivery throughout Singapore and convenient cash on delivery, giving customers a fast shopping experience.
Explore trusted brands such as Vapetape, Lana, RELX, ELFBAR, Snowwolf, ONEM, and SP2. Every product is handpicked to provide excellent performance, satisfying taste, and premium quality.
The store specializes exclusively in pure nicotine vape products. No K Pods and no unauthorized products are included, ensuring customer safety with every purchase.
Receive discounts when ordering more devices. Orders of 6 pieces or more receive $5 OFF. Orders of 11 pieces or more receive $10 OFF. Delivery is free for purchases over $300.
Best-selling products include Vapetape Offgrid Reload, Vapetape Engage, Lana Ultra II 16000 Puffs, Lana Touch 32000 Puffs, Lana Pen Plus 9000 Puffs, ELFBAR Ice King 40000 Puffs, Snowwolf 16000 Puffs, RELX Creator 22000 Puffs, and Vapetape Offgrid 12000 Puffs. These devices deliver long-lasting performance, smooth vapor, and excellent flavor quality.
One of the newest arrivals is the VAPETAPE ENGAGE refillable pod system. The device includes a high-capacity 2600mAh battery, 50W adjustable power output, and dual cartridge options. Choose the 0.4? cartridge for more vapor, or select the 0.6? cartridge for a smoother draw.
SGVape Hub also stocks Vapetape Offgrid compatible cartridges, including ONEM 15K cartridges and Offgrid Reload e-liquid cartridges. The compatible cartridges deliver reliable performance while helping customers save money.
Fast delivery, trusted brands, great pricing, and strict quality standards make SGVape Hub one of the preferred vape shops in Singapore.
Merle · July 22, 2026 at 11:51 am
roland garros derības
my web page – 11.lv kā reģistrēties (Merle)
český pohár fotbal · July 22, 2026 at 12:18 pm
tenis davis cup vysledky
Review my web page; český pohár fotbal
Https://www.agatawheeler.com/ · July 22, 2026 at 12:26 pm
sms české online Casino free spiny bez vkladu 2026 (https://www.agatawheeler.com/) bonus za
registraci
real madrid hoy apuestas · July 22, 2026 at 12:30 pm
casas asiaticas real madrid hoy apuestas
https://makeupbynikolette.net/Wat-we-Kunnen-leren-van-het-andere-gastlanden-Over-organisatie/ · July 22, 2026 at 12:30 pm
waar online live wedden app – https://makeupbynikolette.net/Wat-we-Kunnen-leren-van-het-andere-gastlanden-Over-organisatie/ –
http://kokuryudo.com/mobile/index.cgi?id=1&mode=redirect&no=135&ref_eid=236&url=https://lollybet.com.de/ · July 22, 2026 at 12:33 pm
%random_anchor_text%
References:
http://kokuryudo.com/mobile/index.cgi?id=1&mode=redirect&no=135&ref_eid=236&url=https://lollybet.com.de/
Erik · July 22, 2026 at 12:36 pm
live virtuele wedden
My blog post sportweddenschappen trucs (Erik)
https://www.tmpimeraki.com/Spins-online-echt-geld-willkommensbonus-2026/ · July 22, 2026 at 12:40 pm
top casino mit freispielen
Review my blog post :: slots sofortüBerweisung auszahlung
(https://www.tmpimeraki.com/Spins-online-echt-geld-willkommensbonus-2026/)
Escuelabiodanzalaspalmas.Com · July 22, 2026 at 12:49 pm
Siti Scommesse Bloccati (Escuelabiodanzalaspalmas.Com)
su sanremo
Basketball wetten tipps · July 22, 2026 at 1:07 pm
wettquoten bayern dortmund
Here is my blog post Basketball wetten tipps
eerlijke wedden golf · July 22, 2026 at 1:08 pm
golf eerlijke wedden golf platformen
bingoal wedden op paarden · July 22, 2026 at 1:13 pm
grote bingoal wedden op paarden in nederland
Madelaine · July 22, 2026 at 1:29 pm
estadistica para apuestas deportivas – Madelaine, deportivas futbol
http://image.google.am/ · July 22, 2026 at 1:31 pm
%random_anchor_text%
References:
http://image.google.am/url?sa=t&source=web&rct=j&url=https://lollybet.com.de/
live wetten Basketball tipps · July 22, 2026 at 1:39 pm
über unter live wetten Basketball tipps
strategie
Regeninternational.Techzenau.Com · July 22, 2026 at 1:46 pm
live casino ohne einschränkung
Take a look at my page :: Neue Casinos Mit HöChster Bonus
(Regeninternational.Techzenau.Com)
online slots mit neosurf · July 22, 2026 at 1:48 pm
cluster pays online slots mit neosurf um geld spielen
Lyle · July 22, 2026 at 2:16 pm
estrategia corners apuestas (Lyle) deportivas
ganadas
casino en direct qui Paie le mieux belgique · July 22, 2026 at 2:23 pm
meilleurs casinos rtg
Also visit my webpage; casino en direct qui Paie le mieux belgique
Kā atvērt kontu Bukmeikerī · July 22, 2026 at 2:25 pm
Kā atvērt kontu Bukmeikerī izņemt bonusu
apuestas deportivas 1x2 · July 22, 2026 at 2:40 pm
casas de apuestas deportivas 1×2 legales
http://maps.google.co.in/url?q=https://lollybet.com.de/ · July 22, 2026 at 2:48 pm
%random_anchor_text%
References:
http://maps.google.co.in/url?q=https://lollybet.com.de/
Merle · July 22, 2026 at 3:05 pm
yusaon gold slots, casinos in ontario canada and best casino sites in canada, or bet365 play
united statesn roulette online uk
Take a look at my page; webpage (Merle)
melhor site aposta esportiva · July 22, 2026 at 3:23 pm
resultado melhor site aposta esportiva esportiva
casino klarna bonus ohne einzahlung · July 22, 2026 at 3:30 pm
roulette apple pay auszahlung
My web page … casino klarna bonus ohne einzahlung
Dorie · July 22, 2026 at 3:39 pm
tips wedden op snooker (Dorie) trucs vandaag
nl
Hi-educare.com · July 22, 2026 at 3:39 pm
roulette spiele 123
Also visit my web page … casino 5 euro paypal – Hi-educare.com –
sure Betting tips Apk · July 22, 2026 at 3:44 pm
compare bookmakers
Stop by my homepage; sure Betting tips Apk
Online Casino 15 Euro Google Pay · July 22, 2026 at 3:47 pm
Online Casino 15 Euro Google Pay mit dogecoin einzahlung
bono Gratis apuestas · July 22, 2026 at 3:49 pm
casas de bono Gratis apuestas con handicap asiatico
españa francia apuestas · July 22, 2026 at 3:54 pm
españa francia apuestas bono sin deposito
images.google.com.nf · July 22, 2026 at 4:11 pm
%random_anchor_text%
References:
http://images.google.com.nf/url?sa=t&url=https://lollybet.com.de/
Traci · July 22, 2026 at 4:29 pm
pronosticos y sistema 2 3 apuestas [Traci]
Https://Boostbingesoftworks.Co.uk/ · July 22, 2026 at 4:48 pm
best sports betting platform (https://Boostbingesoftworks.Co.uk/) licensing
beste wedden sites eu · July 22, 2026 at 5:07 pm
wedstrijd virtuele beste wedden sites eu
Betting Aintree · July 22, 2026 at 5:07 pm
horse racing bet winnings calculator
Here is my blog post … Betting Aintree
toolbarqueries.google.com.uy · July 22, 2026 at 5:11 pm
%random_anchor_text%
References:
http://toolbarqueries.google.com.uy/url?sa=t&url=https://lollybet.com.de/
Sally · July 22, 2026 at 5:12 pm
top australian online pokies, canadian gambling statistics 2021 and real money online casinos united states, or free play online does wind creek casino cash personal checks (Sally) canada
baccarat Casino nederland · July 22, 2026 at 5:24 pm
baccarat Casino nederland trucjes
Anastasia · July 22, 2026 at 5:24 pm
como ganan dinero las casas de apuestas (Anastasia) 1×2
blackjack types · July 22, 2026 at 5:37 pm
eur 20 free no deposit casino uk 2021, canada gambling bill
and windsor casino in united states, or age to enter casino in united kingdom
Visit my website – blackjack types
Lucie · July 22, 2026 at 5:43 pm
crypto gambling sites uk, download uk bingo game and real money nya online casinon 2022 (Lucie) casinos united states, or online poker licence
australia
Rhea · July 22, 2026 at 5:44 pm
beste casino kortrijk (Rhea) keno app
Https://Www.Nishikoi.Co.Uk · July 22, 2026 at 6:03 pm
888 poker promotion code united states, united statesn online casinos and gambling issues in australia, or tips for pokies australia
Look at my web site: American Roulette No Download (https://Www.Nishikoi.Co.Uk)
classement casino en ligne Belge · July 22, 2026 at 6:09 pm
dépôt classement casino en ligne Belge litecoin
online Wedden tips Gratis · July 22, 2026 at 6:09 pm
leuke weddenschappen prijs
My site; online Wedden tips Gratis
5 casino · July 22, 2026 at 6:14 pm
new usa online casinos no deposit bonuses, free spins or no deposit bonus and online 5 casino canada no deposit sign up
bonus, or top usa online poker sites
lester cut diamond casino heist · July 22, 2026 at 6:19 pm
canadian casino no deposit bonus codes 2021, new zealand poker
players and how to win china africa bonausaa slot machine, or new
uk paypal lester cut diamond casino heist
http://toolbarqueries.google.com.hk · July 22, 2026 at 6:21 pm
%random_anchor_text%
References:
http://toolbarqueries.google.com.hk/url?sa=t&url=https://lollybet.com.de/
sportweddenschappen Paypal · July 22, 2026 at 6:38 pm
wedden platformen app
Feel free to surf to my web page … sportweddenschappen Paypal
https://thegreenwrap.pk · July 22, 2026 at 7:07 pm
slot city casino joue à des jeux (https://thegreenwrap.pk) jeu
que es el handicap apuestas · July 22, 2026 at 7:07 pm
que es el handicap apuestas real sociedad
Www.Albacasado.com · July 22, 2026 at 7:11 pm
predicciones marca apuestas código promocional (http://Www.Albacasado.com)
tenis
http://www.promwood.com/ · July 22, 2026 at 7:20 pm
%random_anchor_text%
References:
http://www.promwood.com/de/url/?l=lollybet.com.de
Sean · July 22, 2026 at 7:23 pm
web wedden cs go
Feel free to surf to my web blog: golf e-wedden 2026 –
Sean –
apk betting · July 22, 2026 at 7:42 pm
bookie apk betting online
https://www.h3c.com/cn/Aspx/ContractMe/Default.aspx?subject=%u5507%u818f&url=https://lollybet.com.de/ · July 22, 2026 at 7:44 pm
%random_anchor_text%
References:
https://www.h3c.com/cn/Aspx/ContractMe/Default.aspx?subject=%25u5507%25u818f&url=https%3A%2F%2Flollybet.com.de/
http://toolbarqueries.google.rs/url?sa=t&url=https://lollybet.com.de/ · July 22, 2026 at 8:27 pm
%random_anchor_text%
References:
http://toolbarqueries.google.rs/url?sa=t&url=https://lollybet.com.de/
Cathern · July 22, 2026 at 8:34 pm
buy poker machine united kingdom, top casino slots uk and las vegas usa casino online no deposit bonus codes, or free online poker machine
games united kingdom
my web page :: spain bans gambling advertising (Cathern)
https://www.Asociacionalmaestepona.es/ · July 22, 2026 at 8:47 pm
mejores casas de mejor casa apuestas deportivas (https://www.Asociacionalmaestepona.es/) argentina
viresity.com · July 22, 2026 at 8:54 pm
ante post betting for ayr gold cup [viresity.com]
aintree
Pro Betting Tips · July 23, 2026 at 10:22 am
sport spread Pro Betting Tips
https://link.zhihu.com/ · July 23, 2026 at 10:23 am
%random_anchor_text%
References:
https://link.zhihu.com/?utm_oi=35221042888704&target=https://lollybet.com.de/
Best Online Betting Sites Offers · July 23, 2026 at 10:27 am
fouls Best Online Betting Sites Offers tips
https://git.mylocaldomain.online/connielattimor · July 23, 2026 at 10:39 am
References:
Winstar casino oklahoma https://git.mylocaldomain.online/connielattimor
https://wiibiplay.fun/@ouidabellino06?page=about · July 23, 2026 at 10:51 am
References:
Punto banco https://wiibiplay.fun/@ouidabellino06?page=about
Michelle · July 23, 2026 at 10:52 am
best betting sites horse racing
My blog monmore dog results yesterday (Michelle)
bookmyaccountant.co · July 23, 2026 at 11:20 am
References:
Emerald queen casino tacoma https://bookmyaccountant.co/profile/lucindabagot50
idreamarchitects.com · July 23, 2026 at 11:52 am
chelmsford betting tips
Here is my homepage; greyhound results oxford (idreamarchitects.com)
Matched Betting Sites · July 23, 2026 at 12:12 pm
cod esports Matched Betting Sites
Glory · July 23, 2026 at 12:26 pm
betting wolverhampton races
my web page: uk greyhound racing fixtures –
Glory –
harrah casino in st charles mo · July 23, 2026 at 12:32 pm
best online poker usa real money, online pokies free spins on sign up australia and no deposit online canadian casinos, or new zealandn online harrah casino in st charles mo real money
2021
Online Betting Sites That Take Paypal · July 23, 2026 at 12:44 pm
Online Betting Sites That Take Paypal odds and payouts
watch dog racing online · July 23, 2026 at 12:56 pm
st leger meet betting odds
Here is my web page … watch dog racing online
http://gw-generator.kplus.agency/ · July 23, 2026 at 12:58 pm
hrát automaty přes paysafecard
My blog; české casino 500 kč za registraci – http://gw-generator.kplus.agency/,
wap.sogou.com · July 23, 2026 at 1:01 pm
References:
Red hawk casino https://wap.sogou.com/uID=7PHkohezAXrNmf_8/tc?pg=webz&clk=6&url=https://instantcasinodeutschland.de/de-de/
sg vape · July 23, 2026 at 1:07 pm
sg vape hub
SGVape Hub is recognized as a reliable vape shop for pure nicotine vape products in Singapore. Our shop provides quick delivery throughout Singapore and convenient cash on delivery, giving customers an easy shopping experience.
Browse popular brands such as Lana, RELX, SP2, Vapetape, ELFBAR, Snowwolf, and ONEM. Each vape device is carefully chosen to offer smooth vaping, great flavor, and reliable performance.
The store specializes exclusively in clean nicotine vape devices. No K Pods and no unauthorized products are included, giving customers confidence with every purchase.
Enjoy additional savings when ordering more devices. Buy 6 or more items and get $5 OFF. Purchase 11 or more items for a $10 discount. Delivery is free for orders above $300.
Best-selling products include Vapetape Engage, Vapetape Offgrid Reload, RELX Creator 22000 Puffs, Lana Touch 32000 Puffs, ELFBAR Ice King 40000 Puffs, Lana Ultra II 16000 Puffs, Snowwolf 16000 Puffs, Lana Pen Plus 9000 Puffs, and Vapetape Offgrid 12000 Puffs. These devices offer excellent battery life, consistent performance, and satisfying taste.
A featured new product is the Vapetape Engage advanced pod device. The device includes a high-capacity 2600mAh battery, adjustable wattage up to 50W, and multiple cartridge choices. Choose the 0.4? cartridge for larger clouds, or use the 0.6? pod for enhanced flavor.
The store also offers Offgrid replacement cartridges, including ONEM 15K cartridges and Offgrid Reload e-liquid cartridges. These products deliver smooth operation while helping customers save money.
Fast delivery, trusted brands, great pricing, and strict quality standards make SG Vape Hub one of the preferred vape shops in Singapore.
manchester sapphire blue · July 23, 2026 at 1:17 pm
Mevius Original
AUS CIG SHOP online store is an online tobacco shop operating throughout Australia. The website offers a selection of cigarettes and roll-your-own (RYO) tobacco, offering an easy way to order tobacco products online.
A major feature of the website is free delivery Australia wide with no minimum order requirement. Customers can place both small and large orders at no extra delivery cost.
Orders completed before 5:00 am (GMT+11) are sent out the same day, allowing for faster delivery throughout Australia. The company highlights reliable and discreet delivery for customer convenience.
The store accepts multiple payment options, including Wise, PayPal, bank transfer, and USDT, giving customers multiple payment options.
The website offers many popular cigarette brands, including Dunhill, Marlboro, Manchester, Double Happiness, Benson & Hedges, Mevius, Esse, Mac Super Slim, and Oscar Super Slim.
Among the best-selling products are Manchester Royal Red, Dunhill Red, Benson & Hedges Gold, Double Happiness, Mevius Option Purple, Esse Change, Mac Super Slim Ice Cool Blast, and Oscar Super Slim Ice Cool. These items are commonly available in cartons containing 10 packs of 20 cigarettes, with many offered at discounted prices.
According to information on the website all products are supplied by reliable sources and are described as 100% original. The business limits sales to customers aged 18+ and aims to provide competitive prices, dependable service, and customer satisfaction.
The platform also contains informational pages and an FAQ, covering topics such as delivery times, payment options, parcel tracking, shipping fees, cancellations, international delivery, and customer service.
https://www.askmeclassifieds.com · July 23, 2026 at 1:19 pm
References:
Slot marsepeinstein https://www.askmeclassifieds.com/index.php?page=user&action=pub_profile&id=87940&item_type=active&per_page=16
https://www.workbay.online/ · July 23, 2026 at 1:20 pm
References:
Native american casinos https://www.workbay.online/profile/devcalvin19734
https://truthtube.video/@lucyemd2963151?page=about · July 23, 2026 at 1:21 pm
References:
Spa casino palm springs https://truthtube.video/@lucyemd2963151?page=about
https://wiki.computacaonaescola.ufsc.br/api.php?action=https://instantcasinodeutschland.de/en-au/ · July 23, 2026 at 1:22 pm
References:
Brighton casino https://wiki.computacaonaescola.ufsc.br/api.php?action=https://instantcasinodeutschland.de/en-au/
Emperor Casino · July 23, 2026 at 1:23 pm
gambling advertising canada, online poker canada vpn and best online
Emperor Casino united kingdom fast payouts,
or united kingdom online pokies paypal
Basketball Wetten Ab Punktevorsprung Sieg Tippen · July 23, 2026 at 1:35 pm
sichere kombiwetten
Stop by my webpage; Basketball Wetten Ab Punktevorsprung Sieg Tippen
draw betting tips · July 23, 2026 at 1:43 pm
draw betting tips website
Ina · July 23, 2026 at 1:44 pm
betting on a place in kentucky derby horse race winner; Ina,
racing
Florine · July 23, 2026 at 1:45 pm
asian betting shop nottingham; Florine, sites
https://www.garciajavi.com/understanding-risk-management-in-betting/ · July 23, 2026 at 1:45 pm
online sports total goals spread betting explained (https://www.garciajavi.com/understanding-risk-management-in-betting/) ny
https://voomrecruit.com/ · July 23, 2026 at 1:48 pm
References:
Silver reef casino https://voomrecruit.com/employer/online-casino-mit-schnellen-auszahlungen-und-top-boni
https://64.cholteth.com/index/d1?diff=0&utm_source=ogdd&utm_campaign=26607&utm_content=&utm_clickid=g00w000go8sgcg0k&aurl=https://instantcasinodeutschland.de/de-ch/ · July 23, 2026 at 1:51 pm
References:
Casino tucson https://64.cholteth.com/index/d1?diff=0&utm_source=ogdd&utm_campaign=26607&utm_content=&utm_clickid=g00w000go8sgcg0k&aurl=https://instantcasinodeutschland.de/de-ch/
https://ares.astroempires.com · July 23, 2026 at 1:51 pm
References:
Mint casino https://ares.astroempires.com/redirect.aspx?https://instantcasinodeutschland.de/de-be/
http://gamer.kg/proxy.php?link=https://instantcasinodeutschland.de/fr-ca/ · July 23, 2026 at 2:05 pm
References:
Cramps in feet http://gamer.kg/proxy.php?link=https://instantcasinodeutschland.de/fr-ca/
https://www.bud108.com/bbs/board.php?bo_table=free&wr_id=147325 · July 23, 2026 at 2:05 pm
References:
Brimley casino https://www.bud108.com/bbs/board.php?bo_table=free&wr_id=147325
http://maps.google.es/url?q=https://lollybet.com.de/ · July 23, 2026 at 2:07 pm
%random_anchor_text%
References:
http://maps.google.es/url?q=https://lollybet.com.de/
angkot88 · July 23, 2026 at 2:42 pm
angkot88
ore.spongepowered.org · July 23, 2026 at 2:43 pm
References:
Betting odds explained https://ore.spongepowered.org/linkout?remoteUrl=https://instantcasinodeutschland.de/en-ca/
WWW.Agatawheeler.Com · July 23, 2026 at 2:54 pm
acca boost chelsea newcastle Betting Tips (http://WWW.Agatawheeler.Com) sites
basketball unentschieden wetten · July 23, 2026 at 2:57 pm
sichere wett tipps
Also visit my webpage; basketball unentschieden wetten
giaovienvietnam.vn · July 23, 2026 at 3:03 pm
References:
Aristocrat slots https://giaovienvietnam.vn/employer/instant-casino-deutschland-%ef%b8%8f-exklusiver-promo-code-und-vip-programm/
Shanice · July 23, 2026 at 3:08 pm
free silver reef casino birthday rewards; Shanice,
cash no deposit usa, united statesn poker and aristocrat free slots united states, or united kingdom roulette strategy to win big
maps.google.mg · July 23, 2026 at 3:15 pm
References:
Best online casino bonuses http://maps.google.mg/url?sa=t&url=https://instantcasinodeutschland.de/es-es/
http://maps.google.co.ke · July 23, 2026 at 3:24 pm
%random_anchor_text%
References:
http://maps.google.co.ke/url?q=https://lollybet.com.de/
How To Place A Bet Grand National · July 23, 2026 at 3:26 pm
betting tips today cheltenham
Take a look at my web page; How To Place A Bet Grand National
Amie · July 23, 2026 at 3:26 pm
horse race bet calculator
Here is my site; newcastle greyhounds fixtures (Amie)
https://www.ribalkaforum.com/proxy.php?link=https://instantcasinodeutschland.de/de-de/ · July 23, 2026 at 3:29 pm
References:
Club gold casino https://www.ribalkaforum.com/proxy.php?link=https://instantcasinodeutschland.de/de-de/
worldaid.eu.org · July 23, 2026 at 3:42 pm
References:
Silverstar casino https://worldaid.eu.org/discussion/profile.php?id=2064471
http://www.myriad-online.com/ · July 23, 2026 at 3:56 pm
References:
North brunswick http://www.myriad-online.com/cgi-bin/miniboard.pl?file=awafiles/AWMiniboard.txt&url=https://instantcasinodeutschland.de/en-ca/
http://clients1.google.dj/url?q=https://instantcasinodeutschland.de/de-de/ · July 23, 2026 at 3:59 pm
References:
Casino online aams http://clients1.google.dj/url?q=https%3A%2F%2Finstantcasinodeutschland.de%2Fde-de%2F
greyhound derby final Betting · July 23, 2026 at 4:02 pm
horse racing betting apps
Look into my blog post :: greyhound derby final Betting
bolsajobs.com · July 23, 2026 at 4:05 pm
References:
Blackjack surrender https://bolsajobs.com/employer/how-many-words-are-spoken-in-the-phantom-of-the-opera-on-broadway?
https://yooverse.com · July 23, 2026 at 4:10 pm
References:
Casino770 https://yooverse.com/@caridad03j3982
my.steamchina.com · July 23, 2026 at 4:13 pm
%random_anchor_text%
References:
https://my.steamchina.com/linkfilter/?url=https://lollybet.com.de/
Stewart · July 23, 2026 at 4:20 pm
new zealand pokies app, australia slot machine games and 100 no deposit bonus codes 2021 canada, or casino uk paypal
My page: vegas blackjack table minimums (Stewart)
cse.google.bf · July 23, 2026 at 4:30 pm
%random_anchor_text%
References:
http://cse.google.bf/url?sa=t&url=http%3A%2F%2Flollybet.com.de
lj.rossia.org · July 23, 2026 at 4:36 pm
References:
Gala casino bristol https://lj.rossia.org/meme.bml?url=https://instantcasinodeutschland.de/es-es/
Jungle Casino · July 23, 2026 at 4:48 pm
pokie machine laws canada, united states online Jungle Casino slots and play free
usa bingo, or 888 poker deposit new zealand
https://bolsajobs.com/employer/how-to-locate-the-username-and-password-field-within-instagram-login-page-using-chromedriver-and-selenium-python · July 23, 2026 at 4:53 pm
References:
California casino las vegas https://bolsajobs.com/employer/how-to-locate-the-username-and-password-field-within-instagram-login-page-using-chromedriver-and-selenium-python
https://gratisafhalen.be/ · July 23, 2026 at 4:54 pm
tiger online check in
References:
https://gratisafhalen.be/author/bookerelyar/
https://staffsagye.com/bbs/board.php?bo_table=free&wr_id=90680 · July 23, 2026 at 5:01 pm
bitcoin casino
References:
https://staffsagye.com/bbs/board.php?bo_table=free&wr_id=90680
https://schreinerei-leonhardt.de/ · July 23, 2026 at 5:02 pm
wind creek casino atmore
References:
https://schreinerei-leonhardt.de/best-payid-casinos-australia-2026-play-payid-pokies-4
jobpk.pk · July 23, 2026 at 5:10 pm
References:
Red32 casino https://jobpk.pk/companies/instant-casino-review-rating-2026-is-it-safe-legit/
spechrom.com · July 23, 2026 at 5:13 pm
References:
Atlantis casino reno https://spechrom.com:443/bbs/board.php?bo_table=service&wr_id=458024
http://cse.google.al/ · July 23, 2026 at 5:21 pm
References:
Bonus slots http://cse.google.al/url?sa=t&url=http%3A%2F%2Finstantcasinodeutschland.de%2Fes-es%2F
https://resourzter.com · July 23, 2026 at 5:21 pm
palm springs casinos
References:
https://resourzter.com/companies/payid-pokies-instant-deposit-online-pokies-via-payid-in-australia-2026/
findinall.com · July 23, 2026 at 5:25 pm
casino soundtrack
References:
https://www.findinall.com/profile/kendra47s03745
marine-zone.com · July 23, 2026 at 5:47 pm
agente smart casino totale
References:
https://marine-zone.com/employer/instant-payid-withdrawal-casinos-in-australia-fast-payouts/
wiibidate.fun · July 23, 2026 at 5:48 pm
References:
Casinos of winnipeg https://wiibidate.fun/@emorycolebe971
tripleoggames.com · July 23, 2026 at 5:54 pm
diamond jo casino dubuque
References:
https://tripleoggames.com/employer/top-payid-online-casinos-for-aussie-players-in-2025/
https://martdaarad.com/profile/columbusklass5 · July 23, 2026 at 5:56 pm
fruit machines
References:
https://martdaarad.com/profile/columbusklass5
https://govtpkjob.pk/ · July 23, 2026 at 5:59 pm
river palms casino laughlin nv
References:
https://govtpkjob.pk/companies/payid-pokies-no-deposit-bonus-australia-2026-claim/
https://git.farmtowntech.com · July 23, 2026 at 6:08 pm
References:
Lady luck casino vicksburg ms https://git.farmtowntech.com/korymackaness
gitiplay.com · July 23, 2026 at 6:27 pm
References:
Gold coast casino las vegas https://gitiplay.com/@richellebed32?page=about
casino red bonus codes · July 23, 2026 at 6:31 pm
online gambling laws in uk, apple pay casinos australia and nz casino online, or best casino red bonus codes in australia online
https://gt.clarifylife.net/devinuin86879 · July 23, 2026 at 6:38 pm
References:
Cool cat casino https://gt.clarifylife.net/devinuin86879
Herní Automaty Free Spiny Za Registraci · July 23, 2026 at 6:47 pm
casino s Herní Automaty Free Spiny Za Registraci spiny bez vkladu
https://realestate.kctech.com.np · July 23, 2026 at 6:54 pm
best online blackjack
References:
https://realestate.kctech.com.np/profile/jackfrias81100
https://makler.sale · July 23, 2026 at 7:02 pm
References:
Best online blackjack https://makler.sale/index.php?page=user&action=pub_profile&id=7884&item_type=active&per_page=16
basketball Wetten tipps · July 23, 2026 at 7:06 pm
online wettanbieter ohne oasis
Feel free to visit my web page basketball Wetten tipps
https://hayal.site/user/profile/2821 · July 23, 2026 at 7:11 pm
mohawk casino
References:
https://hayal.site/user/profile/2821
college basketball Wetten · July 23, 2026 at 7:16 pm
gegen den euro college basketball Wetten
maps.google.hu · July 23, 2026 at 7:16 pm
References:
Casino barcelona http://maps.google.hu/url?q=https://instantcasinodeutschland.de/de-at/
maps.google.com.bz · July 23, 2026 at 7:18 pm
References:
Colosseum casino http://maps.google.com.bz/url?q=https://instantcasinodeutschland.de/fr-ca/
ok.ru · July 23, 2026 at 7:25 pm
References:
Iowa casinos https://ok.ru/dk?cmd=logExternal&st.name=externalLinkRedirect&st.link=https%3A%2F%2Finstantcasinodeutschland.de%2Ffr-be%2F
http://moldova.sports.md/extlivein.php?url=https://instantcasinodeutschland.de/en-ca/ · July 23, 2026 at 7:30 pm
References:
Solstice arena http://moldova.sports.md/extlivein.php?url=https://instantcasinodeutschland.de/en-ca/
https://myesc.escardio.org/Account/ESCRegister?ReturnUrl=https://instantcasinodeutschland.de/ · July 23, 2026 at 7:44 pm
References:
Casper games https://myesc.escardio.org/Account/ESCRegister?ReturnUrl=https://instantcasinodeutschland.de/
https://jobcop.ca/employer/instant-casino-review-ratings-2026-is-it-legit-safe/ · July 23, 2026 at 7:48 pm
References:
List of las vegas casinos https://jobcop.ca/employer/instant-casino-review-ratings-2026-is-it-legit-safe/
http://clients1.google.ae · July 23, 2026 at 7:54 pm
References:
Sands casino bethlehem pa http://clients1.google.ae/url?q=https://instantcasinodeutschland.de/en-au/
Globalfetishcalendar.com · July 23, 2026 at 7:58 pm
are there any mobile only promos for horse best platforms With live greyhound betting Odds (Globalfetishcalendar.com)
https://tripleoggames.com/employer/payid-is-quietly-becoming-the-fastest-withdrawal-rail-in-australian-online-casinos-and-what-that-tells-investors-about-real-time-payment-adoption/ · July 23, 2026 at 8:01 pm
le richelieu in the french quarter
References:
https://tripleoggames.com/employer/payid-is-quietly-becoming-the-fastest-withdrawal-rail-in-australian-online-casinos-and-what-that-tells-investors-about-real-time-payment-adoption/
Https://Lindonentertainment.com · July 23, 2026 at 8:02 pm
besten sportwetten apps
My web-site; basketball wetten besser als fußball; https://Lindonentertainment.com,
Sean · July 23, 2026 at 8:02 pm
top 10 online casino sites usa, no deposit bonus on sign up usa
and grand mondial casino australia, or usa online casino with
fake money; Sean, casinos gambling
https://old.urso.ru/action.redirect/url/aHR0cHM6Ly9pbnN0YW50Y2FzaW5vZGV1dHNjaGxhbmQuZGUvZW4tYXUv · July 23, 2026 at 8:03 pm
References:
Super scratch programming adventure https://old.urso.ru/action.redirect/url/aHR0cHM6Ly9pbnN0YW50Y2FzaW5vZGV1dHNjaGxhbmQuZGUvZW4tYXUv
https://gladjobs.com/employer/best-australian-online-pokies-payid-in-2026/ · July 23, 2026 at 8:12 pm
rivers casino pittsburgh pa
References:
https://gladjobs.com/employer/best-australian-online-pokies-payid-in-2026/
https://career.braincode.com.bd · July 23, 2026 at 8:16 pm
References:
Gold eagle casino https://career.braincode.com.bd/employer/casino-online-oficial-con-licencia/
Isla · July 23, 2026 at 8:20 pm
ante post betting cheltenham 2026 tips
Here is my web site brighton greyhound racing fixtures (Isla)
jobs.careerincubation.com · July 23, 2026 at 8:30 pm
twist casino
References:
https://jobs.careerincubation.com/employer/top-crypto-casinos-australia-2026-btc-eth-payid-the-european-business-review/
nursingguru.in · July 23, 2026 at 8:37 pm
basic strategy blackjack
References:
https://nursingguru.in/employer/global-payment-processing-platform/
http://aintedles.yoo7.com · July 23, 2026 at 9:05 pm
References:
Aristocrat pokies http://aintedles.yoo7.com/go/aHR0cHM6Ly9pbnN0YW50Y2FzaW5vZGV1dHNjaGxhbmQuZGUvZGEtZGsv
https://worlancer.com · July 23, 2026 at 9:06 pm
References:
Pai gow poker online https://worlancer.com/profile/ggpheath32688
Basketball Wetten Tipps Europa League · July 23, 2026 at 9:16 pm
bester online wettanbieter
Visit my web blog; Basketball Wetten Tipps Europa League
homecamgirl.com · July 23, 2026 at 9:19 pm
References:
Bonus slots https://www.homecamgirl.com:443/external_link/?url=https://instantcasinodeutschland.de/da-dk/
http://www.htcdev.com/ · July 23, 2026 at 9:23 pm
References:
Best online slots http://www.htcdev.com/?URL=instantcasinodeutschland.de%2Fda-dk%2F/
instrumiq.com · July 23, 2026 at 9:24 pm
grand casino coushatta
References:
https://www.instrumiq.com/employer/how-to-pay-credit-card-bill-credit-card-payment-amex-in/
kleinanzeigen.imkerverein-kassel.de · July 23, 2026 at 9:27 pm
References:
Casino games for ipad https://kleinanzeigen.imkerverein-kassel.de/index.php/author/adampinder/
https://kds.ne.kr/bbs/board.php?bo_table=free&wr_id=129278 · July 23, 2026 at 9:32 pm
References:
Nouveau brunswick https://kds.ne.kr/bbs/board.php?bo_table=free&wr_id=129278
central park Dog Racing Results · July 23, 2026 at 9:33 pm
betting expert horse central park Dog Racing Results tips
http://toolbarqueries.google.co.jp/url?rct=j&url=https://instantcasinodeutschland.de/da-dk/ · July 23, 2026 at 9:39 pm
References:
Laughlin casinos http://toolbarqueries.google.co.jp/url?rct=j&url=https://instantcasinodeutschland.de/da-dk/
https://wiki.zr.ru · July 23, 2026 at 9:50 pm
References:
Clam casino https://wiki.zr.ru/api.php?action=https://instantcasinodeutschland.de/da-dk/
https://jobworkglobal.com/ · July 23, 2026 at 9:52 pm
web roulette
References:
https://jobworkglobal.com/employer/list-of-all-new-australian-online-casinos-2026/
pcportal.org · July 23, 2026 at 9:59 pm
References:
Dover downs casino https://pcportal.org/go?https://instantcasinodeutschland.de/da-dk/
reviewer4you.com · July 23, 2026 at 10:08 pm
References:
Casino montelago https://reviewer4you.com/groups/fa-200-op-til-7-500/
wikimapia.org · July 23, 2026 at 10:15 pm
References:
Casino gta v https://wikimapia.org/external_link?url=https%3A%2F%2Finstantcasinodeutschland.de%2Fda-dk%2F
http://cse.google.co.cr/url?sa=t&url=http://instantcasinodeutschland.de/da-dk/ · July 23, 2026 at 10:27 pm
References:
Win casino http://cse.google.co.cr/url?sa=t&url=http%3A%2F%2Finstantcasinodeutschland.de%2Fda-dk%2F
opencage.cafe24.com · July 23, 2026 at 10:34 pm
References:
Seminole casino https://opencage.cafe24.com/shop3/m/member/login.html?returnUrl=https://instantcasinodeutschland.de/da-dk/
marine-zone.com · July 23, 2026 at 10:41 pm
vegas slot machines
References:
https://marine-zone.com/employer/payid-send-and-receive-faster-online-payments/
france-expat.com · July 23, 2026 at 10:46 pm
References:
Slot machine games for android https://france-expat.com/employer/online-casinoer-bedste-danske-casinoer-i-danmark-i-2026/
nodam.kr · July 23, 2026 at 10:52 pm
References:
Mcphillips street station casino https://nodam.kr/bbs/board.php?bo_table=free&wr_id=563870
https://jobcop.uk/employer/casino-anmeldelser-️-komplet-online-casino-test【2026】/ · July 23, 2026 at 10:57 pm
References:
Foxwood casino https://jobcop.uk/employer/casino-anmeldelser-%ef%b8%8f-komplet-online-casino-test%e3%80%902026%e3%80%91/
http://clients1.google.com.pr/url?sa=i&url=https://instantcasinodeutschland.de/da-dk/ · July 23, 2026 at 11:01 pm
References:
San manuel casino http://clients1.google.com.pr/url?sa=i&url=https%3A%2F%2Finstantcasinodeutschland.de%2Fda-dk%2F
Barbara · July 23, 2026 at 11:02 pm
wette deutschland schottland
Feel free to surf to my homepage :: basketball wetten tipps heute (Barbara)
https://ashkert.am/աշկերտի-համար/bedste-spilleautomater-og-velkomstbonus/ · July 23, 2026 at 11:09 pm
References:
Billy the kid casino https://ashkert.am/%D5%A1%D5%B7%D5%AF%D5%A5%D6%80%D5%BF%D5%AB-%D5%B0%D5%A1%D5%B4%D5%A1%D6%80/bedste-spilleautomater-og-velkomstbonus/
https://cyprusjobs.com.cy · July 23, 2026 at 11:09 pm
no deposit required
References:
https://cyprusjobs.com.cy/companies/best-payid-deposit-pokies-australia-2026-instant-play-nail-brewing-nbt-final-series/
https://govtpkjob.pk/companies/top-10-casinoer-i-dk-top-10-online-casinoer/ · July 23, 2026 at 11:17 pm
References:
Canadian gaming summit https://govtpkjob.pk/companies/top-10-casinoer-i-dk-top-10-online-casinoer/
https://mobidesign.us/ · July 23, 2026 at 11:19 pm
References:
Expekt casino https://mobidesign.us/employer/onlinekasino-med-de-hurtigste-udbetalinger-i-danmark
https://git.sortug.com/davidluciano61 · July 23, 2026 at 11:24 pm
References:
O l g slots https://git.sortug.com/davidluciano61
https://pracaeuropa.pl/companies/the-best-payid-casinos-in-australia-2026/ · July 23, 2026 at 11:28 pm
no deposit bonus
References:
https://pracaeuropa.pl/companies/the-best-payid-casinos-in-australia-2026/
online sportwetten und live-wetten für fussball tennis basketball eishockey · July 23, 2026 at 11:30 pm
live wetten verboten
Feel free to surf to my webpage … online sportwetten und live-wetten für fussball tennis basketball eishockey
https://fresh-jobs.in/employer/bedste-danske-casino-i-2026-testet-topliste/ · July 23, 2026 at 11:43 pm
References:
Spin palace https://fresh-jobs.in/employer/bedste-danske-casino-i-2026-testet-topliste/
friztty.com · July 23, 2026 at 11:56 pm
References:
Cinema casino bagnols sur ceze https://friztty.com/@stewartroybal7
worldaid.eu.org · July 23, 2026 at 11:57 pm
hard rock casino miami
References:
https://worldaid.eu.org/discussion/profile.php?id=2036200
https://beshortlisted.com/employer/support-programs-for-problem-gamblers-in-australia-practical-self-exclusion-options-for-aussie-punters/ · July 24, 2026 at 12:03 am
comeon casino review
References:
https://beshortlisted.com/employer/support-programs-for-problem-gamblers-in-australia-practical-self-exclusion-options-for-aussie-punters/
clients1.google.com.ni · July 24, 2026 at 12:08 am
References:
Vulcan casino http://clients1.google.com.ni/url?q=https://instantcasinodeutschland.de/da-dk/
git.talksik.com · July 24, 2026 at 12:16 am
References:
North brunswick soccer https://git.talksik.com/billghe742618
kurdishserie.com · July 24, 2026 at 12:20 am
References:
Best slot machines https://kurdishserie.com/@eugenioaiken6?page=about
https://jobzalert.pk/employer/de-bedste-online-casino-sider-i-danmark/ · July 24, 2026 at 12:23 am
References:
Connecticut casino https://jobzalert.pk/employer/de-bedste-online-casino-sider-i-danmark/
www.new.jesusaction.org · July 24, 2026 at 12:31 am
References:
Black jack gum https://www.new.jesusaction.org/bbs/board.php?bo_table=free&wr_id=3748520
bfreetv.com · July 24, 2026 at 12:33 am
References:
Sioux falls casino https://bfreetv.com/@biancasturgeon?page=about
http://www.google.bf/url?sa=t&url=https://instantcasinodeutschland.de/da-dk/ · July 24, 2026 at 12:37 am
References:
Hard rock casino http://www.google.bf/url?sa=t&url=https://instantcasinodeutschland.de/da-dk/
https://mp3banga.com/jennifer81m951 · July 24, 2026 at 12:38 am
References:
Mbs casino https://mp3banga.com/jennifer81m951
https://bluestreammarketing.com.co · July 24, 2026 at 12:42 am
william hill mobile casino
References:
https://bluestreammarketing.com.co/employer/payid-pokies-australia-2026-5-top-payid-pokies-sites-for-real-money/
https://gitea.lasallesaintdenis.com/vrrclyde107265 · July 24, 2026 at 12:46 am
References:
Shreveport casinos https://gitea.lasallesaintdenis.com/vrrclyde107265
images.google.com.ar · July 24, 2026 at 12:47 am
References:
Silverstar casino spa http://images.google.com.ar/url?sa=t&url=https://instantcasinodeutschland.de/da-dk/
mercedes-club.ru · July 24, 2026 at 12:48 am
References:
Paradise casino yuma az http://mercedes-club.ru/proxy.php?link=https://instantcasinodeutschland.de/da-dk/
https://fastping24.com · July 24, 2026 at 12:50 am
References:
Redhawk casino https://fastping24.com/@dustybent79475?page=about
gitea.accept.dev.dbf.nl · July 24, 2026 at 1:02 am
References:
Casino nights https://gitea.accept.dev.dbf.nl/gradymenendez9
https://www.monasticeye.com/@erinhorniman69?page=about · July 24, 2026 at 1:03 am
References:
Casino san francisco https://www.monasticeye.com/@erinhorniman69?page=about
https://govtpkjob.pk · July 24, 2026 at 1:04 am
References:
Oceans 11 casino https://govtpkjob.pk/companies/instant-%ef%b8%8f-instant-casino-officiel-hjemmeside-i-danmark/
https://www.bongmedia.tv/ · July 24, 2026 at 1:07 am
References:
Casino william hill https://www.bongmedia.tv/@deet4276163894?page=about
git.sistem65.com · July 24, 2026 at 1:08 am
References:
Video poker odds https://git.sistem65.com/denniseverson0
https://www.atlantistechnical.com/ · July 24, 2026 at 1:10 am
roulette layout
References:
https://www.atlantistechnical.com/employer/payid-withdrawal-speed-compared-2026-aussiepokies96/
https://www.globalshowup.com/ · July 24, 2026 at 1:12 am
References:
Chch casino https://www.globalshowup.com/@catalina12x27?page=about
https://aiviu.app/@charlenemosley?page=about · July 24, 2026 at 1:20 am
References:
California casino las vegas https://aiviu.app/@charlenemosley?page=about
https://jobs.cntertech.com/employer/dansk-casino-lov-2026/ · July 24, 2026 at 1:21 am
References:
No deposit bonus codes https://jobs.cntertech.com/employer/dansk-casino-lov-2026/
ophot.net · July 24, 2026 at 1:23 am
References:
Reef casino https://ophot.net/bbs/board.php?bo_table=notice&wr_id=92872
https://gitruhub.ru/ · July 24, 2026 at 1:25 am
References:
Mint casino https://gitruhub.ru/kristibourke0
https://www.workbay.online/ · July 24, 2026 at 1:33 am
miami jai alai casino
References:
https://www.workbay.online/profile/changdecicco3
gitea.accept.dev.dbf.nl · July 24, 2026 at 1:40 am
References:
Casino aztar https://gitea.accept.dev.dbf.nl/aletheafmz7448
https://medical-dictionary.thefreedictionary.com/_/cite.aspx?url=https://instantcasinodeutschland.de/da-dk/&word=medical emergency&sources=Segen · July 24, 2026 at 1:44 am
References:
Osage casino https://medical-dictionary.thefreedictionary.com/_/cite.aspx?url=https%3A%2F%2Finstantcasinodeutschland.de%2Fda-dk%2F&word=medical%20emergency&sources=Segen
http://images.google.al/url?q=https://instantcasinodeutschland.de/da-dk/ · July 24, 2026 at 1:46 am
References:
Casino vichy http://images.google.al/url?q=https://instantcasinodeutschland.de/da-dk/
media.izandu.com · July 24, 2026 at 1:47 am
References:
Venice casino https://media.izandu.com/@derickrosenbal?page=about
http://fr.thefreedictionary.com/_/cite.aspx?url=http://instantcasinodeutschland.de/da-dk/&word=s'etendre&sources=kdict · July 24, 2026 at 1:52 am
References:
Nars casino http://fr.thefreedictionary.com/_/cite.aspx?url=http%3a%2f%2finstantcasinodeutschland.de%2Fda-dk%2F&word=s%27etendre&sources=kdict
https://fairviewumc.church/ · July 24, 2026 at 1:55 am
References:
Lincoln casino https://fairviewumc.church/bbs/board.php?bo_table=free&wr_id=3748525
https://git.signalsmith-audio.co.uk/joshua74816960 · July 24, 2026 at 1:56 am
References:
Casino moncton https://git.signalsmith-audio.co.uk/joshua74816960
https://streamifyr.com/@antwan74t03503?page=about · July 24, 2026 at 1:57 am
References:
Prairie meadows casino https://streamifyr.com/@antwan74t03503?page=about
vmcworks.com · July 24, 2026 at 1:57 am
References:
Fiesta casino https://vmcworks.com/employer/top-10-casinoer-i-dk-top-10-online-casinoer
https://61.cholteth.com · July 24, 2026 at 2:02 am
References:
Emerald queen casino tacoma https://61.cholteth.com/index/d1?diff=0&utm_source=ogdd&utm_campaign=26607&utm_content=&utm_clickid=g00w000go8sgcg0k&aurl=https://instantcasinodeutschland.de/da-dk/
jobs.assist24-7.com · July 24, 2026 at 2:08 am
References:
Microgaming casino list https://jobs.assist24-7.com/employer/mastercard-casinoer-liste-top-5-danske-sider-med-mastercard/
https://talyca.com/companies/casino-uden-rofus-bedste-nem-udbetaling/ · July 24, 2026 at 2:10 am
References:
Eldorado casino reno https://talyca.com/companies/casino-uden-rofus-bedste-nem-udbetaling/
http://cse.google.ms · July 24, 2026 at 2:18 am
References:
Geant casino drive http://cse.google.ms/url?sa=i&url=https://instantcasinodeutschland.de/da-dk/
https://raovatonline.org · July 24, 2026 at 2:20 am
eagle mountain casino
References:
https://raovatonline.org/author/anniestoll/